Introduction
The anterior cruciate ligament (ACL), which resists
anterior tibial translational and rotational loads, is a key
structure in the knee joint and one of the most frequently injured
in clinical practice (1). Magnetic
resonance imaging (MRI) is the preferred method for the diagnosis
of ACL and associated injuries, and has been demonstrated to be
highly accurate in the assessment of the native ACL and complete
ACL tears. However, the sensitivity and specificity of MRI for the
detection of partial ACL tears is low. Grading the injury using MR
images is of benefit when planning ACL reconstruction surgery,
since partial tears do not always require surgical reconstruction.
If only one bundle is predominantly torn, isolated single bundle
reconstruction, rather than full ACL graft reconstruction, may be
undertaken. The grading of ACL tears describes the rupture pattern
more precisely. This may enable surgical planning to be improved
and allow reconstruction of the two bundles based on their
individual status. The early evaluation of partial ACL tears may
improve clinical and surgical management. Anatomical studies have
shown that the ACL consists of two distinct functional bundles,
termed the anteromedial (AM) and posterolateral (PL) bundles, based
on their tibial insertions (2).
The double-bundle model of the ACL is widely accepted. Studies of
biomechanics and kinematics have demonstrated that each bundle is
important in the stability of the knee. The AM and PL bundles have
distinct biomechanical functions, with the AM bundle stabilizing
the knee in flexion and the PL bundle stabilizing the knee in
extension (3,4). The double-bundle reconstruction
technique (DBT) aims to restore the function of the AM and PL
bundles (5). A prerequisite for
diagnosing ACL bundle injury using MR imaging is a clear
delineation of the two bundles and an awareness of their normal
appearance. Routine MRI examination planes are able to delineate
the normal ACL bundle structure in only 42% of knees (6). The value of standard planes to
distinguish injuries of the AM and PL bundles is limited and the
identification of an ideal combination of slice orientation,
thickness and pulse sequences remains a key area of investigation
(7,8). In the current study, we describe an
oblique coronal plane for imaging the normal ACL bundles using
low-field strength MRI at 0.2 T and evaluate the efficacy with
which the normal ACL bundles may be evaluated on this plane
compared with 3D reconstructions of the Chinese Visible Human (CVH)
dataset.
Subjects and methods
Subjects
The study population was selected during the period
from September 2004 to January 2007. This study was conducted in
accordance with the Declaration of Helsinki and with approval from
the Ethics Committee of the Southwest Hospital of the Third
Military Medical University (Chongqing, China). Written informed
consent was obtained from all participants. MR images were obtained
from 120 knees according to the imaging protocol. The inclusion
criteria for the study population consisted of completed growth
(closed epiphyseal plates), an age of ≤50 years and no previous
injury or knee surgery. All knee MR images were reviewed by three
radiologists, and only knees with an intact cruciate ligament were
included. Knees that displayed evidence of notch hypoplasia or
stenosis, or partial or complete ACL or PCL deficiencies were
excluded. The study population consisted of 120 individuals (60
males and 60 females; age range, 22–48 years; mean age, 34 years),
who were divided into four groups: left and right knee in female or
male patients.
MRI was performed with a low-field 0.2 T Artoscan
MRI scanner (Esaote S.p.A., Genova, Italy), with the knee held in
full extension. Images of the knee were typically obtained in the
axial, oblique sagittal and oblique coronal planes, with the
coronal plane oriented parallel to a line drawn through the
epicondyles. The oblique sagittal images were planned on axial
images and oriented at 90° to the coronal images. The MRI protocol
consisted of an oblique sagittal T1-weighted spin echo [repetition
time/echo time (TR/TE)=840/26 msec]; a T2-weighted turbo spin echo
[TR/TE=3,000/80 msec; echo train length (ETL), 4; slice thickness,
4 mm; interval, 0.2 mm; matrix, 256×256; field of view (FOV), 12
cm] and a double echo with T2 and proton density-weighted images
and coronal T2-weighted gradient echo (TR/TE=480–560/16–20 msec,
flip angle, 400). The oblique coronal slices were planned to be
parallel to the course of the femoral intercondylar roof on a
sagittal scout image and acquired in T2-weighting
(TR/TE=3,000–4,000/96 msec; ETL, 2; slice thickness, 2–3 mm;
interval, 0.2–0.3 mm; matrix, 256×125) and T1-weighting
(TR/TE=540–600/28 msec).
For the coronal, sagittal and oblique images, each
observer was asked to evaluate whether they were able to
distinguish the AM and PL bundles at the femoral, mid-substance and
tibial levels. Each MRI was independently read in a blinded fashion
by a total of three observers: one musculoskeletal
fellowship-trained radiologist, one senior orthopedic resident and
one junior orthopedic resident. The time between observations for
each reviewer was at least 4 weeks.
Cryosection of specimens
Following the acquisition of approval from the
Institutional Ethical Committee, middle-sized male cadavers without
organic lesions, as verified by visual inspection, were examined.
Subsequent to vascular perfusion, the specimens were embedded in
gelatin and then placed in a −30°C saline pool for cryopreservation
for 1 week, prior to being stored in the laboratory at −25°C. The
specimens were serially sectioned from head to foot (sectioning
accuracy: 0.0001 mm) using a TK-6530 Digital Sectioner (Hanzhong
Machine Tool Factory, Hangzhou, China). The slice thicknesses were
0.5 and 0.25 mm. Photographic images of all slices were serially
captured using a digital camera (Canon, Tokyo, Japan) with a
resolution of 3,072×2,048 and each sectioned image file of 36 MB
was stored on a personal computer (PC).
Computerized 3D reconstruction
Prior to embedding, four plastic rods were placed in
the mold parallel to the long axis of the cadaver for use as a
reference for the alignment of the computerized slices. The
alignment was performed on a PC. Using the commercially available
Amira® 3D reconstruction software (Visualization
Sciences Group, Boston, MA, USA), the single slices were merged
into a 3D dataset. The 2D images of the ACL were reconstructed in
sagittal, coronal and oblique coronal sections. On the
cryospecimen, the orientation of the coronal oblique plane was
defined along the true anatomical course of the ACL. This was
achieved by adjusting the angle of the cryosectional plane parallel
to the femoral intercondylar roof. The length and the angle of the
ACL were measured on the oblique sagittal planes. The statistical
analysis was performed using standard software (SPSS for Windows,
version 10.0; SPSS, Inc., Chicago, IL, USA). P<0.05 was
considered to indicate a statistically significant result.
Results
Measurement of the ACL
The structure of the two ACL bundles was reviewed on
the MR images. The two bundles of the ACL were not clearly
distinguishable on the oblique sagittal or coronal planes. For the
left and right knee groups, the length, width and coronal angle of
the ACL are summarized in Table I.
The ideal angulations of the oblique coronal slices were obtained
from an average coronal angle of the ACL. There were no significant
differences in the length and thickness of the ACL between the left
and right knee groups; however, significant differences were
observed in the length, thickness and coronal angles between males
and females.
 | Table I.Measurement of the ACL in the oblique
plane (n=60). |
Table I.
Measurement of the ACL in the oblique
plane (n=60).
| Group | Length (mm) | Thickness (mm) | Angle (°) |
|---|
| Left knee | 35.31±1.76 | 5.79±1.08 | 36.3±2.3 |
| Right knee | 35.66±2.53 | 5.75±1.21 | 35.5±2.8 |
| Male | 36.45±1.98 | 6.09±1.07 | 36.4±2.5 |
| Female | 34.52±1.93 | 5.45±1.13 | 35.4±2.5 |
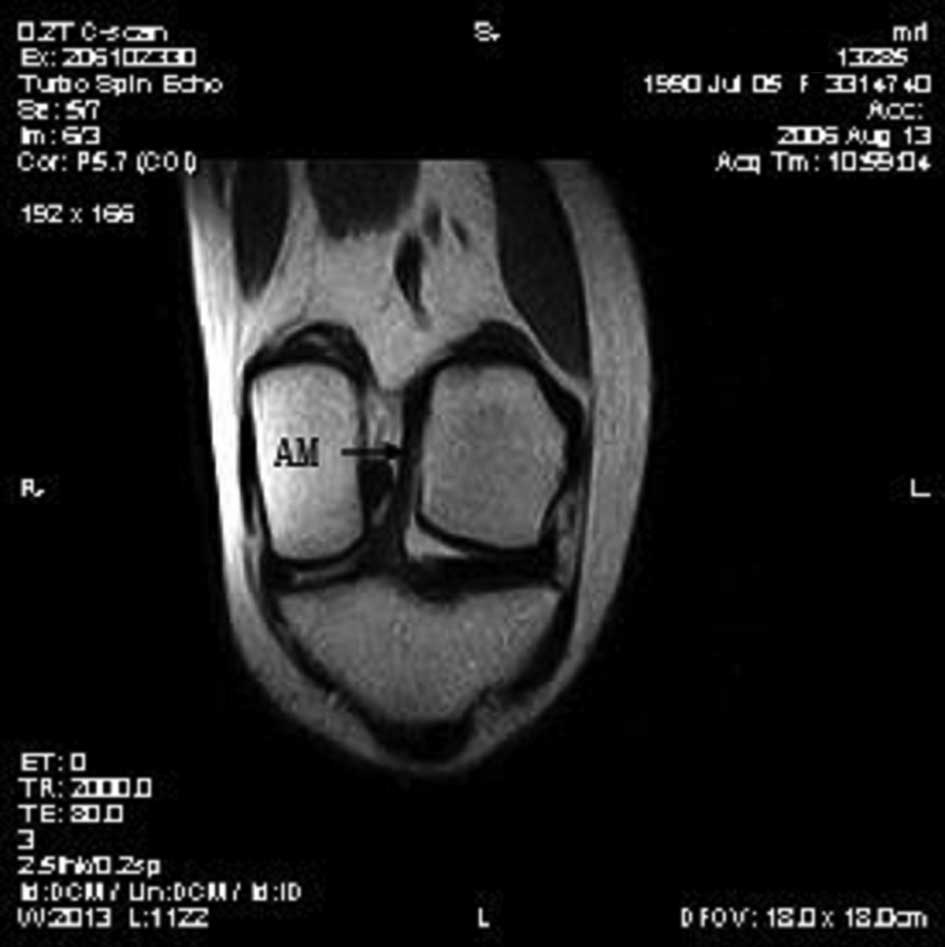
AM and PL bundles
The oblique coronal slices were suitable for
displaying the AM and PL bundles separately. In the imaging slab,
the anterior slices displayed the AM and the posterior slices
displayed the PL bundles (Figs.
1–3; Table II). In the central image, which
showed the two bundles next to each other, a septum-like high
intensity structure was observed between the two bundles. The
oblique coronal plane visualized the femoral and tibial insertion
sites with a greater precision than the sagittal and coronal
planes.
| Table II.Agreement between readers with regard
to the ability to distinguish the AM and PL bundles of the ACL
separately. |
Table II.
Agreement between readers with regard
to the ability to distinguish the AM and PL bundles of the ACL
separately.
| Images | Readers |
|---|
|
|---|
| 1 vs. 2 | 2 vs. 3 | 1 vs. 3 |
|---|
| Oblique oblique
images | 0.88 | 0.91 | 0.93 |
| Oblique coronal
images | 1 | 1 | 1 |
In the Chinese Visible Human male dataset, the 3D
visualization model of the knee provided an anatomical insight into
the ACL in the axial, sagittal and coronal planes; however, the
integrity of the AM and PL bundles in their course was not
displayed. On the coronal oblique slices oriented parallel to the
femoral intercondylar roof inclination, the two bundles were
clearly demonstrated. On the reconstructed images in the coronal
oblique plane, the ACL exhibited a diagonal course from the
posterior superior aspect of the intercondylar surface of the
lateral femoral condyle, corresponding to Blumensaat’s line. The
length was 35 mm and the thickness 6 mm, running obliquely through
the lateral third of the intercondylar notch to the tibial
insertion on the central and medial section of the anterior
intercondylar area of the tibia. On the reconstructed coronal
oblique images, the bony attachment of the ACL was clearly shown on
the posterior inner surface of the lateral femoral condyle. The AM
bundle was inserted into the cartilage of the ascending section of
the central ridge of the medial tibial plateau and the anteromedial
tubercle of the intercondylar eminence. The PL bundle was inserted
into the cartilage of the ascending section of the central ridge of
the lateral tibial plateau, and the posterolateral tubercle of the
intercondylar eminence (Figs.
4–6). A septum-like, fatty
synovial tissue occupied the space between the two bundles. In the
oblique coronal plane, the AM bundle of the ACL was limited
distally by the cartilage covering the medial femoral condyle and
formed the vertically-oriented section of the PCL complex (Fig. 1).
Discussion
MRI is the method of choice for imaging the ACL in
cases of suspected lesions, particularly in surgical planning.
Since the anatomy of this ligament is difficult to capture using
traditional slice orientations, the present study optimized the
slice orientation adapted to the anatomy of the ligaments. To
verify the diagnostic quality of the acquired images, particularly
at a low magnetic field strength of 0.2 T in a dedicated
musculoskeletal MRI scanner, the resulting images were compared
with reconstructed slices from a sectional anatomy dataset: the CVH
dataset.
The ACL is one of the principle ligaments that
stabilize the knee. From a functional perspective, it is composed
of two separate bundles: The AM bundle originates from the superior
aspect of lateral side of the femoral notch and inserts into the
anteromedial part of tibia, whereas the PL bundle arises from a
lower level of the lateral side of the femoral notch and inserts
into the posterolateral part of tibia (9–11).
The results of the present study were consistent with the
double-bundle model. The two bundles are not isometric in flexion
and extension, instead exhibiting different patterns of length
changes during passive knee flexion (12). The AM of the ACL primarily controls
the anterior movement of the tibia underneath the femur, while the
PL bundle is significant in maintaining the rotational stability in
the knee, such as during pivoting, twisting and jumping (13,14).
Hollis et al demonstrated that the AM lengthens and tightens
in flexion, while the PL shortens and becomes slack (15).
Steckel et al (16) evaluated the double-bundle structure
of the ACL with 3 T high-field MRI of cadaver knees. The AM and PL
bundles were visible in the majority of views, suggesting that a
higher field strength may be more effective for distinct imaging.
Starman et al (10)
assessed the standard planes of view for the detection of the AM
and PL bundles. The results suggested that standard sagittal and
coronal views may allow a reliable detection of the AM bundle;
however, the PL bundle is more difficult to image. It is likely
that these results were due to a partial volume or blurring effect
of the low-resolution images of the two adjacent bundles, making
them appear as only one structure.
High-quality visualizations of the individual ACL
bundles may be achieved most effectively in planes that are based
on the natural course of the ACL (7,17).
The ACL has an average angle ranging from 35–40° to the coronal
plane. The measured length of the ACL ranges from 32 to 38 mm, with
a width ranging from 4 to 7 mm in the oblique sagittal plane. In
this plane, it was possible to distinguish the AM and PL
bundles.
The current standard in ACL reconstruction surgery
is the single-bundle arthroscopic technique (18); however, a number of surgeons have
advocated the DBT to restore the AM and PL bundles separately,
based on biomechanical and kinematic studies (3). In a partial tear of the ACL, the AM
or PL bundle may be intact, and novel surgical techniques enable
the preservation of an intact AM or PL bundle (19). The preoperative assessment of the
injured ligament is therefore essential for surgeons, as it is
necessary to identify whether an intact bundle is present. This
leads to a more refined surgical approach and improved outcomes.
Complete ACL tears may be accurately identified in each of the
standard MRI planes (sagittal, coronal and axial) with high
sensitivity and specificity (17,20);
however, the identification of partial ACL tears in standard planes
using a low-field strength musculoskeletal MRI has been
demonstrated to be more challenging (21). The results of the present study
showed that the AM and PL bundles of the ACL may be clearly
displayed on oblique coronal sections on anatomical 3D
reconstructions and low-field MRI. Furthermore, a septum was
observed between the AM and the PL bundles, which was not described
in previous studies (22,23). The septum-like structure was
detected on the present MR images as a high-intensity structure,
which may be correlated to fibrofatty and synovial tissue in the
CVH 3D model.
Using this method of adapting the MRI planes to the
knee anatomy, it may be possible to improve the depiction of
structural details of the AM and PL bundles. The additional
information gained is likely to improve the diagnostic accuracy in
the grading of ACL injuries, which may support the surgical
decision for ACL reconstruction. The oblique coronal plane was
shown to be the preferred imaging plane for the assessment of the
bundle architecture. This result was consistent with the study by
Hong et al (7), which
demonstrated that the diagnostic accuracy for ACL tears was
improved with additional oblique coronal planes compared with the
standard orientations.
High-resolution isotropic datasets from cryosections
and MRI may be reformatted using visualization software on standard
PC hardware. With this technique, images of the knee, and
particularly the ACL, may be reconstructed in virtually every
orientation, in the conventional axial, coronal and sagittal
planes, as well as in the oblique coronal plane. The anatomical
view of the ACL shown with the oblique coronal plane is most
suitable for displaying the shape of the ACL and its anatomical
relationships. The results of the present 3D cryosectional and MRI
visualization study were comparable with the observations by
Stäubli and Rauschning (24),
obtained with contrast magnetic resonance arthrography. The
anatomical orientation of the oblique course of the ACL is parallel
to Blumensaat’s line. In the present study, a triangle was observed
that was formed by the AM and PL bundles and their tibial
attachments and filled by fibrofatty and synovial tissue. The MRI
observations of the ACL were consistent with these results. The 3D
reconstruction revealed that the two bundles were not isometric in
the oblique coronal plane. It was also demonstrated that the long
axes of the two bundles were not parallel.
Based on evidence from the 3D visualization of the
CVH dataset and MRI analysis of the cruciate ligaments in the
oblique coronal plane, oblique coronal imaging of the ACL in
extension may be recommended for inclusion in routine MR knee
imaging protocols for the assessment of ACL tears, particularly if
the diagnosis of an ACL tear is doubtful, based on clinical
findings. Multiplanar reconstruction and the use of the oblique
coronal plane may improve the understanding of the ACL anatomy and
provide a valuable method for teaching and research. The
reconstructed images provide the anatomical basis for imaging
diagnosis and surgery.
This study used a low-field strength musculoskeletal
MRI scanner and 3D visualization in oblique coronal planes for the
assessment of the double-bundle anatomy of the ACL. The results
showed that this technique reliably visualizes the two bundles of
the ACL. The use of additional oblique slices for the evaluation of
the AM and PL bundles offers a potential solution for an improved
evaluation with low-field strength magnets. It may assist in the
preoperative assessment and grading of ACL injuries to facilitate
ACL reconstruction, in addition to being used in research and
teaching.
References
|
1.
|
Matsumoto H, Suda Y, Otani T, Niki Y,
Seedhom BB and Fujikawa K: Roles of the anterior cruciate ligament
and the medial collateral ligament in preventing valgus
instability. J Orthop Sci. 6:28–32. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Amis AA and Dawkins GP: Functional anatomy
of the anterior cruciate ligament. Fibre bundle actions related to
ligament replacements and injuries. J Bone Joint Surg Br.
73:260–267. 1991.PubMed/NCBI
|
|
3.
|
Yagi M, Wong EK, Kanamori A, Debski RE, Fu
FH and Woo SL: Biomechanical analysis of an anatomic anterior
cruciate ligament reconstruction. Am J Sports Med. 30:660–666.
2002.PubMed/NCBI
|
|
4.
|
Yamamoto Y, Hsu WH, Woo SL, Van Scyoc AH,
Takakura Y and Debski RE: Knee stability and graft function after
anterior cruciate ligament reconstruction: a comparison of a
lateral and an anatomical femoral tunnel placement. Am J Sports
Med. 32:1825–1832. 2004. View Article : Google Scholar
|
|
5.
|
Cha PS, Brucker PU, West RV, et al:
Arthroscopic double-bundle anterior cruciate ligament
reconstruction: an anatomic approach. Arthroscopy.
21:12752005.PubMed/NCBI
|
|
6.
|
Kaya A, Karadağ D, Güçlü B, Uçar F and
Benli IT: Evaluation of the two bundles of the anterior cruciate
ligament with 1.5 tesla magnetic resonance imaging. Acta Orthop
Traumatol Turc. 44:54–62. 2010. View Article : Google Scholar
|
|
7.
|
Hong SH, Choi JY, Lee GK, Choi JA, Chung
HW and Kang HS: Grading of anterior cruciate ligament injury.
Diagnostic efficacy of oblique coronal magnetic resonance imaging
of the knee. J Comput Assist Tomogr. 27:814–819. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Katahira K, Yamashita Y, Takahashi M, et
al: MR imaging of the anterior cruciate ligament: value of thin
slice direct oblique coronal technique. Radiat Meds. 19:1–7.
2001.PubMed/NCBI
|
|
9.
|
Steckel H, Vadala G, Davis D and Fu FH: 2D
and 3D 3-tesla magnetic resonance imaging of the double bundle
structure in anterior cruciate ligament anatomy. Knee Surg Sports
Traumatol Arthrosc. 14:1151–1158. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Starman JS, Vanbeek C, Armfield DR, et al:
Assessment of normal ACL double bundle anatomy in standard viewing
planes by magnetic resonance imaging. Knee Surg Sports Traumatol
Arthrosc. 15:493–499. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Montoy M, Euvrard T, Moyen B, Roy P,
Rollier JC and Cotton F: Inter-observer agreement in the
identification of the two bundles of the anterior cruciate ligament
using magnetic resonance imaging. Surg Radiol Anat. 30:557–562.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Girgis FG, Marshall JL and Monajem A: The
cruciate ligaments of the knee joint. Anatomical, functional and
experimental analysis. Clin Orthop Relat Res. 106:216–231. 1975.
View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Amis AA and Dawkins GP: Functional anatomy
of the anterior cruciate ligament. Fibre bundle actions related to
ligament replacements and injuries. J Bone Joint Surg Br.
73:260–267. 1991.PubMed/NCBI
|
|
14.
|
Zantop T, Herbort M, Raschke MJ, Fu FH and
Petersen W: The role of the anteromedial and posterolateral bundles
of the anterior cruciate ligament in anterior tibial translation
and internal rotation. Am J Sports Med. 35:223–227. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Hollis JM, Takai S, Adams DJ, Horibe S and
Woo SL: The effects of knee motion and external loading on the
length of the anterior cruciate ligament (ACL): a kinematic study.
J Biomech Eng. 113:208–214. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Steckel H, Vadala G, Davis D, Musahl V and
Fu FH: 3-T MR imaging of partial ACL tears: a cadaver study. Knee
Surg Sports Traumatol Arthrosc. 15:1066–1071. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Duc SR, Zanetti M, Kramer J, Käch KP,
Zollikofer CL and Wentz KU: Magnetic resonance imaging of anterior
cruciate ligament tears: evaluation of standard orthogonal and
tailored paracoronal images. Acta Radiol. 46:729–733. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Yunes M, Richmond JC, Engels EA and
Pinczewski LA: Patellar versus hamstring tendons in anterior
cruciate ligament reconstruction: A meta-analysis. Arthroscopy.
17:248–257. 2001. View Article : Google Scholar
|
|
19.
|
Ochi M, Adachi N, Deie M and Kanaya A:
Anterior cruciate ligament augmentation procedure with a 1-incision
technique: anteromedial bundle or posterolateral bundle
reconstruction. Arthroscopy. 22:463e1–e5. 2006.
|
|
20.
|
Mellado JM, Calmet J, Olona M, Giné J and
Saurí A: Magnetic resonance imaging of anterior cruciate ligament
tears: reevaluation of quantitative parameters and imaging findings
including a simplified method for measuring the anterior cruciate
ligament angle. Knee Surg Sports Traumatol Arthrosc. 12:217–224.
2004. View Article : Google Scholar
|
|
21.
|
Umans H, Wimpfheimer O, Haramati N,
Applbaum YH, Adler M and Bosco J: Diagnosis of partial tears of the
anterior cruciate ligament of the knee: value of MR imaging. AJR Am
J Roentgenol. 165:893–897. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Odensten M and Gillquist J: Functional
anatomy of the anterior cruciate ligament and a rationale for
reconstruction. J Bone Joint Surg Am. 67:257–262. 1985.PubMed/NCBI
|
|
23.
|
Duthon VB, Barea C, Abrassart S, Fasel JH,
Fritschy D and Ménétrey J: Anatomy of the anterior cruciate
ligament. Knee Surg Sports Traumatol Arthrosc. 14:204–213. 2006.
View Article : Google Scholar
|
|
24.
|
Stäubli HU and Rauschning W: Tibial
attachment area of the anterior cruciate ligament in the extended
knee position. Anatomy and cryosections in vitro complemented by
magnetic resonance arthrography in vivo. Knee Surg Sports Traumatol
Arthrosc. 2:138–146. 1994.PubMed/NCBI
|