Introduction
The flexible ureteroscope has been widely used by
numerous urologists in the management of upper urinary tract
calculi (including renal and ureteral stones), due to its desirable
therapeutic effect. The ureteroscopy process uses the natural
channels of the human body, making it minimally invasive, and
provides an essentially unhindered view throughout. However, the
traditional one-piece flexible ureteroscope is expensive and
vulnerable during surgery. In addition, it has high maintenance
costs and a long repair cycle. Therefore, the German company,
Polydiagnost GmbH (Pfaffenhofen, Germany), has developed a new,
high-end, minimally invasive modular flexible ureteroscope
(PolyScope™). This removable modular flexible ureteroscope has core
components, such as the optical and imaging systems, which have
been designed as independent parts and are convenient to assemble
and disassemble. The optical system of the PolyScope utilizes
single optical fiber technology, and has a soft and tough synthetic
metal wrapped around the surface for protection. During its use, it
is placed into the fiber channel of the lens barrel. The PolyScope
produces stable and clear images; thus, it has been suggested to be
an effective solution for overcoming the shortcomings of the
conventional flexible ureteroscope (1). In the present study, 86 patients with
upper urinary tract calculi with a diameter of <2 cm were
treated with the modular flexible ureteroscope in the Xinghua
Hospital Affiliated to Shanghai Jiao Tong University (Shanghai,
China). The results were satisfactory and are discussed in the
following sections.
Materials and methods
Patients
A total of 86 patients (53 males and 33 females,
aged from 20 to 86 years) with upper urinary tract calculi who were
admitted to the Xinghua Hospital Affiliated to Shanghai Jiao Tong
University from November 2010 to May 2012 were recruited for this
study. Thirty-nine patients presented with upper ureteral calculi,
eight with renal pelvic calculi, three with upper calyceal calculi,
four with middle calyceal calculi, 21 with lower calyceal calculi,
eight with ureteral and lower calyceal calculi, one with ureteral
and middle calyceal calculi, one with renal pelvic and lower
calyceal calculi, and one with middle and lower calyceal calculi.
In addition, 45 patients exhibited left-sided calculi, whereas 41
patients exhibited right-sided calculi. The mean diameter of the
calculi was 1.23±0.27 cm. Nineteen patients (11 patients with
ureteral stenosis, six with urinary tract infection and two with
renal insufficiency) had previously had an indwelling double-J
stent, placed with ureteroscopic guidance, for a duration of 2–8
weeks. The major clinical manifestations of the patients were
ipsilateral lower back pain, abdominal pain, urinary tract
infection and gross or microscopic recurrent hematuria. The
majority of the patients had been hospitalized and undergone
surgery following conservative treatment, such as treatment against
infection; however, the extra water and medical expulsive therapies
failed to cure the symptoms. The case inclusion criteria for the
present study were as follows: The distance from the pelvis to the
upper ureteral calculi was <5 cm; the diameter of the stones was
<2.0 cm in the pelvis and the upper and middle calyces; the
diameter of the stones was <1.5 cm in the lower calyx; and the
patients were without combined surgical contraindications. The
patients and their relatives were briefed with regard to the
details of the surgical intervention for the upper urinary tract
calculi, the choice of surgical approach, the advantages and
disadvantages of flexible ureteroscopy combined with holmium laser
lithotripsy and the surgical risks. This study was conducted in
accordance with the Declaration of Helsinki and with approval from
the Ethics Committee of Xinhua Hospital Affiliated to Shanghai Jiao
Tong University. Written informed consent was obtained from all
participants.
Methods
The patients were placed under general or spinal
anesthesia and in a lithotomy position. Having located the
ipsilateral ureter, a zebra guide wire was inserted and a Wolf
F8/9.8 ureteroscope (Richard Wolf GmbH, Knittlingen, Germany) was
placed into the ureter so as to reach the level of the pelvis and
determine the approximate distribution of the intrarenal calyceal.
Following the removal of the ureteroscope, a Cook F12/14 Ureteral
Access Sheath (UAS; Cook Medical, Inc., Bloomington, IN, USA) was
positioned along the guide wire. The UAS was moved as close to the
level of the ureteropelvic junction as possible. The Polydiagnost
F8 modular flexible ureteroscope (Polydiagnost GmbH) was placed
into the pelvis along the UAS. A 220 mm holmium laser lithotripsy
with a power setting of 1.0 J at 10–20 Hz was used when stones were
encountered. The ‘nibble’ approach was used to break and crumble
the stones into fine granules measuring 2–3 mm, in order to avoid
prolonging the surgery unnecessarily while performing repeated
searches for stones that had been broken into large pieces. Stones
measuring ≤4 mm were removed with a stone basket and some lower
calyceal stones were trans-located with the stone basket from the
lower to the upper or middle calyx, in order to improve the
efficiency of the stone breaking. An F6 double-J stent was
typically indwelling for 4 weeks following the surgery and a
Foley’s urethral catheter was indwelling for 1–7 days. Plain film
of kidney-ureter-bladder (KUB) was performed 1 day subsequent to
the surgery, in order to determine the result of the lithotripsy
and the position of the double-J stent. However, in certain
patients, KUB radiography was performed 2–4 weeks following the
surgery. Extracorporeal shockwave lithotripsy (ESWL) was performed
if the diameter of any residual stones was >6 mm.
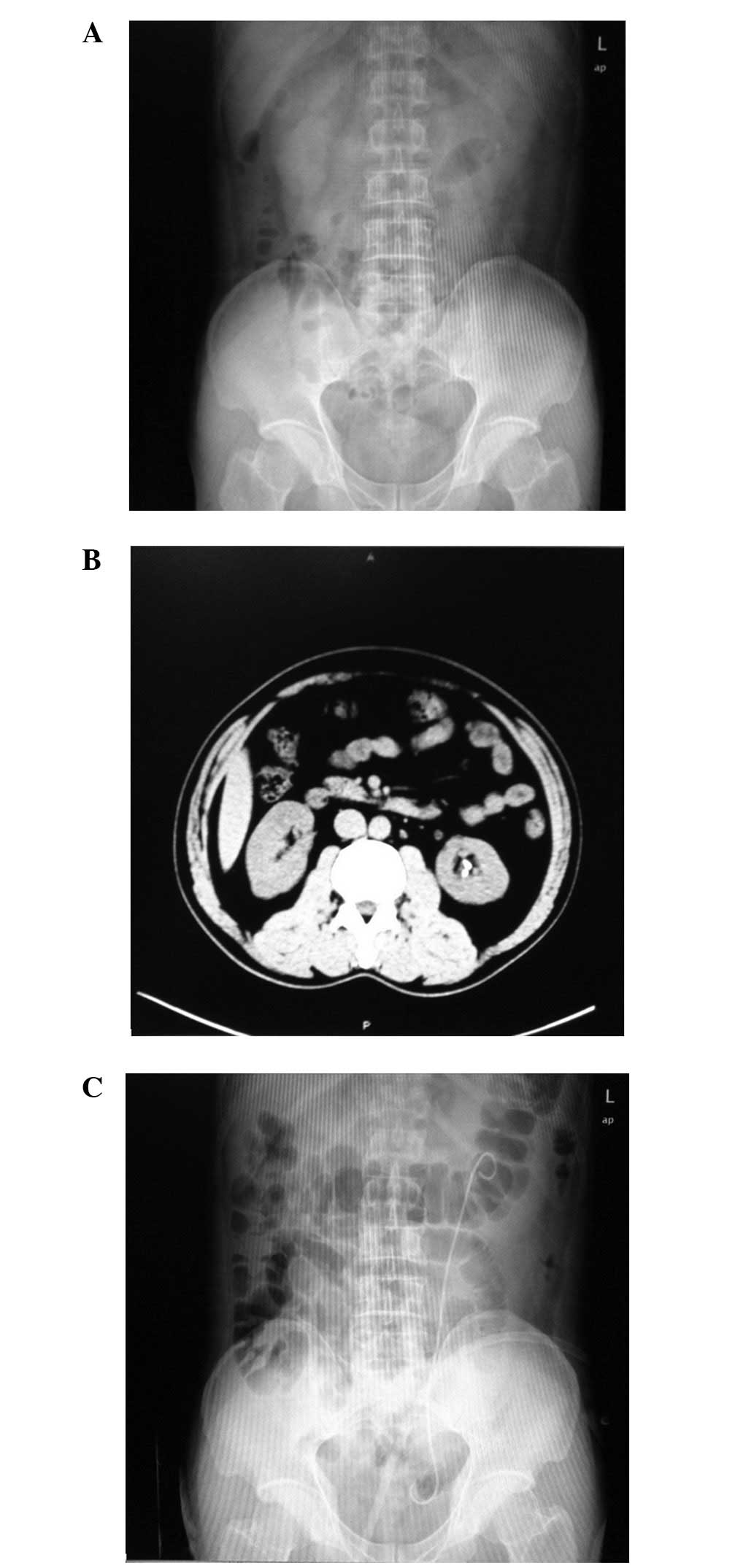
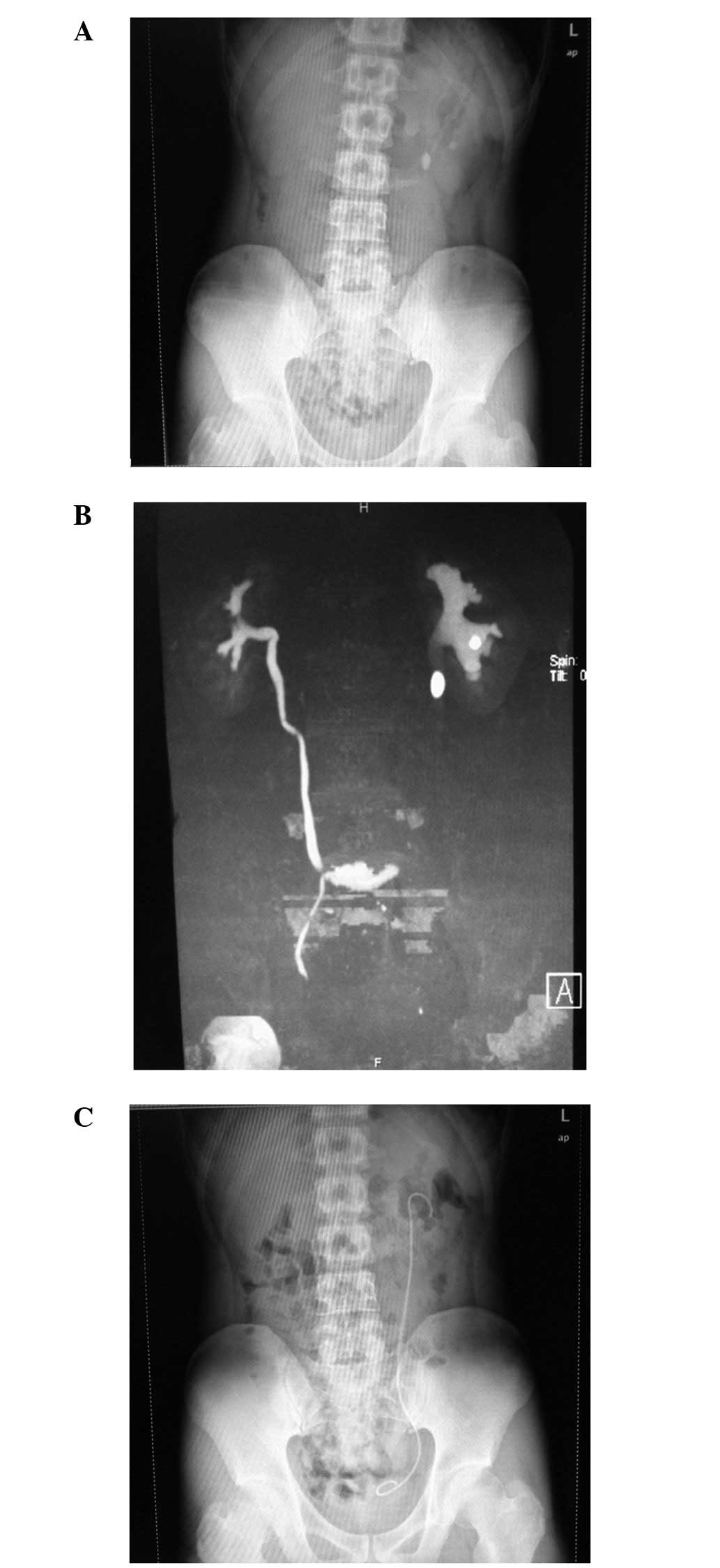
Results
Lithotripsy was performed successfully in 77
patients. The duration of the surgery ranged from 25 to 80 min
(mean duration, 42 min). Little bleeding was recorded. Three
patients presented with a slight fever following the surgery;
however, no ureteral perforation, high fever or septicemia was
observed among the patients following anti-inflammatory treatment.
The stone-free rate (SFR) of the single-pass lithotripsy was 89.5%
(77/86). Among the remaining nine patients, three patients with
upper ureteral calculi and one with calyceal calculi exhibited
postoperative residual stones and underwent ESWL; in addition, one
patient underwent percutaneous nephrolithotomy (PCNL) due to a
narrow and distorted ureteral structure. Among the four cases with
lower calyceal calculi, three underwent ESWL, as the angle of the
funnel pelvis was too narrow (two cases were successful and one
case had residual stones due to the hardness of the calculi). One
patient with lower calyceal calculi did not undergo further
procedures, since the patient’s kidney exhibited severe
hydrocephalus and location of the stones was not possible.
Therefore, the SFR with ESWL was 96.5% (83/86). The postoperative
follow-up period was 1–3 months. No residual fragments measuring
>3 mm remained following the reviews with B-mode ultrasound or
radiography. The longest stone expulsion time was 7 weeks (Figs. 1–3).
Discussion
Calculus of the urinary tract is a common disease
requiring surgical intervention. According to global statistics,
between 5 and 15% of the population suffer from urinary stone
disease (2). The use of
lithotripsy with a flexible ureteroscope for the treatment of renal
or ureteral stones demonstrates numerous advantages, including
minimal invasiveness, safety, good efficacy, little pain, rapid
recovery and direct visibility; thus, an increasing number of
urologists are inclined to use flexible ureteroscopy to manage
renal or ureteral stones. According to the present relevant
guidelines on urolithiasis treatment in Europe and the United
States and from the China Urology Association, the main
international indications for flexible ureteroscopy in the
treatment of renal stones are: X-rays are negative for stones,
leading to difficulties with ESWL positioning (<2 cm); the
presence of residual lower calyceal stones following ESWL surgery;
incarcerated lower calyceal stones, resulting in a poor efficacy
with ESWL; the presence of hard stones (such as calcium oxalate
monohydrate, or cystine calculi) which are unsuitable for ESWL
treatment; extremely obese patients or individuals with a serious
spinal deformity, in whom there may be difficulties establishing
PCNL; and the presence of intradiverticular calyceal stones
accompanied by calyceal neck stenosis. In addition, other special
cases also exist, such as combined hemorrhagic diathesis, horseshoe
kidney, pelvic ectopic kidney, complex renal anatomy, solitary
renal calculi, lower calyceal calculi <2 cm and children with
renal calculi <1.5 cm. Even renal calculi measuring between 2
and 4 cm have been recommended for treatment using flexible
ureteroscopic lithotripsy (3–11).
Therefore, the effects of flexible ureteroscopic lithotripsy have
been demonstrated to be approximately equal to those of PCNL, but
higher than those of ESWL, while the surgical risks of flexible
ureteroscopic lithotripsy have been demonstrated to be lower than
those of PCNL. Furthermore, the convalescence has been shown to be
more rapid for flexible ureteroscopic lithotripsy than PCNL and the
risk of long-term complications has been shown to be lower than
that for ESWL (12,13). Compared with ESWL and PCNL,
flexible ureteroscopy has the advantages of being minimally
invasive, exhibiting a desirable efficacy and resulting in fewer
complications, thus making it more acceptable for doctors and
patients. Therefore, with the increase in risk awareness shown by
doctors and patients, economic development and the widespread focus
on health, the use of a flexible ureteroscope combined with a
holmium laser in the treatment of urinary stones has gradually
become one of the main approaches for lithotripsy (4,7,8).
However, the loss and maintenance of flexible ureteroscopes has
been a major challenge in clinical practice. At present, the
flexible ureteroscope commonly used in clinical practice is
expensive and has a high maintenance cost and long maintenance
cycle, which limit the application of flexible ureteroscopy. It has
been suggested that flexible cystoscopes undergo major damage due
to the passing of certain tools, such as optical fibers and stone
extraction forceps, through the working channel (14). Afane et al (15) assessed a selection of 9Fr flexible
utero-scopes, including the Storz model 11274AA, the double-dagger
Circon-ACMI model AUR-7 and the Wolf 7325.172 model, and observed
that it was necessary for the uteroscopes to be maintained
following 6–15 surgeries and 3–12.8 h of surgical time.
The removable modular flexible ureteroscope is
similar in shape to the traditional flexible ureteroscope; however,
the camera optical fiber, imaging systems and other core components
are provided as independent components. Consumable components, such
as the endoscope, may be removed and replaced easily. The most
valuable component is the optical system, which is adapted from the
technology of a single-mode optical fiber. A metal alloy surrounds
the fiber surface for protection. When the optical system is
utilized, it is placed into the endoscopic fiber channel. Unlike
the traditional quartz collection fiber structure, it has 10,000
pixels, and is able to detect targets with a diameter of ∼0.125 mm
within a distance of 2–4 mm, and is able to transfer clear and
stable images without spots, grids or honeycomb artifacts. The
working channel of the removable modular flexible ureteroscope is
3.6 F, which is similar to that of a traditional flexible
ureteroscope. In an empty working channel, the lens barrel has been
demonstrated to bend at an angle of 265°; the bending angle is
reduced by 10 and 2%, respectively, following the insertion of a
3.0F stone basket or a 200 μm laser fiber (1). At a perfusion pressure of 100 mmHg,
the perfusion flow rate has been reported to decrease by 50 and 70%
(to 28.5 ml/min and 18.3 ml/min) following the insertion of 200
μm and 365 μm fibers, respectively. These conditions
meet the basic visual demand of a flexible ureteroscope with a 10
ml/min flow rate (1,16).
In the present study, the modular flexible
ureteroscope was used to treat 86 cases of kidney and ureter
lithiasis, involving stones located in the renal pelvis, the upper,
middle and lower calyces and the upper ureter. The overall effect
was satisfactory with a single-pass SFR of 89.5% (77/86), a
second-pass SFR of 96.5% (83/86), an upper ureteral calculi SFR of
89.7% (35/39) and a calyceal calculi SFR of 87.1% (27/31). With
regard to the use of a modular flexible ureteroscope combined with
a holmium laser for the treatment of upper urinary calculi in these
86 cases, there were several points of note. It was realized that,
prior to the insertion of the modular flexible ureteroscope, it was
necessary for the UAS of the flexible ureteroscope to be indwelling
and for the end of the UAS to be placed near the level of the
ureteropelvic junction (on encountering ureteral stenosis, it was
not possible to perform a single-pass placement of the UAS in the
ureter; in such cases, an F6 double-J stent was indwelling for a
second lithotrity). The indwelling UAS helped to reduce the renal
pelvic pressure during surgery. Rehman et al (17) observed in their experiments that,
using a UAS, the renal pelvic pressure (RPP) was <20 cm
H2O when the liquid perfusion pressure was 200 cm
H2O. Maintaining the low pressure state of RPP may help
to reduce the intraoperative absorption of lavage fluid and the
incidence of postoperative fever and bacteremia. The indwelling UAS
provided a convenient access point and served as protection for the
lens barrel, which was beneficial for the extraction of stone
fragments. Sanguedolce et al (18) compared cases with an indwelling UAS
(n=66) and those with a non-indwelling UAS (n=74) and observed that
there were no significant differences in the duration of the
surgery, SFR or the incidence of postoperative complications. In
addition, in a long-term follow-up (average follow-up, 25 months),
the UAS indwelling group had no long-term complications of ureteral
stricture.
An additional factor demonstrated in the present
study was that, following the placement of the flexible
ureteroscope into the renal pelvis, it was necessary to initially
distinguish the renal ureteropelvic junction and set it as an index
point. It was then possible to identify the positions of the renal
upper, middle and lower calyces gradually to locate the stones.
Following the location of the stones, it was necessary for the end
of the flexible ureteroscope to be maintained in a stretched state
during the insertion of the 220 μm holmium laser optical
fiber. Subsequent to the appearance of the fiber in the field of
vision, the optical fiber was retracted into the body by 1–2 mm.
Once the target stones were re-identified, the laser optical fiber
was extended out of the mirror body by 3–4 mm to conduct the
lithotripsy. The laser displacement device of the flexible
ureteroscope kit was selected when necessary to fix the optical
fiber and prevent the fiber from rebound damage during the process.
This method aided the protection of the work channel of the lens
barrel and the lens, and prevented the laser optical fiber from
causing mechanical damage to the kidney.
In the process of lithotripsy, the setting power of
the holmium laser lithotripsy was 0.8–1.0 J/5–10 Hz. It was
possible to adjust the frequency to 15–20 Hz, depending on the
circumstances, in order to enhance the effect. The process started
from the surrounding area and adopted the ‘nibble’ approach. A
‘middle drilling’ method was initially performed to break the
larger pelvic or renal calyceal stones in a sequential fashion. It
was observed that it was necessary to crush the stones into
fragments of <4 mm for easy excretion. The modular flexible
ureteroscope exhibited a unidirectional turning design, which
caused it to be less convenient than the traditional flexible
ureteroscope. In the search for calculi and fragments, rotation and
cooperation of the lens barrel and arms was required. It was
possible to lose the sense of direction in the intracavity as a
result of the process of turning the lens barrel; in such
situations, it was possible to extract the mirror from the body to
reorient it. However, the steering amplitude of the bottom of the
lens was proportional to the degree of the crimping of the
operating handle, since the handle portion of the lens barrel was
made of plastic. Therefore, the handle broke easily when pinched
excessively, thereby increasing the losses in the flexible
ureteroscope kit (19).
Modular flexible ureteroscopy has the advantages of
simple operation, clear visibility and a reliable efficacy. When
the optical fiber is inserted, a bending angle of >180° was
achievable, which was sufficient for the clinical needs. Compared
with the conventional optical or electronic flexible ureteroscope,
as single-use designs, the biggest weakness of this type of
flexible ureteroscope is the unidirectional turning design, which
results in it only being possible to turn the ureteroscope in one
direction. Rotation and cooperation of the mirror body and the arms
was necessary during surgery. The sense of direction in the
intracavity may be lost when turning the mirror body, and this
prolongs the duration of the surgery and potentially increases the
risk of intraoperative and postoperative complications. Certain
limitations in the mirror dexterity, functionality, directional
grasp and operational handling remain. Moreover, the vulnerability
of the flexible ureteroscope may not be fundamentally reduced.
However, there are numerous advantages with the clinical
application of the modular flexible ureteroscope. The core
components (such as the optical imaging fiber) are split-type,
well-protected and supported out of the box, while parts that
become worn (such as the mirror body) may be replaced individually,
which greatly reduces the costs, since there is no requirement to
pay for equipment repair and maintenance. The outer casing of the
flexible ureteroscope is replaceable at a low price and the
components are disposable. This avoids the risk of cross-infection
and enables the flexible ureteroscope to be used in successive
procedures (20,21). Modular flexible ureteroscopy is
applicable in cases with large upper urinary tract calculi, for
surgeries with a long duration and for cases with large losses of
lenses. This is likely to facilitate the popularization and
application of flexible ureteroscope technology.
However, due to the limited number of cases involved
in the present study, the use of the PolyScope endoscope system
requires further study, for example, in studies concerning the use
of flexible ureteroscopes for the treatment of renal calyceal
calculi or renal calculi with a diameter >2 cm, and regarding
the combined use of a flexible ureteroscope with a percutaneous
nephroscope for the treatment of certain complex renal calculi.
References
|
1.
|
Bader MJ, Gratzke C, Walther S, et al: The
PolyScope: a modular design, semidisposable flexible
ureterorenoscope system. J Endourol. 24:1061–1066. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Moe OW: Kidney stones: pathophysiology and
medical management. Lancet. 367:333–344. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Dasgupta P, Cynk MS, Bultitude MF, Tiptaft
RC and Glass JM: Flexible ureterorenoscopy: prospective analysis of
the Guy’s experience. Ann R Coll Surg Engl. 86:367–370. 2004.
|
|
4.
|
Chung BI, Aron M, Hegarty NJ and Desai MM:
Ureteroscopie versus percutaneous treatment for medium-size (1–2
cm) renal calculi. J Endourol. 22:343–346. 2008.PubMed/NCBI
|
|
5.
|
Weizer AZ, Springhart WP, Ekeruo WO, et
al: Ureteroscopic management of renal calculi in anomalous kidneys.
Urology. 65:265–269. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Breda A, Ogunyemi O, Leppert JT and
Schulam PG: Flexible ureteroscopy and laser lithotripsy for
multiple unilateral intrarenal stones. Eur Urol. 55:1190–1196.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Cannon GM, Smaldone MC, Wu HY, et al:
Ureteroscopic management of low pole stones in a pediatric
population. J Endourol. 21:1179–1182. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Grasso M, Conlin M and Bagley D:
Retrograde ureteropyeloscopic treatment of 2 cm. or greater upper
urinary tract and minor Staghorn calculi. J Urol. 160:346–351.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Mariani AJ: Combined electrohydraulic and
holmium: YAG laser ureteroscopic nephrolithotripsy of large
(greater than 4 cm) renal calculi. J Urol. 177:168–173. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Turna B, Stein RJ, Smaldone MC, et al:
Safety and efficacy of flexible ureterorenoscopy and holmium: YAG
lithotripsy for intrarenal stones in anticoagulated cases. J Urol.
179:1415–1419. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Hyams ES and Shah O: Percutaneous
nephrostolithotomy versus flexible ureteroscopy/holmium laser
lithotripsy: cost and outcome analysis. J Urol. 182:1012–1017.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Budia A, Trassierra M, Bahilo P, et al:
Efficacy and satisfaction of two minimally invasive techniques for
the treatment of proximal ureteral lithiasis: a prospective and
comparative study. Eur Urol Suppl. 8:2902009. View Article : Google Scholar
|
|
13.
|
Giusti G, Piccinelli A, Maugeri O, et al:
(2009) Retrograde intrarenal surgery (RIRS) in the treatment of
renal calculi: is it a new frontier? Eur Urol Suppl. 8:2902009.
View Article : Google Scholar
|
|
14.
|
Canales BK, Gleason JM, Hicks N and Monga
M: Independent analysis of Olympus flexible ureteroscope repairs.
Urology. 70:11–15. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Afane JS, Olweny EO, Bertcowsky E, et al:
Flexible ureteroscopes: a single center evaluation of the
durability and function of the new endoscopes smaller than 9Fr. J
Urol. 164:1164–1168. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Paffen ML, Keizer JG, de Winter GV, Arends
AJ and Hendrikx AJ: A comparison of the physical properties of four
new generation flexible ureteroscopes: (de) flection, flow
properties, torsion stiffness, and optical characteristics. J
Endourol. 22:2227–2234. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Rehman J, Monga M, Landman J, et al:
Characterization of intra-pelvic pressure during uroteropyeloscopy
with ureteral access sheaths. Urology. 61:713–718. 2003. View Article : Google Scholar
|
|
18.
|
Sanguedolce F, Cracco C, Grande S, et al:
International cooperation in endourology: Ureteral access sheath
utility during flexible ureteroscopy for lower pole kidney stones.
Eur Urol Suppl. 10:4712011. View Article : Google Scholar
|
|
19.
|
Huang YT, Gu SP, Jiao Y and Qi J: Clinical
effectiveness of modular flexible ureteroscope combined with
Holmium laser for treatment of upper urinary calculi: a repot of 33
cases. Academic Journal of Second Military Medical University.
10:1108–1112. 2011. View Article : Google Scholar
|
|
20.
|
Papatsoris AG, Kachrilas S, Howairis M,
Masood J and Buchholz N: Novel technologies in flexible
ureterorenoscopy. Arab J Urol. 9:41–46. 2011.
|
|
21.
|
Giusti G, Taverna G, Zandegiacomo S, et
al: Polyscope™, the first disposable flexible ureteroscope: a
breakthrough in flexible endoscopy. Eur Urol Suppl. 10:3512011.
|