Introduction
Avascular necrosis of the femoral head (ANFH) is
caused by disruption of the blood supply to the bone, followed by
hip dysfunction (1). Femoral head
ischemia results in the death of marrow and osteocytes and the
necrotic segment subsequently collapses (2). X-ray images of ANFH patients in their
early stages usually appear normal. However, in the later stages,
the images often appear increasingly radio-opaque. The necrotic
bones themselves do not demonstrate increases in radio-graphic
opacity, since dead bones do not undergo the bone resorption
usually performed by living osteoclasts. However, the detailed
mechanism for the pathogenesis of non-traumatic ANFH in young
patients is unclear. The common causes of ANFH include short-term
use of a large quantity of steroids and excessive drinking. Certain
diseases may also result in ANFH, such as systemic lupus
erythematous (3),
hemoglobin-opathies (4,5), Legg-Calvé-Perthes disease, Gaucher’s
disease, dysbarism, HIV, hyperlipidemia, pancreatitis and gout
(6,7). Exposure to radiation or cytotoxic
agents may also result in ANFH (8,9).
However, ANFH caused by heroin injection is rarely reported. In the
current study, we report a rare case of ANFH caused by the
bilateral injection of heroin into the femoral vein.
Case report
A 38-year-old male patient presented with bilateral
hip pain that had been occurring for five months. The patient had
no history of smoking or excessive drinking. Prior written and
informed consent were obtained from the patient and the study was
approved by the ethics review board of The Second Xiangya Hospital,
Central South University, (Changsha, China). The patient had smoked
heroin for 13 years and had bilaterally injected heroin into the
femoral vein for two years. Physical examination indicated a 160°
flexion deformity at the bilateral hip joints and point tenderness
in the bilateral inguinal midpoint, but no significant swelling or
skin pigmentation. Routine blood test results of liver and kidney
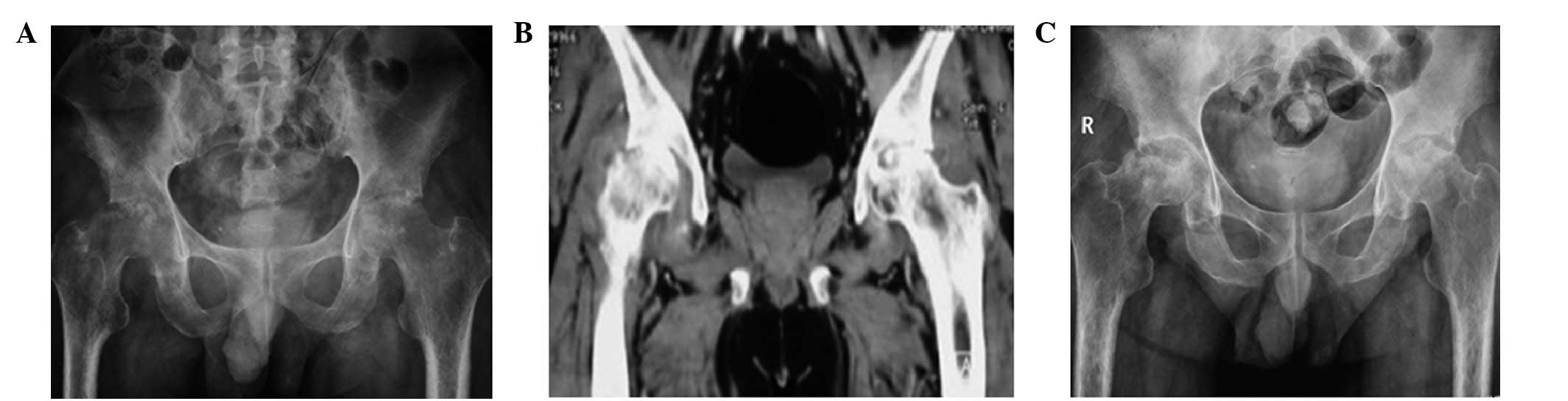
electrolytes were normal. Pelvic X-ray examination showed ischemic
necrosis of the bilateral femoral head, subluxation of the right
hip and osteoporosis of the pelvis and bilateral femurs (Fig. 1A). A computed tomography (CT) scan
of the hip joint indicated ischemic necrosis of the bilateral
femoral head, detectible effusion in the right hip joint and soft
tissue swelling in the bilateral hip (Fig. 1B). Vascular color Doppler
ultrasound revealed double lower limb phlebitis and disseminated
thrombosis. The single-photon emission computed tomography (SPECT)
results indicated that the metabolism of the bilateral hip joint
was active. The electrocardiogram (ECG) and chest X-ray results
were normal.
The patient was treated with Aescuven®
forte (Cesra Arzneimittel GmbH & Co. KG, Baden-Baden, German)
300 mg orally, twice a day, alfacalcidol (Chemvon Biotechnology
Co., Ltd., Shanghai, China) 0.5 μg orally, once a day, and
one D-Cal® tablet (300 mg of Calcium and 100 IU of
Vitamin D3; A&Z Pharmaceutical Inc., New York, NY, USA) orally,
twice a day. The patient stopped injecting heroin during the
treatment. Following six months of treatment, the bilateral hip
pain of the patient was reduced. Physical examination indicated a
reduction in bilateral inguinal tenderness compared with that
exhibited six months previously. The self-movement of the hip had
also improved and the hip was now capable of bending from 180 to
140°. However, the bilateral hip extension, adduction, abduction,
rotation and other functions remained limited. The blood
sedimentation, C-reactive protein level and blood coagulation
function returned to normal levels. An X-ray of the pelvis revealed
that the bilateral femoral head of the patient had collapsed
(Fig. 1C). Vascular color Doppler
ultrasound revealed thromboses in the veins in the patient’s lower
limbs.
Discussion
ANFH caused by the intravenous injection of heroin
is rare, but there are many cases of thrombophlebitis resulting
from the intravenous injection of heroin (10,11).
Pieper and Templin observed that chronic venous insufficiency is a
common symptom in patients who have injected drugs (12). The femoral intravenous injection of
heroin promotes platelet adhesion and fibrin deposition, leading to
venous thrombosis (6,7,13).
Venous thrombosis leads to increased intraosseus venous pressure
and reduced arterial flow, which results in hypoxic bone death
(6,13). The inflammation and thrombosis of
the venous system of the hip due to the long-term intravenous
injection of heroin demonstrates a marked correlation with ANFH and
the destruction of the surrounding bone (14,15).
Our results suggest that the long-term injection of heroin into the
femoral vein of the patient leads to increased blood viscosity,
phlebitis and disseminated thrombosis, which inhibits the blood
circulation to the femoral head, leading to ischemic necrosis of
the femoral head (17–19).
The efficacy of drug treatment for ANFH is usually
unsatisfactory. In the current case, following admission, the
patient received therapy to improve the blood circulation to the
femoral head and to facilitate the formation of new bone. As the
blood supply to the ischemic femoral head improved, the pain
decreased. However, the formation of new bone is a slow process.
Furthermore, the patient did not carefully follow the
recommendations of the doctor and performed weight-bearing
exercises, which led to the further collapse of the femoral
head.
References
|
1.
|
Claffey TJ: Avascular necrosis of the
femoral head. An anatomical study. J Bone Joint Surg Br.
42-B:802–809. 1960.PubMed/NCBI
|
|
2.
|
Hasan SS and Romeo AA: Nontraumatic
osteonecrosis of the humeral head. J Shoulder Elbow Surg.
11:281–298. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Abu-Shakra M, Buskila D and Shoenfeld Y:
Osteonecrosis in patients with SLE. Clin Rev Allergy Immunol.
25:13–24. 2003. View Article : Google Scholar
|
|
4.
|
Akinyoola AL, Adediran IA, Asaleye CM and
Bolarinwa AR: Risk factors for osteonecrosis of the femoral head in
patients with sickle cell disease. Int Orthop. 33:923–926. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Mukisi MM, Bashoun K and Burny F:
Sickle-cell hip necrosis and intraosseous pressure. Orthop
Traumatol Surg Res. 95:134–138. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Seamon J, Keller T, Saleh J and Cui Q: The
pathogenesis of nontraumatic osteonecrosis. Arthritis.
2012:6017632012. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Glueck CJ, Freiberg RA, Sieve L and Wang
P: Enoxaparin prevents progression of stages I and II osteonecrosis
of the hip. Clin Orthop Relat Res. 435:164–170. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Abdulkareem IH: Radiation-induced femoral
head necrosis. Niger J Clin Pract. 16:123–126. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Hancock BW, Huck P and Ross B: Avascular
necrosis of the femoral head in patients receiving intermittent
cytotoxic and corticosteroid therapy for Hodgkin’s disease.
Postgrad Med J. 54:545–546. 1978.PubMed/NCBI
|
|
10.
|
Gillis K, Seenan JP, Cahill A and Tyers A:
An unusual infection in an injecting drug user. Scott Med J.
56:592011. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Ghosheh FR and Kathuria SS: Intraorbital
heroin injection resulting in orbital cellulitis and superior
ophthalmic vein thrombosis. Ophthal Plast Reconstr Surg.
22:473–475. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Pieper B and Templin T: Chronic venous
insufficiency in persons with a history of injection drug use. Res
Nurs Health. 24:423–432. 2001. View
Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Manekeller S, Tolba RH, Schroeder S, et
al: Analysis of vascular complications in intra-venous drug addicts
after puncture of femoral vessels. Zentralbl Chir. 129:21–28.
2004.(In German).
|
|
14.
|
Raso AM, Visentin I, Zan S, et al:
Vascular pathology of surgical interest in drug addicts. Minerva
Cardioangiol. 48:287–296. 2000.(In Italian).
|
|
15.
|
Mackenzie AR, Laing RB, Douglas JG,
Greaves M and Smith CC: High prevalence of iliofemoral venous
thrombosis with severe groin infection among injecting drug users
in North East Scotland: successful use of low molecular weight
heparin with antibiotics. Postgrad Med J. 76:561–565. 2000.
View Article : Google Scholar
|
|
16.
|
Jensenius M, Holm B, Calisch TE, Haugen K
and Sandset PM: Deep venous thrombosis in intravenous drug addicts.
Tidsskr Nor Laegeforen. 116:2556–2558. 1996.(In Norwegian).
|
|
17.
|
Trisolini SM, Capria S, Cafolla A, et al:
Inherited thrombophilia in patients with thrombotic
thrombocytopenic purpura. Thromb Res. 124:512–513. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Mont MA, Ulrich SD and Seyler TM: Role of
thrombotic and fibrinolytic alterations in the pathogenesis and
treatment of osteonecrosis. J Rheumatol. 34:466–468.
2007.PubMed/NCBI
|
|
19.
|
Glueck CJ, Freiberg RA and Wang P:
Heritable thrombophiliahypofibrinolysis and osteonecrosis of the
femoral head. Clin Orthop Relat Res. 466:1034–1040. 2008.
View Article : Google Scholar : PubMed/NCBI
|