Introduction
Asthma is a chronic inflammatory airway disease that
is associated with airway remodeling and airway hyperresponsiveness
(AHR). Airway remodeling is characterized by the increased
deposition of collagen (fibrosis) in the subepithelial basement
membrane region and submucosal layers, smooth muscle hypertrophy
and hyperplasia, fibroblast hyperplasia, epithelial metaplasia and
goblet cell proliferation (1). The
poor response to treatment observed in patients with refractory
asthma may be a consequence of ongoing airway remodeling that
results in fixed airway obstruction (2). Regardless of the advances in
understanding the inflammatory and immunological features of
asthma, the molecular mechanisms underlying the remodeling changes
associated with chronic asthma have not been fully determined.
Nerve growth factor (NGF) is a member of the
neurotrophin family of proteins that regulate neuronal development,
maintenance and recovery from injury. However, NGF has been
implicated in allergic inflammation. High levels of NGF have been
detected in the bronchoalveolar lavage fluids (BALF) and serum from
asthmatic patients, suggesting that NGF is regulated in the airways
and that NGF expression levels are associated with severity of the
allergic disease (3,4).
A previous study identified that NGF results in the
differentiation of human B cells to plasma cells, modulates
chemotaxis and mediates their release by allergic and inflammatory
cells. Moreover, NGF enhances chemotaxis and superoxide production
by neurotrophils and primes histamine release by human basophils
(5).
In addition to neurons and inflammatory cells, NGF
affects the contraction, migration, differentiation and
proliferation of airway structural cells (6,7). NGF
is also synthesized in airway structural cells, such as epithelial
cells, pulmonary fibroblasts and smooth muscle cells (8). Several studies have suggested that
structural cells may be a target of NGF action in the airways. NGF
stimulates the in vitro contraction and migration of human
pulmonary fibroblasts and their differentiation into
myofibroblasts, which induces the proliferation of airway smooth
muscle cells through activation of its TrkA receptor and causes
matrix metalloproteinase-9 (MMP-9) expression in vascular smooth
muscle cells (9,10). These events represent an important
step in the airway remodeling process and links NGF to the
remodeling mechanism. Therefore, we hypothesized that NGF levels
are strongly upregulated and participate in airway remodeling
mechanisms. To explore the mechanisms involved in NGF-induced
airway remodeling in the airways, we established a rat model of
chronic allergic airway inflammation in which the pathological
processes of airway remodeling may be demonstrated.
Materials and methods
Animals
A total of 32 specific pathogen-free normal female
Wistar rats (weight, 120–140 g) were obtained from the Laboratory
Animal Research Center in Shengjing Hospital of China Medical
University (Shenyang, China). Rats were maintained in a 12 h
light:dark cycle with access to food and water ad libitum.
Initially, the rats were randomly divided into four groups:
control, ovalbumin (OVA), NGF and anti-NGF (n=8 per group). All
animal experiments were performed in accordance with the National
Institute of Health Guide for the Care and Use of Laboratory
Animals (8th Edition, 2012). The animal-use protocol has been
reviewed and approved by the Institutional Animal Care and Use
Committee of the Shengjing Hospital of China Medical University
(Shenyang, China).
OVA sensitization
Sensitization and challenge protocols were performed
according to the methods of Li and Shang (11) and Vanacker et al (12) with certain modifications as
described below. On days 0 and 7, all rats with the exception of
those in the control group were actively sensitized with an
intraperitoneal (i.p) injection of 1 mg OVA (Grade V; Sigma, St.
Louis, MO, USA) and 200 μg aluminum hydroxide (Sigma) in 0.5
ml sterile phosphate-buffered saline (PBS). The OVA-sensitized rats
were exposed to 1% aerosolized OVA (1 g OVA in 100 ml sterile PBS
in a nebulizer) for 30 min, every two days from day 14 to day 70.
As neurotrophic factors are highly conserved in different species,
we used exogenous murine NGF (NGF-7S; Alomone Labs, Jerusalem,
Israel) and blocked endogenous NGF activity using 100 μg/ml
goat anti-rat-β-NGF antibody (R&D Systems, Minneapolis, MN,
USA) for our rat model. The NGF and anti-NGF groups were
administered an i.p injection of NGF-7S (80 ng/kg) or anti-NGF
antibody (4 ml/kg) diluted at 1:1,000 in sterile PBS, respectively,
3 h prior to the OVA aerosol challenge. The administration route,
timing and dose of the NGF and anti-NGF treatments were chosen
based on a previous study (13).
The OVA group received 4 ml/kg PBS 3 h prior to the OVA aerosol
challenge. The control group was subjected to the same protocol
using sterile PBS.
Analysis of AHR
Airway reactivity to methacholine (MCH) was assessed
in vivo 24 h following the last OVA challenge as previously
described (14). Rats were
anesthetized with 100 mg/kg pentobarbital sodium (i.p), a tracheal
cannula was inserted via tracheotomy for mechanical ventilation and
a small catheter (22G) was inserted into the external jugular vein
for the administration of MCH (Sigma-Aldrich, Beijing, China). The
rats were then placed in a sealed whole body plethysmograph and
connected to a rodent ventilator (ML-V2; Shanghai Benda
Biotechnology Co., Ltd., Shanghai, China). Ambient air was
administered with a tidal volume of 8 ml/kg and a frequency of 90
strokes per min. Transducers (ML-AMP II; Shanghai Benda
Biotechnology Co.,Ltd.) connected to the ventilatory circuit
provided voltage signals of pressure and flow, which were amplified
and transmitted to the analog/digital card (National Instruments,
Austin, TX, USA) of a microcomputer running the AniRes2005 software
(Beijing Bestlab High-Tech Co., Ltd., Beijing, China), which was
used to calculate the inspiratory and expiratory resistances of the
respiratory system from the digitized pressure and flow signals.
Following stabilization of respiratory parameters (10–15 min) rats
received MCH (dissolved in 0.9% sodium chloride) intravenously at
an initial dose of 0.0625 mg/kg with the dose increasing 2-fold
with each injection up to 1 mg/kg to obtain a response curve of
lung resistance increase over baseline. Injections were
administered at 5-min intervals. The MCH volume was 50 μl,
which was administered over 3–4 sec based on the return of
resistance curves to the pre-MCH level prior to the next MCH
injection. Response was measured as the peak increase above the
baseline immediately following MCH administration.
BAL
Following assessment of airway reactivity, the rats
were bled and sacrificed via anesthetic overdose. BAL was performed
in the left lungs. The left lungs were washed thrice with 1 ml
saline. Lavage fluid was recovered by gentle manual aspiration with
a syringe. The retrieved volume, which averaged 75–80% of the
instilled saline was immediately centrifuged (10 min, 4°C, 1,000 ×
g) and the supernatant was stored at −70°C until the levels of IL-4
and IL-13 were measured. The pellet was kept on ice, washed twice
with saline and resuspended in 1 ml saline. The total number of
leukocytes in the BALF were determined with a Coulter counter
(Coulter Electronics Ltd., Harpenden, UK). A differential cell
count was performed on Cytospin (Thermo Shandon, Inc,, Pittsburgh,
PA, USA) by Wright-Giemsa staining.
ELISA
After measuring airway reactivity, serum was
obtained by lethal cardiac puncture of anesthetized rats and stored
at −70°C for measurement of OVA-specific IgE by ELISA.
Tissue collection
Lung tissues were weighed (total lung weight) and
then separated into individual lobes for hydroxyproline analysis,
histological analysis, western blotting, quantitative polymerase
chain reaction (qPCR) and MMP zymography.
Lung histopathology
The middle lobes of the right lung were fixed in 4%
paraformaldehyde for 18–24 h, embedded in paraffin and then
routinely processed. Serial 5-μm tissue sections were
stained with hematoxylin and eosin (H&E), Masson’s trichrome
and periodic acid-Schiff (PAS) for the assessment of peribronchial
inflammation, collagen particles and goblet cells,
respectively.
Morphometric analysis
A minimum of five bronchi (luminal diameter, 150–350
μm) were analyzed per rat for various parameters using a
Leica image analysis system (Leica, Cambridge, UK). Using a 10-fold
magnification objective, four representative areas were chosen.
Subsequently, with a 40-fold magnification corresponding to one
microscopic field, hyperplasia of the goblet cells in the
epithelial lining was recorded against a score based on the
percentage of goblet cells observed in the epithelial cells. The
length of the epithelial basement membrane of the bronchus of one
area was ≥500 μm. To minimize sampling errors, a 5-point
scoring system (grades 0–4) was adopted: grade 0, no goblet cells;
grade 1, <25% goblet cells; grade 2, 25–50% goblet cells; grade
3, 50–75% goblet cells; and grade 4, ≥75% goblet cells (15). The mean score of the total
epithelial cells in the four areas of one rat were counted. The
mean score of hyperplasia of the goblet cells was calculated for
7–8 rats.
Masson’s trichrome-stained tissue sections were used
for the assessment of subepithelial fibrosis using the Leica image
analysis system. As described previously, three representative
areas were chosen using a 10-fold magnification objective.
Subsequently, with a 40-fold magnification, epithelial basement
membrane areas of ≥250 μm were selected, and the thickness
of the epithelial layer and fibrotic area (stained in blue), which
were 30 μm beneath the basement membrane of the standardized
sampling points, were measured (16). The mean fibrotic area divided by
the length of the basement membrane were calculated for 7–8
rats.
Hydroxyproline analysis
Total collagen content in the fresh lung samples of
all rats were determined by hydroxyproline assay. The
hydroxyproline content was detected with a commercial
hydroxyproline detection kit (Nanjing Jiancheng Bioengineering
Institute, Nanjing, China) following the manufacturer’s
instructions.
Western blot analysis
Protein homogenates of lung tissue samples were
prepared by rapid homogenization in 10 volumes of lysis buffer (2
mM EDTA, 10 mM EGTA, 0.4% NaF, 20 mM Tris-HCl, 1 mg/ml leupeptin, 1
mg/ml aprotinin and 1 mM Na3VO4 at pH 7.5).
Samples were centrifuged at 12,000 × g for 1 h and the protein
concentration of the soluble material was determined using the
Coomassie Brilliant Blue G250 (Beyotime Institute of Biotechnology,
Jiangsu, China) binding method (17). Proteins (10 μg) from each
sample were loaded onto an 8% sodium dodecyl sulfate-polyacrylamide
gel. Electroblotted proteins were transferred from the gel to
nitro-cellulose membranes, which were incubated with 1:1,000 goat
anti-NGF. The NGF band (140 kD) was visualized using an enhanced
chemiluminescence kit (Santa Cruz Biotechnology, Inc., Santa Cruz,
CA, USA). Integrated density values (IDV) were analyzed using a
computerized image analysis system (Fluor Chen 2.0; Bio-Rad,
Hercules, CA, USA) and normalized to those of β-actin.
qPCR
Rat lung tissues were dissected and stored in TRIzol
reagent (Invitrogen Life Technologies, Carlsbad, CA, USA). The
levels of MMP-9 mRNA were determined using the ABI PRISM 7500
Real-Time PCR system (Applied Biosystems, Foster City, CA, USA).
The RNA was extracted using TRIzol reagent in accordance with the
manufacturer’s instructions. RNA purity was determined and cDNA
synthesis was conducted using a SYBR® PrimeScript™
RT-PCR kit (Takara Biotechnology, (Dalian) Co., Ltd., Dalian,
China). The volume of rat MMP-9 mRNA was determined by qPCR. The
primers for MMP-9 were 5′-CCCACTTACTTTGGAAACG-3′ (forward) and
5′-GAAGATGAATGGAAATACGC-3′ (reverse), and those for GAPDH were
5′-GCAAGTTCAACGGCACA-3′ (forward) and 5′-CATTTGATGTTAGCGGGAT-3′
(reverse) [Takara Biotechnology (Dalian) Co., Ltd]. Gene expression
levels of MMP-9 were analyzed by the
2−ΔΔCT method (18).
Zymography
Total MMPs were extracted from a similar section of
each lung tissue and analyzed by gelatin zymography (Genmed
Scientifics Inc., Arlington, MA, USA) according to the
manufacturer’s instructions. The resulting bands on the zymograph
were analyzed by densitometry using a GS-710 densitometer (Bio-Rad
Laboratories, Richmond, CA, USA) and Quantity-One software
(Bio-Rad). The mean ± standard error density of each MMP was
plotted in a graph and expressed as the relative ratio of the
values in the control group, which were expressed as one.
Statistical analysis
Data are expressed as the mean ± standard error of
the mean for each group. One-way analysis of variance (ANOVA)
followed by the Bonferroni post hoc test was used to compare group
differences, whereas two-way ANOVA was used to assess differences
in airway resistance. P<0.05 was considered to indicate a
statistically significant difference.
Results
Airway resistance measurement
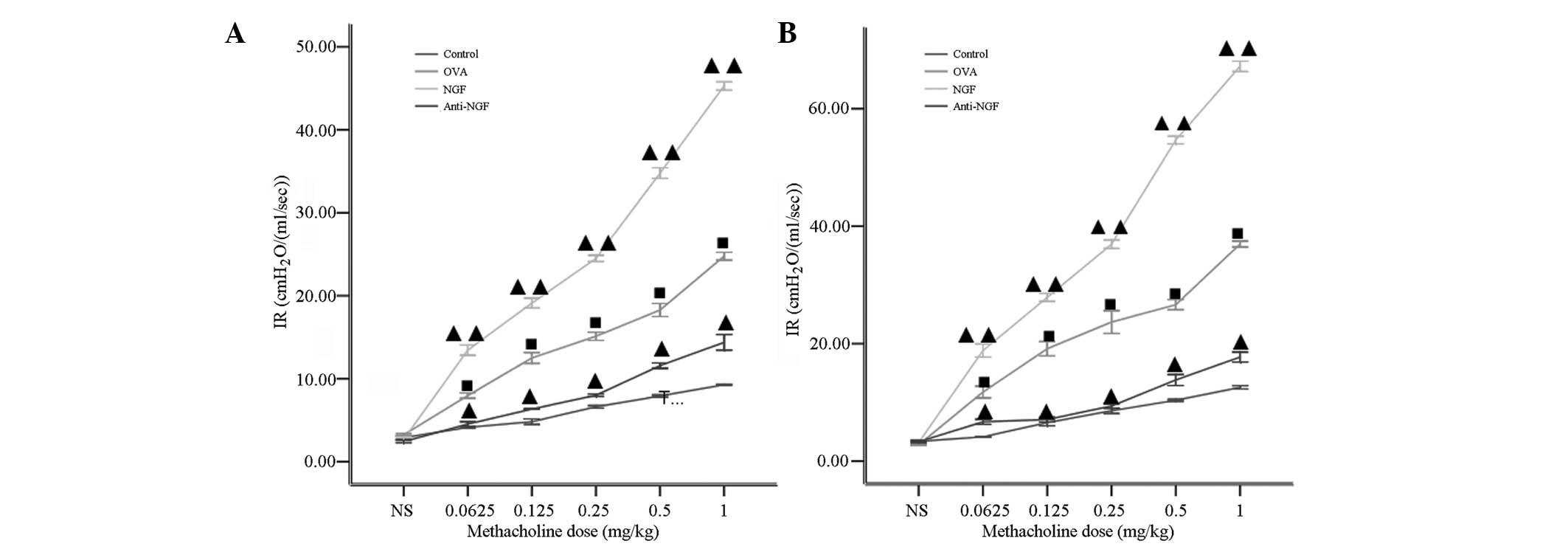
All experimental rats exhibited dose-dependent
augmentation of inspiratory and expiratory resistance in response
to increasing doses of intravenously administered MCH. No
statistically significant differences in baseline inspiratory and
expiratory resistance values among all experimental groups was
observed. The airway response to MCH significantly increased in the
OVA and NGF groups compared with that of the control group
(P<0.01). Treatment of OVA-sensitized rats with anti-NGF prior
to the OVA challenge prevented the increase in airway reactivity,
which was reflected by a shift in the dose-response curves
(Fig. 1) and significantly
decreased reactivity compared with that of the OVA group
(P<0.01).
Airway inflammation
To investigate the function of NGF in
antigen-induced inflammatory infiltration in the airways, we
examined the effects of NGF and anti-NGF antibodies in the
asthmatic rat model. As shown in Table
I, the number of total cells, eosinophils, macrophages,
lymphocytes and neutrophils increased in the BALF of the untreated
OVA-sensitized and NGF-treated rats compared with those in the
PBS-treated rats (controls) (Table
I). By contrast, anti-NGF treatment significantly inhibited the
increase in the number of total leukocytes, eosinophils and
lymphocytes in the BALF following antigen inhalation.
 | Table I.Total white blood cells and cellular
composition in the BALF. |
Table I.
Total white blood cells and cellular
composition in the BALF.
| Group | Total cells
(×106) | Cellular
Composition (%)
|
|---|
| Macrophages | Eosinophils | Neutrophils | Lymphocytes |
|---|
| Control | 3.64±0.20 | 94.06±0.45 | 1.45±0.09 | 1.33±0.48 | 3.52±1.31 |
| OVA | 12.23±0.43a | 57.75±0.63a | 4.58±0.19a | 32.05±0.79a | 5.61±0.85 |
| NGF | 17.18±0.44b | 50.13±0.69b | 5.42±0.15c | 37.75±0.37b | 6.68±0.58a |
| Anti-NGF | 5.43±0.36b | 81.25±0.62b | 2.96±0.23b | 11.37±0.56b | 4.41±0.63 |
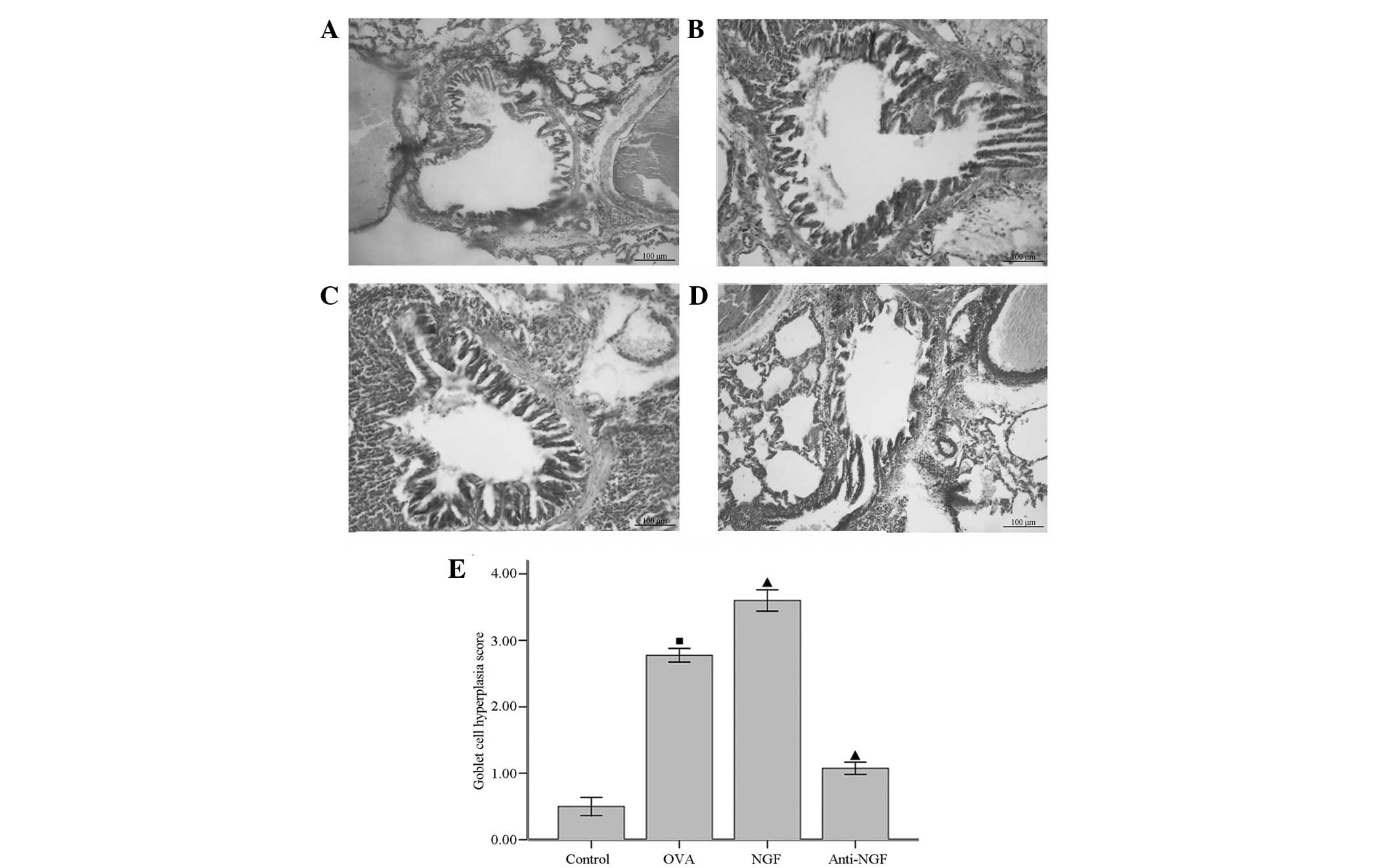
Goblet cell hyperplasia
To evaluate the effects of NGF on antigen-induced
goblet cell hyperplasia in the airway epithelium, which is a
cardinal feature of bronchial asthma, lung sections were stained
with PAS for detection (Fig. 2).
Goblet cell hyperplasia was then quantitatively estimated in terms
of grade as described in Materials and methods (Fig. 2E). As shown in Fig. 2A, histological analyses of lungs
from the PBS-treated rats showed normal lung histology. However,
the number of goblet cells in the epithelium greatly increased
following repeated antigen challenge (Fig. 2B), and goblet cells in the
epithelium showed hypertrophic features. Antigen-induced goblet
cell hyperplasia was greatly increased by NGF administration
(Fig. 2C), but significantly
reduced by anti-NGF treatment (Fig.
2D).
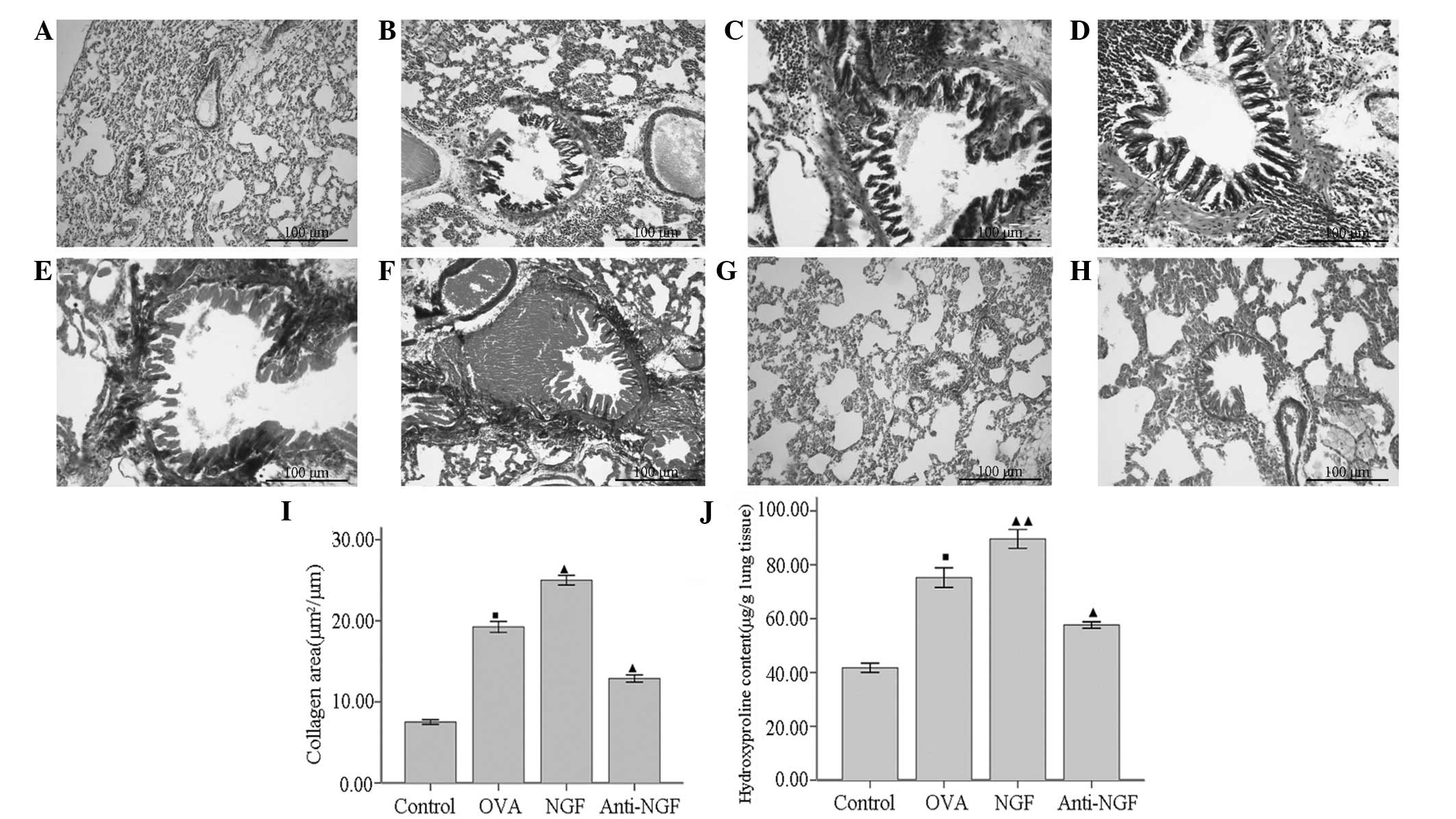
Allergen-induced airway remodeling
To determine whether NGF is involved in the
development of airway remodeling, we evaluated the peribronchial
cellular infiltration, airway smooth muscle thickness and lung
collagen content in all experimental rats. Representative sections
of each group were stained with either H&E (Fig. 3A–D) or Masson’s trichrome (Fig. 3E–H). As shown in Fig. 3A, no inflammation, mucosal edema
and epithelial lesions were observed in the control group. Moderate
inflammation, mucosal edema and epithelial lesions were observed in
the anti-NGF group (Fig. 3B),
whereas sensitization in the OVA group was associated with
predominantly moderate to severe inflammation, mucosal edema and
epithelial lesions (Fig. 3C). In
particular, only NGF-treated rats developed severe inflammation,
mucosal edema and epithelial lesions, which included interstitial
infiltrates and large lymphoid aggregates (Fig. 3D). Peribronchial fibrosis (Fig. 3I) and lung collagen content
(Fig. 3J) were quantitatively
estimated. Exposure to OVA increased the peribronchial
trichrome-stained area and lung collagen levels in the OVA
(Fig. 3E) and NGF groups (Fig. 3F) when compared with those in the
control group (Fig. 3G).
Anti-NGF-treated rats showed reduced peribronchial collagen
staining (Fig. 3H) compared with
that in the OVA-treated rats. Lung collagen levels in the
anti-NGF-treated rats were significantly reduced (57.6±1.19
μg collagen/g lung tissue) compared with those in the
OVA-treated rats (75.23±3.64 μg collagen/g lung tissue)
(P<0.01).
Cytokine response
We analyzed the concentrations of Th2-associated
cytokines (IL-4 and IL-13) in the BALF. As shown in Table II, the IL-4 and IL-13 levels were
higher in the BALF of the untreated OVA-sensitized and NGF-treated
rats compared with those of the PBS-treated rats (controls).
Anti-NGF-treated rats showed reduced levels of IL-4 and IL-13
compared with those of the untreated OVA-sensitized rats.
| Table II.Effects of NGF on the levels of IL-4
and IL-13 in the BALF and serum levels of OVA-specific IgE. |
Table II.
Effects of NGF on the levels of IL-4
and IL-13 in the BALF and serum levels of OVA-specific IgE.
| Group | BALF (pg/ml)
| Serum
(μg/ml) OVA-specific IgE |
|---|
| IL-4 | IL-13 |
|---|
| Control | 21.25±2.78 | 71.50±3.79 | - |
| OVA | 66.00±2.27a | 132.50±4.64a | 11.15±0.43a |
| NGF | 82.50±4.05b | 149.75±3.12b | 14.98±0.73c |
| Anti-NGF | 51.00±3.02b | 90.75±2.32c | 5.63±0.46c |
Serum levels of OVA-specific IgE
To confirm that the presence of the OVA antigen
resulted in immunological sensitization, OVA-specific IgE serum
levels were measured. Serum IgE levels were increased in all
OVA-sensitized groups compared with those of the control group.
However, serum IgE levels were reduced in the anti-NGF group
compared with those of the OVA group (Table II).
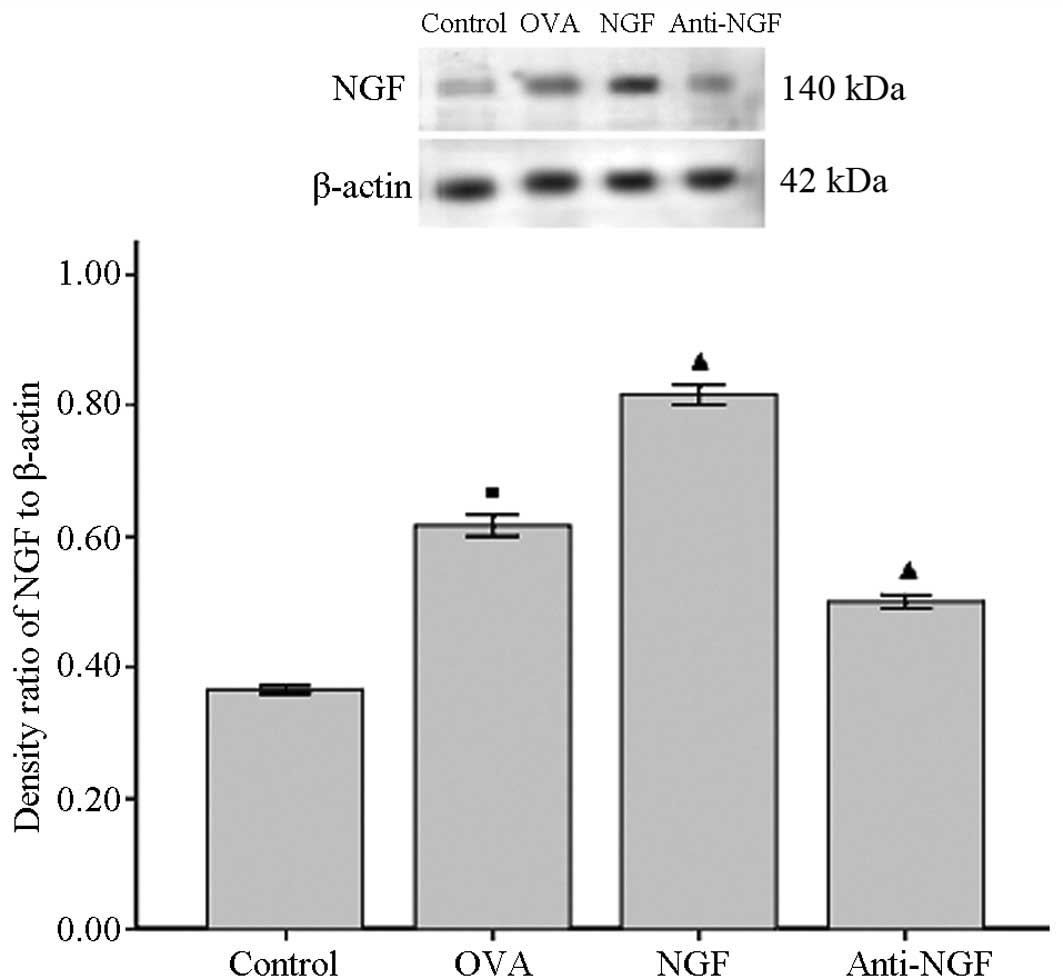
Western blot analysis
NGF protein levels in all groups were detected by
western blotting. In the lung tissues of the control group, NGF was
expressed at low levels, but these levels were markedly increased
in the OVA and NGF groups. However, anti-NGF treatment markedly
decreased the NGF upregulation caused by OVA and NGF (Fig. 4). The mean IDV ratio of NGF to
β-actin was 0.36±0.01 in the control group, 0.62±0.02 in the OVA
group, 0.50±0.02 in the anti-NGF group and 0.81±0.02 in the NGF
group (Fig. 4).
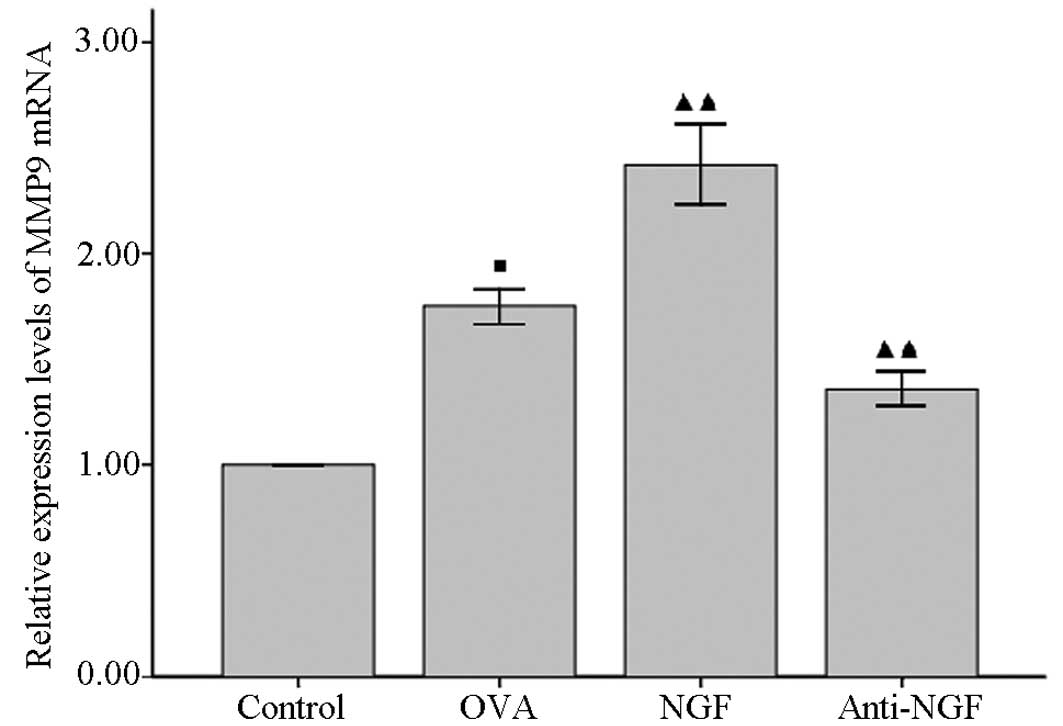
qPCR
qPCR was used to examine the expression levels of
MMP-9 mRNA in the pulmonary tissues of all groups. MMP-9 mRNA
expression levels were significantly higher in the OVA and NGF
groups than in the control group, but anti-NGF treatment
significantly decreased MMP-9 mRNA expression levels in the
OVA-sensitized rats (Fig. 5).
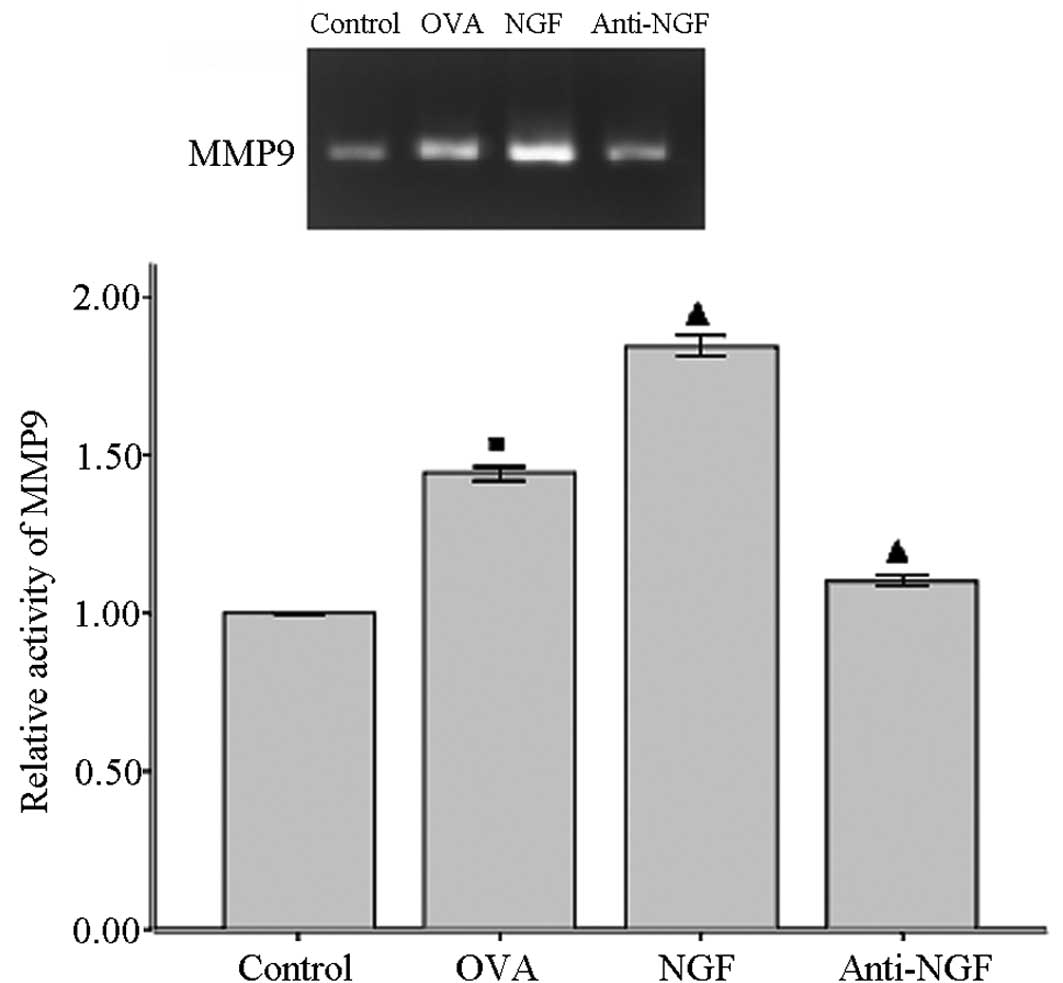
Lung zymography
Gelatin zymography of the lung tissues from the rats
in all experimental groups was used to demonstrate changes in the
activity of MMP-9. Densitometric analysis of the zymographs
demonstrated that MMP-9 activity in the lung tissues of all
OVA-sensitized rats was significantly increased compared with that
of the controls (Fig. 6). By
contrast, a significant reduction in MMP-9 activity in the lung
tissues of the anti-NGF-treated rats compared with that in the
OVA-treated rats was observed.
Discussion
In the present study, we evaluated the effects of
NGF on an experimental rat model of chronic allergic lung
inflammation in rats. Our results showed that NGF exacerbated
allergic inflammation, airway responsiveness and airway remodeling
in sensitized rats, characterized by a significant increase in the
number of inflammatory cells in the BALF and airway walls, AHR and
in the volume proportion of collagen fibers. Moreover, NGF-induced
changes were shown to be mediated by an increase in the release of
IL-4 and IL-13 by inflammatory cells. Notably, anti-NGF treatment
decreased all studied parameters of the OVA-sensitized rats. This
indicates that anti-NGF administration decreased airway
inflammation, remodeling and AHR in OVA-sensitized rats.
The functions of NGF in allergic airway inflammation
have been investigated using NGF transgenic, NGF-treated or
anti-NGF-treated mice. Numerous findings have indicated that NGF
may influence developmental differentiation, chemo-taxis and
mediate the release of inflammatory cells (19,20).
However, the involvement of NGF in antigen-induced airway
eosinophilic inflammation and in the pathogenesis of
allergen-induced airway remodeling have not been fully
investigated. Kerzel et al demonstrated that in a model of
experimental asthma, transgenic mice, which constitutively
overexpressed NGF in the lung epithelial cells, recruited
significantly more eosinophils following allergic sensitization
than the wild-type animals (21).
By contrast, p75NTR-deficient mice exhibited a significant
reduction in eosinophilic infiltration (22) and similar effects were found
following the inactivation of NGF by the intranasal application of
an anti-NGF antibody during allergic sensitization (23). These findings clearly demonstrated
that NGF in the airways may have detrimental effects on asthma.
However, the exogenous administration of NGF or NGF-neutralizing
antibodies did not modify IgE and eosinophil parameters; whereas in
control rats, NGF administration did not induce an increase in IgE
or eosinophils in the BALF and lungs (24).
Therefore, prior to evaluating the effects of NGF,
we first examined whether NGF levels increased following repeated
antigen challenge in our chronic asthma model. The repeated antigen
challenge resulted in increased levels of NGF protein in the lung
tissues and of OVA-specific IgE in the serum compared with the
respective levels in the control rats. As expected, anti-NGF
administration markedly inhibited the increase of NGF protein
levels and serum levels of OVA-specific IgE; whereas NGF treatment
significantly promoted the increase. Mast cells are resident tissue
cells, and in allergic diseases they are critical effector cells as
they are the main contributors to immediate hypersensitivity
reactions when activated through IgE and specific antigens. Mast
cells predominantly depend on NGF for homing, survival and
differentiation. NGF is a chemoattractant for mast cells and acts
as a cofactor together with the stem cell factor to prevent
apoptosis (25). NGF and the
combination of NGF and stem cell factor increase or induce the
expression of typical mast cell markers, such as IgE-receptor type
I, chymase or mast-cell specific tryptase.
In allergic inflammatory responses, a number of
cytokines and chemokines are released from various cell types. In
bronchial asthma, CD4+ T cells produce and secrete a
large quantity of Th2 cytokines, such as IL-4, IL-5 and IL-13, and
these cytokines promote allergic airway inflammation (26). In the present study, the
administration of NGF significantly exacerbated airway eosinophilic
inflammation, increased the total inflammatory cell number and the
production of IL-13 and IL-4 in the BALF, as well as goblet cell
hyperplasia in the epithelium whereas treatment with anti-NGF
clearly reduced these factors. The observed changes in pulmonary
inflammation and mucus production possibly resulted from
concomitant changes in the levels of Th2-type cytokines, IL-4 and
IL-13 in the BALF (27). Moreover,
administration of NGF aggravated AHR. The precise mechanisms
underlying allergen-induced AHR remain unclear; however, recent
studies using IL-4-gene-knockout mice and IL-13-gene-knockout mice
have demonstrated that AHR is dependent on Th2 cytokines (28,29).
In conclusion, these observations indicate that Th2 cytokines are
important in the development of allergen-induced AHR. Therefore,
increased Th2 cytokine production in the BALF may subsequently
result in aggravated AHR, which was observed in NGF treatment.
Notably, regardless of exacerbated lung inflammation
and AHR, the administration of NGF further increased collagen
deposition in the airway walls. We suggest that these changes may
have been mediated by an increase in MMP-9 activity in the lung
tissues, which was observed in our animals following NGF
administration. MMP-9 belongs to a family of extracellular
proteases that are responsible for the degradation of the
extracellular matrix during tissue remodeling (26). Levels of MMP-9 (gelatinase B) are
significantly increased in the BALF of OVA-sensitized BALB/c mice,
blood and sputum of patients with allergic asthma (30,31).
Studies of MMP-9-deficient mice demonstrated that when challenged
with an allergen, mice showed relatively less peribronchial
fibrosis and total lung collagen compared with that of the
wild-type mice (32). In terms of
the potential effects of MMP-9 on airway inflammation in asthma,
in vitro studies have shown that MMP-9 may be important in
mediating the migration of eosinophils across the basement membrane
of blood vessels (33). Moreover,
in vitro studies have identified that NGF may induce MMP-9
expression in vascular smooth muscle cells and human bronchial
smooth muscle cells, and induce the proliferation of airway smooth
muscle cells through activation of its TrkA receptor (9,34).
We speculate that the increase in collagen deposition in the airway
walls and the enhanced smooth muscle thickness induced by NGF are
possibly mediated by the increased expression of MMP-9.
In conclusion, our results suggest that NGF
exacerbated the effects of OVA sensitization (airway inflammation,
remodeling and hyperresponsiveness) via Th2 and MMP-9 pathways.
However, the extent to which the results obtained in our rat model
of allergic inflammation may be transposed to patients with asthma
remain unclear.
NGF has been used as a therapeutic agent for
Alzheimer’s disease, peripheral neuropathies, amyotrophic lateral
sclerosis and human corneal and skin ulcers (35,36).
No deleterious effects of NGF have been confirmed. However, the
exacerbation of allergic chronic lung inflammation observed in the
present study suggests that NGF treatment may exhibit deleterious
effects in individuals with allergic conditions, such as asthma,
whereas anti-NGF treatment is potentially beneficial in the
prevention and treatment of asthma.
Acknowledgements
This study was supported by a grant
from the Educational Department of Liaoning Province (grant no.
20060953).
References
|
1.
|
Wilson JW and Li X: The measurement of
reticular basement membrane and submucosal collagen in the
asthmatic airway. Clin Exp Allergy. 27:363–371. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Hamid Q: Airway remodeling in asthma. J
Allergy Clin Immunol. 111:1420–1421. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Kassel O, de Blay F, Duvernelle C, et al:
Local increase in the number of mast cells and expression of nerve
growth factor in the bronchus of asthmatic patients after repeated
inhalation of allergen at low-dose. Clin Exp Allergy. 31:1432–1440.
2001. View Article : Google Scholar
|
|
4.
|
Olgart Höglund C, de Blay F, Oster JP, et
al: Nerve growth factor levels and localisation in human asthmatic
bronchi. Eur Respir J. 20:1110–1116. 2002.PubMed/NCBI
|
|
5.
|
Raap U, Fokkens W, Bruder M, Hoogsteden H,
Kapp A and Braunstahl GJ: Modulation of neurotrophin and
neurotrophin receptor expression in nasal mucosa after nasal
allergen provocation in allergic rhinitis. Allergy. 63:468–475.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Freund V and Frossard N: Expression of
nerve growth factor in the airways and its possible role in asthma.
Prog Brain Res. 146:335–346. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Frossard N, Freund V and Advenier C: Nerve
growth factor and its receptors in asthma and inflammation. Eur J
Pharmacol. 500:453–465. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Kemi C, Grunewald J, Eklund A and Höglund
CO: Differential regulation of neurotrophin expression in human
bronchial smooth muscle cells. Respir Res. 7:182006. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Freund-Michel V, Bertrand C and Frossard
N: TrkA signalling pathways in human airway smooth muscle cell
proliferation. Cell Signal. 18:621–627. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Khan KM, Falcone DJ and Kraemer R: Nerve
growth factor activation of Erk-1 and Erk-2 induces matrix
metalloproteinase-9 expression in vascular smooth muscle cells. J
Biol Chem. 277:2353–2359. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Li M and Shang YX: Inhaled corticosteroids
inhibit substance P receptor expression in asthmatic rat airway
smooth muscle cells. BMC Pulm Med. 12:792012. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Vanacker NJ, Palmans E, Kips JC and
Pauwels RA: Fluticasone inhibits but does not reverse
allergen-induced structural airway changes. Am J Respir Crit Care
Med. 163:674–679. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
de Vries A, Dessing MC, Engels F, Henricks
PA and Nijkamp FP: Nerve growth factor induces a neurokinin-1
receptor-mediated airway hyperresponsiveness in guinea pigs. Am J
Respir Crit Care Med. 159:1541–1544. 1999.PubMed/NCBI
|
|
14.
|
Zhu MM, Zhou QH, Zhu MH, et al: Effects of
nebulized ketamine on allergen-induced airway hyperresponsiveness
and inflammation in actively sensitized Brown-Norway rats. J
Inflamm (Lond). 4:102007. View Article : Google Scholar
|
|
15.
|
Tanaka H, Masuda T, Tokuoka S, et al: The
effect of allergen-induced airway inflammation on airway remodeling
in a murine model of allergic asthma. Inflamm Res. 50:616–624.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Wakahara K, Tanaka H, Takahashi G, et al:
Repeated instillations of Dermatophagoides farinae into the
airways can induce Th2-dependent airway hyperresponsiveness,
eosinophilia and remodeling in mice: effect of intratracheal
treatment of fluticasone propionate. Eur J Pharmacol. 578:87–96.
2008.
|
|
17.
|
Sedmak JJ and Grossberg SE: A rapid,
sensitive, and versatile assay for protein using Coomassie
brilliant blue G250. Anal Biochem. 79:544–552. 1977. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2-ΔΔCT Method. Methods. 25:402–408. 2001.
|
|
19.
|
Abram M, Wegmann M, Fokuhl V, et al: Nerve
growth factor and neurotrophin-3 mediate survival of pulmonary
plasma cells during the allergic airway inflammation. J Immunol.
182:4705–4712. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Sawada J, Itakura A, Tanaka A, et al:
Nerve growth factor functions as a chemoattractant for mast cells
through both mitogen-activated protein kinase and
phosphatidylinositol 3-kinase signaling pathways. Blood.
95:2052–2058. 2000.PubMed/NCBI
|
|
21.
|
Päth G, Braun A, Meents N, et al:
Augmentation of allergic early-phase reaction by nerve growth
factor. Am J Respir Crit Care Med. 166:818–826. 2002.PubMed/NCBI
|
|
22.
|
Kerzel S, Päth G, Nockher WA, et al:
Pan-neurotrophin receptor p75 contributes to neuronal
hyperreactivity and airway inflammation in a murine model of
experimental asthma. Am J Respir Cell Mol Biol. 28:170–178. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Shi Y, Jin Y, Guo W, Chen L, Liu C and Lv
X: Blockage of nerve growth factor modulates T cell responses and
inhibits allergic inflammation in a mouse model of asthma. Inflamm
Res. 61:1369–1378. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
Stampachiacchiere B, Aloe L, Micera A and
Bonini S: Allergic bronchial airway inflammation in nerve growth
factor (NGF)-deprived rats: evidence suggesting a
neuroimmunomodulatory role of NGF. Exp Lung Res. 32:305–320. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
25.
|
Kanbe N, Kurosawa M, Miyachi Y, Kanbe M,
Saitoh H and Matsuda H: Nerve growth factor prevents apoptosis of
cord blood-derived human cultured mast cells synergistically with
stem cell factor. Clin Exp Allergy. 30:1113–1120. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
26.
|
Atkinson JJ and Senior RM: Matrix
metalloproteinase-9 in lung remodeling. Am J Respir Cell Mol Biol.
28:12–24. 2003. View Article : Google Scholar
|
|
27.
|
Temann UA, Prasad B, Gallup MW, et al: A
novel role for murine IL-4 in vivo: induction of MUC5AC gene
expression and mucin hypersecretion. Am J Respir Cell Mol Biol.
16:471–478. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
28.
|
Kim HK, Lee CH, Kim JM, Ayush O, Im SY and
Lee HK: Biphasic late airway hyperresponsiveness in a murine model
of asthma. Int Arch Allergy Immunol. 160:173–183. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
29.
|
Komai M, Tanaka H, Masuda T, et al: Role
of Th2 responses in the development of allergen-induced airway
remodelling in a murine model of allergic asthma. Br J Pharmacol.
138:912–920. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
30.
|
Hsu CH, Hu CM, Lu KH, et al: Effect of
selective cysteinyl leukotriene receptor antagonists on airway
inflammation and matrix metalloproteinase expression in a mouse
asthma model. Pediatr Neonatol. 53:235–244. 2012. View Article : Google Scholar
|
|
31.
|
Lee YC, Lee HB, Rhee YK and Song CH: The
involvement of matrix metalloproteinase-9 in airway inflammation of
patients with acute asthma. Clin Exp Allergy. 31:1623–1630. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
32.
|
Lim DH, Cho JY, Miller M, McElwain K,
McElwain S and Broide DH: Reduced peribronchial fibrosis in
allergen-challenged MMP-9-deficient mice. Am J Physiol Lung Cell
Mol Physiol. 291:L265–L271. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
33.
|
Mori S, Pawankar R, Ozu C, Nonaka M, Yagi
T and Okubo K: Expression and roles of MMP-2, MMP-9, MMP-13,
TIMP-1, and TIMP-2 in allergic nasal mucosa. Allergy Asthma Immunol
Res. 4:231–239. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
34.
|
Dagnell C, Kemi C, Klominek J, et al:
Effects of neurotrophins on human bronchial smooth muscle cell
migration and matrix metalloproteinase-9 secretion. Transl Res.
150:303–310. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
35.
|
Allen SJ, Watson JJ and Dawbarn D: The
neurotrophins and their role in Alzheimer’s disease. Curr
Neuropharmacol. 9:559–573. 2011.
|
|
36.
|
Aloe L, Rocco ML, Bianchi P and Manni L:
Nerve growth factor: from the early discoveries to the potential
clinical use. J Transl Med. 10:2392012. View Article : Google Scholar : PubMed/NCBI
|