Introduction
Blue rubber bleb nevus syndrome (BRBNS) is a rare
disorder characterized by multiple recurrent vascular
malformations, including hemangioma, which are primarily located on
the skin and gastrointestinal (GI) tract (1). Other organ systems that may be
affected include the central nervous system (2), liver, kidney, bladder, heart, thyroid
and spleen. However, these are affected less often than the GI
tract (3). Although cases that
appear to have an autosomal dominant transmission have been
reported (4,5), the majority of cases are sporadic
with no family history of the disorder (6,7).
Cutaneous angiomas are blue or purple, soft, rubbery, sessile,
‘nipple-like’ nodules with wrinkled and hyperhydrotic surfaces.
However, they may also lie deep in the skin and appear as bluish
macules (8).
A variety of therapeutic strategies have been
proposed for the management of GI bleeding in BRBNS, including
anti-angiogenic agents and surgical resection (9–18).
However, no particular method has been demonstrated to be reliably
effective in reducing bleeding or controlling blood loss
permanently. Furthermore, surgical resection has been condemned as
overly aggressive and unhelpful due to the theory that lesions may
recur after removal (16).
Endoscopy is considered a less invasive alternative for the
treatment of BRBNS.
Case report
The informed consent was obtained from the patient.
In March 2012, a 22-year-old female with iron-deficiency anemia,
secondary to recurrent episodes of melena, presented as an
outpatient to the Department of Gastroenterology at the Second
Affiliated Hospital of Nanjing Medical University (Nanjing, China).
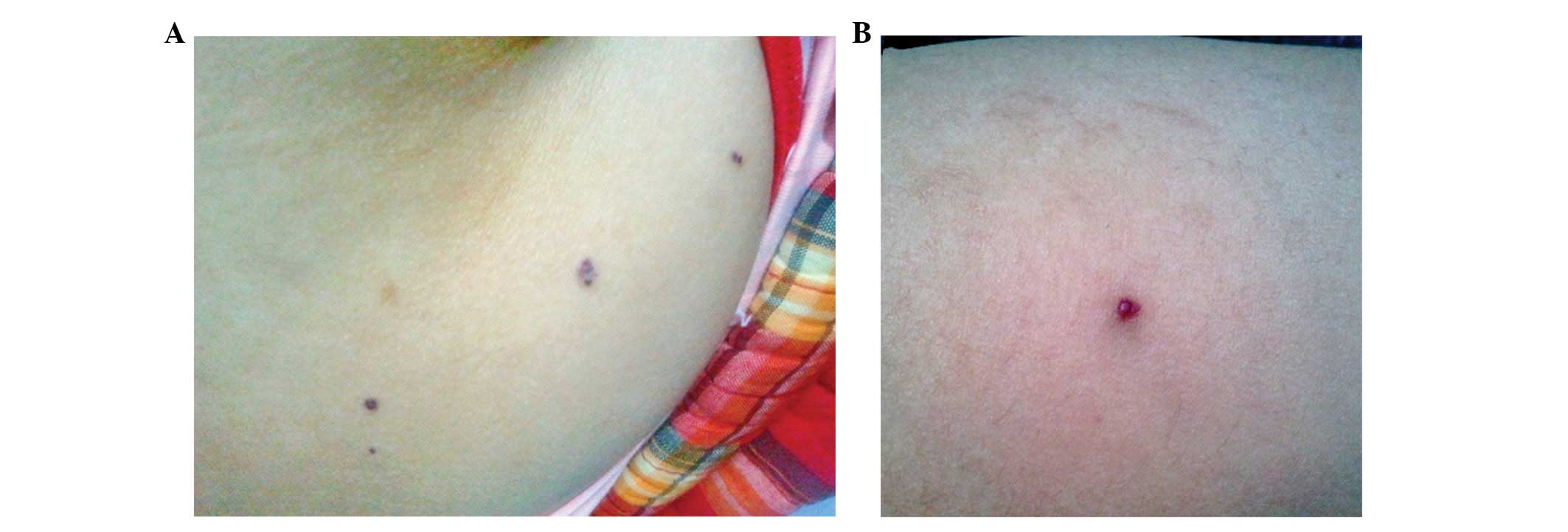
Since infancy, the patient had exhibited massive characteristic
venous malformations of the skin, which were deep blue, soft,
rubbery and easily compressible. Between 1991 and 2012, the patient
had a history of recurrent GI bleeding and iron-deficiency anemia.
The patient did not have any history of non-steroidal
anti-inflammatory drug use or peptic ulcers. The patient had
received several blood transfusions and, at 12 years of age, an
abdominal surgery was performed to resect the hemangiomas in the
stomach. A pathological report revealed hemangioma. According to
laboratory examinations, the patient exhibited a hemoglobin level
of 41.0 g/l, a red blood cell count of 2,410/mm3, a
reduced white blood cell count and an increased neutrophil
granulocyte count. Skin lesions of various sizes occurred on the
abdomen, hip and leg of the patient (Fig. 1). The patient received a blood
transfusion and hemostatic therapy. Following hemostatic therapy, a
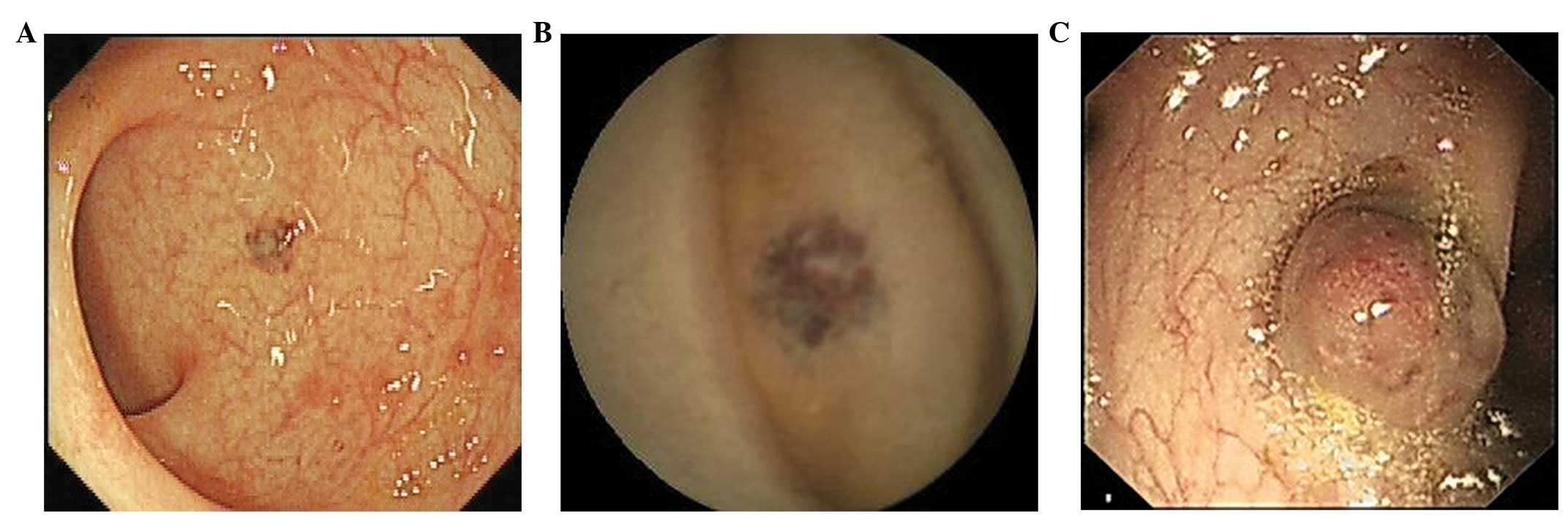
fecal occult blood test yielded negative results. In order to
detect the origin of the hemorrhage, a colonoscopy and capsule
endoscopy were performed. Endoscopy revealed several
strawberry-like mucosal polypoid lesions with abundant vasculature
in the colon and lesions ranging between 8 and 20 mm were
blue-violet and sessile (Fig. 2).
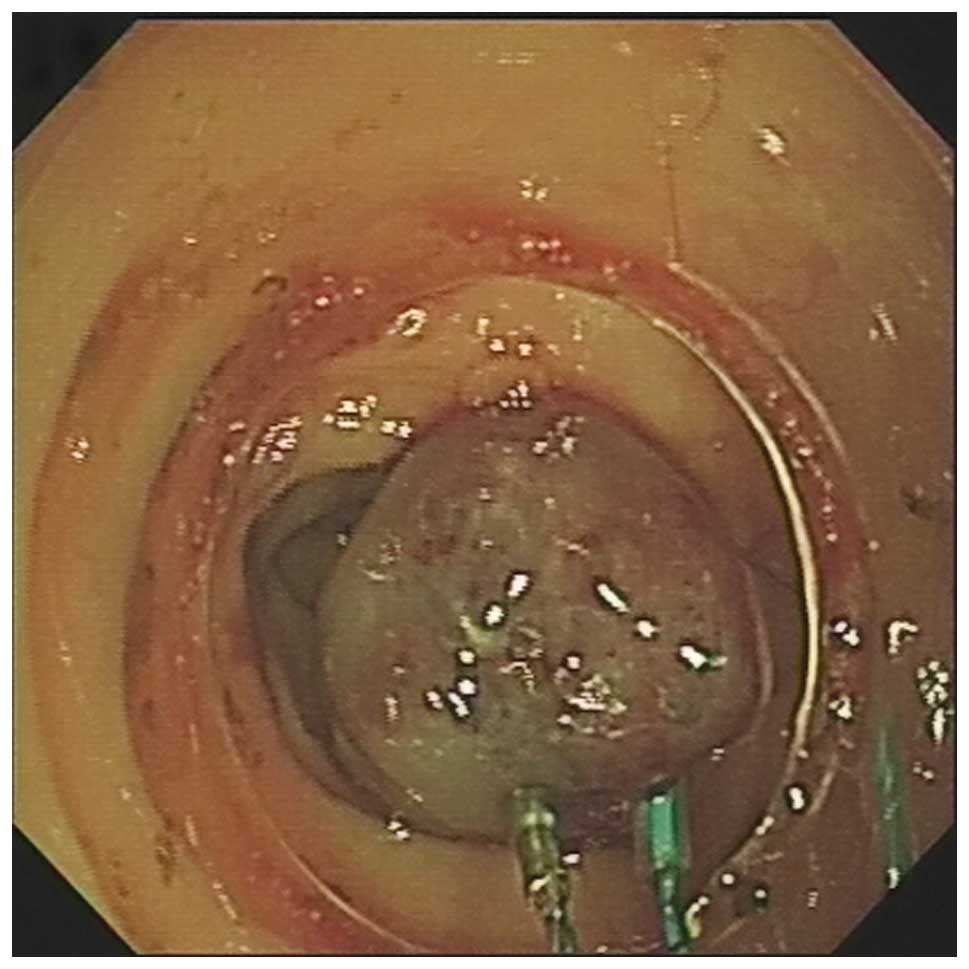
Colon lesions were removed in an attempt to eliminate bleeding
under colonoscopy. During surgery, hemangiomas were ligated with a
nylon cord and several small blue mucosal polypoid lesions were
treated with sclerosing agent during colonoscopy (Fig. 3). The patient was discharged in a
good condition. A repeat endoscopy at 3 months revealed completely
normal mucosa in the original lesions. A number of small lesions
that remained were treated with sclerosing agent. Over the
subsequent three and a half years, the patient was reviewed
regularly and no more bleeding episodes were noted.
We were able to diagnose the patient with BRBNS,
according to the cutaneous angiomas and the GI mass lesions that
were identified to be hemangiomas. However, it is necessary to
differentiate BRBNS from hereditary hemorrhagic telangiectasia,
Peutz-Jeghers syndrome, Klippel-Trénaunay syndrome and Maffucci
syndrome.
Discussion
BRBNS is a rare disorder characterized by multiple
recurrent vascular malformations, including hemangiomas, which
primarily locate on the skin and GI tract (1). Cutaneous angiomas are blue or purple,
soft, rubbery, sessile, ‘nipple-like’ nodules with wrinkled and
hyperhydrotic surfaces. However, they may also lie deep in the skin
and appear as bluish macules. A number of studies have reported
that BRBNS patients experience a gradual increase in pain (19). Pain may be caused by the
contraction of smooth muscle fibers surrounding the vascular tumors
(20). The molecular mechanisms
underlying this disease are yet to be fully elucidated. It has been
identified that normal endothelial cells of adult vessels do not
show c-kit expression, whereas at least partial c-kit positivity
has been reported in angiosarcomas (21). In addition, it has been
demonstrated that pharmacological inhibition of the c-kit signaling
pathway in cavernous hemangiomas by selective kinase inhibitors may
offer options in the treatment of BRBNS patients (22). Nobuhara et al (23) identified mutations in the TIE2 gene
that encode an endothelial cell tyrosine kinase receptor, which may
govern the thickness of the smooth muscle wall of a vessel.
Various treatments for BRBNS are shown in Table I. Progress in endoscopic technology
has advanced medical practice concerning the GI tract. Endoscopic
diagnosis and treatment of conditions has now supplanted a number
of surgical procedures and ongoing technical improvements, and
innovations continue to extend the potential for endoscopic
therapies (24). In the present
case, the patient had exhibited gastrointestinal hemorrhage for 22
years. The patient had received several blood transfusions and iron
replacement therapy for anemia by mouth. Endoscopy demonstrated
that there were a number of hemangiomas in the GI tract. Further
endoscopy was then undertaken to treat the hemangiomas using
sclerosis and banding ligation. During a 12-month follow-up, the
patient did not exhibit hemorrhage or anemia, and the hemoglobin
level was in the normal range.
 | Table I.Treatments for blue rubber bleb nevus
syndrome. |
Table I.
Treatments for blue rubber bleb nevus
syndrome.
| Year of
publication | Author | Therapeutic
methods | Complications related
to treatment | Outcome | Ref |
|---|
| 1990 | Maunoury et
al | Nd:YAG laser and
bipolar electrocoagulation | None | Avoided hemorrhagic
recurrence of lesions in the small bowel | (10) |
| 1996 | Carr et
al | Enterotomies | - | Stable at follow-up 5
years later | (14) |
| 1999 | Sala Felis et
al | Endoscopic treatment
by sclerosis and banding ligation | None | Effective | (9) |
| 2001 | Place | Multiple resectional
surgeries (partial gastrectomy, partial small bowel resection,
total abdominal colectomy and end ileostomy) | Iron-deficiency,
anemia nephrolithiasis, major depression, and malnutrition | Significant long-term
complications | (16) |
| 2003 | Ng and Kong | Argon plasma
coagulation | - | Simple, inexpensive
and effective treatment | (13) |
| 2006 | Anzinger et
al | Therapeutic double
balloon enteroscopy | None | Effective | (11) |
| 2007 | Okabayashi et
al | Laparoscopic
surgery | None | Without iron
deficiency anemia for a year following the operation | (12) |
| 2008 | Emami et
al | Endoscopic
polypectomy resection | None | Useful | (18) |
| 2010 | Blaise et
al | Polidocanol foam
sclerotherapy | None | Technique has not yet
been standardized | (15) |
| 2012 | Yuksekkaya et
al | Sirolimus | No drug adverse
reaction at 20-month follow-up | Vascular masses were
reduced rapidly and there was no gastro-intestinal bleeding | (17) |
Surgery is an alternative therapy option. It is an
effective method of hemostasis and allows the removal of
hemangiomas simultaneously. However, if there are several vascular
malformations along the whole digestive tract, surgical methods may
not be feasible. Place (16)
reported that multiple resectional surgeries (partial gastrectomy,
partial small bowel resection, total abdominal colectomy and end
ileostomy) resulted in significant long-term complications,
including iron-deficiency anemia, nephrolithiasis, major depression
and malnutrition. In the present case, endoscopic banding ligation
and sclerotherapy were selected. Combined with interferon α, GI
bleeding in the patient may be controlled effectively. The results
achieved were comparable with those of surgery. Therefore, patients
are more willing to accept endoscopic treatment than surgical
therapy. Endoscopic management of BRBNS may not only increase the
quality of life, but may also reduce the medical cost and
hospitalization time of patients.
References
|
1.
|
Bean WB: Blue rubber bleb nevi of the skin
and gastrointestinal tract. Vascular Spiders and Related Lesions of
the Skin. Charles C Thomas; Springfield, IL: pp. 17–185. 1958
|
|
2.
|
Tomelleri G, Cappellari M, Di Matteo A,
Zanoni T, Colato C, Bovi P and Moretto G: Blue rubber bleb nevus
syndrome with late onset of central nervous system symptomatic
involvement. Neurol Sci. 31:501–504. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Nahm WK, Moise S, Eichenfield LF, Paller
AS, Nathanson L, Malicki DM and Friedlander SF: Venous
malformations in blue rubber bleb nevus syndrome: variable onset of
presentation. J Am Acad Dermatol. 50(Suppl): S101–S106. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Gallione CJ, Pasyk KA, Boon LM, Lennon F,
Johnson DW, Helmbold EA, Markel DS, et al: A gene for familial
venous malformations maps to chromosome 9p in a second large
kindred. J Med Genet. 32:197–199. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
McKinlay JR, Kaiser J, Barrett TL and
Graham B: Blue rubber bleb nevus syndrome. Cutis. 62:97–98.
1998.
|
|
6.
|
Fishman SJ, Smithers CJ, Folkman J, Lund
DP, Burrows PE, Mulliken JB and Fox VL: Blue rubber bleb nevus
syndrome: surgical eradication of gastrointestinal bleeding. Ann
Surg. 241:523–528. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Shin SH, Chae HS, Ji JS, Kim HK, Cho YS,
Chang ED and Choi KY: A case of blue rubber bleb nevus syndrome.
Korean J Intern Med. 23:208–212. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Torchia D, Schincaglia E and Palleschi GM:
Blue rubber-bleb naevus syndrome arising in the middle age. Int J
Clin Pract. 64:115–117. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Sala Felis T, Urquijo Ponce JJ, López
Viedma B, Pertejo Pastor V and Berenguer Lapuerta J: Blue nevus
syndrome: endoscopic treatment by sclerosis and banding ligation.
Gastroenterol Hepatol. 22:136–138. 1999.(In Spanish).
|
|
10.
|
Maunoury V, Turck D, Brunetaud JM, Marti
R, Cortot A, Farriaux JP and Paris JC: Blue rubber bleb nevus
syndrome. 3 cases treated with a Nd:YAG laser and bipolar
electrocoagulation. Gastroenterol Clin Biol. 14:593–595. 1990.(In
French).
|
|
11.
|
Anzinger M, Gospos J, Pitzl H, Koletzko S,
Heldwein W and Schmitt W: Blue rubber-bleb nevus syndrome and
therapeutic double balloon enteroscopy. Z Gastroenterol.
44:1141–1144. 2006.(In German).
|
|
12.
|
Okabayashi K, Hasegawa H, Nishibori H,
Ishii Y and Kitajima M: A case of laparoscopic surgery for blue
rubber bleb nevus syndrome. Hepatogastroenterology. 54:451–453.
2007.PubMed/NCBI
|
|
13.
|
Ng WT and Kong CK: Argon plasma
coagulation for blue rubber bleb nevus syndrome in a female infant.
Eur J Pediatr Surg. 13:137–139. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Carr MM, Jamieson CG and Lal G: Blue
rubber bleb nevus syndrome. Can J Surg. 39:59–62. 1996.PubMed/NCBI
|
|
15.
|
Blaise S, Riom H, Charavin-Cocuzza M,
Templier I, Zambelli L and Diamand JM: Blue rubber bleb nevus
syndrome treated with polidocanol foam sclerotherapy. Dermatol
Surg. 36:2067–2068. 2010. View Article : Google Scholar
|
|
16.
|
Place RJ: Blue rubber bleb nevus syndrome:
a case report with long-term follow-up. Mil Med. 166:728–730.
2001.PubMed/NCBI
|
|
17.
|
Yuksekkaya H, Ozbek O, Keser M and Toy H:
Blue rubber bleb nevus syndrome: successful treatment with
sirolimus. Pediatrics. 129:e1080–e1084. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Emami MH, Haghdani S, Tavakkoli H and
Mahzouni P: Endoscopic polypectomy resection of blue rubber bleb
nevus lesions in small bowel. Indian J Gastroenterol. 27:165–166.
2008.PubMed/NCBI
|
|
19.
|
Kishikawa H, Okada Y, Kawahara T, Saito K
and Tanaka Y: A case of blue rubber bleb nevus syndrome treated by
etidronate. J Bone Miner Metab. 25:138–141. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Fine RM, Derbes VJ and Clark WH Jr: Blue
rubber bleb nevus. Arch Dermatol. 84:802–805. 1961. View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Miettinen M, Sarlomo-Rikala M and Lasota
J: KIT expression in angiosarcomas and fetal endothelial cells:
lack of mutations of exon 11 and exon 17 of c-kit. Mod Pathol.
13:536–541. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Mogler C, Beck C, Kulozik A, Penzel R,
Schirmacher P and Breuhahn K: Elevated expression of c-kit in small
venous malformations of blue rubber bleb nevus syndrome. Rare
Tumors. 2:e362010. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Nobuhara Y, Onoda N, Fukai K, et al: TIE2
gain-of-function mutation in a patient with pancreatic lymphangioma
associated with blue rubber-bleb nevus syndrome: report of a case.
Surg Today. 36:283–286. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
ASGE Standards of Practice Committee;
Early DS, Ben-Menachem T, Decker GA, et al: Appropriate use of GI
endoscopy. Gastrointest Endosc. 75:1127–1131. 2012. View Article : Google Scholar : PubMed/NCBI
|