Introduction
A number of drugs may produce lung injury and novel
anticancer drugs, including molecular targeted drugs, are causative
of severe lung injury (1–3). The development of novel anticancer
drugs and biological agents may result in an increase in the
incidence of drug-induced lung injury.
Although poorly understood, direct cellular injury
by anti-cancer drugs and their metabolites, and/or indirect injury
via the activation of immune cells have been suggested as
mechanisms underlying the onset of drug-induced lung injury
(4,5). The onset of lung injury is also
modified by a variety of background factors, including genes
involved in drug metabolism, genetic factors, such as
immunity-related genes, patient age, total drug dose, synergistic
effects of drug combinations, previous or current radiation
therapy, background respiratory disease, a history of smoking,
oxygen inhalation/respirator management, bone marrow/stem cell
transplants and renal failure (6,7).
At present there is no appropriate non-invasive
clinical test for drug-induced lung injury. Pathological and
imaging findings are non-specific and do not facilitate the
identification of causative drugs (8). In addition, the same drug may produce
different patterns of lung injury depending on the dose and
individual responses. While steroids and immunosuppressants are
used to suppress lung inflammation, they fail to improve the
prognosis of patients (9).
The fibrosis inhibitor pirfenidone (10), the antioxidant edaravone (11) and the cytoprotective agent
erythropoietin (12) have
different mechanisms of action. Using a rabbit model of
bleomycin-induced lung injury we studied the effectiveness of these
drugs in suppressing lung tissue injury. We evaluated time-course
changes on computed tomography (CT) images and compared concurrent
imaging and pathological findings.
Materials and methods
This study was approved by the Ethics Committee on
Animal Experiments of Shiga University of Medical Science (Otsu,
Japan).
Animal model and drugs
Nine Japanese white rabbits (SLC Inc., Shizuoka,
Japan) weighing 3 kg were divided into three equal groups. Group 1
served as the control, group 2 received monotherapy with
pirfenidone (Shionogi & Co. Ltd., Osaka, Japan) and group 3 was
treated with pirfenidone, edaravone (Mitsubishi Pharma Co., Osaka,
Japan), and erythropoietin (Chugai Pharma Co., Ltd., Tokyo, Japan).
Bleomycin hydrochloride (30 mg; Nihon Kayaku Co., Tokyo, Japan),
dissolved in 2 ml physiological saline, was delivered into the
trachea by a 22-gauge indwelling needle. To obtain drug
distribution throughout the lungs, 0.5 ml of this solution was
administered iteratively with postural changes of the recipients.
Pirfenidone was administered orally (90 mg/day) for 28 days.
Edaravone and erythropoietin were intravenously administered at 3.6
mg/day for 7 days and 30,000 IU/day for 3 days, respectively.
CT examination
CT images were acquired on a four-row multidetector
computed tomography (MDCT) scanner (Toshiba Medical Systems
Corporation, Tokyo, Japan) before, immediately after and 14 and 28
days after the administration of bleomycin. The scanning parameters
were as follows: X-ray tube voltage, 120 kV; X-ray tube current, 50
mA; collimation, 1 mm; field of view, 100 mm; and helical pitch
(HP), 0.8. Following CT scanning on day 28, the rabbits were
euthanized and their lungs were resected. Inflated fixed lungs were
prepared according to the method of Heitzman (13).
The CT images were reconstructed; horizontal 1-mm
thick cross-sections were constructed at 3-mm intervals from the
apex of the lungs in the lung window. The images were recorded
using Aquarius NetStation iNtuition Edition (Tera Recon Inc., San
Mateo, CA, USA) and analyzed with Segmentation Analysis and
Tracking (SAT) image software (Tera Recon Inc., San Mateo, CA,
USA). Two radiologists individually measured the normal and
affected areas (ground-glass opacities and infiltrative shadows) in
each cross-section, calculated the average area of abnormal shadows
in the lung field and evaluated time-course changes. When the
measurements were consistent they were adopted for analysis.
Histopathological examination
The resected lungs were fixed in formaldehyde and
consecutive 4-μm thick slices were stained with hematoxylin
and eosin and Elastica van Gieson stain. One cross-section on each
glass slide was selected from the center of the craniocaudal axis
in the bilateral anterior and posterior lobes. These slides were
scanned with Coolscan (Nikon, Tokyo, Japan) for macroscopic
evaluation. Lesions were measured using ImageJ software (version
1.43, US National Institutes of Health) and the average size was
compared among the three groups. Macroscopic images (magnification,
×200) were evaluated by one pathologist and one radiologist
specializing in chest diseases. The evaluators consensually scored
the degree of inflammatory cell infiltration in the alveolar wall
and alveoli using the method of Hirose et al (14), on a scale of 0 (mild) to 5
(severe). The sum of the scores (0–10) in the bilateral anterior
and posterior lobes of each rabbit was recorded and the average was
calculated to evaluate inflammatory changes. To evaluate the degree
of fibrosis, interstitial fibrosis and the formation of honeycomb
lung lesions were recorded on a score of 0 to 5 and the degree of
alveolar metaplasia and smooth muscle proliferation in interstitial
tissue was recorded on a score of 0 to 2. The average of the sum of
the scores, from 0 to 14, in the bilateral anterior and posterior
lobes was evaluated (14).
Microscopic slides were examined by a pathologist with 16 years of
experience.
Statistical analysis
CT and pathological findings from the three groups
of rabbits were compared using the t-test. Findings from
microscopic images were assessed using Tukey’s honestly significant
difference (HSD) test. P<0.05 was considered to indicate a
statistically significant difference; a trend toward a significant
difference was considered to be present at 0.05<P<0.10.
Results
CT examination
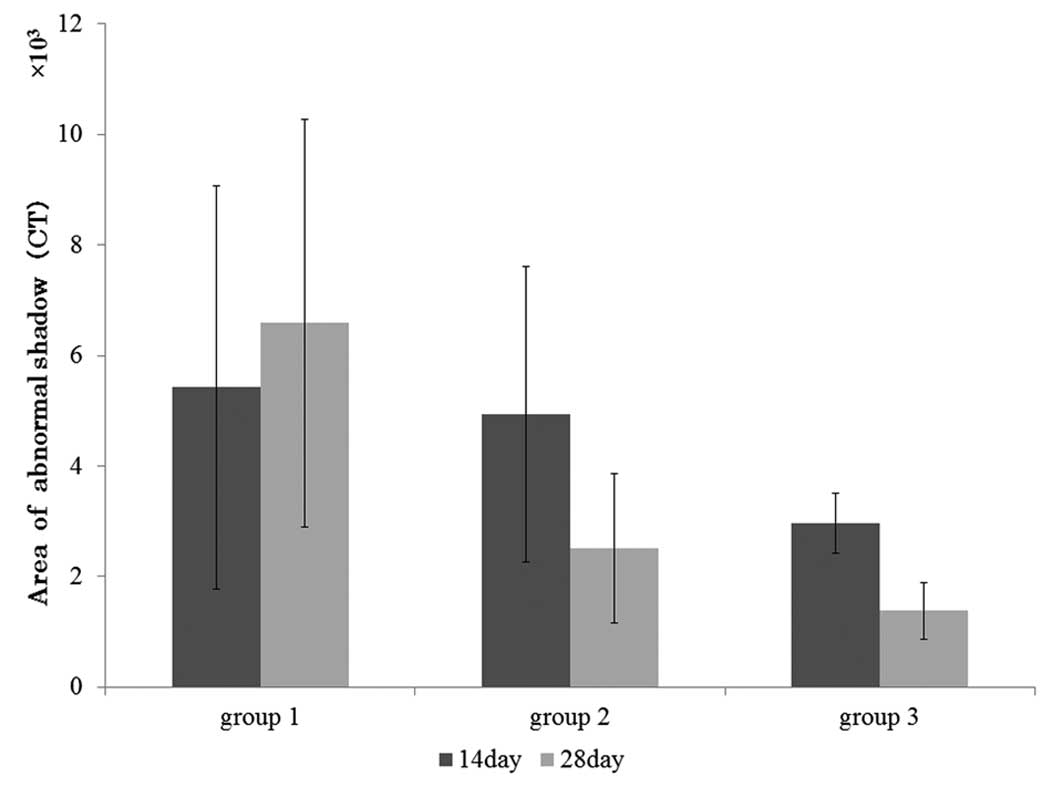
On CT images acquired 14 and 28 days after the
administration of bleomycin, the average size of the abnormal areas
was largest in the control group, followed by rabbits subjected to
monotherapy and triple therapy (groups 1, 2 and 3, respectively;
Fig. 1 and Table I). The mean values for groups 1, 2
and 3 on day 14 were 5.42, 4.95 and 2.96×103
mm2, respectively and on day 28 were 6.59, 2.51 and
1.38×103 mm2, respectively. While there was
no significant difference among the three groups on day 14, on day
28 the abnormal area was markedly smaller in group 3 compared with
that in group 1 (P=0.071). There was no significant difference
between groups 2 and 3. On day 28 the area with abnormal shadows
was smaller compared with that on day 14 in the two experimental
groups, while it was slightly larger in the controls.
 | Table I.Effect of different treatments on the
size of the abnormal area, as measured using CT
(mm2). |
Table I.
Effect of different treatments on the
size of the abnormal area, as measured using CT
(mm2).
| Group | Rabbit 1 | Rabbit 2 | Rabbit 3 |
|---|
| Day 14 | | | |
| Group 1 | 5,255.63 | 1,849.79 | 9,151.77 |
| Group 2 | 6,460.87 | 6,497.77 | 1,863.44 |
| Group 3 | 3,546.37 | 2,865.62 | 2,484.55 |
| Day 28 | | | |
| Group 1 | 2,711.62 | 10,062.89 | 6,998.04 |
| Group 2 | 3,276.21 | 3,310.37 | 937.38 |
| Group 3 | 1,748.98 | 1,589.65 | 798.37 |
Histopathological examination
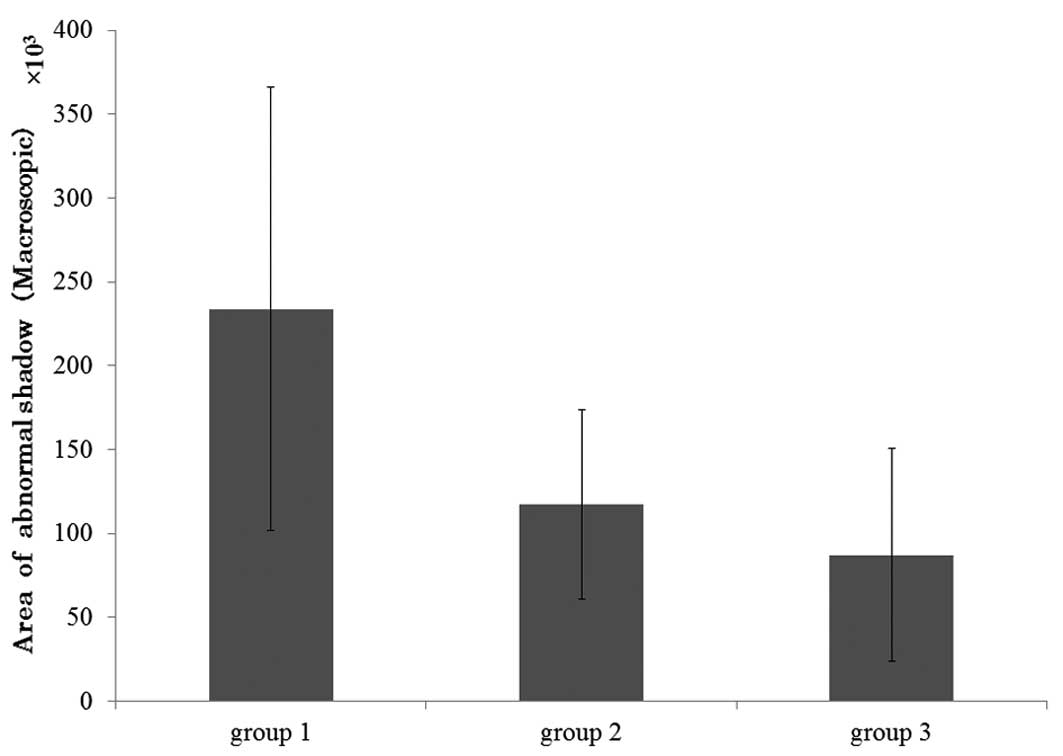
Macroscopic findings.
Macroscopically, group 1 exhibited the largest
abnormal areas; average size of abnormal areas,
233.80×103 (group 1) vs. 117.25×103 (group 2)
and 87.1×103 μm2 (group 3). The
difference between groups 1 and 3 was significant (P<0.05) and
there was a marked difference (P= 0.09) between groups 1 and 2.
There was no significant difference between groups 2 and 3
(Fig. 2 and Table II).
| Table II.Size of the abnormal area in the
macroscopic pathology image of each group
(μm2). |
Table II.
Size of the abnormal area in the
macroscopic pathology image of each group
(μm2).
| Group | Rabbit 1 | Rabbit 2 | Rabbit 3 |
|---|
| Group 1 | 271647.5 | 319624.5 | 110117.3 |
| Group 2 | 115202.5 | 61994.0 | 128822.8 |
| Group 3 | 144483.3 | 67646.3 | 49180.5 |
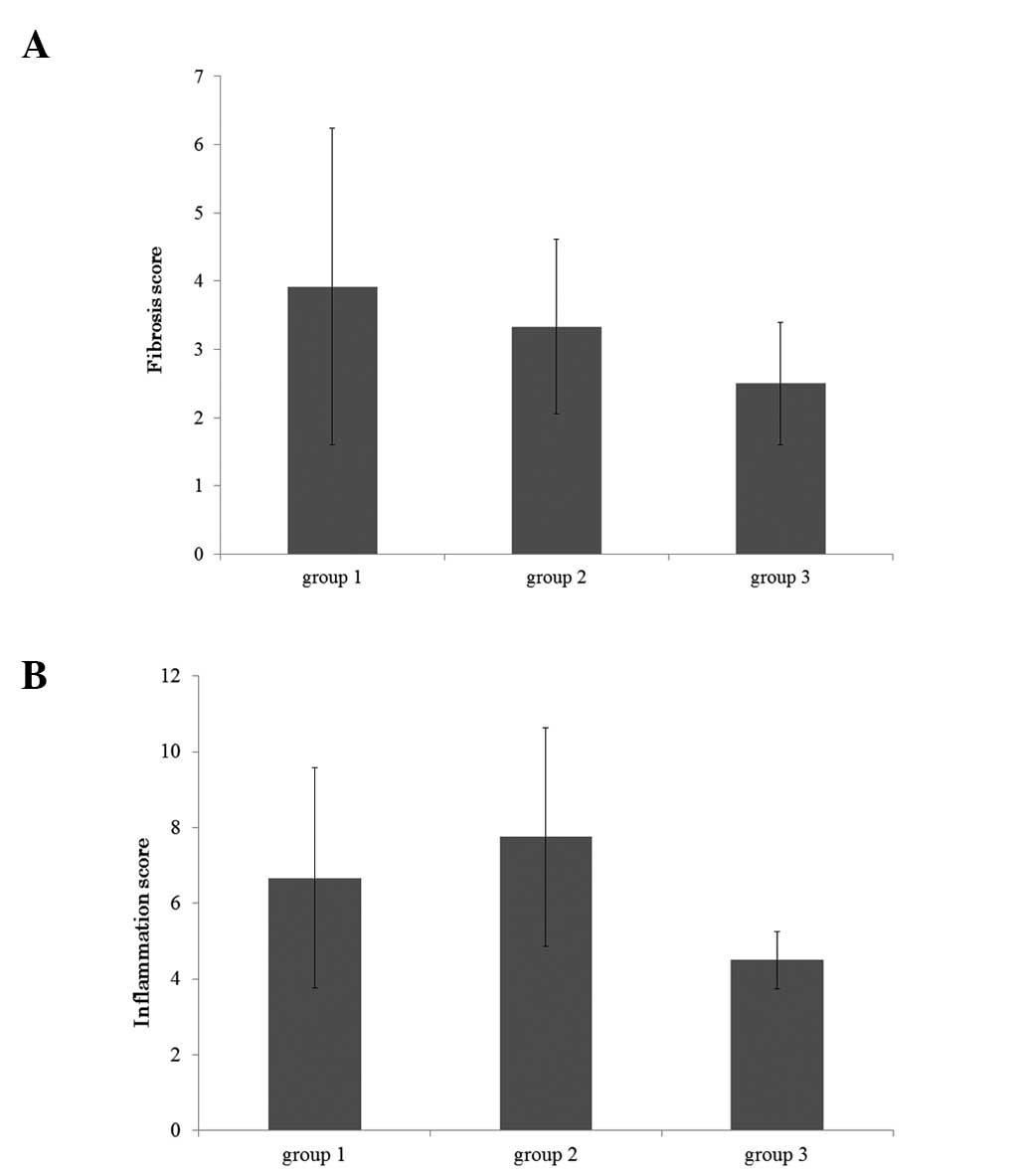
Microscopic findings.
The average fibrosis score was highest in group 1
followed by groups 2 and 3 (group 1, 3.92; group 2, 3.33; group 3,
2.50; Fig. 3A and Table III). Group 2 presented the highest
average inflammation score, followed by groups 1 and 3 (control,
6.67; group 2, 7.75; group 3, 4.50; Fig. 3B and Table III). There was no significant
difference in the average fibrosis score among the three
groups.
| Table III.Microscopic findings (fibrosis and
inflammation score). |
Table III.
Microscopic findings (fibrosis and
inflammation score).
| Scores | Rabbit 1 | Rabbit 2 | Rabbit 3 |
|---|
| Fibrosis score | | | |
| Group 1 | 7.75 | 2.75 | 1.25 |
| Group 2 | 2.25 | 4.75 | 3.00 |
| Group 3 | 2.75 | 1.50 | 3.25 |
| Inflammation
score | | | |
| Group 1 | 10.00 | 4.75 | 5.25 |
| Group 2 | 4.50 | 8.75 | 10.00 |
| Group 3 | 4.50 | 3.75 | 5.25 |
Discussion
Among anticancer drugs, bleomycin elicits the
highest rate of drug-induced interstitial pneumonitis and pulmonary
fibrosis; ∼10% of patients treated with bleomycin develop lung
injuries (15). Molecules of this
drug harbor an iron-binding site and an iron ion induces a free
radical, which in turn plays a role in cleaving DNA.
Although the mechanism(s) by which bleomycin induces
pulmonary fibrosis remain to be elucidated, reactive oxygen species
(ROS) produced by bleomycin directly injure the lung epithelium and
endothelium (16–18). Early lung injuries induce an
increase in the recruitment of activated inflammatory cells into
the lung parenchyma. The production of ROS by inflammatory cells,
including alveolar macrophages and polymorphonuclear leukocytes, is
considered to be closely associated with the pathogenesis of
bleomycin-induced pulmonary fibrosis (19).
Fibrosis inhibitors, anti-oxidants and
cytoprotective agents have been evaluated for ability to attenuate
the effects of bleomycin. Pirfenidone, a fibrosis inhibitor, was
first approved in 2008 for the treatment of idiopathic pulmonary
fibrosis (20). The production of
inflammatory cytokines, including tumor necrosis factor (TNF)-α,
interleukin (IL)-1 and IL-6 is suppressed while the production of
anti-inflammatory cytokines, including IL-10 is stimulated by this
drug. These activities suppress the reduction in the interferon
(IFN)-γ level and this corrects the imbalance in Th2-type
predominant reactions (i.e., correction of the Th1/Th2 balance). As
pirfenidone also suppresses the production of growth factors
related to fibrosis formation, including transforming growth factor
(TGF)-β1, basic fibroblast growth factor (b-FGF) and
platelet-derived growth factor (PDGF), it regulates the production
of a variety of cytokines and growth factors (21,22).
The suppressive effect of pirfenidone on fibroblast proliferation
and collagen production may be involved in its suppression of
fibrosis.
The antioxidant edaravone, approved for use in Japan
in April 2001, is the first brain protective agent (23). It eliminates or detoxifies harmful
free radicals and protects the brain from oxidative stress. It has
been reported that the inhibition of interstitial edema and of
infiltration by inflammatory cells via ROS suppresses the progress
of pulmonary fibrosis (18).
Erythropoietin, a hematopoietic cytokine produced in
the kidneys, induces erythroblast differentiation and plays a major
role in stimulating hematopoiesis. It also stimulates
apoptosis-inhibitory factors, inhibits apoptosis by inhibiting
apoptosis-inducing factors, and exerts cytoprotective activity by
binding the erythropoietin receptor (EPOR) expressed in the heart,
vascular system and brain. As human recombinant erythropoietin
(rhEPO) directly inhibits pulmonary fibrosis by binding to EPOR on
alveolar and bronchial epithelial cells (24), it may promote the healing of these
cells damaged by anticancer drugs via the induction of vascular
endothelial precursor cells in the bone marrow, thereby indirectly
inhibiting pulmonary fibrosis (25).
In the present study we compared abnormal shadows on
CT scans in rabbits. The results demonstrate that the area of
abnormal shadows was slightly larger on day 28 compared with that
on day 14 after bleomycin administration, which may be attributable
to persistent, aggravated drug-induced lung injury. At the two
time-points, these areas were smallest in the triple therapy group;
in the two experimental groups, the average size of abnormal areas
was significantly smaller on day 28 compared with day 14. This
observation suggests that the combined administration of edaravone,
erythropoietin, and pirfenidone more potently suppressed the
progression of drug-induced lung injury than monotherapy with
pirfenidone.
While we identified no difference among the three
groups on day 14 after bleomycin administration, on day 28 there
was a marked difference between the controls and rabbits subjected
to triple therapy. According to Nagatani et al (26) and Izbicki et al (27), the tracheal delivery of bleomycin
results in lung injury, which suggests that interstitial
inflammation and edematous changes occur in the early stage prior
to the manifestation of fibrotic changes. We posit that the
abnormal shadows we detected on CT scans obtained on day 14 were
indicative of not only early-stage fibrosis, but also of
inflammatory changes, and that images acquired on day 28
demonstrated fibrotic changes following the amelioration of
interstitial inflammation. Comparison of groups 2 and 3 revealed
that triple therapy resulted in the prolonged, potent suppression
of fibrosis in rabbits treated with bleomycin.
Fibrotic and inflammatory changes were compared in
the present study. Macroscopically, the average area of abnormal
shadows was largest in group 1 followed, in order, by groups 2 and
3. There was a marked difference between the controls and group 1
(P=0.09) and there was a significant difference between the
controls and group 3 (P<0.05). These findings suggest that
bleomycin-induced lung injury, including inflammation and fibrosis
of lung tissue, was reduced by monotherapy with pirfenidone and by
triple therapy with edaravone, erythropoietin and pirfenidone.
Microscopic analysis revealed no significant
difference in the fibrosis score of the three groups; however, the
severity of fibrosis was greater in group 1 compared with that in
groups 2 and 3, and greater in group 2 than in group 3, suggesting
that triple therapy suppressed fibrosis more potently than
monotherapy.
Although there was no significant difference in the
inflammation score among the three groups, the average score for
inflammatory changes was the highest in group 2, followed by group
1 and group 3. We offer two explanations for the difference between
this observation and our CT and pathological findings: i) Fibrotic
changes are the final stage while inflammatory changes are the
mid-term process of drug-induced lung injury (26,27).
In the rabbits in the present study, lung inflammation had subsided
and the development of fibrosis had begun by day 28 after bleomycin
administration. The observation that inflammation subsided earlier
in the control than in the monotherapy group supports this
hypothesis; ii) since monotherapy with pirfenidone suppresses the
production of inflammatory cytokines and stimulates the production
of anti-inflammatory cytokines, inflammatory changes may have
advanced more slowly in rabbits treated with pirfenidone than in
the controls where these changes quickly shifted to fibrosis.
As we acquired all the pathological samples on day
28 after the delivery of bleomycin, we were unable to perform
time-course studies of the lung injury induced by bleomycin.
We attribute the absence of significant differences
in the fibrosis and inflammation scores among the three groups to
our selection process for microscopic evaluation, since only one
slide from bilateral specimens of the anterior and posterior lobes
was used. Consequently, the slides we studied may not have included
portions with severe fibrosis and inflammatory changes. In future
studies we will refer to CT images to identify areas exhibiting
severe changes prior to selecting the slides to be used for
pathological evaluation.
The mechanism(s) underlying the lung injury induced
by drugs remain poorly understood. With respect to anticancer drugs
and their metabolites, indirect mechanisms based on allergic
reactions have been suggested (28), although both direct and indirect
mechanisms may result in drug-induced lung injury.
Direct injury to lung capillary and alveolar
epithelial cells results in increased vascular permeability and
interstitial edema, and promotes fibrosis by stimulating
fibroblasts. As these changes are drug dose-dependent and become
chronic, the onset of drug-induced lung injury may be predictable.
Indirect cellular injury as a consequence of allergic reactions is
induced by drugs and their metabolites; changes in immune reactions
evoked by drugs and the involvement of type III and IV reactions
are suspected (29–32). As these changes are not
dose-dependent, it is not possible to predict their manifestation
and in certain instances an acute clinical course may lead to
respiratory insufficiency within a few days of the start of drug
administration (33). In addition,
depending on the patient’s background, a variety of clinical
courses and symptoms may be elicited in patients receiving the same
drug. This suggests the involvement of different mechanisms in the
elicitation of drug-induced lung injury.
The rabbit model of bleomycin-induced lung injury
used in the present study demonstrated that triple therapy with
pirfenidone, edaravone and erythropoietin was more effective than
monotherapy with pirfenidone. We posit that triple therapy
suppressed lung fibrosis more effectively than monotherapy since
the different mechanisms of action of pirfenidone, edaravone and
erythropoietin concurrently slowed the progression of lung
fibrosis.
Our study has a number of limitations. The
distribution of bleomycin in the lungs may not have been uniform
among individual rabbits and injury in different lung areas may
have resulted in differences in the degree and distribution of
abnormal areas among the animals. To assess the degree of
suppression of lung fibrosis by the administered drugs more
accurately, studies are underway to determine the rate change in
abnormal areas.
In conclusion, since allergy-based lung injury
induced by anticancer drugs progresses quickly and leads to
respiratory insufficiency within days, immediate and appropriate
treatment is imperative. We demonstrated that the combined
administration of pirfenidone, edaravone and erythropoietin
effectively limited the extent of lung damage in a rabbit model of
bleomycin-induced lung injury.
References
|
1.
|
Inoue A, Saijo Y, Maemondo M, Gomi K,
Tokue Y, et al: Severe acute interstitial pneumonia and gefitinib.
Lancet. 361:137–139. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Camus P, Kudoh S and Ebina M: Interstitial
lung disease associated with drug therapy. Br J Cancer. 91(Suppl
2): S18–S23. 2004. View Article : Google Scholar
|
|
3.
|
Camus PH, Foucher P, Bonniaud P and Ask K:
Drug-induced infiltrative lung disease. Eur Respir J Suppl.
32:93s–100s. 2001.PubMed/NCBI
|
|
4.
|
Matsuno O: Drug-induced interstitial lung
disease: mechanisms and best diagnostic approaches. Respir Res.
13:392012. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Cooper JA Jr, Zitnik RJ and Matthay RA:
Mechanisms of drug-induced pulmonary disease. Annu Rev Med.
39:395–404. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Cooper JA Jr, White DA and Matthay RA:
Drug-induced pulmonary disease. Part 1: Cytotoxic drugs. Am Rev
Respir Dis. 133:321–340. 1986.PubMed/NCBI
|
|
7.
|
Cooper JA Jr, White DA and Matthay RA:
Drug-induced pulmonary disease. Part 2: Noncytotoxic drugs. Am Rev
Respir Dis. 133:488–505. 1986.PubMed/NCBI
|
|
8.
|
Cleverley JR, Screaton NJ, Hiorns MP, et
al: Drug-induced lung disease: high-resolution CT and histological
findings. Clin Radiol. 57:292–299. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Ohnishi H, Yokoyama A, Yasuhara Y,
Watanabe A, Naka T, et al: Circulating KL-6 levels in patients with
drug induced pneumonitis. Thorax. 58:872–875. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Gan Y, Herzog EL and Gomer RH: Pirfenidone
treatment of idiopathic pulmonary fibrosis. Ther Clin Risk Manag.
7:39–47. 2011.PubMed/NCBI
|
|
11.
|
Asai T, Ohno Y, Minatoguchi S, Funaguchi
N, Yuhgetsu H, et al: The specific free radical scavenger edaravone
suppresses bleomycin-induced acute pulmonary injury in rabbits.
Clin Exp Pharmacol Physiol. 34:22–26. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Kakavas S, Demestiha T, Vasileiou P and
Xanthos T: Erythropoetin as a novel agent with pleiotropic effects
against acute lung injury. Eur J Clin Pharmacol. 67:1–9. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Markarian B and Dailey ET: Preparation of
inflated lung specimens. Heitzman’s the Lung: Radiologic-Pathologic
Correlations. Groskin SA: 3rd edition. Mosby; St. Louis, MO: pp.
4–12. 1993
|
|
14.
|
Hirose N, Lynch DA, Cherniack RM and
Doherty DE: Correlation between high resolution computed tomography
and tissue morphometry of the lung in bleomycin-induced pulmonary
fibrosis in the rabbit. Am Rev Respir Dis. 147:730–738. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Du M, Irani RA, Stivers DN, Lee SJ and
Travis EL: H2-Ea deficiency is a risk factor for bleomycin-induced
lung fibrosis in mice. Cancer Res. 64:6835–6839. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Galvan L, Huang CH, Prestayko AW, Stout
JT, Evans JE and Crooke ST: Inhibition of bleomycin-induced DNA
breakage by superoxide dismutase. Cancer Res. 41:5103–5106.
1981.PubMed/NCBI
|
|
17.
|
Cunningham ML, Ringrose PS and Lokesh BR:
Inhibition of the genotoxicity of bleomycin by superoxide
dismutase. Mutat Res. 135:199–202. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Tajima S, Bando M, Ishii Y, Hosono T,
Yamasawa H, et al: Effects of edaravone, a free-radical scavenger,
on bleomycin-induced lung injury in mice. Eur Respir J.
32:1337–1343. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Martin WJ II and Kachel DL:
Bleomycin-induced pulmonary endothelial cell injury: evidence for
the role of iron-catalyzed toxic oxygen-derived species. J Lab Clin
Med. 110:153–158. 1987.PubMed/NCBI
|
|
20.
|
Iyer SN, Gurujeyalakshmi G and Giri SN:
Effects of pirfenidone on transforming growth factor-beta gene
expression at the transcriptional level in bleomycin hamster model
of lung fibrosis. J Pharmacol Exp Ther. 291:367–373.
1999.PubMed/NCBI
|
|
21.
|
Raghu G, Johnson WC, Lockhart D and Mageto
Y: Treatment of idiopathic pulmonary fibrosis with a new
antifibrotic agent, pirfenidone: results of a prospective,
open-label Phase II study. Am J Respir Crit Care Med.
159:1061–1069. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Azuma A, Nukiwa T, Tsuboi E, Suga M, Abe
S, Nakata K, et al: Double-blind, placebo-controlled trial of
pirfenidone in patients with idiopathic pulmonary fibrosis. Am J
Respir Crit Care Med. 171:1040–1047. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Shichinohe H, Kuroda S, Yasuda H, Ishikawa
T, Iwai M, Horiuchi M and Iwasaki Y: Neuroprotective effects of the
free radical scavenger edaravone (MCI-186) in mice permanent focal
brain ischemia. Brain Res. 1029:200–206. 2004.PubMed/NCBI
|
|
24.
|
MacRedmond R, Singhera GK and Dorscheid
DR: Erythropoietin inhibits respiratory epithelial cell apoptosis
in a model of acute lung injury. Eur Respir J. 33:1403–1414. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
25.
|
Ozer EA, Kumral A, Ozer E, Yilmaz O, Duman
N, Ozkal S, et al: Effects of erythropoietin on hyperoxic lung
injury in neonatal rats. Pediatr Res. 58:38–41. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
26.
|
Nagatani Y, Nitta N, Otani H, Mukaisho K,
Sonoda A, Nitta-Seko A, et al: Quantitative measurement of
bleomycin-induced lung fibrosis in rabbits using sequential in vivo
regional analysis and high-resolution computed tomography:
correlation with pathologic findings. Acad Radiol. 18:672–681.
2011. View Article : Google Scholar
|
|
27.
|
Izbicki G, Segel MJ, Christensen TG,
Conner MW and Breuer R: Time course of bleomycin-induced lung
fibrosis. Int J Exp Pathol. 83:111–119. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
28.
|
Ozkan M, Dweik RA and Ahmad M:
Drug-induced lung disease. Cleve Clin J Med. 68:782–795. 2001.
View Article : Google Scholar
|
|
29.
|
Gruchalla RS: Drug metabolism, danger
signals, and drug induced hypersensitivity. J Allergy Clin Immunol.
108:475–488. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
30.
|
Foucher P, Biour M, Blayac JP, Godard P,
Sgro C, et al: Drugs that may injure the respiratory system. Eur
Respir J. 10:265–279. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
31.
|
Camus P, Fanton A, Bonniaud P, Camus C and
Foucher P: Interstitial lung disease induced by drugs and
radiation. Respiration. 71:301–326. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
32.
|
Schnabel A, Richter C, Bauerfeind S and
Gross WL: Bronchoalveolar lavage cell profile in methotrexate
induced pneumonitis. Thorax. 52:377–379. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
33.
|
du Bois RM: An earlier and more confident
diagnosis of idiopathic pulmonary fibrosis. Eur Respir Rev.
21:141–146. 2012.PubMed/NCBI
|