Introduction
Paraquat, a member of the bipyridyl group of
herbicides, has been demonstrated to be an effective weedkiller and
is used worldwide. When used as intended, the compound is
relatively safe; however, misuse has led to a significant number of
deaths (1). The herbicide
properties of paraquat were identified in 1955 and it was
introduced commercially in 1962 (2). Paraquat is inactive when in contact
with almost all naturally occurring soils, and is a relatively
non-selective foliage-applied contact herbicide (3). The active ingredient in paraquat is
1,1′-dimethyl-4,4′-bipyridinium, a non-volatile, white, crystalline
solid, which decomposes at 300°C. 1,1′-Dimethyl-4,4′-bipyridinium
is particularly soluble in water, although insoluble in the
majority of organic solvents. It is highly toxic for humans, and
has been the cause of numerous cases of acute poisoning (4). Pulmonary fibrosis due to lipid
peroxidation is a major symptom of paraquat intoxication (5). The majority of cases of paraquat
poisoning result from its intentional ingestion, and in moderate to
severe cases the cause of death is normally hypoxemia, secondary to
lung fibrosis (6). However,
paraquat may be absorbed through skin injuries, and since 1978
there have been several reported cases of severe paraquat poisoning
by this pathway (7–10). Since the beginning of its
widespread use in 2000, acute paraquat poisoning has continued to
be a major public health problem in the rural areas of China,
normally from deliberate ingestion or accidental exposure (11). To the best of our knowledge, these
instances are rare in China. The aim of this case report was to
describe the successful treatment of two patients admitted with
dermal paraquat absorption following a crop-dusting accident in
which they obtained 3 and 2% total body surface area (TBSA) burns,
respectively. Informed consent was obtained from the patients.
Furthermore, the relevant literature was analyzed and the treatment
that led to the successful result was discussed.
Case reports
Case 1
A 51-year-old female presented at the Department of
Poisoning and Occupational Disease, Qilu Hospital of Shandong
University (Jinan, China) with mixed thickness burns to the upper
and lower limbs, and with progressive dyspnea. The patient was a
contractual worker who had been spraying paraquat in an orchard.
The solution in the knapsack spraying device contained 150 ml
commercialized concentrated formulation of 20% w/v paraquat and ~50
kg water. The patient had worked from 9:00 am to 12:00 am in the
summer and, due to the high temperature (~30°C), the patient’s
upper and lower limbs had been fully exposed to the solution,
without any protection. The solution had adhered to the patient’s
skin, particularly on the lower limbs. The patient did not wash the
affected area immediately. In the afternoon, the skin covered by
paraquat had developed erythema followed by blistering and
hemorrhaging hemorrhagic diabrosis. The patient was treated by a
community doctor for five days. Six days subsequent to the
incident, the patient’s condition deteriorated, with progressive
dyspnea, and the patient was sent to the Qilu Hospital of Shandong
University. Upon admission a general examination revealed that the
mentation of the patient was intact and the mental status was
normal. Physically, the patient presented with ~3% TBSA deep
second-degree chemical burns on the surface of the forearm and
lower limbs. The skin was raw, macerated and oozing pus, and
topical silver sulfadiazine had been applied to the affected area
(Fig. 1). The chest auscultation
breath sounds were rough, but no rhonchi or rales were observed.
The pulse rate was 88 beats/min at a regular rhythm with no extra
heart sounds or murmurs on auscultation of the various valve areas.
The abdomen was soft and nontender. The liver and spleen were
untouched under the ribs. Neurological examinations and the results
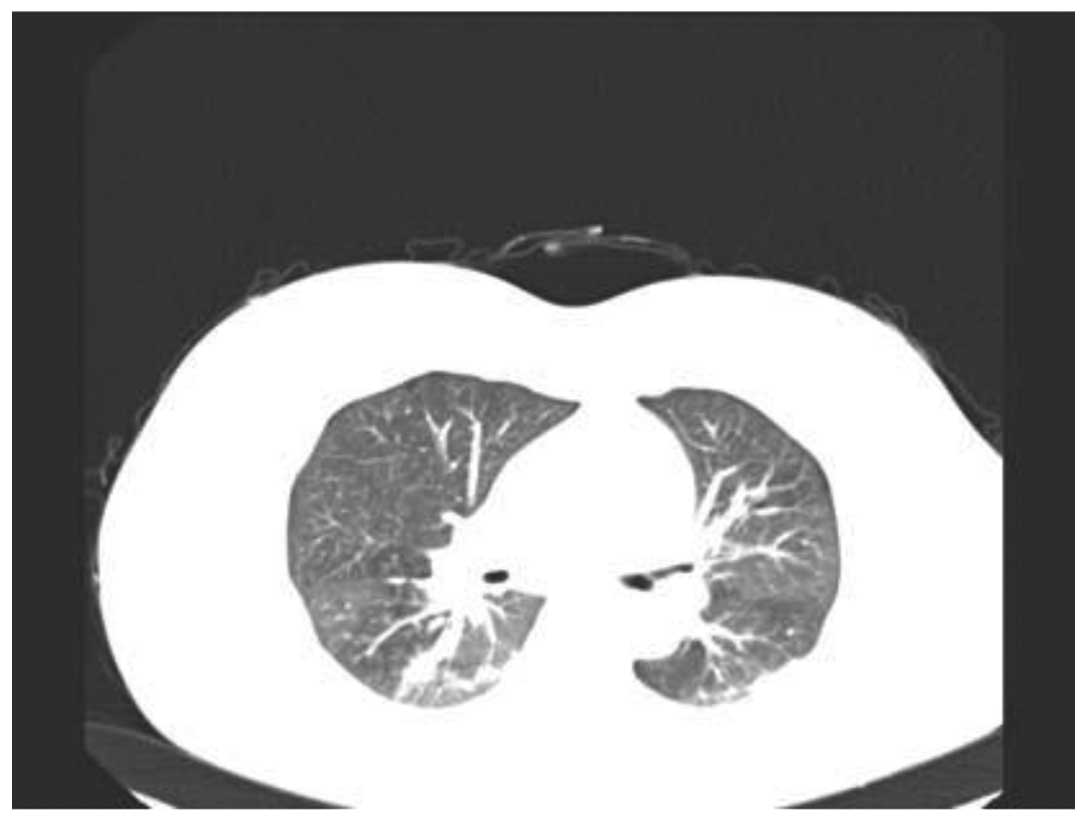
of the routine blood and urine tests were normal. The serum urea
level was 11.3 mmol/l and the serum creatinine level was 145
μmol/l. Computed tomography (CT) revealed interstitial pneumonitis
(Fig. 2). Following admission to
the Department of Poisoning and Occupational Disease, the patient
underwent an urgent surgical debridement and rinse. The patient was
administered with 500 mg methylprednisolone per day by an
intravenous drip for three days followed by 200 mg intravenously
every day, and five days later the dosage of methylprednisolone was
gradually decreased according to the condition of the patient.
Cyclophosphamide (800 mg) was administered intravenously on the
first day and etanercept (25 mg) was administered by a hypodermic
injection twice a week for three weeks. Simultaneously, antibiotics
and nutrition were actively administered. By the time of discharge,
21 days later, the patient had recovered well. The burns on the
limbs had healed, with pigmentation and topical scar formation,
kidney function had recovered and the lung CT revealed no signs of
pulmonary fibrosis. A month later, the patient presented at the
hospital with herpes zoster on the right side of the back and
waist. The patient received vitamins B1 and B12 and antiviral
therapy and recovered 20 days later.
Case 2
A 55-year-old female presented at the Qilu Hospital
of Shandong University with 2% TBSA shallow second-degree chemical
burns on the lower limbs. The patient was a contractual worker
spraying paraquat in the orchard with the patient from Case 1 and
had also worked from 9:00 am to 12:00 am. Due to the high
temperature the upper and lower limbs of the patient were fully
exposed to the solution without any protection. Some solution
adhered to the skin of the patient, particularly on the lower
limbs. The patient did not wash the skin immediately. In the
afternoon, the skin coated by paraquat had developed erythema
followed by blistering. The patient was treated by a community
doctor for five days. Six days subsequent to the incident, the
condition of the patient deteriorated and the patient was sent to
Qilu Hospital of Shandong University. Upon examination, the
mentation of the patient was intact and the mental status was
normal. Physically, the patient had 2% TBSA shallow second-degree
chemical burns on the forearm and the surface of the lower limbs.
The skin was raw, macerated and oozing pus (Fig. 3). The heart, lungs and abdomen were
normal. The results of the routine blood tests and liver and kidney
functions were normal. The lung CT was also normal. Following
admission to the Qilu Hospital of Shandong University, the patient
underwent urgent surgical debridement. Methylprednisolone and
Levofloxacin (400mg ivdrip per day) were administered for 7 days.
Fifteen days later, the burns on the limbs of the patient had
healed with pigmentation formation.
Discussion
Paraquat is a commonly used non-selective herbicide
(12). According to the
International Program for Chemical Safety Classification System of
Pesticides by the World Health Organization (WHO), paraquat is
classified as ‘moderately hazardous’ (WHO class II) (13). The herbicide industry claims that
paraquat is safe if handled as instructed, yet paraquat poisoning
remains a severe health problem globally and the degree of the
severity depends on the exposure route and dose. In general, oral
ingestion of paraquat is fatal as it is acutely toxic to humans. As
a result, many accidental and suicidal deaths have been reported
(14–16). In 1978, a middle-aged female was
reported to have died from respiratory failure caused by
percutaneous paraquat absorption (7). This showed the extreme toxicity of
paraquat and demonstrated that lethal quantities may be absorbed
from apparently trivial skin wounds. In 1983, it was reported that
a patient whose scrotal skin had been exposed to a concentrated
paraquat solution suffered from renal and respiratory failure and
hepatic damage, although the patient eventually recovered. This
demonstrated that dermal exposure to paraquat, particularly via the
scrotum, may produce serious systemic toxicity (9). Data from the Israel Poison
Information Center regarding 15 cases of single exposure to the
skin or eyes during work with paraquat solutions revealed that a
single exposure of healthy skin to paraquat solutions caused local
lesions. No systemic effect was detected in these patients
(17). However, two males from
Israel were admitted to hospital for severe pain due to extensive
chemical burns in the perineal and scrotal regions, caused by
Ducatalon (a mixture of diquat and paraquat) leaking from defective
equipment used for spraying the herbicide (18). There has been a recent rise in case
reports regarding paraquat poisoning following dermal exposure
(19–21). In the two cases documented in this
case report, the high temperature and humidity together with the
lack of protection for the sprayers increased the risk of dermal
exposure. In Case 1, the paraquat entered the body through the
damaged skin and caused renal injury and pulmonary fibrosis. In
Case 2, the paraquat caused serious skin injuries similar to that
of Case 1.
One of our previous studies demonstrated that
methylprednisolone combined with cyclophosphamide and intensive
etanercept therapy has a curative effect on acute paraquat
poisoning (22).
Methythylprednisolone, cyclophosphamide and etanercept were used in
Case 1 and demonstrated a favorable curative effect. The occurrence
of herpes zoster may be associated with the administration of
immunosuppressive treatment. The patients eventually recovered
fully without any sequelae.
These cases suggest that paraquat is well absorbed
through abraded or injured skin and may result in severe toxicity.
Therefore, it is important to wash the contaminated skin, including
hair and nails, vigorously, with soap following dermal exposure to
paraquat. Broken skin should be treated for superficial burns
following a thorough cleansing. Stricter precautions, including the
mandatory use of protective clothing, should be recommended
whenever paraquat is used.
Acknowledgements
This study was supported by the Natural Science
Foundation of Shandong Province (grant no. Y2008C123).
References
|
1
|
Carson DJ and Carson ED: The increasing
use of paraquat as a suicidal agent. Forensic Sci. 7:151–160. 1976.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Huang CJ, Yang MC and Ueng SH: Subacute
pulmonary manifestation in a survivor of severe paraquat
intoxication. Am J Med Sci. 330:254–256. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sagar GR: Uses and usefulness of paraquat.
Hum Toxicol. 6:7–11. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Rhodes ML, Zavala DC and Brown D: Hypoxic
protection in paraquat poisoning. Lab Invest. 35:496–500.
1976.PubMed/NCBI
|
|
5
|
Rebello G and Mason JK: Pulmonary
histological appearances in fatal paraquat poisoning.
Histopathology. 2:53–66. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Dinis-Oliveira RJ, Sarmento A, Reis P, et
al: Acute paraquat poisoning: report of a survival case following
intake of a potential lethal dose. Pediatr Emerg Care. 22:537–540.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Newhouse M, McEvoy D and Rosenthal D:
Percutaneous paraquat absorption. An association with cutaneous
lesions and respiratory failure. Arch Dermatol. 114:1516–1519.
1978. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bismuth C, Garnier R, Dally S, et al:
Prognosis and treatment of paraquat poisoning: a review of 28
cases. J Toxicol Clin Toxicol. 19:461–474. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Tungsanga K, Chusilp S, Israsena S and
Sitprija V: Paraquat poisoning: evidence of systemic toxicity after
dermal exposure. Postgrad Med J. 59:338–339. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gear AJ, Ahrenholz DH and Solem LD:
Paraquat poisoning in a burn patient. J Burn Care Rehabil.
22:347–351. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ruan YJ, Jian XD and Guo GR: Progress in
research on mechanism of pathogenesis and treatment of acute
paraquat poisoning. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi.
27:114–116. 2009.(In Chinese).
|
|
12
|
Wesseling C, van Wendel de Joode B,
Ruepert C, et al: Paraquat in developing countries. Int J Occup
Environ Health. 7:275–286. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
WHO. The WHO Recommended Classification of
Pesticides by Hazard and Guidelines to Classification: 2004. World
Health Organization; Geneva, Switzerland: pp. 21–25. 2005
|
|
14
|
Sabzghabaee AM, Eizadi-Mood N, Montazeri
K, et al: Fatality in paraquat poisoning. Singapore Med J.
51:496–500. 2010.PubMed/NCBI
|
|
15
|
Gawarammana IB and Dawson AH: Peripheral
burning sensation: a novel clinical marker of poor prognosis and
higher plasma-paraquat concentrations in paraquat poisoning. Clin
Toxicol (Phila). 48:347–349. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chen JG, Eldridge DL, Lodeserto FJ, et al:
Paraquat ingestion: a challenging diagnosis. Pediatrics.
125:e1505–e1509. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hoffer E and Taitelman U: Exposure to
paraquat through skin absorption: clinical and laboratory
observations of accidental splashing on healthy skin of
agricultural workers. Hum Toxicol. 8:483–485. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ronnen M, Klin B and Suster S: Mixed
diquat/paraquat-induced burns. Int J Dermatol. 34:23–25. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Soloukides A, Moutzouris DA, Kassimatis T,
et al: A fatal case of paraquat poisoning following minimal dermal
exposure. Ren Fail. 29:375–377. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Peiró AM, Zapater P, Alenda C, et al:
Hepatotoxicity related to paraquat and diquat absorption through
intact skin. Dig Dis Sci. 52:3282–3284. 2007.PubMed/NCBI
|
|
21
|
Lin NC, Lin JL, Lin-Tan DT and Yu CC:
Combined initial cyclophosphamide with repeated methylprednisolone
pulse therapy for severe paraquat poisoning from dermal exposure. J
Toxicol Clin Toxicol. 41:877–881. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Jian XD, Guo GR, Ruan YJ, et al: Clinical
study on treatment of acute paraquat poisoning. Zhonghua Lao Dong
Wei Sheng Zhi Ye Bing Za Zhi. 26:549–552. 2008.PubMed/NCBI
|