1. Introduction
Spinal cord injury (SCI) typically results in a
permanent disability, which may be an economic burden on the family
of the patient and society, and to date there is no effective
method of treatment (1). Every
year there are 12,000 new cases of SCI in the USA, with the total
number of American individuals living with a SCI estimated at
~259,000 (2). The development of a
cure for SCI is a research topic of particular interest.
SCI triggers a series of pathological steps that
include the original insult and subsequent secondary steps, such as
ischemia, anoxia, free-radical formation and excitotoxicity
(3). The original insult refers to
the mechanical trauma that leads to the SCI. During this period,
the spinal cord tissue is disrupted by an external force, produced
by the original insult mechanism. The most recognized mechanism for
injury includes the following steps (4,5): i)
contusion of the spinal cord when injury occurs and ii) prolonged
compression due to displacement of vertebral bony structures and
tissues. Following the initial spinal cord trauma, secondary damage
is apparent. The post-trauma inflammatory response is particularly
significant and, through a series of complicated cellular and
molecular interactions, plays a key role in the entire secondary
phase following SCI (6,7).
Clinically, the treatment of SCI mainly focuses on
reducing secondary damage and the prevention of complications
(8). However, if the aim is to
successfully repair the SCI and promote functional recovery, the
following must be achieved (9,10):
i) reduction of the death of neuronal cells, ii) inhibition of
glial scar formation, since glial scarring decreases axon growth,
iii) provision of a matrix at the injury site to supply the
nutrients required to support axonal growth, iv) elimination of
immune reactions and v) facilitation of the build-up of functional
synapses and the transmission of neurotransmitters by regenerating
axons. The key to treatment is to establish axonal regeneration in
the damaged area with the anticipation that it will extend through
the damaged area to establish a connection with the target neurons
in the spinal cord. To date, it has been demonstrated that blocking
inhibitory molecules and antagonizing secondary injury mechanisms
promotes axon growth, by using trophic factors, cellular
transplants and polymeric scaffolds (11). However, no significant functional
recovery has been observed; therefore, a novel method is
required.
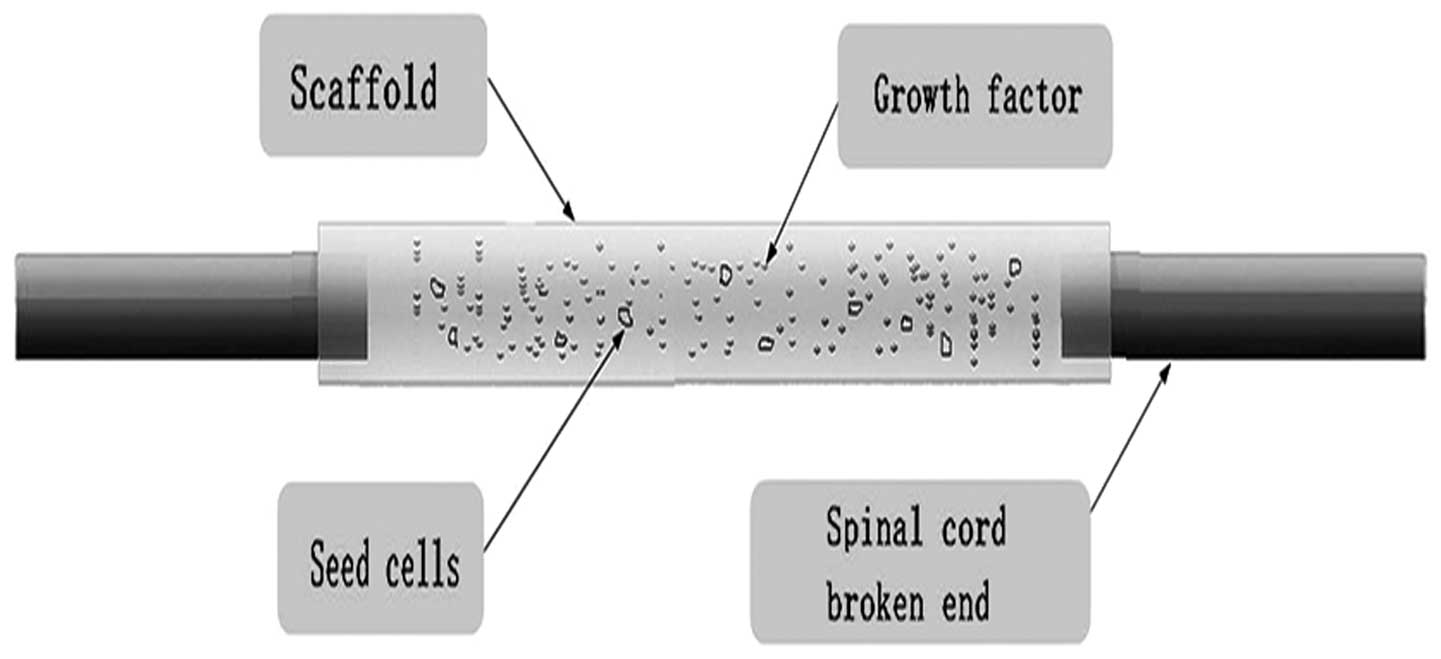
Tissue engineering is an emerging area in
biomaterial research that possesses great therapeutic potential.
However, in order for it to be used clinically there are challenges
that need to be overcome (12). In
recent years, studies have begun to explore the possibility of
using tissue engineering technology to repair SCIs, specifically,
by using seed cells, neurotropic factors and a biological scaffold
(Fig. 1). The aim of this review
is to discuss this tissue engineering method and investigate the
hypothesis that, if a suitable seed cell, scaffold and growth
factor are identified, tissue engineering offers bright prospects
for future research and the potential for clinical use.
2. Seed cell
The basis for tissue engineering is the seed cell,
which is also the bottleneck that has been restricting the
development of tissue engineering. The main reason for this is that
certain cells, such as cartilage cells and endothelial cells, are
limited and it is not possible to construct a large organization
through small quantities of tissues in vitro (13). In general, tissue engineering seed
cells must meet the following criteria (14,15):
i) successful ability to proliferation in vitro, ii) good
cell viability and function, iii) high level of purity, iv) no
rejection by the immune system and v) high safety. With the
continuous development of tissue engineering, stem cells, including
embryonic stem (ES) cells, and adult stem cells are gradually
entering the seed cell field, with many advantages, including wide
availability, a strong ability to proliferate, the ability to
differentiate into a variety of cells and the ability to form the
corresponding organization. At present there are clinical problems
with using seed cells, the selection of a suitable seed cell may
resolve this problem (16).
ES cells and neural stem cells are the most
important types of stem cell that were used in the early stages of
seed cell research (17,18). Transplanting ES cells into the
brain was shown to significantly improve neurological function in
an animal model of Parkinson’s disease (19). The reason for this success is that
the cells survived and were differentiated into different cells,
such as oligodendrocytes, astrocytes and neurons. However, this
method has certain ethical issues and problems with regard to
rejection reactions (20). In
addition, the availability of neural stem cells is limited and,
therefore, their widespread clinical use is not viable (21). With advances in stem cell research,
mesenchymal stem cells (MSCs) extracted from bone marrow (BMSCs)
have been shown to contain pluripotent precursor cells, which have
the ability to differentiate into various types of brain cell
(22). In vivo
transplantation of BMSCs into the brain has established that they
migrate throughout various brain regions where they undergo
differentiation into cells with astrocytic and neuronal phenotypes
(23). However, if BMSCs are to be
used clinically, the extraction of bone marrow from patients is
necessary, which is likely to result in patient trauma. Therefore,
an increasing number of studies have suggested the use of adult
stem cells, which have all the advantages of BMSCs, but without the
need to induce trauma in the patients in order to extract them.
Muscle-derived stem cells (MPSCs) are adult stem
cells, commonly used in tissue engineering. Alessandri et al
(24), have demonstrated that
adult human skeletal muscle includes a population of progenitor
stem cells capable of generating cells of the same lineage and have
suggested that MPSCs are ideal seed cells. Lavasani et al
(25) and Wu et al
(26) have shown that MPSCs have
the ability to differentiate into various cell types when placed
within specialized inducing media. Danisovic et al (27,28)
focused on the immunological properties of MPSCs and hypothesized
that their potential for differentiation may be useful in cell
therapy for a variety of degenerative diseases. However, the
majority of studies have investigated the use of MPSCs to cure
coronary and urological diseases, with a limited number using MPSCs
to repair nerve injuries. Woo et al (29) transplanted MDSCs into a cavernous
nerve injury in a rat model, the result of which demonstrated that
MDSCs were capable of improving erectile function. Stulpinas et
al (30) and Shibuya et
al (31) investigated the
potential use of MPSCs in the treatment of non-acute myocardial
infarction, with a swifter recovery. Kwon et al (32,33)
found that although MPSCs are a good seed cell, capable of
differentiating into numerous cell types, the neural
differentiation capacity of MDSCs is less than that of
adipose-derived stem cells (ADSCs). Therefore, ADSCs may be the
most suitable type of adult stem cell for use as seed cells in SCI
treatment.
Adipose tissue is abundant in the body. Zuk
(34) extracted cells from adipose
tissue and observed that the morphology, biological characteristics
and immune phenotypes of the cells were similar to those of BMSCs.
An advantage of using ADSCs is that obtaining these cells is
minimally invasive to the patient. If different types of induction
medium are used, the cells may differentiate into adipocytes,
osteoblasts, chondrocytes and neurons, which are the most common
types of seed cells currently used in research, and represent a
promising tool for SCI treatment (35–38).
Recently, studies have shown that due to the secretion of various
growth factors, such as hepatocyte growth factor (HGF), tumor
necrosis factor-α (TNF-α), vascular endothelial growth factor
(VEGF), brain-derived neurotropic factor (BDNF) and nerve growth
factor (NGF), ADSCs may be used in the acute stages of SCI and have
the potential to improve functional recovery, tissue preservation
and neuronal regeneration (39–41).
Oh et al (42) used ADSCs
to treat SCI and observed functional improvements. Similar results
were demonstrated by Barriga et al (43), Ferrero-Gutierrez et al
(44) and Chung et al
(45). Therefore, this type of
stem cell may be considered to be the most suitable for use as a
seed cell for the treatment of SCI.
3. Scaffold
Maintaining cell growth is challenging if the cells
are injected directly into the damaged area. Opening the meninges
may lead to cell loss, which is likely to inhibit the ability of
the cells to adhere to the damaged tissues and proliferate.
Therefore, in addition to seed cells, tissue-engineering scaffolds
are also important and their potential use in the repair of the
spinal has been the subject of study for several years (46).
The requirements of a scaffold for spinal cord
regeneration are as follows (47,48):
i) good biocompatibility, in order to avoid reactions with the
immune system, ii) an ideal degradation rate and the formation of
non-toxic degradation products, and iii) mechanical properties that
are suitable for cell adhesion and axonal regrowth. There have been
several studies that have concentrated on the microstructural
design of porous scaffolds, which must be conditioned in
vivo prior to implantation (49,50).
However, this has the major disadvantage of increasing the
difficulty of the design at the engineering level and surgical
implantation may also be challenging. The best solution is to
create a scaffold with a simpler design, that is easier to
transplant and is suitable for various types of injury (51,52).
Silk fibroin (SF) is obtained by degumming silk and
acts as a natural structural albumen without physiological
activity. It mainly consists of three simple amino acids: glycine,
alanine and serine, which account for 85% of the total protein.
Furthermore, SF has excellent mechanical properties, good
compatibility and induces only a slight inflammation reaction in
vivo. SF has been used as a scaffold for the treatment of SCI
in certain experiments, but the disadvantage of this material is
that when it is dry it is particularly brittle and difficult to
handle (53). Therefore, in order
to overcome this shortcoming, another polymer, chitosan, is added
to the SF formulation. Chitosan has been investigated for its
biocompatibility, biodegradability and toxicity in tissue
engineering for several years, despite the disadvantages that it
degrades rapidly and has a high swelling property (54,55).
Therefore, a blend of both materials to make silk fibroin-chitosan
(SFCS) may avoid the limitations of pure SF and CS. Furthermore,
the blend has good mechanical properties and may be used as a
scaffold material for the repair of SCIs (56,57).
In addition to SFCS scaffolds derived from natural
components, injectable scaffolds are also particularly important
for tissue engineering, as they are capable of filling the damaged
site and may be delivered using a minimally invasive method
(58). This type of scaffold also
possesses the ability to mold to irregularly shaped damaged sites.
Comolli et al (59) used a
poly(N-isopropylacrylamide)-co-poly(ethylene glycol) (PNIPAAm-PEG)
injection scaffold, which provided the sustained release of BDNF
and neurotrophin-3 (NT-3) for up to four weeks; the constant
secretion of these growth factors was identified to be a positive
factor in functional recovery. However, the majority of these
scaffolds require gelation (crosslinking) in vivo, which may
result in complications, either from unreacted monomers or excess
reactant (60).
Further to the two previously discussed types of
scaffold, other scaffolds have been used successfully in the
treatment of SCI. Kang et al (61) used poly (D,L-lactide-co-glycolide)
to successfully treat transected spinal cords in rats; a certain
degree of nerve regeneration and functional recovery was observed.
A study by Liu et al (62)
using nanofibrous collagen nerve conduits demonstrated that this
type of scaffold is capable of promoting neural fiber growth
following SCI, and is also capable of inhibiting glial scar
hyperplasia. Zhu et al (63) used nanofibrous scaffolds as a drug
delivery vehicle for the treatment of SCI in rats, and observed
significant improvements in hindlimb function after three weeks.
Teng et al (64) studied
the use of a poly(lactic-co-glycolic acid) (PLGA) scaffold to treat
SCI in rats. The authors identified that corticospinal tract fibers
permeated the epicenter of the injury to the caudal cord and that
local GAP-43 expression was increased, which lead them to
hypothesize that PLGA increases the possibility of recovery
following SCI. However, in contrast to the findings of Teng et
al, a study by Du et al (65) demonstrated that a gelatin sponge is
more suitable than a PLGA scaffold for transplantation into the
spinal cord to promote the recovery of SCI.
In order to successfully use tissue engineering to
repair SCI, the selection of a suitable scaffold is particularly
important. Compared with a single component scaffold, a mixed
scaffold (comprising several ingredients) may be more successful as
it may minimize the disadvantages of the single component scaffold
and provide a scaffold with increased functionality. Furthermore,
compared with synthetic scaffolds, scaffolds prepared from natural
components may be more advantageous, as the reaction of the immune
system and the inflammatory reaction is reduced following
implantation into the body.
4. Growth factor
Neurotrophic factors play an important role in
functional recovery following SCI, as they protect neuronal cells
from apoptosis and promote axonal regeneration (66). Neurotrophic factors may be divided
into neurotrophins, ciliary neurotropic factor, the glial cell
line-derived neurotrophic factor family and other growth factors or
cytokines (67–69). The most frequently used
neurotrophic factors are NGF, NT-3 and BDNF. NGF was discovered in
1950 and, as a core factor in the regulation of peripheral
innervations, was found to have an effect on the CNS (70). Allen et al (71) demonstrated that NGF has a promising
future as a therapeutic option for neurodegeneration. Weishaupt
et al (72,73) extracted BDNF from a porcine brain
and identified that it had a broad-spectrum effect on peripheral
and central neurons, with the exception of the ciliary ganglion
neurons, sensory neurons, hippocampal neurons, cerebellar neurons,
motor neurons, cholinergic neurons of the basal forebrain and
midbrain dopaminergic neurons. BDNF expresses its biological
effects through the activation and binding of TrkB (74). Stokols et al (75) discovered that a BDNF-incorporated
agarose scaffold implanted into the spinal cord of a rat resulted
in the linear-fashioned growth of regenerating axons through the
scaffold. NT-3, which may be generated by the cloning of a
multifunctional NGF gene, not only maintains motor neurons,
sympathetic neurons and dopaminergic neuron differentiation, but
also maintains the survival of sympathetic and sensory neurons and
promotes nerve outgrowth in vitro (76,77).
To date, NT-3 is considered to be the only gene to promote the
growth of the corticospinal tract (CST) following SCI. The
biological effect of NT-3 is produced by the binding and activation
of TrkC; NT-3 also has effects on TrkA and TrkB, but these are weak
(78,79).
Neurotrophic factors may be applied by the following
three methods: local injection, cerebrospinal fluid injection and
gene modification (80). Of these
methods, the most important is gene modification. Studies have
shown that the direct injection of neurotrophins into the site of
injury results in an improved functional recovery compared with
that in a control group to which growth factor is not administered;
however, due to several factors, such as concentration, time
limitation, and a short half-life, this treatment was unable to
fully meet the requirements for nerve regeneration (81,82).
Cerebrospinal fluid injection has certain disadvantages, including
the fact that it is not possible to restrict the location of the
neurotrophic factor to the injury site, and recovery is less
successful compared with that achieved using other methods.
Therefore, an increasing number of researchers are focusing on gene
modification (79).
There are two methods of applying gene therapy for
the treatment of SCI (83–85): the direct transfer of the gene into
the target cells in the human body, and cell-mediated gene therapy.
The latter method, which requires the target gene to be transferred
into an appropriate transplant cell, the selection of cells with a
high level of gene expression, and the transplantation of the cells
into the target tissue, is the most commonly used. Researchers have
used transgenic technology to modify fibroblast cells, muscle cells
and Schwann cells, which are subsequently transplanted into the
injured area. The genetically modified cells may continue to
express nutritional factor, the purpose of which is to promote
nerve regeneration. Gene transfer vectors are divided into viral
vectors and non-viral vectors (86). Viral vectors include adenoviruses,
retroviruses and chronic viruses; retroviruses and chronic viruses
are of particular interest as their transfer into the host genome
may lead to long-term expression (87–89);
Morizono and Chen (89) compared
the efficiencies of three types of virus for the transfection of
ADSCs, and observed that the highest transfection efficiency was
achieved with a chronic virus. When an exogenous gene was
transferred by chronic virus carriers into adipose stem cells,
which were then induced in vitro, detection of the gene
remained possible following osteogenic and adipogenic
differentiation. Therefore, the combination of stem cells and
chronic virus carriers is currently being studied (89). However, the clinical application
may be simpler if growth factors are slowly released from
scaffolds, rather than being delivered by gene transfer, using
biomaterials that are capable of providing the protracted release
of loaded proteins.
5. Conclusion
Tissue engineering is a promising method that may be
used for the treatment of SCI. It involves three factors: the seed
cell, the scaffold and a growth factor. For the repair strategy to
be successful, the selection of an appropriate seed cell, scaffold
and growth factor is required. Considering the seed cell, adult
stem cells, particularly stem cells derived from adipose tissue,
appear to be more suitable than fibroblasts, neuronal stem cells
and ES cells. For the scaffold, scaffolds formed from natural
components are more advantageous than scaffolds composed of
artificial and synthetic materials. However, the blending of
natural and synthetic materials may reduce the disadvantages of
using synthetic material while also avoiding the disadvantages of
using solely natural components. The growth factor is important as
it enhances the repairing effect, particularly when the virus
carrier used to transfect the stem cells enables the consistent
expression of the growth factor gene. We hypothesize that the use
of a combination of growth factors may be more effective than the
use of a single growth factor. Therefore, the construction of a
virus capable of carrying several genes together requires further
study. In conclusion, although tissue engineering has a promising
future for the treatment of SCI, extensive further studies are
necessary for the successful treatment of SCI to be achieved.
Acknowledgements
The authors are grateful to Ying Mao for the
guidance provided while writing this review.
References
|
1
|
Findley PA, Banerjea R and Sambamoorthi U:
Excess mortality associated with mental illness and substance use
disorders among veteran clinic users with spinal cord injury.
Disabil Rehabil. 33:1608–1615. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wang M, Zhai P, Chen X, Schreyer DJ, Sun X
and Cui F: Bioengineered scaffolds for spinal cord repair. Tissue
Eng Part B Rev. 17:177–194. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hulsebosch CE: Recent advances in
pathophysiology and treatment of spinal cord injury. Adv Physiol
Educ. 26:238–255. 2002.PubMed/NCBI
|
|
4
|
Baumgaertner W, Spitzbarth I and Beineke
A: New knowledge on the pathology of spinal cord disease in dogs -
views on therapy. Praktische Tierarzt. 93:794–796. 2012.
|
|
5
|
Wasner G: Spinal cord injury pain - from
symptom to pathology. In: Proceedings of the 3rd International
Congress on Neuropathic Pain (NeuPSIG); Medimond, Bologna. pp.
107–111. 2010
|
|
6
|
Shimizu H, Kakita A and Takahashi H:
Spinal cord tau pathology in cervical spondylotic myelopathy. Acta
Neuropathol. 115:185–192. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Norenberg MD, Smith J and Marcillo A: The
pathology of human spinal cord injury: defining the problems. J
Neurotrauma. 21:429–440. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Banerjea R, Findley PA, Smith B, Findley T
and Sambamoorthi U: Co-occurring medical and mental illness and
substance use disorders among veteran clinic users with spinal cord
injury patients with complexities. Spinal Cord. 47:789–795. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
May L, Day R and Warren S: Evaluation of
patient education in spinal cord injury rehabilitation: knowledge,
problem-solving and perceived importance. Disabil Rehabil.
28:405–413. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cruz CD and Cruz F: Spinal cord injury and
bladder dysfunction: new ideas about an old problem.
ScientificWorldJournal. 11:214–234. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Qu WS, Tian DS, GUO ZB, et al: Inhibition
of EGFR/MAPK signaling reduces microglial inflammatory response and
the associated secondary damage in rats after spinal cord injury. J
Neuroinflammation. 9:1782012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Madigan NN, McMahon S, O’Brien T,
Yaszemski MJ and Windebank AJ: Current tissue engineering and novel
therapeutic approaches to axonal regeneration following spinal cord
injury using polymer scaffolds. Respir Physiol Neurobiol.
169:183–199. 2009. View Article : Google Scholar
|
|
13
|
Hernandez J, Torres-Espín A and Navarro X:
Adult stem cell transplants for spinal cord injury repair: current
state in preclinical research. Curr Stem Cell Res Ther. 6:273–287.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
He X, Fu W and Zheng J: Cell sources for
trachea tissue engineering: past, present and future. Regen Med.
7:851–863. 2012.PubMed/NCBI
|
|
15
|
Malik A and Khan W: Stem cell therapy and
tissue engineering applications for bone. Curr Stem Cell Res Ther.
8:183–184. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Khan WS and Malik A: Stem cell therapy and
tissue engineering applications for cartilage regeneration. Curr
Stem Cell Res Ther. 7:241–242. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Salehi M, Pasbakhsh P, Soleimani M, et al:
Repair of spinal cord injury by co-transplantation of embryonic
stem cell-derived motor neuron and olfactory ensheathing cell. Iran
Biomed J. 13:125–135. 2009.
|
|
18
|
Wilcock AC, Swedlow JR and Storey KG:
Mitotic spindle orientation distinguishes stem cell and terminal
modes of neuron production in the early spinal cord. Development.
134:1943–1954. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Daadi MM, Grueter BA, Malenka RC, Redmond
DE Jr and Steinberg GK: Dopaminergic neurons from
midbrain-specified human embryonic stem cell-derived neural stem
cells engrafted in a monkey model of Parkinson’s disease. PLoS One.
7:e411202012.PubMed/NCBI
|
|
20
|
Meamar R, Dehghani L and Karamali F:
Toxicity effects of methamphetamine on embryonic stem cell-derived
neuron. J Res Med Sci. 17:470–474. 2012.PubMed/NCBI
|
|
21
|
Tavares I: Human neural stem cell
transplantation in spinal cord injury models: how far from clinical
application? Stem Cell Res Ther. 4:612013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Deda H, Inci MC, Kurekci AE, et al:
Treatment of chronic spinal cord injured patients with autologous
bone marrow-derived hematopoietic stem cell transplantation: 1-year
follow-up. Cytotherapy. 10:565–574. 2008.PubMed/NCBI
|
|
23
|
Kim JW, Ha KY, Molon JN and Kim YH: Bone
marrow-derived mesenchymal stem cell transplantation for chronic
spinal cord injury in rats: comparative study between intralesional
and intravenous transplantation. Spine (Phila Pa 1976).
38:E1065–E1074. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Alessandri G, Pagano S, Bez A, et al:
Isolation and culture of human muscle-derived stem cells able to
differentiate into myogenic and neurogenic cell lineages. Lancet.
364:1872–1883. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lavasani M, Lu A, Thompson SD, Robbins PD,
Huard J and Niedernhofer LJ: Isolation of muscle-derived
stem/progenitor cells based on adhesion characteristics to
collagen-coated surfaces. Methods Mol Biol. 976:53–65. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Wu X, Wang S, Chen B and An X:
Muscle-derived stem cells: isolation, characterization,
differentiation, and application in cell and gene therapy. Cell
Tissue Res. 340:549–567. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Danisovic L, Varga I, Polák S, Bajciková
B, Adamkov M and Vojtassák J: Biological and morphological
characterization of in vitro expanded human muscle-derived stem
cells. Tsitologiia. 53:482–487. 2011.PubMed/NCBI
|
|
28
|
Danisovic L, Varga I, Polák S, Ulicna M,
Bohmer D and Vojtassák J: Morphology of in vitro expanded human
muscle-derived stem cells. Biomed Pap Med Fac Univ Palacky Olomouc
Czech Repub. 152:235–238. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Woo JC, Bae WJ, Kim SJ, et al:
Transplantation of muscle-derived stem cells into the corpus
cavernosum restores erectile function in a rat model of
cavernous nerve injury. Korean J Urol. 52:359–363. 2011.PubMed/NCBI
|
|
30
|
Stulpinas A, Imbrasaité A and Kalvelyté
AV: Daunorubicin induces cell death via activation of apoptotic
signalling pathway and inactivation of survival pathway in
muscle-derived stem cells. Cell Biol Toxicol. 28:103–114. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Shibuya M, Miura T, Fukagawa Y, et al:
Tongue muscle-derived stem cells express connexin 43 and improve
cardiac remodeling and survival after myocardial infarction in
mice. Circ J. 74:1219–1226. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Kwon EB and Lee JY, Piao S, Kim IG, Ra JC
and Lee JY: Comparison of human muscle-derived stem cells and human
adipose-derived stem cells in neurogenic trans-differentiation.
Korean J Urol. 52:852–857. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kwon JS, Kim GH, Kim da Y, et al:
Chitosan-based hydrogels to induce neuronal differentiation of rat
muscle-derived stem cells. Int J Biol Macromol. 51:974–979. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Zuk PA: The adipose-derived stem cell:
looking back and looking ahead. Mol Biol Cell. 21:1783–1787. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Wilson B, Liotta LA and Petricoin EF:
Dynamic protein pathway activation mapping of adipose-derived stem
cell differentiation implicates novel regulators of adipocyte
differentiation. Mol Cell Proteomics. 12:2522–2535. 2013.
View Article : Google Scholar
|
|
36
|
Su SJ, Chang KL, Su SH, Yeh YT, Shyu HW
and Chen KM: Caffeine regulates osteogenic differentiation and
mineralization of primary adipose-derived stem cells and a bone
marrow stromal cell line. Int J Food Sci Nutr. 64:429–436. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Merceron C, Portron S, Masson M, et al:
The effect of two- and three-dimensional cell culture on the
chondrogenic potential of human adipose-derived mesenchymal stem
cells after subcutaneous transplantation with an injectable
hydrogel. Cell Transplant. 20:1575–1588. 2011. View Article : Google Scholar
|
|
38
|
Liqing Y, Jia G, Jiqing C, et al: Directed
differentiation of motor neuron cell-like cells from human
adipose-derived stem cells in vitro. Neuroreport. 22:370–373. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Valenzuela CD, Allori AC, Reformat DD, et
al: Characterization of adipose-derived mesenchymal stem cell
combinations for vascularized bone engineering. Tissue Eng Part A.
19:1373–1385. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Kleintjes WG: Treatment of basal cell
carcinoma with autogenous growth factors and adipose-derived stem
cells. Plast Reconstr Surg. 126:312e–313e. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Sterodimas A, de Faria J, Nicaretta B and
Pitanguy I: Tissue engineering with adipose-derived stem cells
(ADSCs): current and future applications. J Plast Reconstr Aesthet
Surg. 63:1886–1892. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Oh JS, Park IS, Kim KN, Yoon do H, Kim SH
and Ha Y: Transplantation of an adipose stem cell cluster in a
spinal cord injury. Neuroreport. 23:277–282. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Barriga A, Medrano M, De-Juan J and Burgos
J: Intravenous infusion of adult adipose tissue stem cells for
repairing spinal cord ischaemic lesions. An experimental study on
animals. Rev Esp Cir Ortop Traumatol. 57:89–94. 2013.(In
Spanish).
|
|
44
|
Ferrero-Gutierrez A, Menendez-Menendez Y,
Alvarez-Viejo M, Meana A and Otero J: New serum-derived albumin
scaffold seeded with adipose-derived stem cells and olfactory
ensheathing cells used to treat spinal cord injured rats. Histol
Histopathol. 28:89–100. 2013.
|
|
45
|
Chung JY, Kim W, Im W, et al:
Neuroprotective effects of adipose-derived stem cells against
ischemic neuronal damage in the rabbit spinal cord. J Neurol Sci.
317:40–46. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Barry DS, Pakan JM, O’Keeffe GW and
McDermott KW: The spatial and temporal arrangement of the radial
glial scaffold suggests a role in axon tract formation in the
developing spinal cord. J Anat. 222:203–213. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Roberts A, Li WC and Soffe SR: A
functional scaffold of CNS neurons for the vertebrates: the
developing Xenopus laevis spinal cord. Dev Neurobiol.
72:575–584. 2012. View Article : Google Scholar
|
|
48
|
Yoshii S, Ito S, Shima M, Taniguchi A and
Akagi M: Functional restoration of rabbit spinal cord using
collagen-filament scaffold. J Tissue Eng Regen Med. 3:19–25. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Ellis-Behnke RG and Schneider GE: Peptide
amphiphiles and porous biodegradable scaffolds for tissue
regeneration in the brain and spinal cord. Methods Mol Biol.
726:259–281. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Stokols S and Tuszynski MH: Freeze-dried
agarose scaffolds with uniaxial channels stimulate and guide linear
axonal growth following spinal cord injury. Biomaterials.
27:443–451. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Guo SZ, Ren XJ, Wu B and Jiang T:
Preparation of the acellular scaffold of the spinal cord and the
study of biocompatibility. Spinal Cord. 48:576–581. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Silva NA, Salgado AJ, Sousa RA, et al:
Development and characterization of a novel hybrid tissue
engineering-based scaffold for spinal cord injury repair. Tissue
Eng Part A. 16:45–54. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Chung TW and Chang YL: Silk
fibroin/chitosan-hyaluronic acid versus silk fibroin scaffolds for
tissue engineering: promoting cell proliferations in vitro. J Mater
Sci Mater Med. 21:1343–1351. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Hilmi AB, Halim AS, Hassan A, Lim CK,
Noorsal K and Zainol I: In vitro characterization of a chitosan
skin regenerating template as a scaffold for cells cultivation.
Springerplus. 2:792013. View Article : Google Scholar
|
|
55
|
Guan L, Tian P, Ge H, et al:
Chitosan-functionalized silk fibroin 3D scaffold for keratocyte
culture. J Mol Histol. May 1–2013.(Epub ahead of print).
|
|
56
|
She Z, Liu W and Feng Q: Self-assembly
model, hepatocytes attachment and inflammatory response for silk
fibroin/chitosan scaffolds. Biomed Mater. 4:0450142009. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
She Z, Jin C, Huang Z, Zhang B, Feng Q and
Xu Y: Silk fibroin/chitosan scaffold: preparation,
characterization, and culture with HepG2 cell. J Mater Sci Mater
Med. 19:3545–3553. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Cigognini D, Satta A, Colleoni B, et al:
Evaluation of early and late effects into the acute spinal cord
injury of an injectable functionalized self-assembling scaffold.
PLoS One. 6:e197822011. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Comolli N, Neuhuber B, Fischer I and
Lowman A: In vitro analysis of PNIPAAm-PEG, a novel, injectable
scaffold for spinal cord repair. Acta Biomater. 5:1046–1055. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Kubinová S, Horák D, Hejčl A, et al:
SIKVAV-modified highly superporous PHEMA scaffolds with oriented
pores for spinal cord injury repair. J Tissue Eng Regen Med.
February 11–2013.(Epub ahead of print).
|
|
61
|
Kang KN, Lee JY, Kim da Y, et al:
Regeneration of completely transected spinal cord using scaffold of
poly(D,L-lactide-coglycolide)/small intestinal submucosa seeded
with rat bone marrow stem cells. Tissue Eng Part A. 17:2143–2152.
2011. View Article : Google Scholar
|
|
62
|
Liu T, Houle JD, Xu J, Chan BP and Chew
SY: Nanofibrous collagen nerve conduits for spinal cord repair.
Tissue Eng Part A. 18:1057–1066. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Zhu Y, Wang A, Shen W, et al: Nanofibrous
patches for spinal cord regeneration. Adv Funct Mater.
20:1433–1440. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Teng YD, Lavik EB, Qu X, et al: Functional
recovery following traumatic spinal cord injury mediated by a
unique polymer scaffold seeded with neural stem cells. Proc Natl
Acad Sci USA. 99:3024–3029. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Du BL, Zeng CG, Zhang W, Quan DP, Ling EA
and Zeng YS: A comparative study of gelatin sponge scaffolds and
PLGA scaffolds transplanted to completely transected spinal cord of
rat. J Biomed Mater Res A. June 15–2013.(Epub ahead of print).
|
|
66
|
McCall J, Weidner N and Blesch A:
Neurotrophic factors in combinatorial approaches for spinal cord
regeneration. Cell Tissue Res. 349:27–37. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
de Leon RD: Could neurotrophins replace
treadmill training as locomotor therapy following spinal cord
injury? Focus on ‘neurotrophic factors promote and enhance
locomotor recovery in untrained spinalized cats’. J Neurophysiol.
98:1845–1846. 2007.PubMed/NCBI
|
|
68
|
Sharma HS: Neurotrophic factors in
combination: a possible new therapeutic strategy to influence
pathophysiology of spinal cord injury and repair mechanisms. Curr
Pharm Des. 13:1841–1874. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Sharma HS and Sharma A: Rodent spinal cord
injury model and application of neurotrophic factors for
neuroprotection. Methods Mol Biol. 846:393–415. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Berry A, Bindocci E and Alleva E: NGF,
brain and behavioral plasticity. Neural Plast.
2012:7840402012.PubMed/NCBI
|
|
71
|
Allen SJ, Watson JJ, Shoemark DK, Barua NU
and Patel NK: GDNF, NGF and BDNF as therapeutic options for
neurodegeneration. Pharmacol Ther. 138:155–175. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Weishaupt N, Blesch A and Fouad K: BDNF:
the career of a multifaceted neurotrophin in spinal cord injury.
Exp Neurol. 238:254–264. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Weishaupt N, Li S, Di Pardo A, Sipione S
and Fouad K: Synergistic effects of BDNF and rehabilitative
training on recovery after cervical spinal cord injury. Behav Brain
Res. 239:31–42. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Mantilla CB, Gransee HM, Zhan WZ and Sieck
GC: Motoneuron BDNF/TrkB signaling enhances functional recovery
after cervical spinal cord injury. Exp Neurol. 247:101–109. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Stokols S, Sakamoto J, Breckon C, Holt T,
Weiss J and Tuszynski MH: Templated agarose scaffolds support
linear axonal regeneration. Tissue Eng. 12:2777–2787. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Shang AJ, Hong SQ, Xu Q, et al:
NT-3-secreting human umbilical cord mesenchymal stromal cell
transplantation for the treatment of acute spinal cord injury in
rats. Brain Res. 1391:102–113. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Shumsky JS, Tobias CA, Tumolo M, Long WD,
Giszter SF and Murray M: Delayed transplantation of fibroblasts
genetically modified to secrete BDNF and NT-3 into a spinal cord
injury site is associated with limited recovery of function. Exp
Neurol. 184:114–130. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Chen Q, Smith GM and Shine HD: Immune
activation is required for NT-3-induced axonal plasticity in
chronic spinal cord injury. Exp Neurol. 209:497–509. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Guo JS, Zeng YS, Li HB, et al:
Cotransplant of neural stem cells and NT-3 gene modified Schwann
cells promote the recovery of transected spinal cord injury. Spinal
Cord. 45:15–24. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Wang X, Li Y, Gao Y, et al: Combined use
of spinal cord-mimicking partition type scaffold architecture and
neurotrophin-3 for surgical repair of completely transected spinal
cord in rats. J Biomater Sci Polym Ed. 24:927–939. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Hara T, Fukumitsu H, Soumiya H, Furukawa Y
and Furukawa S: Injury-induced accumulation of glial cell
line-derived neurotrophic factor in the rostral part of the injured
rat spinal cord. Int J Mol Sci. 13:13484–13500. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Lin S, Wang Y, Zhang C and Xu J:
Modification of the neurotrophin-3 gene promotes cholinergic
neuronal differentiation and survival of neural stem cells derived
from rat embryonic spinal cord in vitro and in vivo. J Int Med Res.
40:1449–1458. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Yao L, Yao S, Daly W, Hendry W, Windebank
A and Pandit A: Non-viral gene therapy for spinal cord
regeneration. Drug Discov Today. 17:998–1005. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Bo X, Wu D, Yeh J and Zhang Y: Gene
therapy approaches for neuroprotection and axonal regeneration
after spinal cord and spinal root injury. Curr Gene Ther.
11:101–115. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Blesch A, Fischer I and Tuszynski MH: Gene
therapy, neurotrophic factors and spinal cord regeneration. Handb
Clin Neurol. 109:563–574. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Foust KD, Flotte TR, Reier PJ and Mandel
RJ: Recombinant adeno-associated virus-mediated global anterograde
delivery of glial cell line-derived neurotrophic factor to the
spinal cord: comparison of rubrospinal and corticospinal tracts in
the rat. Hum Gene Ther. 19:71–82. 2008. View Article : Google Scholar
|
|
87
|
Koda M, Hashimoto M, Murakami M, et al:
Adenovirus vector-mediated in vivo gene transfer of brain-derived
neurotrophic factor (BDNF) promotes rubrospinal axonal regeneration
and functional recovery after complete transection of the adult rat
spinal cord. J Neurotrauma. 21:329–337. 2004. View Article : Google Scholar
|
|
88
|
Blits B, Kitay BM, Farahvar A, Caperton
CV, Dietrich WD and Bunge MB: Lentiviral vector-mediated
transduction of neural progenitor cells before implantation into
injured spinal cord and brain to detect their migration, deliver
neurotrophic factors and repair tissue. Restor Neurol Neurosci.
23:313–324. 2005.
|
|
89
|
Morizono K and Chen IS: Targeted gene
delivery by intravenous injection of retroviral vectors. Cell
Cycle. 4:854–856. 2005. View Article : Google Scholar : PubMed/NCBI
|