Introduction
Epilepsy is a frequently occurring neurological
condition resulting from the sudden discharge of brain neurons. It
is the most common serious neurological disorder globally, and
adversely affects social, vocational and psychological functioning
(1). The prevalence of epilepsy in
developed countries ranges from 4 to 10 cases per 1,000 (2). Approximately two-thirds of patients
with epilepsy will achieve a seizure-free status with antiepileptic
medications; however, one-third of cases are intractable to
antiepileptic drugs (AEDs) and therefore require surgical
intervention (3). However,
surgical treatment fails to provide a seizure-free outcome in
20–30% of patients with temporal lobe epilepsy (TLE) (4). Patients with bitemporal lobe
epileptogenic foci are representative of poor candidates for
resective surgery due to the difficulty of achieving a favorable
outcome (5–7). Independent bitemporal seizure onset
is largely assessed using electroencephalography monitoring, which
is limited by its duration. The number of seizure recordings
required to assure unilateral seizure onset is debatable, and
depends on the proportion of seizures from each temporal lobe and
the tendency of seizures to cluster from one temporal lobe as a
result of a short interseizure interval or other such factors
(8–12). In the present study, a rare case of
a patient with bitemporal lobe epilepsy, who received unilateral
standard temporal lobectomy, is described. In addition, the
possible pathogenesis of bitemporal lobe epilepsy is discussed. The
present study was approved by the ethics committee of Dalian
Medical University (Dalian, China; number 2013-002-08). Informed
consent was obtained from all patients.
Case report
A 27-year-old, right-handed female who had suffered
from recurrent seizures since the age of 11 was referred to the
Epileptic Center of Liaoning (The Second Affiliated Hospital of
Dalian Medical University) for medically refractory epilepsy. The
patient had tried almost all types of AEDs, yet none of them were
capable of controlling the seizures. The patient had experienced
two types of seizure attacks: One was characterized by a paroxysmal
loss of consciousness followed by automatic movements, such as
gazing eyes, a sudden halting of action, swallowing or lip
smacking, with the symptoms taking ~1 min to ease; the other type
also began with an impairment of consciousness, yet evolved into a
generalized tonic-clonic seizure (GTCS), which was characterized by
the head and eyes deviating to the left side, drooling and limb
flexing, shaking and stiffening, which was sustained for 4–5 min
and was usually followed by some sleep. Initially, the two types of
seizures occurred three to four times; however, this gradually
increased to eight to nine times per month. The patient was born a
mature infant, but had a history of encephalitis and febrile
convulsion at the age of six. Neurological and neuropsychological
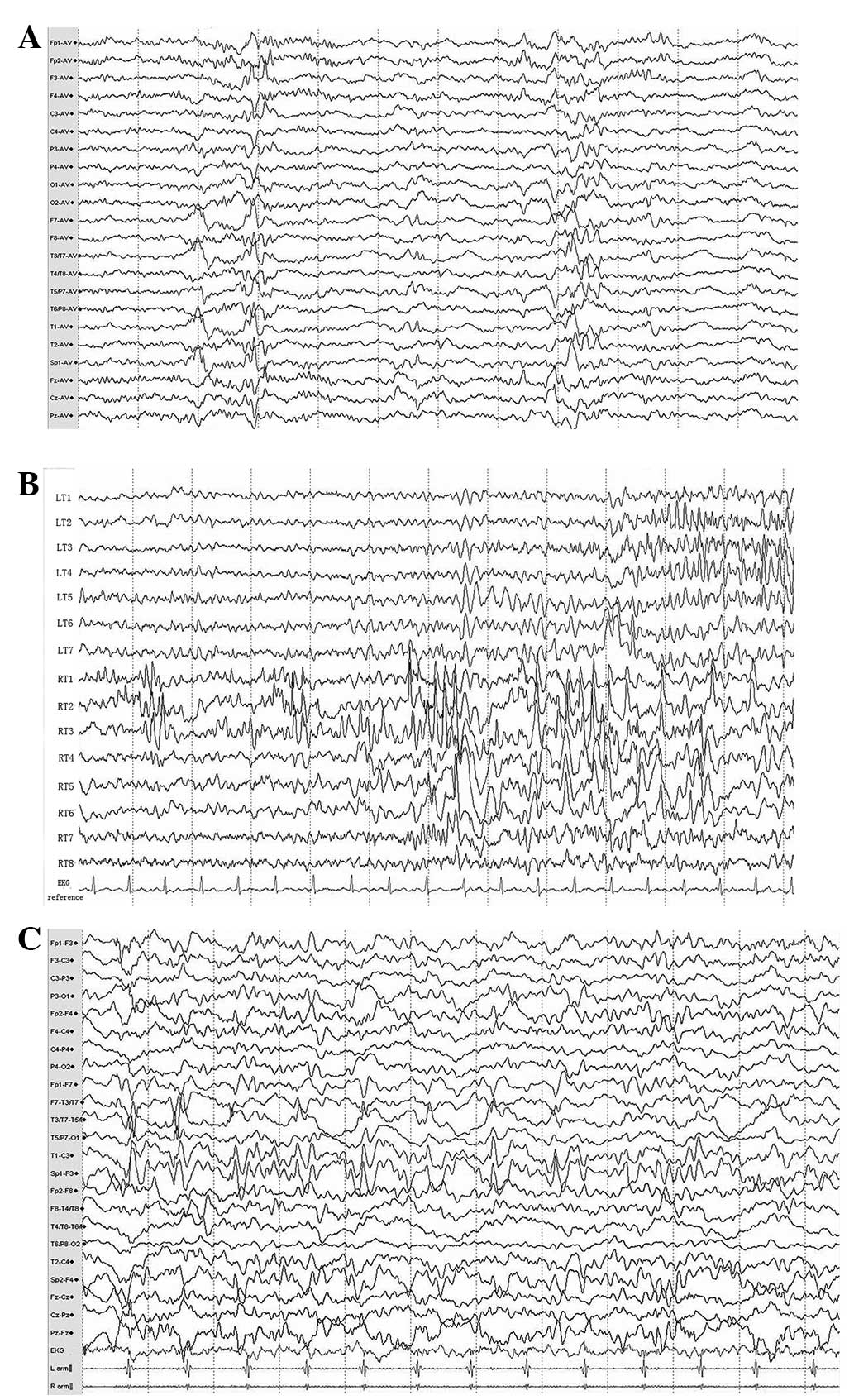
examinations were normal. Scalp video-electroencephalogram (V-EEG)
monitoring revealed intermittent multiple spikes, middle-amplitude
waves and interictal spikes from the bilateral anterior temporal
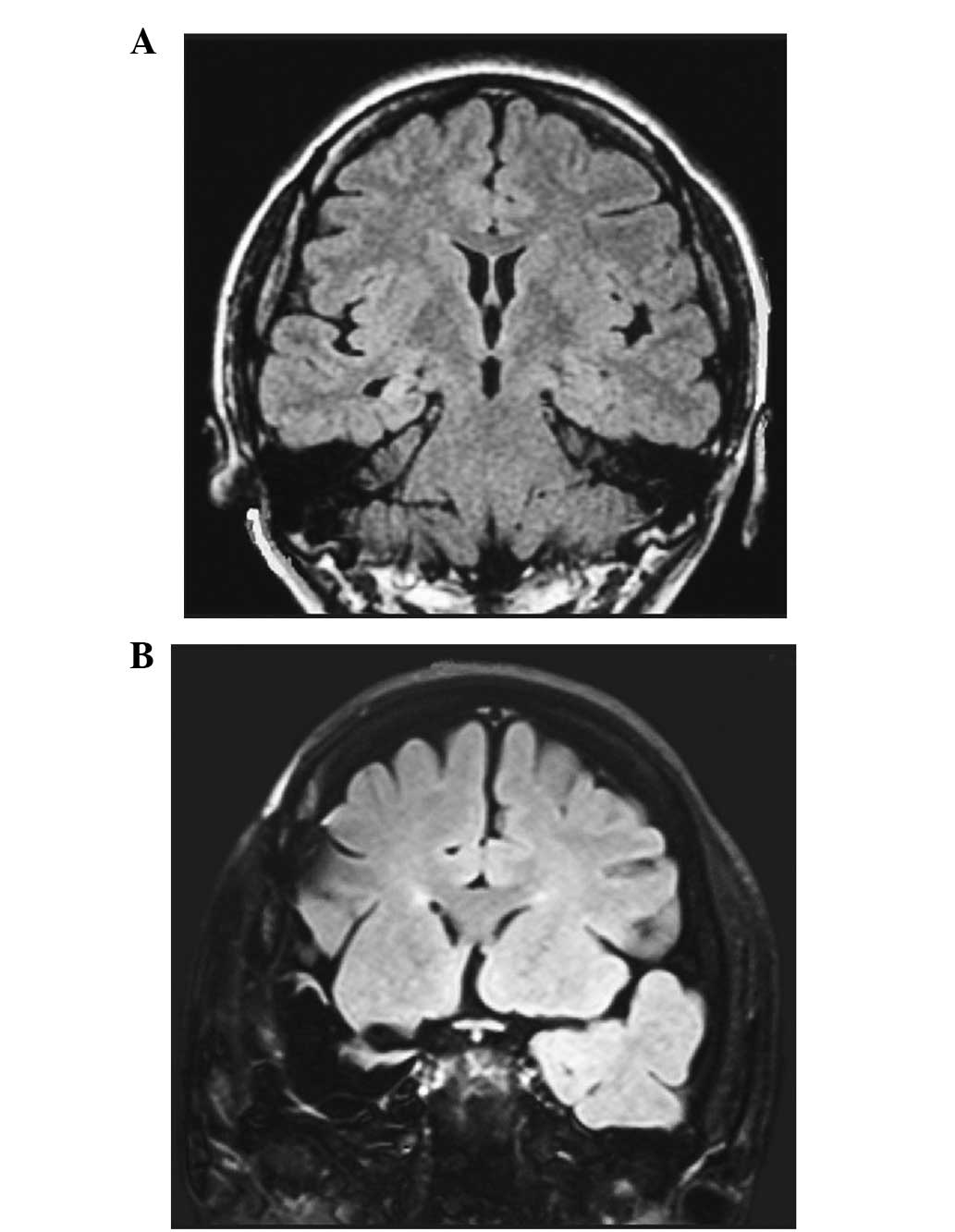
lobes (Fig. 1A). Fluid-attenuated
inversion recovery magnetic resonance imaging (FLAIR MRI) revealed
an increased signal within the right mesial temporal structures,
suggesting right mesial temporal sclerosis (Fig. 2A). Fluorodeoxyglucose-positron
emission tomography (FDG-PET) imaging showed mild hypometabolism in
the bilateral temporal lobes.
Based on the presurgical evaluation, it was
suggested that the patient had bitemporal lobe epilepsy. However,
the imaging and EEG results did not coincide with regard to the
side that required surgical resection. Therefore, cortex and depth
electrodes were implanted in the two temporal lobes for surgical
evaluation. The five-day electrocorticogram (ECoG) monitoring
displayed two different and independent onsets on the two sides of
the mesial temporal structures (Fig.
1B), which specifically included 11 typical episodes of GTCSs
originating from the left mesial temporal lobe, as well as six
clinical episodes of complex partial seizures (CPSs) arising from
the right mesial temporal region, which indicated a typical
bitemporal lobe epilepsy. Considering the patient’s FLAIR MRI
results, a resection of the right anterior temporal lobe,
hippocampus and amygdala was performed, and postsurgical MRI
confirmed the total removal of the right epileptogenic foci
(Fig. 2B). Pathological
examination of the surgical specimen confirmed hippocampal
sclerosis. However, despite the easing of the patient’s CPSs the
GTCSs were aggravated and occurred more frequently. Postsurgical
EEG assessment showed epileptiform discharges from the left
temporal lobe (Fig. 1C). As a
result, the patient currently takes 150 mg lamotrigine and 400 mg
phenobarbital daily.
Discussion
This case is notable due to the contradiction
between the imaging and EEG results. A previous study by Van Ness
et al (13) estimated that
17 serial seizures were required to be recorded to confidently
establish that <20% of seizures arose from a second site
(13). Subsequently, Blum
(8) used Bayes’ theorem and
selected data from an epilepsy monitoring unit to constrain the
statistical possibilities and estimate that recording five serial
seizures from a single focus confidently established that site as
the sole focus (8). In the present
case, scalp EEG displayed equal discharges from the bilateral
temporal lobe and the implanted electrodes further confirmed the
diagnosis. However, FLAIR MRI showed a unilateral abnormality. This
contradiction enhanced the difficulty of selecting the optimal
surgical strategy for this case. Despite this, it was decided to
resect one side of the mesial temporal lobe only, in order to avoid
memory function impairment. Relying on the MRI results, the right
side was selected. However, surgery did not leave the patient
seizure-free. Even though the CPSs arising from the right side
gradually eased, the GTCSs originating from the left side became
severely aggravated.
In normal circumstances, noninvasive methods are
used to provide a diagnosis of bitemporal lobe epilepsy and
invasive intracranial electrodes are able to suggest the
predominance of unitemporal seizure onset (14). However, traditional invasive
monitoring methods are limited by the duration of the recordings
(7). Patients with bitemporal lobe
epilepsy may cycle seizures from one side to the other side at
various intervals (5), and the
proportion of seizures arising from one temporal lobe during the
standard invasive evaluation is not a reliable prognostic factor of
epilepsy surgery (15). Therefore,
the selection of the resection side during a limited period of the
recording may be challenging. It is not possible to overcome this
problem of sampling with short-term monitoring, and a long-term
invasive evaluation is likely to be beneficial in these patients
(16–18). This may be one primary reason that
the correct side for resection was not selected in the present
case.
In describing this case, it is suggested that
clinicians should pay more attention to the patients’ symptoms when
confronted with similar cases, as GTCSs have a greater effect on
the patients’ quality of life. Furthermore, clinicians should
consider alternative options, such as responsive cortical
stimulation. This is a recently developed method for the treatment
of epilepsy that reduces the frequency of disabling partial
seizures and monitors epileptic discharges long enough to judge the
side of the majority of the seizures, therefore enabling the
modification of the surgical strategy (5,16–18,19).
If epileptic activities of either side arise from the temporal
neocortex, it is suggested that bipolar coagulation on functional
cortices (BCFC) or multiple subpial transection (MST) are combined
with selective amygdalohippocampectomy (SAH), respectively,
according to the sites of the epileptogenic foci, i.e., in the
amygdalohippocampal complex or temporal neocortex (20,21).
Furthermore, it is suggested that additional points of view are
sought in the treatment of similar cases of epilepsy.
References
|
1
|
Engel J Jr: Progress in the field of
epilepsy. Curr Opin Neurol. 26:160–162. 2013. View Article : Google Scholar
|
|
2
|
Téllez-Zenteno JF and Hernández-Ronquillo
L: A review of the epidemiology of temporal lobe epilepsy. Epilepsy
Res Treat. 2012:6308532012.
|
|
3
|
Kwan P and Brodie MJ: Early identification
of refractory epilepsy. N Engl J Med. 342:314–319. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Harroud A, Bouthillier A, Weil AG and
Nguyen DK: Temporal lobe epilepsy surgery failures: a review.
Epilepsy Res Treat. 2012:2016512012.PubMed/NCBI
|
|
5
|
Spencer D, Gwinn R, Salinsky M and
O’Malley JP: Laterality and temporal distribution of seizures in
patients with bitemporal independent seizures during a trial of
responsive neurostimulation. Epilepsy Res. 93:221–225. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hirsch LJ, Spencer SS, Williamson PD,
Spencer DD and Mattson RH: Comparison of bitemporal and unitemporal
epilepsy defined by depth EEG. Ann Neurol. 30:340–346. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Nair DR, Burgess R, McIntyre CC and Luders
H: Chronic subdural electrodes in the management of epilepsy. Clin
Neurophysiol. 119:11–28. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Blum D: Prevalence of bilateral partial
seizure foci and implications for electroencephalographic telemetry
monitoring and epilepsy surgery. Electroencephalogr Clin
Neurophysiol. 91:329–336. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Todorov AB, Lesser RP, Uematsu SS, et al:
Distribution in time of seizures during presurgical EEG monitoring.
Neurology. 44:1060–1064. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Haut SR, Legatt AD, O’Dell C, et al:
Seizure lateralization during EEG monitoring in patients with
bilateral foci: the cluster effect. Epilepsia. 38:937–940. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Haut SR, Swick C, Freeman K and Spencer S:
Seizure clustering during epilepsy monitoring. Epilepsia.
43:711–715. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Choi EJ, Kang JK and Lee SA: Effect of
interseizure interval on seizure lateralization in patients with
bilateral seizure foci. Seizure. 15:576–581. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Van Ness PC, So NK, Collura T, et al: AES
Proceedings: Ictal and interictal EEG: what constitutes an adequate
sample for epilepsy surgery? Epilepsia. 31:6231990.
|
|
14
|
Diehl B and Lüders HO: Temporal lobe
epilepsy: when are invasive recordings needed? Epilepsia. 41(Suppl
3): S61–S74. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Boling W, Aghakhani Y, Andermann F,
Sziklas V and Olivier A: Surgical treatment of independent
bitemporal lobe epilepsy defined by invasive recordings. J Neurol
Neurosurg Psychiatry. 80:533–538. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Fridley J, Thomas JG, Navarro JC and
Yoshor D: Brain stimulation for the treatment of epilepsy.
Neurosurg Focus. 32:E132012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Morrell MJ; RNS System in Epilepsy Study
Group. Responsive cortical stimulation for the treatment of
medically intractable partial epilepsy. Neurology. 77:1295–1304.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sohal VS and Sun FT: Responsive
neurostimulation suppresses synchronized cortical rhythms in
patients with epilepsy. Neurosurg Clin N Am. 22:481–488. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kossoff EH, Ritzl EK, Politsky JM, et al:
Effect of an external responsive neurostimulator on seizures and
electrographic discharges during subdural electrode monitoring.
Epilepsia. 45:1560–1567. 2004. View Article : Google Scholar
|
|
20
|
Patil AA, Andrews RV, Johnson M and
Rodriguez-Sierra JF: Is epilepsy surgery on both hemispheres
efective? Stereotact Funct Neurosurg. 82:214–221. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kagawa K, Iida K, Katagiri M, et al:
Successful treatment of mesial temporal lobe epilepsy with
bilateral hippocampal atrophy and false temporal scalp ictal onset:
a case report. Hiroshima J Med Sci. 61:37–41. 2012.PubMed/NCBI
|