Introduction
Portopulmonary hypertension (POPH) refers to the
condition of simultaneous pulmonary arterial and portal
hypertension. Hemodynamically, it is defined as a mean pulmonary
artery pressure (MPAP) >25 mmHg and normal volume status or
pulmonary capillary wedge pressure (PCWP) <15 mmHg in patients
with chronic liver disease and portal hypertension (1–3).
POPH has been reported in ∼6–9% of patients with advanced liver
disease, that are referred for liver transplants (4,5).
This variation in prevalence results from the different groups of
cirrhotic patients studied and different diagnostic procedures
used.
Clinical manifestations of portal hypertension
typically precede those of pulmonary artery hypertension by 2–15
years. The most common symptoms of POPH include dyspnea upon
exertion, syncope, chest pain, fatigue, hemoptysis and orthopnea.
The presence of molecular markers is also likely, as one study
supported the hypothesis that pulmonary vasculature may be exposed
to either cytokines or excess circulating vasoconstrictors,
including interleukin-6 and endotoxin produced by the diseased
liver (6). However, to date, the
predictors of and biological mechanism responsible for the
development of this complication remain unknown.
There are no known clinical factors that determine
the risk of POPH in patients with advanced liver disease.
Similarly, the mechanism for pulmonary vascular obliteration in
patients with portal hypertension, characterized by systemic
vasodilation remains unclear. It follows that the identification of
patient characteristics associated with an increase or decrease in
the probability of developing POPH may not only be clinically
useful, but may also shed light on the etiology of this relatively
common comorbidity of portal hypertension. Therefore, the aims of
this study were to explore the clinical features of POPH and to
identify risk factors associated with POPH in cirrhotic
patients.
Patients and methods
Patients
From March 2011 to May 2012, 145 consecutive adult
patients with cirrhosis (102 males, 43 females) from our hospital
were enrolled in the study. The only inclusion criterion was the
presence of clinical portal hypertension with intrinsic liver
cirrhosis. Patients with significant obstructive lung disease,
restrictive ventilatory defects, human immunodeficiency virus,
severe aortic or mitral stenosis, regurgitation or significant left
ventricular dysfunction were excluded. Also excluded were
individuals with hepatocellular carcinoma or any other malignancy,
known hemostatic disorders other than liver disease, bacterial
infection, a clinical history of peripheral venous thrombosis or
Budd-Chiari syndrome, spleen resection, lung and liver
transplantation and those receiving endoscopic treatment or
anticoagulation therapy. A total of 100 patients were considered
acceptable and were enrolled in our study. Informed consent was
obtained from all patients and the study was carried out according
to the principles of the declaration of Helsinki and the guidelines
of the institutional ethics committee.
Liver cirrhosis was diagnosed by clinical findings
or morphology and liver function of the POPH patients was scored
using the Child-Pugh classification (7). Past medical history and social
history were recorded. Non-invasive screening for POPH was
performed and evaluated by Doppler echocardiography. In order to
identify risk factors associated with POPH, the patients were
classified into two groups: a POPH group [pulmonary artery systolic
pressure (PASP) ≥40 mmHg] and a non-POPH group (PASP <40 mmHg)
(8,9).
Diagnosis of POPH
Pulmonary vascular resistance (PVR) is considered an
essential feature of POPH. Diagnostic measurements of PVR are
traditionally obtained by right heart catheterization (RHC)
(10,11); however, since bleeding
complications are a concern among cirrhotic patients, other forms
of diagnosis are preferred. Results of Doppler echocardiography are
comparable to RHC in non-cirrhotic patients with pulmonary
hypertension (12,13). For cirrhotic patients undergoing
liver transplantation (14,15),
it decreases the requirement for repeated invasive measurements. In
our study, PASP (measured by Doppler echocardiography) was used to
diagnose POPH.
Noninvasive color Doppler echocardiographies were
performed on all patients. The MPAP was calculated from PASP (MPAP
= 0.61 PASP + 2 mmHg). PASP values of 38–54 mmHg were considered to
represent mild POPH, 55–69 mmHg were moderate and values ≥70 mmHg
were severe (16).
Collection and analysis of blood
samples
Blood samples (20 ml) were collected from patients
following at least 12 h of fasting. Hemoglobin (Hb) and blood
platelet count (BPC) were determined using a Sysmex XE-2100
automated analyzer (Sysmex, Kobe, Japan). Total bilirubin (TBIL)
and albumin (ALB) were determined using diazotization and the
bromocresol green (BCG) assay method, respectively (Roche
Cobas-c702, Germany). D-dimer and high sensitivity C-reactive
protein (hs-CRP) levels were detected using the corresponding kits
from Sun Biotech Co., Ltd. (Shanghai, China), following the
manufacturer’s instructions. Prothrombin time (PT), activated
partial prothrombin time (APTT) and fibrinogen (Fib) were
determined by routine coagulation methods with a coagulation
detector, using a Sysmex CA-6000 automated analyzer (Sysmex, Milton
Keynes, UK). Intercellular adhesion molecule 1 (ICAM-1),
interferon-α (IFN-α) and tumor necrosis factor-α (TNF-α) were
measured by enzyme-linked immunosorbent assay (ELISA).
Statistical analysis
The SPSS software package for Windows (SPSS version
11.0, SPSS Inc., Chicago, IL, USA) was used for statistical
analysis. Continuous data were summarized using mean ± standard
deviation (SD) or median (interquartile range), as appropriate.
Categorical variables were displayed as frequencies. Statistical
analysis was performed using the appropriate parametric or
non-parametric tests. Differences between the POPH and non-POPH
groups were evaluated by Chi-square test. For continuous data, the
assumption of normality was evaluated using a normality test. The
Pearson Chi-square test, corrected Chi-square test and Fisher’s
exact test were used, as appropriate. Multivariate binary logistic
regression was performed to evaluate the correlation between the
presence of portal vein thrombosis and thrombotic risk factors with
respect to the odds of occurrence for an event. The model was
estimated using a backward stepwise method (Wald). In this
multivariate analysis, we used a number of variables, including
those that were not significant univariate predictors, since they
may contribute to a multiple regression model in unforeseen ways
due to complex intercorrelations among them. The coefficients
obtained from the logistic regression analyses were also expressed
in terms of odds ratios (ORs) with 95% confidence intervals.
Considering the number of cases, we determined that the final
multivariate model should include ≤4 predictors to prevent
overfitting. A two-tailed P-value ≤0.05 was considered to indicate
a statistically significant difference.
Results
Clinical features
Ten of the 100 study patients (10%) were diagnosed
with POPH. Five of these (50%) were males aged 30–79 years
(bivariate correlation analysis was used) with a mean age of
59.0±24.0 years. Five (50%) were females aged 62–82 years, with a
mean age of 73.0±9.0 years. The median age of the 10 POPH patients
was 66 years. With regard to the etiology of subjects, eight of the
POPH patients had viral cirrhosis [hepatitis B virus (HBV),
hepatitis C virus (HCV) or HBV and HCV], one had autoimmune
cirrhosis and one had cryptogenic cirrhosis. POPH was not observed
in schistosomal or alcoholic cirrhosis patients. Among the ten POPH
patients, PASP values were 40–70 mmHg. The severity of POPH in the
subjects is listed in Table I.
 | Table I.Demographic and clinical features of
the ten cirrhotic patients with POPH. |
Table I.
Demographic and clinical features of
the ten cirrhotic patients with POPH.
| Case | Age (years) | Gender | Etiology | Child-Pugh class | PASP (mmHg) | Degree |
|---|
| 1 | 82 | Female | HBV+HCV | A | 68 | Moderate |
| 2 | 68 | Female | HBV | B | 63 | Moderate |
| 3 | 79 | Male | HCV | C | 44 | Mild |
| 4 | 77 | Male | Autoimmune | B | 70 | Severe |
| 5 | 82 | Female | HBV | C | 41 | Mild |
| 6 | 76 | Male | HBV | B | 44 | Mild |
| 7 | 30 | Male | HCV | C | 43 | Mild |
| 8 | 62 | Female | HBV | B | 40 | Mild |
| 9 | 72 | Female | Cryptogenic | B | 41 | Mild |
| 10 | 36 | Male | HBV | B | 43 | Mild |
Clinical symptoms or signs
The presentations of the decompensate liver
cirrhosis and portal hypertension, including jaundice, ascites,
splenomegaly, edema and gastrointestinal hemorrhage were observed
in the cirrhotic patients with POPH. Although a number of patients
with POPH are asymptomatic (17),
other POPH patients presented with syndromes and signs of pulmonary
hypertension. Two patients presented dyspnea upon exertion, two
with syncope, one with chest pain and one with hemoptysis.
Risk factors analysis
There were no significant differences in age or
gender between the POPH and the non-POPH groups (mean age,
66.0±18.0 vs. 61.6±13.9 years; P=0.86, P=0.15, respectively). Of
the etiologies studied, only the prevalence of HCV-related
cirrhosis patients differed between the two groups (P=0.001). With
regards to liver function, we identified that one POPH patient was
Child-Pugh grade A, six were grade B and three were grade C. There
were no significant differences in Child-Pugh grade between the two
groups (P=0.76). With regard to the severity of POPH, liver damage
was mild in seven patients, moderate in two patients and severe in
one patient. With respect to past medical history only the
incidence of portal vein thrombosis differed significantly between
the POPH and non-POPH groups (P=0.02; Tables II and III).
| Table II.Comparison of the clinical
characteristics between cirrhotic patients with and without
POPH. |
Table II.
Comparison of the clinical
characteristics between cirrhotic patients with and without
POPH.
| POPH | Non-POPH | t/χ2 | P-value |
|---|
| N | 10 (10%) | 90 (90%) | | |
| Age (years) | 66.0±18.0 | 61.6±13.9 | 0.19 | 0.86 |
| Gender
(male/female) | 5/5 | 65/25 | 2.15 | 0.15 |
| Etiology | | | | |
| HBV | 5 (50%) | 51 (56.7%) | 0.10 | 0.72 |
| HCV | 2 (20%) | 1 (1.1%) | Fisher’s exact
test | 0.03 |
| Alcoholic | 0 (0%) | 5 (5.6%) | Fisher’s exact
test | 1.00 |
| Schistosomal | 0 (0%) | 7 (7.8%) | 0.07 | 0.79 |
| Autoimmune | 1 (10%) | 8 (8.9%) | 0.01 | 0.91 |
| Cryptogenic | 1 (10%) | 18 (20%) | 0.59 | 0.44 |
| HBV+HCV | 1 (10%) | 0 (0%) | Fisher’s exact
test | 0.10 |
| Child-Pugh class | | | | |
| A | 1 | 13 | | |
| B | 6 | 56 | 0.55 | 0.76 |
| C | 3 | 21 | | |
| Severity of POPH | | | | |
| Mild | 7 | 0 | | |
| Moderate | 2 | 0 | | |
| Severe | 1 | 0 | | |
| Table III.Comparison of medical histories
between patients with and without POPH. |
Table III.
Comparison of medical histories
between patients with and without POPH.
| Variable | POPH (%) | Non-POPH (%) | χ2 | P-value |
|---|
| N | 10 | 90 | | |
| GI hemorrhage | 50 | 27.8 | 2.12 | 0.15 |
| Hepatic
encephalopathy | 20 | 23.3 | 0.06 | 0.81 |
| Hepatorenal
syndrome | 20 | 21.1 | 0.01 | 0.94 |
| Ascites | 80 | 77.8 | 0.03 | 0.87 |
| Smoking | 20 | 23.3 | 0.06 | 0.81 |
| Alcohol abuse | 10 | 10.0 | 0.00 | 1.00 |
| High blood
pressure | 20 | 26.7 | 0.21 | 0.65 |
| Diabetes
mellitus | 10 | 11.1 | 0.01 | 0.92 |
| Coronary artery
disease | 10 | 5.6 | 0.32 | 0.58 |
| Blood
transfusion | 60 | 51.1 | 0.29 | 0.59 |
| Portal vein
thromosis | 50 | 16.7 | 5.63 | 0.04 |
| Drug use | 10 | 0.0 | Fisher’s exact
test | 0.10a |
The levels of BPC, ALB, TBIL, Hs-CRP, D-dimer,
thrombin time (TT), Fib, ICAM-1, IFN-α and TFN-α did not differ
significantly between POPH and non-POPH patients. There were no
significant differences in the levels of APTT and PT between the
two groups. However, the levels of Hb were lower in the POPH group
than those in the non-POPH groups (P=0.001). Hb was determined to
be a risk factor of POPH by univariate analysis (Table IV).
| Table IV.Comparison of laboratory results
between patients with and without POPH. |
Table IV.
Comparison of laboratory results
between patients with and without POPH.
| Variable | POPH | Non-POPH | t | P-value |
|---|
| Hb (g/l) | 72.6±14.2 | 98.6±24.1 | 2.46 | 0.00 |
| BPC
(×109/l) | 82.1±44.3 | 83.4±46.9 | −0.08 | 0.93 |
| TBIL (μmol/l) | 30.1±12.3 | 40.8±25.4 | 1.38 | 0.17 |
| ALB (g/l) | 26.1±5.5 | 26.8±6.1 | 0.33 | 0.75 |
| Hs-CRP (mg/l) | 9.8±9.0 | 17.1±2.4 | 0.93 | 0.36 |
| D-dimer (mg/l) | 0.3±0.2 | 0.6±0.1 | 1.09 | 0.28 |
| APTT (sec) | 39.3±9.2 | 36.6±10.4 | −0.79 | 0.43 |
| PT (sec) | 14.7±2.8 | 14.1±2.9 | −0.61 | 0.54 |
| TT (sec) | 18.7±2.2 | 21.2±5.1 | 1.45 | 0.14 |
| Fibrinogen
(g/l) | 2.4±0.7 | 2.8±0.3 | 0.40 | 0.69 |
| ICAM-1(ng/ml) | 14.9±10.1 | 19.3±2.5 | 0.54 | 0.59 |
| IFN-α (pg/ml) | 23.0±13.7 | 37.4±16.6 | 0.68 | 0.50 |
| TNF-α (pg/ml) | 14.5±4.7 | 21.3±3.2 | 0.66 | 0.51 |
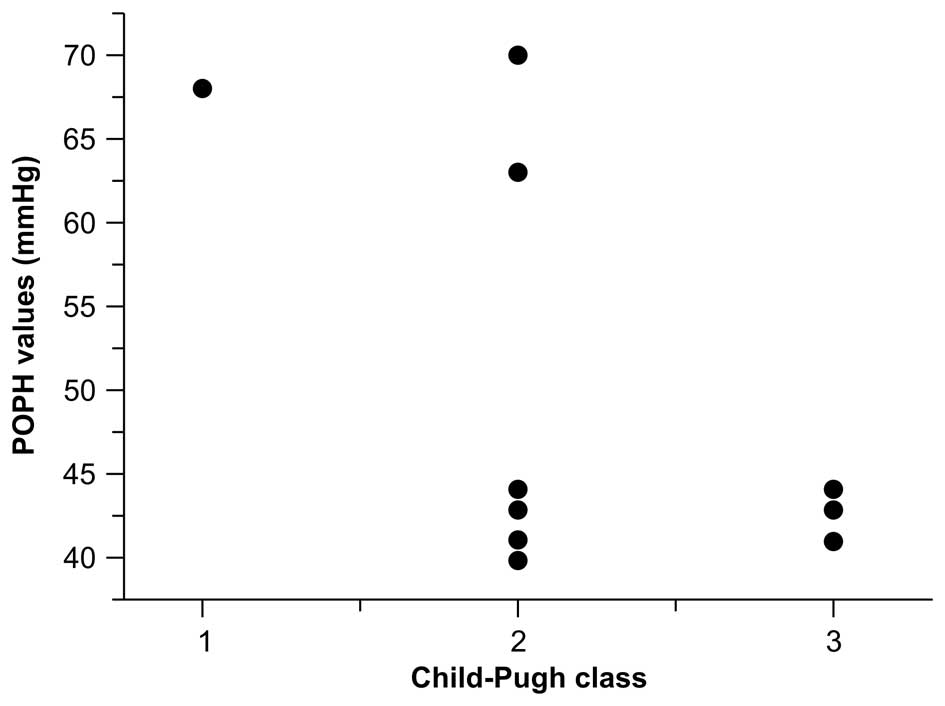
Correlation between Child-Pugh class and
severity of POPH
In our study, a correlation between Child-Pugh class
and severity of POPH (reflected by the value of PASP) was
investigated. The results revealed that the PASP values were not
significantly correlated with Child-Pugh class (R=−0.06, P=0.09;
Fig. 1).
Multivariate analysis
The Hb, HCV, D-dimer and portal vein thrombosis were
included in multivariate logistic regression analysis. Only Hb was
identified as an independent factor associated with an increased
risk of POPH (OR=0.952; Table
V).
| Table V.Results of backward, stepwise
logistic regression analysis of the correlation between POPH and Hb
level, HCV, D-dimer level and portal vein thrombosis. |
Table V.
Results of backward, stepwise
logistic regression analysis of the correlation between POPH and Hb
level, HCV, D-dimer level and portal vein thrombosis.
| Variables | β-value | SE | Wald value | P-value | OR | 95% CI |
|---|
| Hb | −0.049 | 0.021 | 5.478 | 0.02 | 0.952 | 0.913–0.992 |
| HCV | 2.464 | 1.787 | 1.901 | 0.17 | 11.746 | 0.354–389.915 |
| D-D | −0.020 | 0.025 | 0.625 | 0.43 | 0.981 | 0.934–1.0290 |
| PVT | 1.129 | 0.778 | 2.296 | 0.13 | 3.252 | 0.707–14.949 |
Discussion
In the present study, POPH was diagnosed in 10% of
patients with cirrhosis. This is within the range of prevalence
reported in the literature (20).
In previous studies, POPH has been estimated to occur with a
prevalence of 16.1% in patients with cirrhosis and refractory
ascites and 0.25–4% in patients with cirrhosis without refractory
ascites (18,19).
Although our results demonstrated that there are
higher percentages of females with cirrhosis that develop POPH, no
significant difference was observed in the incidence of POPH across
the gender (results not shown). This indicates that males and
females with cirrhosis are at risk of developing POPH. These
results contradict the findings of a previous study that identified
that females are at a higher risk of POPH (11).
In our study, the majority of the POPH patients had
viral cirrhosis (HBV and HCV). Viral cirrhosis was the most common
type of cirrhosis among our Chinese population; however, our
results demonstrated that a higher incidence of POPH exists among
patients with viral cirrhosis. While previous research identified
that HCV infection was negatively correlated with POPH (11), this was not supported by our data.
In contrast, the high incidence of POPH among patients with HCV
infection indicates that patients with HCV cirrhosis may be at
higher risk of developing POPH.
With regard to the severity of POPH, our results
demonstrated that the severity of POPH is unrelated to liver
function, as we were unable to identify an association between POPH
severity and Child-Pugh class. However, this conclusion is based on
a small number of cases and larger studies are required to verify
this correlation.
Previously hypothesized risk factors of POPH were
not associated with POPH in our study. Age, gender and Child-Pugh
class did not differ between the POPH and non-POPH groups. Also,
hepatic complications, including GI hemorrhage, hepatorenal
syndrome ascites and encephalopathy did not differ between the
groups. Similarly, HBP, DM, coronary artery disease, drug use and
blood transfusion did not appear to affect the risk of developing
POPH and smoking and alcohol use were common in the two groups.
With respect to patient medical histories, only
portal vein thrombosis differed between the two groups, indicating
that portal vein thrombosis is associated with POPH. These results
are supported by a previous study that described microembolism of
the lungs in hepatic fibrosis due to recurrent cholangitis. The
passage of small emboli to the lungs was attributed to the presence
of small hepatic arteriovenous fistulae (21). The correlation between POPH and
portal vein thrombosis may be explained by a similar anatomical
mechanism. Portal venous obstruction secondary to portal vein
thrombosis would likely enlarge such communications, resulting in
repeated microembolism of the lungs. This may lead to pulmonary
hypertension and, ultimately, congestive failure due to chronic cor
pulmonale (21).
Among the laboratory parameters examined in our
study, levels of Hb were lower in the POPH group than in the
non-POPH group. To our knowledge, a correlation between POPH and Hb
has not been described previously. However, it is known that a
decrease in Hb leads to a significant increase in cardiac output
and exacerbated hyperdynamic splanchnic circulation (22). The hyperdynamic splanchnic
circulation is a major contributor to portal hypertension.
Therefore, it is not surprising that Hb levels were significantly
lower in the POPH group and that Hb level was the only variable
independently associated with POPH. These findings indicate that Hb
level is an independent risk factor and plays a key role in the
development of POPH. While HCV and PVT were also associated with a
higher incidence of POPH, these factors were not independent
predictors of POPH. Perhaps they contributed to the formation of
POPH through interactions with other unknown factors. However,
significant differences between the two groups were not observed
for any of the other markers that we investigated.
In conclusion, within our study population POPH was
present in 10% of cirrhotic patients. It was most common among
patients with viral cirrhosis and absent among schistosomal and
alcoholic cirrhosis patients. Notably, the severity of POPH was
unrelated to liver function (Child-Pugh classification). HCV
infection and portal vein thrombosis may play important roles
during the development of POPH; however, Hb level is the only
significant, independent predictor of POPH. Future studies should
examine the mechanistic role of these factors in the development of
POPH.
Acknowledgements
This study was supported by the
Natural Science Foundation of China (81070343) and the Shanghai
Excellent Academic Pacesetters Program (08xD14045)
References
|
1.
|
Hadengue A, Benhayoun M, Lebrec D and
Benhamou J: Pulmonary hypertension complicating portal
hypertension: prevalence and relation to splanchnic hemodynamics.
Gastroenterology. 100:520–528. 1991.
|
|
2.
|
Simonneau G, Galič N, Rubin LJ, Langleben
D, Seeger W, Domenighetti G, Gibbs S, Lebrec D, Speich R and
Beghetti M: Clinical classification of pulmonary hypertension. J Am
Coll Cardiol. 43:S5–S12. 2004. View Article : Google Scholar
|
|
3.
|
Krowka MJ: Hepatopulmonary syndrome versus
portopulmonary hypertension: distinctions and dilemmas. Hepatology.
25:1282–1284. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Castro M, Krowka MJ, Schroeder DR, Beck
KC, Plevak DJ, Rettke SR, Cortese DA and Wiesner RH: Frequency and
clinical implications of increased pulmonary artery pressures in
liver transplant patients. Mayo Clinic Proc. 71:543–551. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Kawut SM, Krowka MJ, Trotter JF, Roberts
KE, Benza RL, Badesch DB, Taichman DB, Horn EM, Zacks S and
Kaplowitz N: Clinical risk factors for portopulmonary hypertension.
Hepatology. 48:196–203. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Kalambokis GN, Mouzaki A, Rodi M, Pappas
K, Korantzopoulos P and Tsianos EV: Circulating endotoxin and
interleukin-6 levels are associated with Doppler-evaluated
pulmonary vascular resistance in cirrhotic patients. Hepatol Int.
6:783–789. 2012. View Article : Google Scholar
|
|
7.
|
Shetty K, Rybicki L and Carey WD: The
Child-Pugh classification as a prognostic indicator for survival in
primary sclerosing cholangitis. Hepatology. 25:1049–1053. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Cotton CL, Gandhi S, Vaitkus PT, Massad
MG, Benedetti E, Mrtek RG and Wiley TE: Role of echocardiography in
detecting portopulmonary hypertension in liver transplant
candidates. Liver Transpl. 8:1051–1054. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Sciomer S, Magrì D and Badagliacca R:
Non-invasive assessment of pulmonary hypertension:
Doppler-echocardiography. Pulm Pharmacol Ther. 20:135–140. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Krowka MJ: Evolving dilemmas and
management of portopulmonary hypertension. Semin Liver Dis.
26:265–272. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Golbin JM and Krowka MJ: Portopulmonary
hypertension. Clin Chest Med. 28:203–218. 2007. View Article : Google Scholar
|
|
12.
|
Scapellato F, Temporelli PL, Eleuteri E,
Corrà U, Imparato A and Giannuzzi P: Accurate noninvasive
estimation of pulmonary vascular resistance by Doppler
echocardiography in patients with chronic heart failure. J Am Coll
Cardiol. 37:1813–1819. 2001. View Article : Google Scholar
|
|
13.
|
Abbas AE, Fortuin FD, Schiller NB,
Appleton CP, Moreno CA and Lester SJ: A simple method for
noninvasive estimation of pulmonary vascular resistance. J Am Coll
Cardiol. 41:1021–1027. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Farzaneh-Far R, McKeown BH, Dang D,
Roberts J, Schiller NB and Foster E: Accuracy of Doppler-estimated
pulmonary vascular resistance in patients before liver
transplantation. Am J Cardiol. 101:259–262. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Kim W, Krowka MJ, Plevak DJ, Lee J, Rettke
SR, Frantz RP and Wiesner RH: Accuracy of Doppler echocardiography
in the assessment of pulmonary hypertension in liver transplant
candidates. Liver Transpl. 6:453–458. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Chemla D, Castelain V, Humbert M, Hébert
JL, Simonneau G, Lecarpentier Y and Hervé P: New formula for
predicting mean pulmonary artery pressure using systolic pulmonary
artery pressure. Chest. 126:1313–1317. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Robalino BD and Moodie DS: Association
between primary pulmonary hypertension and portal hypertension:
analysis of its pathophysiology and clinical, laboratory and
hemodynamic manifestations. J Am Coll Cardiol. 17:492–498. 1991.
View Article : Google Scholar
|
|
18.
|
Benjaminov F, Prentice M, Sniderman K, Siu
S, Liu P and Wong F: Portopulmonary hypertension in decompensated
cirrhosis with refractory ascites. Gut. 52:1355–1362. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Hoeper MM, Krowka MJ and Strassburg CP:
Portopulmonary hypertension and hepatopulmonary syndrome. Lancet.
363:1461–1468. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Humbert M, Sitbon O, Chaouat A, Bertocchi
M, Habib G, Gressin V, Yaici A, Weitzenblum E, Cordier JF and
Chabot F: Pulmonary arterial hypertension in France. Am J Respir
Crit Care Med. 173:1023–1030. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Lai K, McFadzean A and Yeung R:
Microembolic pulmonary hypertension in pyogenic cholangitis. Br Med
J. 1:22–24. 1968. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Groszmann RJ: Hyperdynamic circulation of
liver disease 40 years later: pathophysiology and clinical
consequences. Hepatology. 20:1359–1363. 1994.
|