Introduction
Coronary air embolism is a well-recognized
complication of coronary catheterization and occurs in 0.1–0.3% of
cases (1,2). The causes of coronary artery air
embolism include incomplete aspiration of angiographic or guiding
catheters, balloon rupture, insinuation of air with balloon
catheter introduction or withdrawal, structural failures of the
equipment and constant negative suction of self-venting catheters
left out of the body (2,3). Herein, we report a rare case of
unexpected contralateral coronary artery air embolism during
left-side coronary angiography.
Case report
A 65-year-old female with stable angina was
scheduled to undergo follow-up for coronary angiography 9 months
after the performance of an index procedure. According to the
routine procedure, a standard JL4 diagnostic catheter via the right
femoral artery was employed to catheterize the left coronary
artery. On engagement and initial injection of the left coronary
artery, the patient began to experience severe chest pain and the
ST segment in leads II and III began to rise. Immediately, the
catheter was exchanged and right coronary artery angiography was
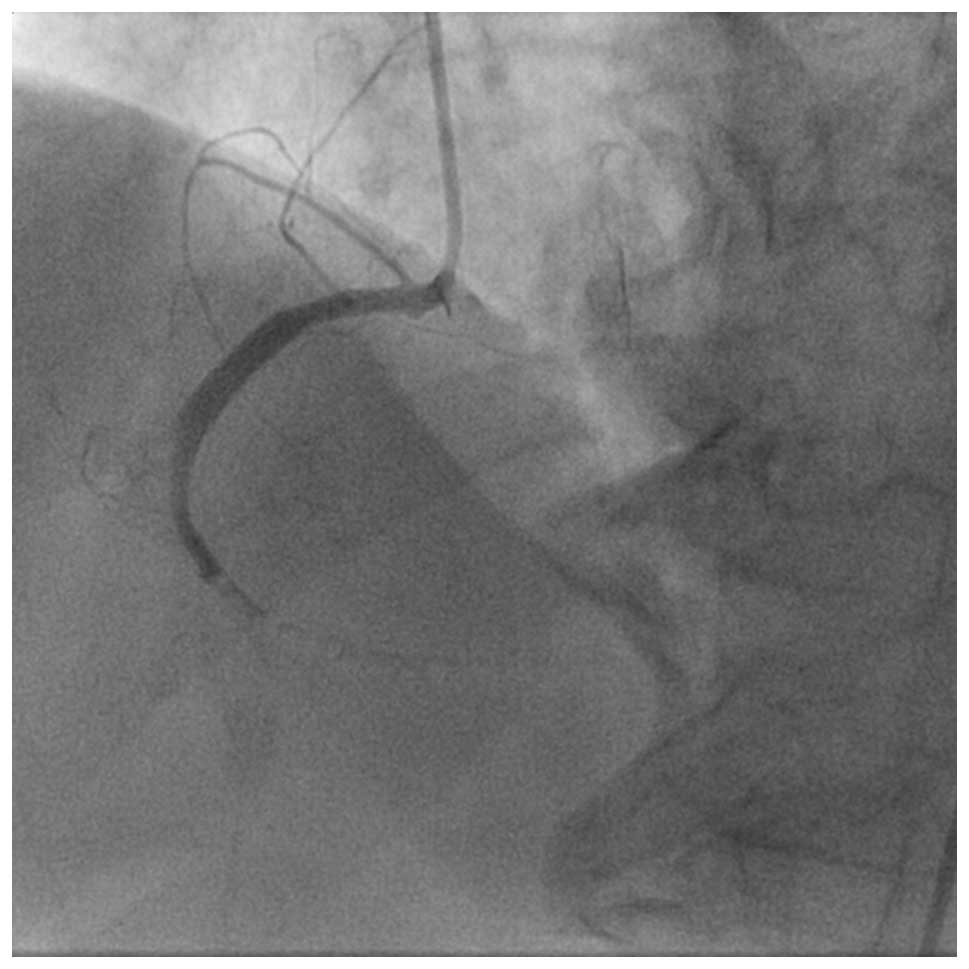
performed. Multiple small bead-like shadow defects suspected to be
air bubbles were present in the mid-portion of the right coronary
artery and interruption of blood flow was observed (Fig. 1). The patient went into a shock
state with complete atrioventricular block and hypotension.
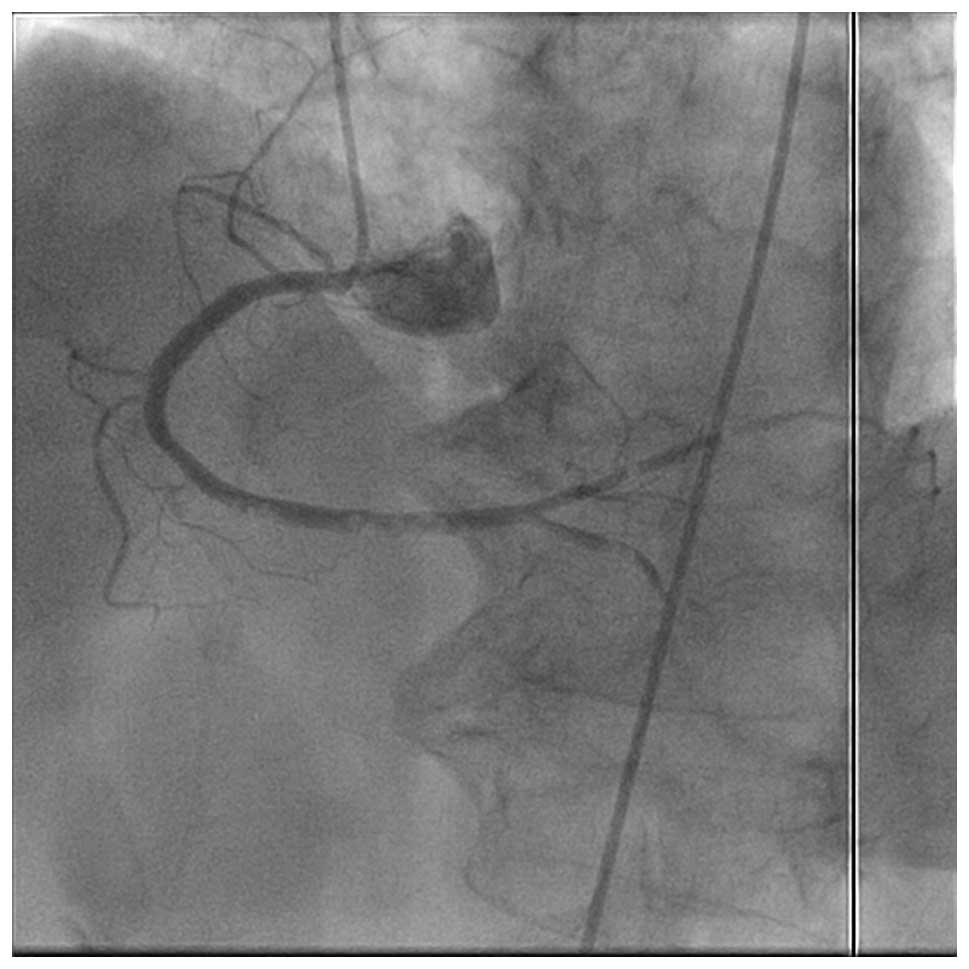
Immediately, the patient received 100% oxygen inhalation through a
facemask. Contrast dye was forcefully injected several times and
the air bubbles dispersed distally (Fig. 2). The treatments were successful in
terms of improvement in the condition of the patient. Subsequently,
the patient recovered from the state of shock. Later, angiography
confirmed the disappearance of air embolism and sufficient blood
flow was obtained in the right coronary artery. The patient had an
uneventful overnight stay and was discharged the following day with
a normal electrocardiogram (ECG) and cardiac enzyme levels. Written
informed consent was obtained from the patient.
Discussion
Our case demonstrated an unusual process by which
air was introduced into the right coronary artery during left
coronary artery angiography. The cause may be due to incomplete
aspiration of the angiographic catheter. However, the mechanism of
contralateral air embolism is unclear. Inoue et al (4) reported similar cases and insisted
that the air was injected through the sidehole. However, we used a
diagnostic catheter without a sidehole so this does not explain the
mechanism of contralateral air embolism. Another report (5) speculated that the air trapped in the
catheter lumen followed the path of least resistance and exited
forcefully from the end hole of the diagnostic catheter. The force
of the contrast injection directed the mixture of blood-air towards
the medial wall of the left aortic cusp from where it rebound
towards the right coronary cusp, resulting in its admixture with
the forward ejectate, which was then distributed into the right
coronary artery and aortic arch vessels.
Immediate management of coronary air embolism has
not yet been established. When small to moderate amounts of air are
involved, inhalation of 100% oxygen is appropriate since oxygen
facilitates the absorption of the air embolus through the
microcirculation. When large amounts of air are involved, more
aggressive modalities, including air aspiration and forceful
injection of saline or contrast medium are suggested (2,3,6,7).
Previously, stirring the mass of air using a 0.014-inch guidewire
and balloon catheter for coronary angioplasty has also been
suggested, which worked by breaking up the larger air mass into a
number of smaller bubbles to increase the surface area (4).
Prevention of iatrogenic massive air embolism is
paramount. Back bleeding from the catheter during its introduction
is protective against the entrapment of any air present in the
catheter. In addition, the catheter should be tested in the
ascending aorta, distal to the aortic cusp to prevent the
occurrence of adverse events (5).
In conclusion, awareness that air embolism may occur
in contralateral coronary artery angiography is essential, and
complete air aspiration during coronary angiography should be
ensured.
References
|
1
|
Dodek A, Boone JA, Hooper RO, et al:
Complications of left coronary arteriography. Can Med Assoc J.
128:934–936. 1983.
|
|
2
|
Khan M, Schmidt DH, Bajwa T and Shalev Y:
Coronary air embolism: incidence, severity, and suggested
approaches to treatment. Cathet Cardiovasc Diagn. 36:313–318. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Khan JK and Hartzler GO: The spectrum of
symptomatic coronary air embolism during balloon angioplasty:
causes, consequences, and management. Am Heart J. 119:1374–1377.
1990. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Inoue T, Yaguchi I, Mizoguchi K, et al:
Air embolism in the right coronary artery occurring during the left
coronary angioplasty using the guiding catheter with a side hole.
Catheter Cardiovasc Interv. 49:331–334. 2000. View Article : Google Scholar
|
|
5
|
Janin Y: Letter to the editor by Janin.
Catheter Cardiovasc Interv. 50:5102000. View Article : Google Scholar
|
|
6
|
Solodky A, Birnbaum Y, Assali A, et al:
Coronary air embolism treated by bubble aspiration. Catheter
Cardiovasc Interv. 49:452–454. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Patterson MS and Kiemeneij F: Coronary air
embolism treated with aspiration catheter. Heart. 91:e362005.
View Article : Google Scholar : PubMed/NCBI
|