Introduction
Benign masseteric hypertrophy is a major reason for
a wide lower face. Several treatment methods may be used on
patients with masseteric hypertrophy in order to improve facial
contours. To date, the major treatment methods involve surgery,
including mandibular angle osteotomy and masseter muscle resection,
and there are non-surgical methods, including injection with
botulinum toxin type A (1,2). Jin Park et al reported on
radiofrequency (RF) volumetric reduction for masseteric hypertrophy
(3). RF-induced tissue coagulation
necrosis of the masseter muscle did not lead to any infections or
limitations with regard to mouth opening, and the clinical
improvement was well maintained following treatment (3). However, thus far, there have been no
studies on the efficacy and safety of RF and injection with
botulinum toxin A for the treatment of masseteric hypertrophy. In
the present study, these two methods were compared by measuring the
thickness of the masseter muscle at 6 and 12 months following
surgery.
Materials and methods
Patients
The study was approved by the Institutional Review
Board of the Affiliated Hospital of Nanjing University of
Traditional Chinese Medicine (Nanjing, China). A total of 24
Chinese patients (female, 23; male, 1; mean age, 27 years; age
range, 21–48 years; Fitzpatrick skin types, IV) with moderate to
severe masseteric hypertrophy were included in this study. All
patients provided informed consent and were randomly assigned to
two groups (the botulinum toxin A and RF ablation groups). Patients
with concomitant treatments, including surgical resection or RF
ablation of the masseter muscle nerve and injection with botulinum
toxin A into the muscle in the previous year, were excluded.
Patients who were pregnant or who presented with a neuromuscular or
immunosuppressive disease were also excluded from this study.
Botulinum toxin A injection
The masseter muscle on both sides was treated with
botulinum toxin A (Lanzhou Biological Products Institute of China,
Lanzhou, China) at three identical injection sites. After asking
the patients to clench their teeth, the anterior and posterior
borders of the master muscle were identified. The injection points
were below the ear lobe-mouth corner line and ~1.5 cm above the
mandibular angle border. The injection points were in the center of
the lower third of the muscle, 1 cm apart. Injections were
perpendicular to the skin and intramuscular to the middle third of
the needle. The doses of botulinum toxin A were determined
according to the individual severity of masseteric hypertrophy.
Photographs were captured prior to and following the injections at
the baseline and at 2, 8 and 12 weeks following treatment.
RF ablation treatment
Prior to surgery, the masseter muscle margins were
marked with gloss vinyl ink while the patients clenched their jaws.
Subsequently, diagrams for the insertion of the RF probes were
created by drawing several parallel lines on the skin within the
lower third of the masseter muscles. In addition, four to five
horizontal parallel lines and two oblique lines were marked on the
masseter muscles. Surgery was performed in an outpatient room with
the patients under local anesthesia and sedation. All the patients
received 5 mg valium 30 min prior to the procedure for its sedative
effect. Once the patients had gargled with a povidone solution, a
10% xylocaine spray was applied to the oral mucosa. Subsequently,
3.6 ml lidocaine (1%) with 1:100,000 epinephrine solution was
injected evenly into the masseter muscles through the oral mucosa.
Next, 7-mm-long exposed active tips of 120-mm-long insulated needle
electrodes were placed into the masseter muscles. A 17-gauge guide
needle and custom-designed monopolar RF probes (Ellman
International, Inc., New York, NY, USA) were inserted into the
lower third of the masseter muscles, as close to the periosteum of
mandible as possible, in order to prevent any thermal injury to the
adjacent soft tissues, buccal branches of the facial nerves, deep
middle masseteric arteries or Stensen’s ducts. A protective sheath
was used on the proximal portions of the electrodes to diminish any
injury to the oral mucosa. The probes were located slightly below
~30 mm above the gonion, along the posterior border of the masseter
muscles in order to prevent damage to the deep middle masseteric
arteries, which enter the masseter muscles from the external
carotid arteries ~30 mm above the gonion. RF energy (mean power, 40
W±10%) was delivered with monopolar electrodes over a period of
5–10 sec for each spot.
Evaluation
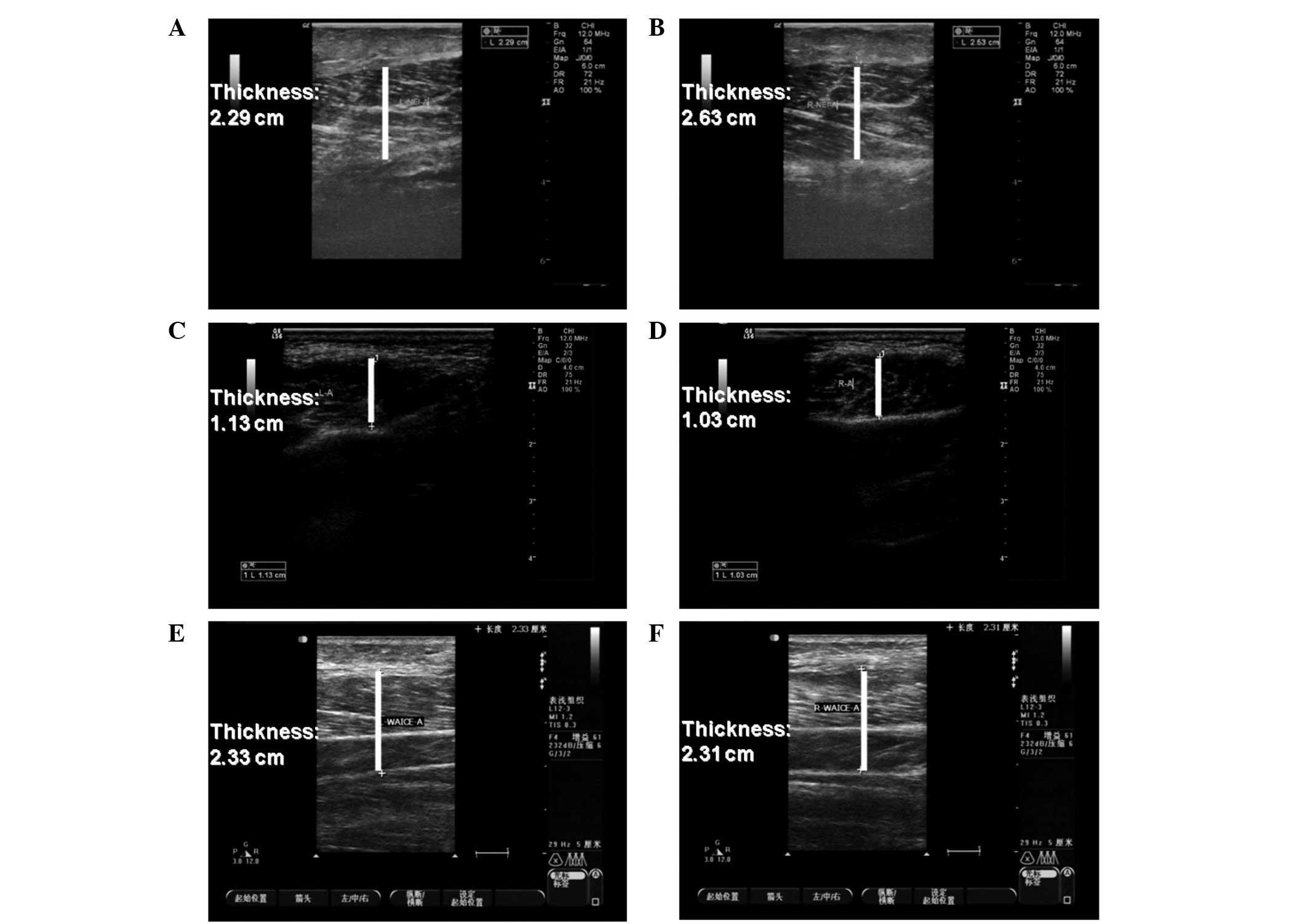
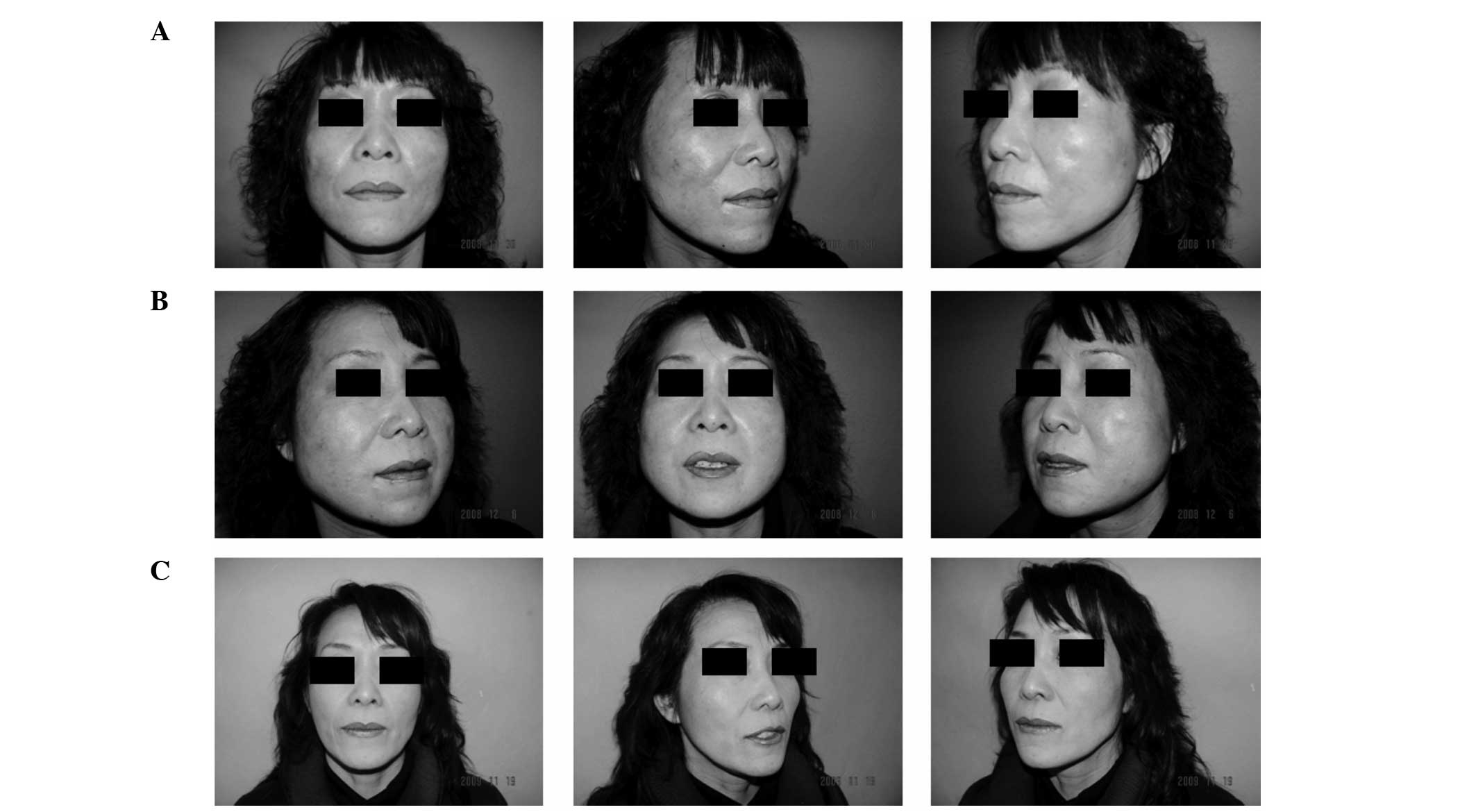
To evaluate the long-term clinical effects, any side
effects were monitored during follow-up. Ultrasound measurements of
the thickness of the masseter muscle under tension were performed
and clinical photographs were captured prior to treatment and at 6
and 12 months following treatment.
Statistical analysis
Data were analyzed using SPSS 11.0 software (SPPS,
Inc., Chicago, IL, USA). The statistical significance of the
difference between the groups was determined with one way analysis
of variance followed by the Bonferroni t-test for multiple
comparisons. P<0.05 was considered to indicate a statistically
significant difference.
Results
Masseteric thickness
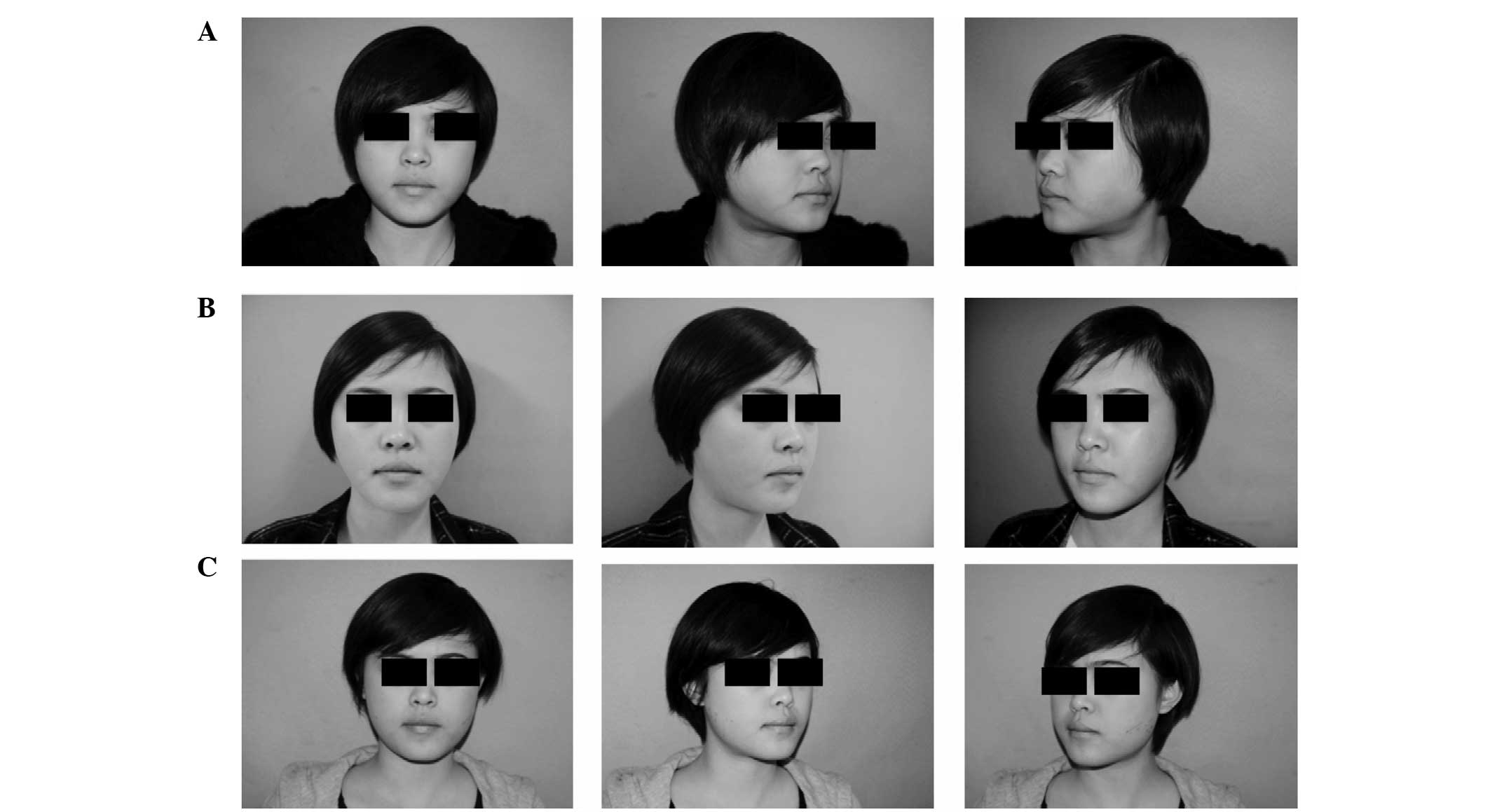
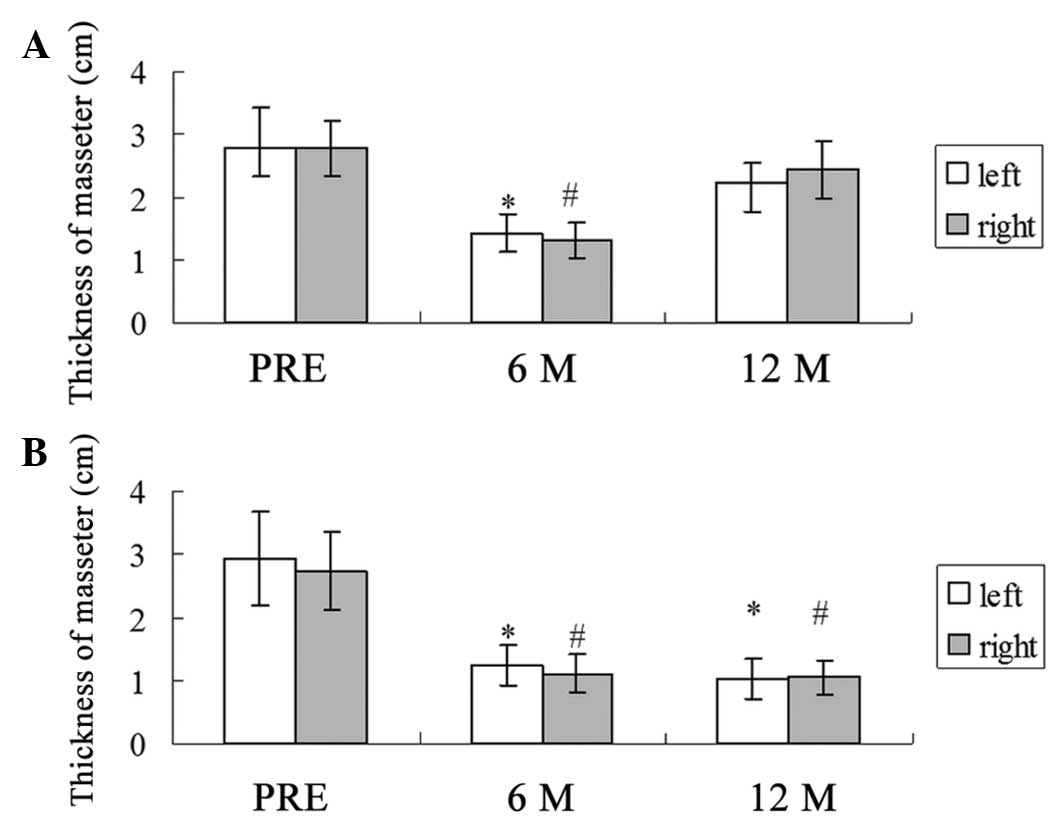
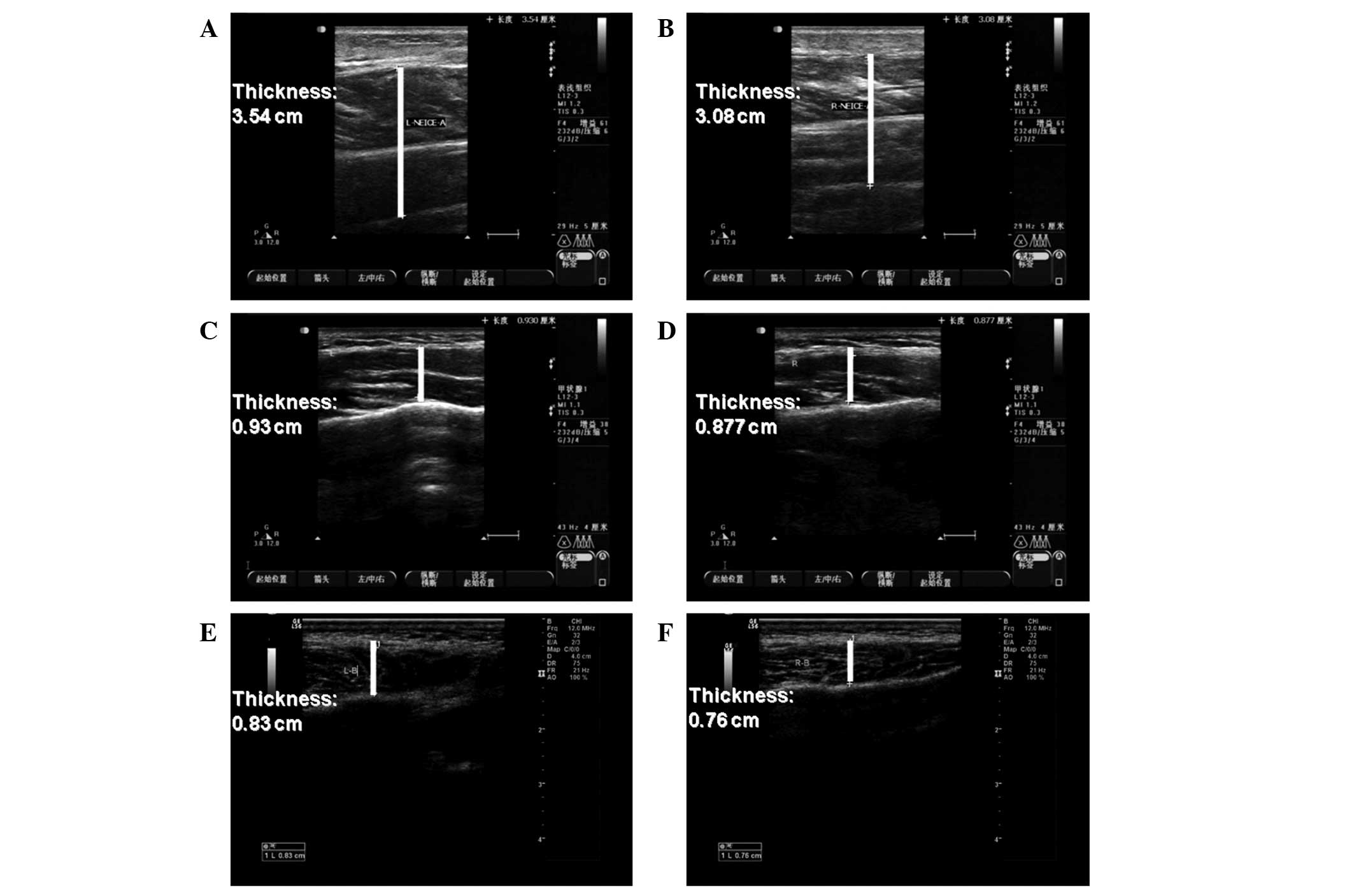
The mean masseteric thicknesses prior to injection
with botulinum toxin A were 2.79 cm on the left side and 2.78 cm on
the right side, as measured by ultrasound. The mean masseteric
thicknesses at 6 and 12 months after injection were 1.43 and 1.31
cm on the left side, and 2.24 and 2.45 cm on the right side,
respectively (Figs. 1, 2 and 3A). The mean masseteric thicknesses prior
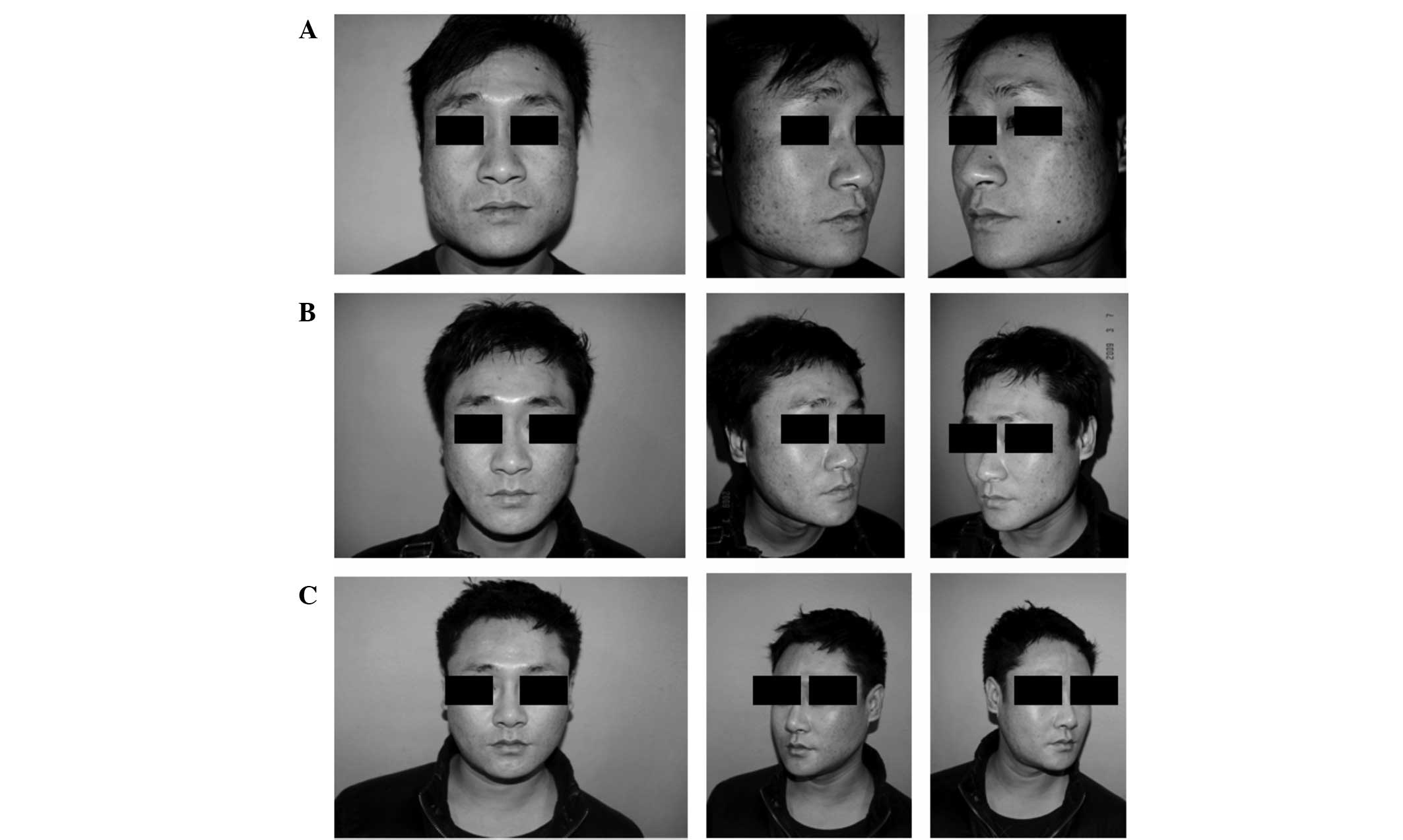
to treatment with RF ablation were 2.93 cm on the left side and
2.73 cm on the right side. The mean masseteric thicknesses at 6 and
12 months following surgery were 1.23 and 1.11 mm on the left side,
and 1.02 and 1.05 cm on the right side, respectively (Figs. 3B, 4 and 5).
In the botulinum toxin A injection group, the masseteric thickness
measured by ultrasound decreased to the lowest point 6 months after
the injections, but increased 12 months following the injection.
However, in the RF ablation treatment group, masseteric thickness
decreased steadily over the 12 months following surgery (Figs. 2, 4 and 5).
Complications
In the botulinum toxin A injection group, the main
local side effects were difficulty in masticating hard food types,
speech disturbance and pain at the injection sites. These
complaints were transient, usually lasting between 1 and 4 weeks
after the injection. Furthermore, facial asymmetry and prominent
zygoma were observed. For those treated with RF ablation, marked
swelling was observed in the treatment area within 1–2 weeks, but
disappeared two weeks later (Fig.
6). One patient demonstrated unilateral intraoperative district
hematoma 3 days after surgery. Pressure was applied with bandages
to the hematoma area for 3 days and the hematoma diminished 2
months later. One patient exhibited little effect 2 months after
the surgery and received a second ablation. Following the second
ablation, the patient was satisfied with the effect. All patients
complained of discomfort while chewing and mouth pain of varying
degrees within 2 weeks of the surgery, however, these discomforts
disappeared spontaneously. No patients complained of injuries to
the facial nerve or of parotid duct or oral dysfunction.
Discussion
Masseteric hypertrophy can be treated with surgical
or non-surgical methods (4,5). It
is difficult to assess the amount and depth of resection of the
masseter muscle during surgical excision. Furthermore, the process
is complex and may result in postoperative complications, including
bleeding, hematoma, facial nerve damage, asymmetry and the
inability to masticate (2,4). Botulinum toxin A injection for the
treatment of masseteric hypertrophy is popular due to the
simplicity of the procedure and the rapid postoperative recovery
times (6). In 2007, Jin Park et
al first reported on the usage of RF ablation for the
correction of masseteric hypertrophy in 340 patients and achieved
favorable clinical results (3). To
date, there have been no studies comparing the treatment and side
effects of injection with botulinum toxin A with those of RF
ablation for the treatment of masseteric hypertrophy.
In the present study, the thickness of the masseter
muscle was analyzed pre- and post-botulinum toxin A injection or RF
ablation treatment in 24 Chinese patients. In the botulinum toxin A
injection group, masseteric thickness decreased to the lowest point
6 months after the injection, but increased until 12 months after
the injection. However, in the RF ablation treatment group, muscle
thickness decreased steadily over the 12 months following
surgery.
The main advantages of injection with botulinum
toxin A when treating masseteric hypertrophy are that the procedure
is easy with fast postoperative recovery (7). Toxin injection was demonstrated to be
safe with no evident complications occurring within two years of
the injection. However, the present study indicated that the
efficacy of botulinum toxin A lasted for a shorter time when
compared with RF ablation. Within 6 months of the injection, the
majority of the participants reported an improvement in their
facial contours. However, in the botulinum toxin A injection
treatment group, the thickness returned to the baseline 12 months
after the injection. Therefore, in order to maintain the
therapeutic effects, the patients usually require repeated
injections.
As demonstrated by the results of the present study,
RF ablation exhibited no serious complications for the treatment of
masseteric hypertrophy. However, a previous study has reported that
a mild injury to the facial nerve and parotid duct may occur
postoperatively (3). In order to
avoid parotid duct and facial nerve injury, in the present study, a
new needle electrode was designed that reduced the amount of
mucosal injury. One patient was unsatisfied with the postoperative
results after receiving RF ablation treatment, which may be due to
the lack of experience when using this newly designed RF ablation
setting. In addition, when assessing the clinical experiences, the
shortcomings of RF ablation included clear swelling 1–2 weeks
following surgery and certain patients were unable to withstand
this therapy. In order to achieve the expected results for the
change in masseter muscle volume, locating an accurate anatomical
location of the masseter muscle is required, as well as having a
good understanding of the performance of the instrument. However,
there are certain advantages to RF ablation therapy when compared
with other therapies. Firstly, the patient may eat after surgery.
Secondly, the biting force of the teeth returns to normal within 3
months of the surgery. Thirdly, 3 months after treatment, the
masseter muscle retains the shrinking trend and the effect appears
stable even at 6 months following surgery. Finally, RF therapy
carries a low risk of injury to the peripheral structures.
Therefore, it may be concluded that injection with botulinum toxin
A and RF ablation therapy are safe and effective treatment options
for masseteric hypertrophy.
The present study had certain limitations. A
split-face study was not conducted on a patient when comparing
these two methods. However, very few patients are willing to accept
such treatments. Furthermore, as this is a single-center study, the
observations of the present study require further verification in a
study with a larger number of patients.
References
|
1
|
Al-Ahmad HT and Al-Qudah MA: The treatment
of masseter hypertrophy with botulinum toxin type A. Saudi Med J.
27:397–400. 2006.PubMed/NCBI
|
|
2
|
Hakam MM, Beheiry MG and Helmy ES:
Surgical management of benign masseteric hypertrophy (B.M.H.).
Egypt Dent J. 41:1435–1440. 1995.PubMed/NCBI
|
|
3
|
Jin Park Y, Woo Jo Y, Bang SI, et al:
Radiofrequency volumetric reduction for masseteric hypertrophy.
Aesthetic Plast Surg. 31:42–52. 2007.PubMed/NCBI
|
|
4
|
Hashimoto T, Kuroda S, Kamioka H, Mishima
K, Sugahara T and Takano-Yamamoto T: Bimaxillary protrusion with
masseter muscle hypertrophy treated with titanium screw anchorage
and masseter surgical reduction. Am J Orthod Dentofacial Orthop.
135:536–548. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Özkan BT, Tabrizi R and Cigerim L:
Management of bilateral masseter muscle hypertrophy. J Craniofac
Surg. 23:14–16. 2012.
|
|
6
|
Peretta R, Melison M, Meneghello R, et al:
Unilateral masseter muscle hypertrophy: morphofunctional analysis
of the relapse after treatment with botulinum toxin. Cranio.
27:200–210. 2009.PubMed/NCBI
|
|
7
|
Andrade NN and Deshpande GS: Use of
botulinum toxin (botox) in the management of masseter muscle
hypertrophy: a simplified technique. Plast Reconstr Surg.
128:24–26. 2012. View Article : Google Scholar : PubMed/NCBI
|