Introduction
Coronary artery fistulas (CAFs), defined as abnormal
vascular communications between any coronary artery and any of the
cardiac chambers or great vessels, are generally noticed
incidentally on diagnostic cardiac catheterization in the adult
population (1). CAF is a type of
rare congenital coronary anomaly. Its actual incidence is unknown.
Symptoms are mainly dependent on the severity of left-to-right
shunt. The majority of the adult cases are generally asymptomatic
and rare, but certain cases cause severe life-threatening events.
At present, various imaging modalities are available for coronary
artery assessment. Due to the complex structural anatomy and the
probability of the multiple fistulas arising from different
segments of the coronary arteries and coronary sinuses,
conventional coronary angiography (CAG) may not be sufficient.
Temporal and spatial resolution of MR angiography and
echocardiography was inferior to that of CAG. Computer tomography
coronary angiography (CTCA) not only non-invasively demonstrates
the origin, structural anatomy of coronary, but also is easy to
follow-up (2). CTCA has been the
most important method for evaluating the coronary artery diseases.
Dual-source computed tomography (DSCT), with two arrays consisting
of an X-ray tube and detectors arranged at a 90° angle and a gantry
rotation time of 330 msec, allows temporal resolution of 83 msec
and provides higher image quality compared with multi-detector CT.
At present, few reports focus on the value of DSCT evaluation of
CAFs. In the present study, we aim to evaluate the incidence and
morphologic features, imaging quality of CAF by the dual-source CT
coronary angiography (DSCT).
Materials and methods
Patients
In total, 19,584 consecutive patients that had
undergone CTCA between January 2011 and January 2013 in two imaging
centers (The Department of Radiology of Beijing Chaoyang Hospital
and The Department of Radiology of Beijing Puren Hospital, Beijing,
China) were retrospectively screened. Each CTCA image was reviewed
by two radiologists using a Picture Archiving Communication System
(Radiology RA 1000 Worksation; GE Healthcare, Fairfield, CT, USA)
and 66 patients were diagnosed with CAFs. Next, the medical records
of these patients were reviewed retrospectively. The ethics
committee of Beijing Chaoyang Hospital and Beijing Puren Hospital
approved the study and written informed consent was provided by all
patients.
DS-CTCA
The DS-CT system (SOMATOM Definition; Siemens
Healthcare, Erlangen, Germany) was used to scan all patients. All
CTCA procedures were performed without heart rate (HR) modulation
by administrating β-blockers. A mechanical injector was used for
intravenous bolus injections of 370 mg/ml iopromide (Ultravist;
Bayer Healthcare Pharmaceuticals, Berlin, Germany) at a flow rate
of 5.0 ml/sec. Coronary contrast was controlled by bolus tracking
in the ascending aorta (signal attenuation threshold, 120 HU). All
injections were followed by further injections of 50 ml saline.
CTCA was performed with the prospective electrocardiogram
(ECG)-triggering or the retrospective ECG-triggering protocols,
according to HR of the patient. If the HR was <70 bpm, the
prospective ECG-triggering scan mode was selected, but if the HR
was ≥70 bpm, the retrospective ECG-triggering scan mode was used.
The ECG-triggering CTCA scanned with the following parameters:
Detector collimation, 2×32×0.6 mm; slice acquisition, 2×64×0.6 mm
by the means of a z-flying focal spot; and gantry rotation time,
330 msec. Tube current was adapted automatically to the weight of
each patient using CARE Dose 4D automatic exposure control (Siemens
Healthcare) and a reference tube current of 320 mAsec was used. A
tube voltage of 120 kV was selected when the body mass index (BMI)
of the patient was ≥24 kg/m2, while 100 kV was selected
when the BMI was <24 kg/m2. For the retrospective
ECG-triggering protocol, the ECG-pulsing window was set at 35–75%
of the RR interval with a pitch of 0.2–0.43, which was
automatically adapted to the HR.
Image quality and reconstruction
All CTCA images were transferred to a dedicated
workstation (ADW 4.2; GE Healthcare) and reconstructed by a
cardiovascular radiologist with ten years’ experience. CAF was
assessed by two radiologists with consensus. Following the
evaluation of axial and oblique multiplanar reconstructions, other
rendering methods were used to create images, including
three-dimensional volume-rendered (VR), curved multiplanar and
maximum intensity projection (MIP) images. Image quality was
assessed using the following four point scale: Excellent, no
artifacts, unrestricted evaluations of the fistula; good, minor
artifacts, good diagnostic quality; adequate, moderate artifacts,
acceptable diagnostic quality; unacceptable, severe artifacts
impairing accurate evaluation. The origin vessels, draining veins,
presence of aneurysm, combined congenital or acquired anomaly and
the relationship with adjacent structures were assessed from the
axial and the reformatted images together.
Results
Diagnosis of CAFs
Among the 19,548 cases, CAFs were diagnosed in 66
patients (female, 37; male, 29; age, 35–79 years, mean, 58.1±10.1
years), an incidence of 0.34% (66/19,548). A total of 52 patients
were examined by the retrospective ECG-triggering protocol. For
this method the mean dose length product (DLP) was 611.0±266.5
mGy·cm, corresponding to an effective dose estimation of 13.8±5.1
mSv. The remaining 14 patients were examined by the prospective
ECG-triggering protocol in the 70%-RR interval (mean HR, 58±5 bpm).
The mean DLP was 207.3±57.7 mGy·cm, which corresponded to an
effective dose estimation of 4.1±1.9 mSv. The image quality was
excellent for 61 patients and moderate for 5 patients. None of the
images were considered to be of adequate or unacceptable
quality.
Diagnosis of coronary pulmonary artery
fistulas (CPAFs) and coronary left ventricular fistulas
Among the 66 patients with CAFs, 60 patients were
diagnosed with having a CPAF (female, 35; male, 25; age, 39–79
years, mean, 58.1±10.5 years) and the remaining six patients were
diagnosed with a coronary left ventricular fistula (female, 2;
male, 4; age, 54–65 years). The incidence of CPAF was 0.31%
(60/19,548). Invasive CAG was performed in 10 patients (female, 3;
male, 7; age, 51–72 years), which included six cases of CPAFs and
four cases of coronary left ventricular fistulas. The CTCA and CAG
observations of these 10 patients are summarized in Table I. Four patients with CPAFs were
treated with fistula coiling.
 | Table ICTCA and CAG observations of patients
with CAFs. |
Table I
CTCA and CAG observations of patients
with CAFs.
| Patient | Age, years | Gender | CTCA
observations | CAG observations |
|---|
| 1 | 63 | F | LAD-PA | LAD-PA
Transcatheter closure of coronary artery to pulmonary artery
coil |
| 2 | 56 | M | LAD-PA-RCA | LAD-PA-RCA |
| 3 | 61 | M | LMA-PA | LMA-PA
Transcatheter closure of coronary artery to pulmonary artery
coil |
| 4 | 67 | M | RCA-PA | RCA-PA
Transcatheter closure of coronary artery to pulmonary artery
coil |
| 5 | 64 | M | LAD-PA-RCA | LAD-PA-RCA |
| 6 | 51 | M | LMA-PA | LMA-PA
Transcatheter closure of coronary artery to pulmonary artery
coil |
| 7 | 54 | M | LAD-LV | LAD-LV |
| 8 | 68 | F | RCA-LV | RCA-LV |
| 9 | 72 | M | LAD-LV | LAD-LV |
| 10 | 65 | F | RCA-LV | RCA-LV |
Clinical presentations
Among the 66 patients, 40 patients undergoing CTCA
presented with chest pain, five patients presented with chest
tightness and syncope and one patient had heart failure. Six cases
had already been diagnosed with coronary artery disease, four cases
were under follow-up observation and 10 patients were suspected of
ischemic heart disease from other tests. Using CTCA, 36 patients
were diagnosed with isolated CAFs without other cardiac diseases or
malformations, 25 patients were found to have lipid or calcified
plaques, four patients had coronary myocardial bridges and two
patients had undergone coronary angioplasty. DS-CTCA observations
are summarized in Table II.
| Table IICTCA observations of patients with
CAFs. |
Table II
CTCA observations of patients with
CAFs.
| CTCA
manifestation | Patients, n |
|---|
| CAF | 66 |
| CPAF | 60 |
| Coronary left
ventricular fistula | 6 |
| Isolated CAF | 36 |
| Isolated CPAF | 35 |
| Isolated coronary
left ventricular fistula | 2 |
| Lipid or calcified
plaque | 25 |
| Coronary artery
stenosis >50% | 5 |
| Percutaneous
transluminal coronary angioplasty | 2 |
| Myocardial
bridging | 4 |
| Coronary
aneurysm | 1 |
| Permanent left
superior vena cava | 1 |
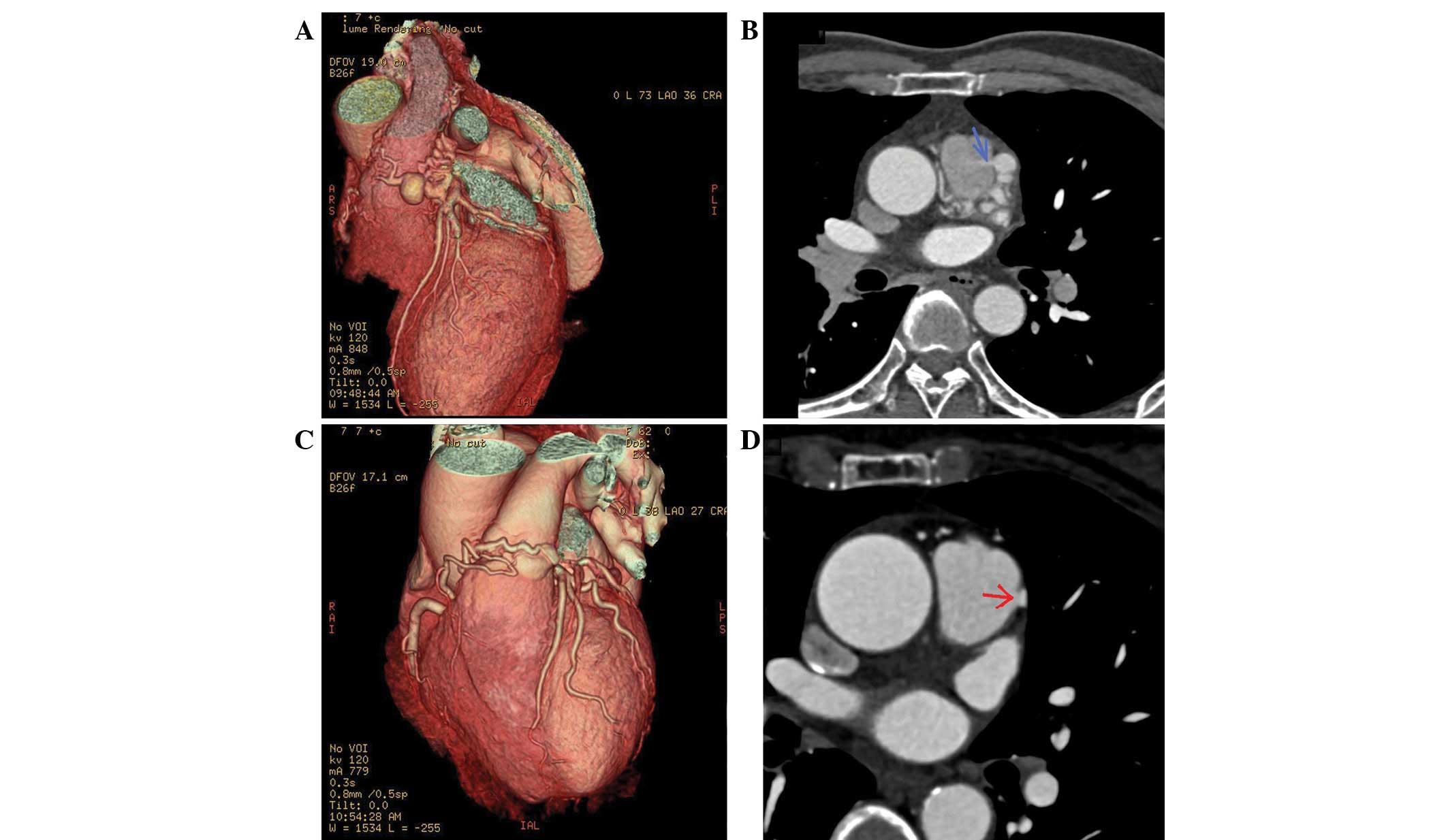
Fistula locations
In 24 patients, CPAFs were identified as small and
tortuous vessels (Fig. 1), while
in 36 patients, CPAFs were identified as dilated vessels close to
the surface of the pulmonary artery (PA). The drainage sites were
located on the left lateral side of the pulmonary trunk in 54
patients and on the anterior side of the pulmonary trunk in six
patients. Small aneurysms of fistula vessels were identified in 11
patients (Fig. 1A). The mean
diameter of the detected fistulas, measured with CTCA, was 3.1±1.9
mm (range, 1.4–13.3 mm). A high-density flow jet of contrast agent
shunting from the fistula into the low density PA was observed in
46 CPAF cases(Fig. 1B) and small
defects of the PA wall, without shunting flow jet, were observed in
14 patients (Fig. 1C and D).
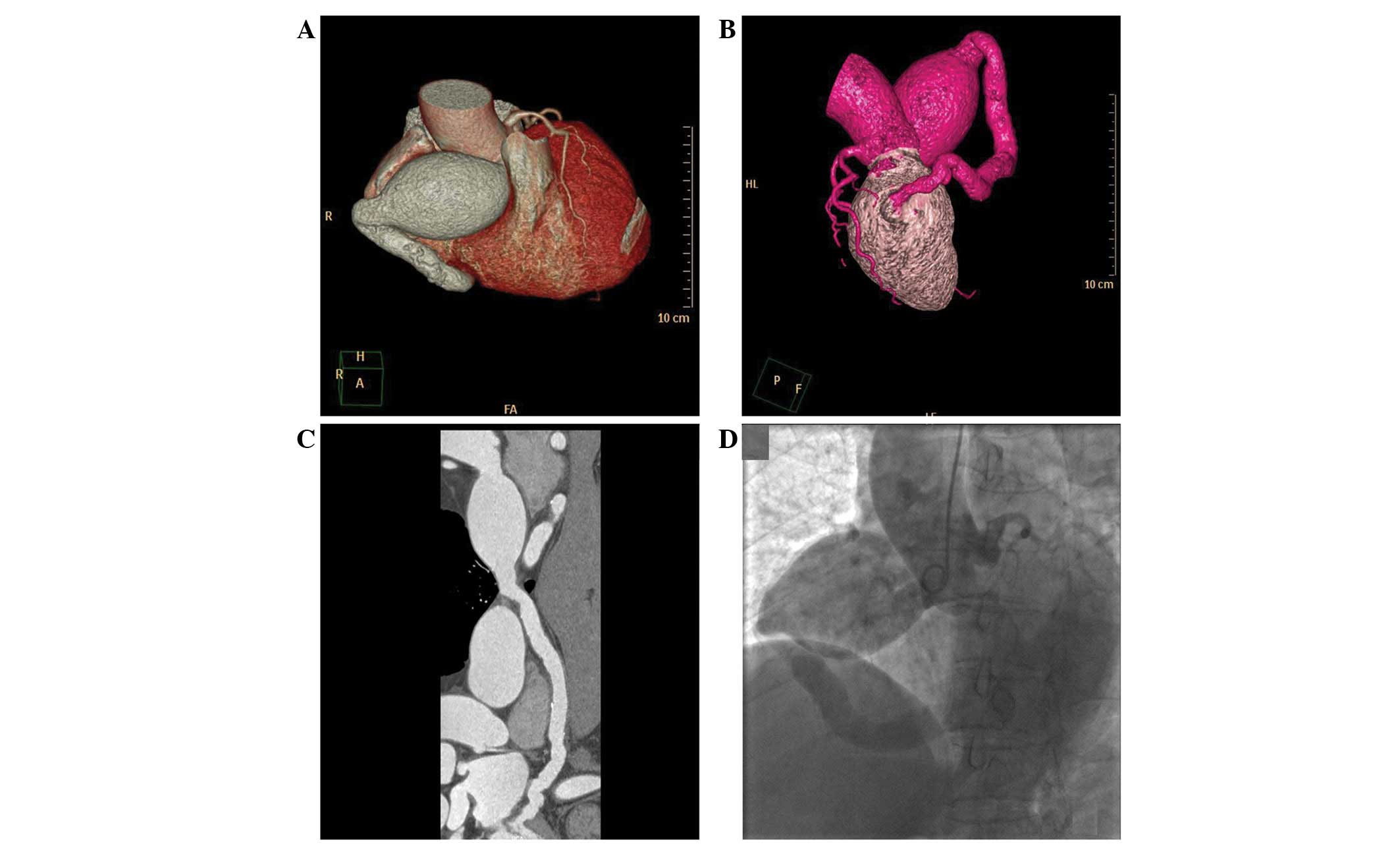
From the CTCA images, coronary left ventricular
fistulas in six patients were identified in the dilated vessels
draining into the posterior wall of the left ventricle (LV).
Moreover, a large right coronary aneurysm was observed in one
patient with a large fistula of the right coronary artery (RCA) to
the LV (Fig. 2).
Fistula origins
In the 66 patients with CAFs, 54 patients had one
fistula that could be traced and the remaining 12 patients were
shown to have two fistula vessels. It was shown that 31 cases
(47.0%) originated from the left coronary artery (LCA), 26 cases
(39.4%) originated from the RCA and 9 cases (13.6%) originated from
the LCA and RCA. Among the 60 CPAF patients, 29 cases (48.3%)
originated from the LCA, 22 cases (36.7%) originated from the RCA
and nine cases (15%) originated from the LCA and RCA. Among the 29
cases that originated from the LCA, 27 cases were found to
originate from the left anterior descending artery (LAD) and two
cases from the left main artery (LMA). Among the nine cases
originating from the LCA and RCA, two cases originated from the LMA
and proximal RCA and seven cases originated from the LAD and
proximal RCA. Among the six detected coronary left ventricular
fistula cases, the fistula vessels were found to originate from the
RCA in four patients and the LAD in two patients and lead to the
LV.
Discussion
In total, 19,548 patients that had undergone DS-CTCA
were included in the study, which to the best of our knowledge is
the largest study cohort from two centers. Only 66 patients with
CAFs were detected using CTCA, which was an incidence rate of
0.34%. CAFs are rare congenital malformations that are highly
variable. The majority of cases are generally asymptomatic;
however, specific cases can cause severe life threatening events
(4,5). CAFs were accidentally identified
during routine cardiac catheterization in patients suspected of
having atherosclerotic coronary artery disease and since then CAG
has been used as the standard modality for diagnosis (6). The incidence of CAFs in the adult
population is reported to be 0.05% (7). In the present study, 66 patients
(66/19,548) were diagnosed with CAFs using CTCA and only 10 of the
patients (10/66) with CAFs were examined by CAG for the
investigation of significant symptoms and the other 56 patients
choose a long-time follow-up. Therefore, the true incidence of CAFs
is highly speculative since numerous CAF cases are symptomless and
may not be detected. The present study revealed the incidence of
CPAFs to be 0.31% using DS-CTCA, which is consistent with the
incidence of 0.32% indicated by 64-slice multidetector-CT (2).
DS-CT performed with two arrays consisting of an
X-ray tube, detectors arranged at a 90° angle and a gantry rotation
time of 330 msec, allows temporal resolution of 83 msec and
provides higher image quality compared with that of
multidetector-CT (3). The scanning
mode was selected according to the HR and BMI of the patients.
Patients with significant arrhythmia were not recommended to
undergo a CTCA scan. In the present study, the image quality was
not considered to be unacceptable for any of the patients, despite
HR not being controlled prior to CTCA. A total of 52 patients were
examined by the retrospective ECG-triggering protocol and 14
patients were examined by the prospective ECG-triggering protocol.
The prospective method uses a significantly lower radiation dose
compared with that used by the retrospective ECG-gated technique.
This indicates that the prospective ECG-triggering protocol
provides the clear anatomy of CAFs with a lower radiation dose.
Moreover, the use of multiplanar reformatted images clearly
demonstrates the site of origin, the termination of abnormal blood
vessels and small defects of the pulmonary wall. VR images provided
an excellent overview of the cardiac and vascular anatomy. From the
MIP images, a high-density flow jet of contrast agent shunting from
the fistula into the low density PA was clearly observed and small,
tortuous or dilated vessels close to the surface of the PA were
clearly demonstrated in VR images. These were the direct
manifestations of CAFs in CTCA.
There have been numerous types of CAF reported. Over
90% of fistulas reported drain into the venous circulation and the
most common drainage site is the right ventricle (8). CPAFs constitute 15–30% of all CAF
cases (9). However, Kim et
al (2) indicated that CPAFs
account for 89.5% of CAF cases. In the present study, the most
common CAF was CPAF, which is consistent with the study by Yun
et al (10). The other six
patients were diagnosed with coronary left ventricular fistulas.
The present study indicated that CPAFs accounted for 91% of the CAF
cases.
It has been reported (11) that ~50% of CAF cases arise from the
RCA, ~42% from the LCA and ~5% from the RCA and LCA. In the present
study, the CAFs originated from the RCA in 39.4% of patients, the
LCA in 47.0% and the RCA and LCA in 13.6% of patients. The
incidence of CAFS arising from the RCA and LCA in the present study
is less than the 22.9% reported by Yun et al (10). In the CPAF group, the most common
drainage coronary artery was the LAD followed by the proximal RCA
and then the LMA.
Clear guidelines for the treatment of CPAFs have not
yet been established. According to Liberthson et al
(12), patients ≥20 years old who
have undergone coronary arteriovenous fistula ligation have an
increased probability of complications (23%), including
postoperative mortality (7%) and myocardial infarction (7%).
However, in the present study, there were no patients <20
years-old and the patients that received treatment did not develop
any of the aforementioned problems.
The main limitation of the present study is that it
is a retrospective study. Although the image quality was acceptable
for each case, the majority of cases underwent CTCA with the
retrospective ECG-triggering protocol, leading to a higher
radiation dose compared with that used in the prospective
ECG-triggering method. A number of studies have indicated that the
prospective ECG-triggering protocol is successful in providing
acceptable image quality with a significant reduction of radiation
dose, even in patients with a high HR. Only 14 patients in the
current study were scanned by this method and the CAFs were
depicted clearly with a lower radiation dose. Therefore, the
prospective ECG-triggering protocol should be used for evaluating
CAFs in future practice. Patients who underwent CTCA were suspected
of having coronary artery disease. However, the majority of cases
of CAF are generally asymptomatic. This indicates that the true
incidence of CAF in the population is not clear.
In conclusion, the incidence of CAFs detected by
DS-CTCA in the present study was 0.34%. DS-CTCA is a reliable
noninvasive tool that allows accurate the delineation of CAFs and
provides detailed three-dimensional anatomical information.
References
|
1
|
Meyer J, Reul GJ, Mullins CE, McCoy J,
Hallman GL and Cooley DA: Congenital fistulae of the coronary
arteries. Clinical considerations and surgical management in 23
patients. J Cardiovasc Surg (Torino). 16:506–511. 1975.PubMed/NCBI
|
|
2
|
Kim MS, Jung JI and Chun HJ: Coronary to
pulmonary artery fistula: morphologic features at multidetector CT.
Int J Cardiovasc Imaging. 26(Suppl 2): 273–280. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sabarudin A, Md Yusof AK, Tay MF, Ng KH
and Sun Z: Dual-source CT coronary angiography: effectiveness of
radiation dose reduction with lower tube voltage. Radiat Prot
Dosimetry. 153:441–447. 2013.PubMed/NCBI
|
|
4
|
Sherwood MC, Rockenmacher S, Colan SD and
Geva T: Prognostic significance of clinically silent coronary
artery fistulas. Am J Cardiol. 83:407–411. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lau G: Sudden death arising from a
congenital coronary artery fistula. Forensic Sci Int. 73:125–130.
1995. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Gowda RM, Vasavada BC and Khan IA:
Coronary artery fistulas: clinical and therapeutic considerations.
Int J Cardiol. 107:7–10. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Cebi N, Schulze-Waltrup N, Frömke J,
Scheffold T and Heuer H: Congenital coronary artery fistulas in
adults: concomitant pathologies and treatment. Int J Cardiovasc
Imaging. 24:349–355. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lin FC, Chang HJ, Chern MS, Wen MS, Yeh SJ
and Wu D: Multiplane transesophageal echocardiography in the
diagnosis of congenital coronary artery fistula. Am Heart J.
130:1236–1244. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Dodge-Khatami A, Mavroudis C and Backer
CL: Congenital heart surgery nomenclature and database project:
anomalies of the coronary arteries. Ann Thorac Surg. 69(4 Suppl):
S270–S297. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Yun H, Zeng MS, Yang S, Jin H and Yang X:
Congenital coronary artery fistulas: dual-source CT findings from
consecutive 6,624 patients with suspected or confirmed coronary
artery disease. Chin Med J (Engl). 124:4172–4177. 2011.PubMed/NCBI
|
|
11
|
Nakamura M, Matsuoka H, Kawakami H, et al:
Giant congenital coronary artery fistula to left brachial vein
clearly detected by multidetector computed tomography. Circ J.
70:796–799. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Liberthson RR, Sagar K, Berkoben JP,
Weintraub RM and Levine FH: Congenital coronary arteriovenous
fistula. Report of 13 patients, review of the literature and
delineation of management. Circulation. 59:849–854. 1979.
View Article : Google Scholar : PubMed/NCBI
|