Introduction
Thrombocytosis can be induced by a number of primary
and secondary factors. Primary thrombocytosis is a type of
myeloproliferative disease with 50–70% of patients exhibiting
mutations in the JAK2V617F gene and PLT levels
>600×109/l and even up to 1,000×109/l
(1). Secondary thrombocytosis is
caused by drugs or other diseases, including inflammation,
infection, rheumatism, anemia and malignancy, where patients
exhibit moderately increased PLT levels that are between 400 and
800×109/l (2–4). After excluding the diagnosis of
essential thrombocythemia, preoperative cancer patients with a PLT
count of >400×109/l are considered to have secondary
thrombocytosis (5–7). However, the threshold remains
controversial.
Since the 1980s, the phenomenon that a comorbidity
between blood hypercoaguable state and malignant solid tumors has
caused widespread concerned and been increasingly studied. Although
the specific mechanism is not completely understood, the
association between thrombocythemia and the hypercoagulability
state has been confirmed repeatedly (8). Prior to the evidence that malignant
tumors lead to coagulation abnormality, Riess firstly proposed the
symptoms of unexplained thrombocytosis in malignancies (9). Previously, thrombocytosis, as a
paraneoplastic syndrome, has been successively identified in oral
squamous cell, renal cell and hepatocellular carcinomas, as well as
lung, esophageal, gastric (GC), colorectal, pancreatic and
gynecological cancers (2,10–12).
Numerous studies agree that malignancies with
unknown causes of thrombocytosis may be a valuable adjuvant
parameter in predicting the prognosis of cancer (2,4,5,11).
However, the complex effect of thrombocytosis in malignancy has
been rarely reported. GC is the second most common malignancy in
China, however, there are few specific early clinical
manifestations and accurate predictors of prognosis. Therefore, GC
patients with a high risk of recurrence may benefit from a reliable
predicting indictor. In the present study, associations between
thrombocytosis and clinicopathological features, survival time and
tumor recurrence were systematically investigated in GC patients.
The aim was to provide a new approach in the diagnosis and
prognosis of GC.
Methods and methods
Definition of the blood test
indicator
Primary thrombocytosis was eliminated using bone
marrow cytomorphological examinations, and thrombocytosis was
diagnosed as a PLT count >400×109/l, which was in
accordance with other studies (5,7,13).
As the normal PLT count of patients at the First Affiliated
Hospital of Wenzhou Medical College (Wenzhou, China) ranges between
100 and 300×109/l, individuals with a PLT count
>300×109/l were also analyzed. Carcinoembryonic
antigen (CEA), carbohydrate antigen 19-9 (CA19-9), D-dimer,
fibrinogen, prothrombin time (PT) and activated partial
thromboplastin time (APTT) standards were as follows: 0–5 μg/l;
0–37 U/ml; 0–0.5 mg/l; 2–4 g/l; 11–13 sec; and 30–45 sec,
respectively. Sodium citrate anticoagulated blood samples were
collected and analyzed with a COULTER Gen-S automatic blood
analyzer (Beckman Coulter, Inc., Miami, FL, USA) and Stago STA-R
Evolution automatic coagulometer (Diagnostica Stago, Inc., Beijing,
China).
Patients
A total of 1,763 patients who underwent surgical
treatment for GC in the First Affiliated Hospital of Wenzhou
Medical University between July 2005 and June 2008 were eligible
for retrospective review in the study. None of the patients had
received radiation therapy or chemotherapy prior to surgery, but
had received strict chemical therapy following surgery, according
to the National Comprehensive Cancer Network GC guidelines.
Histopathological diagnosis of gastric adenocarcinoma was confirmed
by the Pathology Department following surgery, according to the
World Health Organization’s criteria. In total, 71 patients with GC
and thrombocytosis were enrolled in study cohort A. These patients
had a mean age of 63±9.15 years (range, 27–84 years). A total of
213 patients with a PLT count >300×109/l were
included in study cohort B and these individuals had a mean age of
63±10.02 years (range, 27–84 years). Control group A comprised 107
patients with benign gastric lesions that had a mean age of 41±6.33
years (range, 23–66 years). Control group B comprised 100 cases
that had been randomly selected from 1,550 GC individuals with
normal PLT counts. The mean age was 66±8.46 years (range, 34–88
years).
Blood samples were collected from the individuals
within 1 week prior to surgery, ~4 weeks following surgery and
during the follow-up period. B-mode ultrasound and physical
examinations were performed postoperatively for patients with major
complaints to assess the status of deep vein thrombosis (DVT).
Imageological examinations, including computed tomography (CT) and
enhanced CT scans, were performed to assess recurrence during the
follow-up period. Informed written consent was provided by each
patient and the study was approved by the Human Research Ethics
Committee of the First Affiliated Hospital of Wenzhou Medical
University.
Statistical analysis
Associations between thrombocytosis and
clinicopathological features were analyzed using the χ2
test, Fisher’s exact test, independent sample t-test, Pearson’s
correlation test and logistic regression analysis. A Kaplan-Meier
survival curve and Cox regression model were used to evaluate the
clinical significance of thrombocytosis in GC. Area under the
receiver operating characteristic curve (AUROC) and the Z-test were
applied to analyze the sensitivities and specificities of PLTs in
predicting recurrence. P<0.05 was considered to indicate a
statistically significant difference. All analyses were performed
using SPSS version 16.0 for Windows (SPSS, Inc., Chicago, IL,
USA).
Results
Thrombocytosis in GC patients
As shown in Table
I, when compared with control group A (benign gastric lesion,
0%, 0/107), the morbidity [4.03%, 71/1,763; 95% confidence interval
(CI), 3.11–4.94] of GC patients with thrombocytosis (PLT
>400×109/l) increased significantly (P=0.014). This
was also observed in patients with a PLT count
>300×109/l (12.08%, 213/1,763; 95% CI, 10.56–13.60;
P<0.001).
 | Table IThrombocytosis in patients with
gastric carcinomas or benign gastric lesions. |
Table I
Thrombocytosis in patients with
gastric carcinomas or benign gastric lesions.
| | PLT
>300×109/l | PLT
>400×109/l |
|---|
| |
|
|
|---|
| Group | PLT
≤300×109/l, n | n | P-value | n | P-value |
|---|
| Gastric
carcinoma | 1,550 | 213 | <0.001 | 71 | 0.014a |
| Benign gastric
lesions | 106 | 1 | | 0 | |
Correlation between thrombocytosis and
clinicopathological features
As shown in Table
II, the incidence of thrombocytosis, defined as a PLT count
>400×109/l, exhibited statistically significant
differences when compared with the normal PLT cohort in tumor size
(P<0.001), tumor, node and metastasis (TNM) classification
(particularly for phase I, P=0.002) and depth of penetration
(P=0.003). No statistically significant differences were identified
in age, tumor location, type, degree of differentiation, vascular
invasion, perineural invasion, lymphatic invasion, distant
metastasis or tumor markers CEA/CA19-9 (P>0.05). The same result
was verified in patients with a PLT count >300×109/l
with regard to tumor size (P=0.001), TNM classification
(P<0.001) and penetration (P<0.001). Analysis of enumeration
data revealed that no statistical significance existed between
thrombocythemia and clinicopathological features in the cancer
group (data not shown). In addition, to exclude the interaction
between tumor size, type, differentiation, lymphatic invasion,
penetration and TNM classification, risk assessments were used to
measure the effect of these independent variables on
thrombocytosis. Tumor size [P=0.002; odds ratio (OR), 2.179; 95%
CI, 1.347–3.526], TNM classification (P<0.001; OR, 1.763; 95%
CI, 1.317–2.360) and depth of penetration (P=0.001; OR, 1.643; 95%
CI, 1.232–2.191) functioned as moderate positive factors for the
occurrence of thrombocythemia.
| Table IIThrombocytosis and clinicopathological
variables in GC. |
Table II
Thrombocytosis and clinicopathological
variables in GC.
| | PLT
>300×109/l | PLT
>400×109/l |
|---|
| |
|
|
|---|
| Variable | PLT
≤300×109/l, n | n | P-value | n | P-value |
|---|
| Age, years |
| <60 | 39 | 75 | 0.516 | 24 | 0.488 |
| ≥60 | 61 | 138 | | 47 | |
| Location |
| Upper third | 20 | 31 | 0.082 | 10 | 0.339 |
| Middle third | 36 | 105 | | 33 | |
| Lower third | 44 | 77 | | 28 | |
| Tumor size, cm |
| <5 | 58 | 79 | 0.001 | 21 | <0.001 |
| ≥5 | 42 | 134 | | 50 | |
| Type |
|
Adenocarcinoma | 98 | 198 | 0.191a | 67 | 0.263a |
| Squamous
carcinoma | 0 | 3 | | 1 | |
|
Undifferentiated | 2 | 12 | | 3 | |
| Degree of
differentiation |
| Well | 15 | 19 | 0.242 | 10 | 0.886 |
| Moderate | 17 | 38 | | 10 | |
| Poor | 66 | 156 | | 48 | |
| Vascular
invasion |
| Present | 34 | 67 | 0.653 | 29 | 0.422 |
| Absent | 66 | 146 | | 42 | |
| Perineural
invasion |
| Present | 37 | 80 | 0.924 | 26 | 0.959 |
| Absent | 63 | 133 | | 45 | |
| Lymphatic
invasion |
| Present | 71 | 174 | 0.172 | 57 | 0.168 |
| Absent | 29 | 49 | | 14 | |
| TNM
classification |
| I | 21 | 12 | <0.001 | 1 | 0.002a |
| II | 21 | 49 | | 16 | |
| III | 44 | 105 | | 39 | |
| IV | 14 | 47 | | 15 | |
| Depth of
penetration |
| T1 | 18 | 10 | <0.001 | 1 | 0.003a |
| T2 | 4 | 15 | | 5 | |
| T3 | 53 | 97 | | 37 | |
| T4 | 25 | 91 | | 28 | |
| Distant
metastasis |
| Present | 86 | 166 | 0.093 | 56 | 0.221 |
| Absent | 14 | 47 | | 15 | |
| CEA |
| Abnormal | 23 | 43 | 0.570 | 22 | 0.305 |
| Normal | 77 | 170 | | 49 | |
| CA19-9 |
| Abnormal | 25 | 55 | 0.877 | 19 | 0.795 |
| Normal | 75 | 158 | | 52 | |
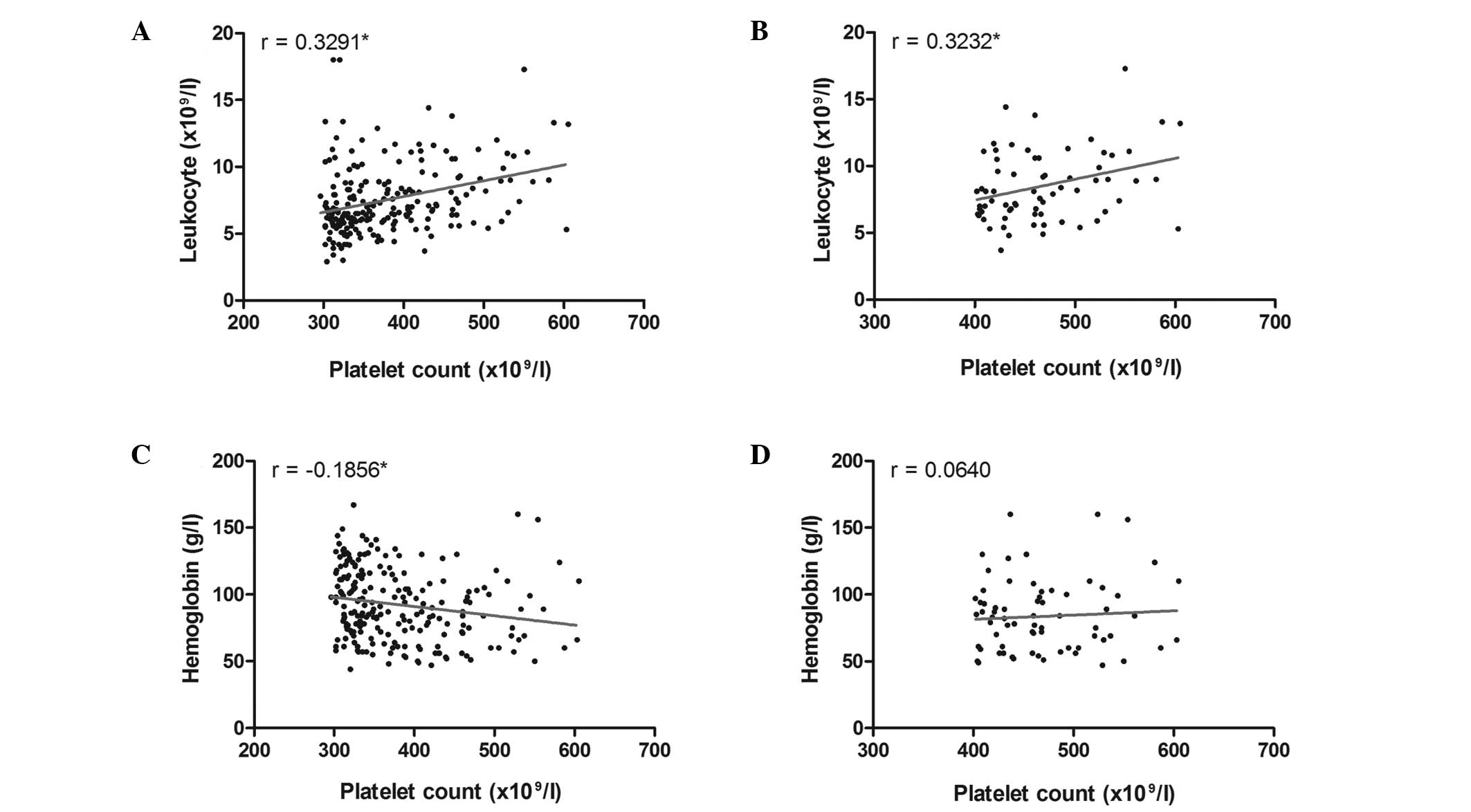
The mean pretreatment PLT count for thrombocytosis
patients was 469.23±53.99×109/l (range,
402–605×109/l), the leukocyte count was
8.54±2.61×109/l (range, 3.7–17.3×109/l) and
the hemoglobin concentration was 83.51±26.68 g/l (range, 47–160
g/l). The mean PLT count for GC patients that had preoperative PLT
levels >300×109/l in study group B was
379.92±73.23×109/l (range, 302–605×109/l),
while the leukocyte count was 7.81±3.95×109/l (range,
2.9–20.6×109/l) and the hemoglobin concentration was
92.61±27.14 g/l (range, 44–167 g/l). A significant positive linear
correlation was identified between the PLT and leukocyte counts
when the PLT count was >300 or 400×109/l (r=0.3291;
P<0.001; and r=0.3232; P=0.006, respectively; Fig. 1A and B). However, a correlation
between the PLT count and hemoglobin concentration was only
verified in patients with a PLT count >300×109/l
(r=−0.1856; P=0.006; Fig. 1C),
since P=0.599 for patients with a PLT count
>400×109/l (Fig.
1D).
Correlation between thrombocytosis and
the blood hypercoagulable state
Although ultrasonic examinations did not reveal any
statistically significant differences between the control group and
study cohorts with PLT count >300×109/l or
400×109/l (P=0.444 and 0.083, respectively), DVT was
more likely to affect tumor patients with thrombocytosis (7.04%,
5/71) than patients with a PLT count >300×109/l
(3.29%, 7/213). Abnormal D-dimer and fibrinogen concentrations
occurred more frequently in patients with thrombocytosis
(PLT>400×109/l; P=0.004 and 0.013, respectively), but
no statistically significant differences were observed when the
threshold was defined as 300×109/l. In addition, no
correlation was observed between the occurrence of anomalous PLT
counts and decreased PT/APTT (Table
III). As aforementioned, the enumeration data of thrombocytosis
demonstrated that no statistical significance was present between
the cancer groups with regard to blood hypercoagulability (data not
shown).
| Table IIIThrombocytosis and coagulation
markers in GC. |
Table III
Thrombocytosis and coagulation
markers in GC.
| | PLT
>300×109/l | PLT
>400×109/l |
|---|
| |
|
|
|---|
| Variable | PLT
≤300×109/l, n | n | P-value | n | P-value |
|---|
| PT |
| Decreased | 8 | 28 | 0.158 | 12 | 0.071 |
| Normal | 90 | 175 | | 57 | |
| APPT |
| Decreased | 11 | 30 | 0.465 | 13 | 0.204 |
| Normal | 83 | 172 | | 56 | |
| Fibrinogen |
| Normal | 83 | 158 | 0.061 | 51 | 0.042 |
| Increased | 15 | 52 | | 20 | |
| D-dimer |
| Normal | 87 | 172 | 0.172 | 51 | 0.013 |
| Increased | 13 | 41 | | 20 | |
| DVT |
| Present | 1 | 7 | 0.444a | 5 | 0.083a |
| Absent | 99 | 206 | | 66 | |
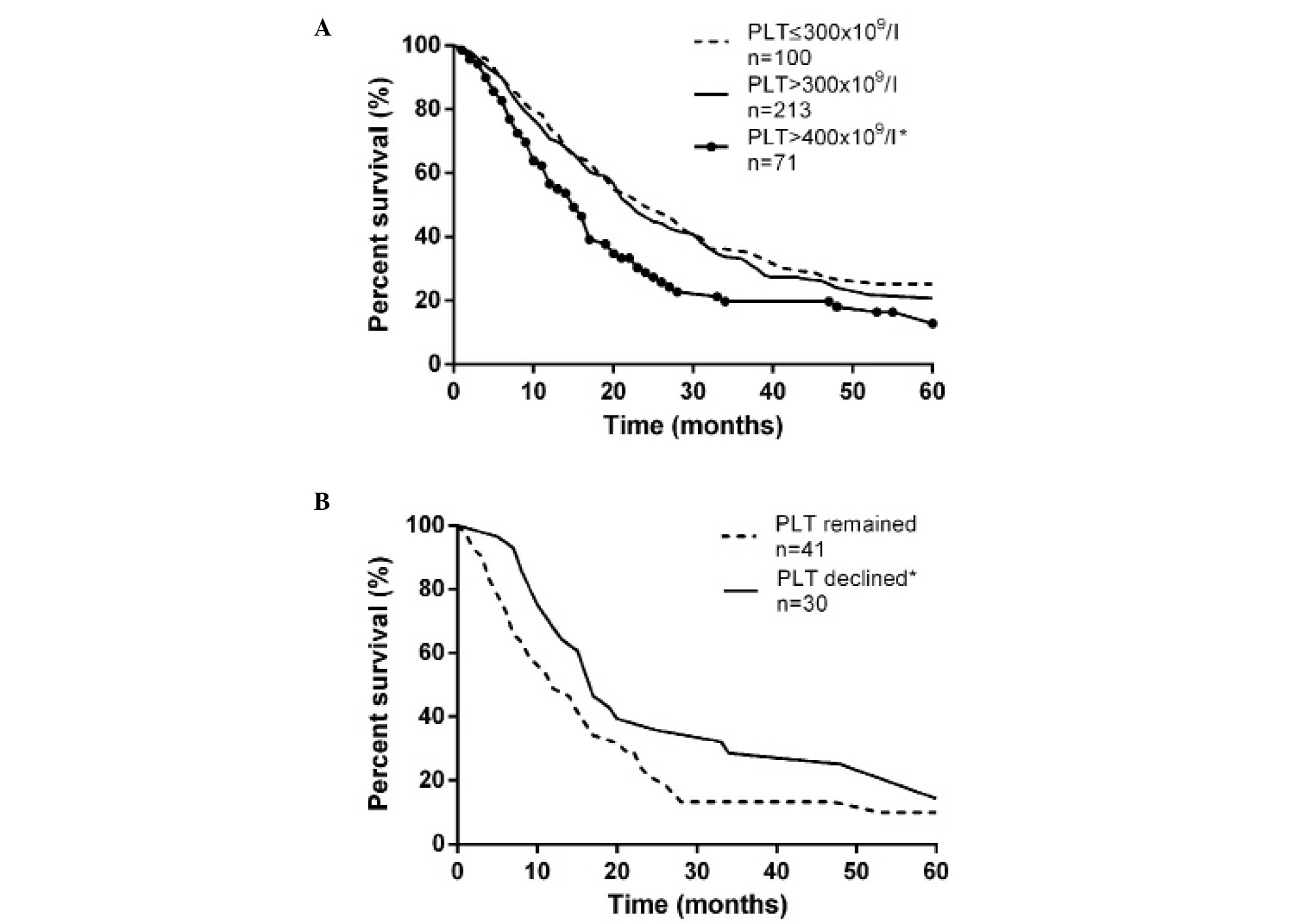
Survival analysis in GC patients with
thrombocytosis
The overall 5-year survival rate of tumor patients
with thrombocytosis (PLT >400×109/l) was 16.90%,
while the survival rate was 31.00% in individuals with a normal PLT
count. Median survival times were 15 and 24 months, respectively
(P=0.008, as determined by the logrank test; Fig. 2A). However, when compared with
control group B, individuals with a PLT count
>300×109/l exhibited no significant difference in
prognosis (P=0.227). The results demonstrated that ~42.25% (30/71)
of patients did not have thrombocytosis following resection,
however, the reason was unknown. Due to preoperative PLT counts
being maintained at a high level in the most advanced-stage
patients who were unable to undergo D2 dissection, the
postoperative PLT count was also useful for predicting prognosis
(P=0.046; Fig. 2B).
Prior to multivariate analysis, association analysis
between thrombocytosis and clinicopathological features allowed the
exclusion of age, location, type, vascular invasion and perineural
invasion. Thus, PLT counts, TNM classification, depth of
penetration, tumor size, degree of differentiation and lymphatic
invasion were evaluated using the Cox proportional hazard model. Of
the six factors, PLT count, TNM classification and lymphatic
invasion were identified as independent prognostic indicators of
survival (Table IV). Individuals
with thrombocytosis had a relative risk (RR) for mortality of 1.538
(95% CI, 1.041–2.271; P=0.031), 1.994 for TNM classification (95%
CI, 1.432–2.777; P<0.001) and 3.975 for lymphatic invasion
(95%CI, 1.565–9.203; P=0.003).
| Table IVMultivariate analysis of the
prognostic indicators. |
Table IV
Multivariate analysis of the
prognostic indicators.
| Factors | RR | 95% CI | P-value |
|---|
| PLT,
×109/l |
| ≤300 | 1.000 | | |
| >400 | 1.538 | 1.041–2.271 | 0.031 |
| TNM
classification |
| I | 1.000 | | |
| II | 1.692 | 0.544–5.267 | 0.364 |
| III | 3.339 | 0.941–11.852 | 0.062 |
| IV | 6.875 | 1.824–25.914 | 0.004 |
| Depth of
penetration |
| T1 | 1.000 | | |
| T2 | 0.664 | 0.225–1.954 | 0.457 |
| T3 | 0.856 | 0.447–1.641 | 0.640 |
| T4 | 0.927 | 0.473–1.816 | 0.825 |
| Lymphatic
invasion |
| Absent | 1.000 | | |
| Present | 3.795 | 1.565–9.203 | 0.003 |
| Tumor size, cm |
| <5 | 1.000 | | |
| ≥5 | 0.826 | 0.555–1.228 | 0.344 |
| Degree of
differentiation |
| Well | 1.000 | | |
| Moderate | 1.685 | 0.808–3.517 | 0.164 |
| Poor | 1.239 | 0.656–2.344 | 0.509 |
Thrombocytosis monitoring for the
recurrence of GC
To evaluate the role of thrombocytosis (PLT
>400×109/l) in cancer recurrence, differences were
compared between tumor patients with a normal PLT count and a group
of individuals whose PLT count decreased from
>400×109/l to normal following surgery. Sensitivities
for predicting the recurrence of malignancy in patients with normal
and decreased PLT counts were 24.1 and 70.8%, respectively. In
addition, the specificities of the two groups were 88.2 and 83.3%,
respectively. Therefore, thrombocytosis in cancer patients with a
decreased postoperative PLT count had a significant advantage for
predicting tumor recurrence with AUROC, as compared with patients
that had a normal PLT count prior to surgery (0.847 vs. 0.550;
P=0.004; Table V).
| Table VComparison of tumor recurrence among
PLT levels. |
Table V
Comparison of tumor recurrence among
PLT levels.
| | Sensitivities and
specificities for recurrence |
|---|
| |
|
|---|
| Group | PLT,
×109/l | Imaging | n | Sensitivity, % | Specificity, % | AUROC | P-value |
|---|
| Normal PLT
(n=100) | >400 | + | 20 | | | | |
| − | 2 | | | | |
| ≤400 | + | 63 | | | 0.5500 | |
| − | 15 | 24.1 | 88.2 | 95% CI,
408-0.691 | 0.521 |
| Declined PLT
(n=30) | >400 | + | 17 | | | | |
| − | 1 | | | | |
| ≤400 | + | 7 | | | 0.847a | |
| − | 5 | 70.8 | 83.3 | 95% CI,
0.707-0.988 | 0.010 |
Discussion
As a multifunctional factor, an abnormal surplus of
PLTs is associated with tumor size, TNM classification, invasive
degree, prognosis and tumor recurrence in GC, as well as D-dimer
and fibrinogen blood concentrations. The association between DVT
and thrombocytosis remains to be clarified as ultrasonic testing
was only performed on suspected patients that exhibited major
complaints. In addition, the decrease in the number of PLTs
temporarily following surgery may have been due to the surgical
patients suffering blood loss during the procedure. Furthermore,
clinical infusion during the fasting period contributed to
hemodilution.
Malignant tumors with secondary thrombocythemia have
been increasingly studied. Without a uniform standard,
thrombocytosis has been defined as a PLT count
>400×109/l in the majority of studies (5–7).
However, 220, 300, 350 and 500×109/l have also been used
as the threshold in previous studies (5,14–16).
The confusion in the definition of thrombocytosis has caused
deviation in experimental results and the reduction of lateral
comparability between studies. As demonstrated in the present
study, no statistically significant differences were identified
between the two cancer groups with PLT counts of
>300×109/l and >400×109/l with regard
to the linear correlation between the PLT and leukocyte counts or
the associated clinicopathological features. The difference in the
linear correlation between hemoglobin concentrations and PLT levels
was omitted due to the slight correlation. Survival analysis also
illustrated the advantage of using PLT >400×109/l as
the standard for predicting prognosis. Clinically, there are a
number of situations that can cause secondary thrombocytosis in
patients with malignant solid tumors, including infection, anemia,
inflammation and necrosis. Therefore, it is a reasonable hypothesis
to define thrombocytosis in GC patients as those with a PLT count
>400×109/l. This excludes clinical confounding
without causing a statistical deviation.
Although speculation remains, several hypotheses
have been proposed with regard to the mechanisms by which
thrombocytosis develops in malignancies. Released by the liver,
kidney and skeletal muscle, thrombopoietin (TPO) specifically
stimulates the proliferation and maturation of megakaryocytes, as
well as the release of PLTs. In specific cases of tumor-associated
thrombocytosis, the concentration of plasmatic TPO significantly
increased due to complex pathophysiological factors (17). In addition, activation of the TPO
receptor and the feedback regulation of TPO mRNA in the bone marrow
participate in this phenomenon (18). However, TPO is not the only factor,
as the body is able to produce a few PLTs following TPO gene
knockout and the elimination of the TPO receptor (19). Interleukin-1 and -6 are bone
marrow-stimulating cytokines that are associated with
thrombocytosis and may potentially facilitate the production of
PLTs (20,21). As previous studies have shown, the
morbidity of thrombocytosis in various malignancies is
inhomogeneous. It was found that ~42.5% of ovarian epithelial
cancer cases presented with concurrent thrombocytosis, as well as
56.8% of renal cell carcinoma cases (2, 22).
These results are much higher compared with other tumors, where the
occurrence of thrombocytosis was 4.0% in GC patients and 4.5% in
non-small-cell lung cancer patients (23). With regard to histoembryology
classification, hematopoietic cells and the urogenital system
originate from the same mesoderm, while the digestive and
respiratory system originate from the same endoderm. Thus, we
hypothesized that compared with the digestive system, the
biological function of malignant tumors derived from the urogenital
system may be more inclined to thrombocytosis.
Thrombocytosis may adversely affect survival in
malignancies by promoting neoplasm invasion, adhesion and
proliferation. Tumor cell-induced PLT aggregation may activate and
aggregate PLTs to mediate adhesion to cancer cells via
glycoproteins-Ib-IX, IIb/IIIa or adenosine diphosphate (24). PLTs efficiently shield and protect
malignant cells from the host’s immune system and provide a useful
medium for the adhesion of cancer cells to the vascular endothelium
through forming tumor thrombi and adhesion molecules, including
P-selectin and von Willebrand factor (25,26).
Following adhesion, PLTs also play a role in tumor growth by
secreting several tumor growth and angiogenic factors, including
PLT-derived growth factor, arachidonic acid and vascular
endothelial growth factor (VEGF). VEGF highly correlates with PLTs
as an angiogenic factor and was shown to adversely affect survival
in GC (27,28). Neovascularization is necessary for
the development of neoplasm, which also explains the association
between thrombocytosis and TNM classification, depth of
penetration, tumor size and prognosis. However, predicting cancer
recurrence with PLTs has been rarely reported. Although the
mechanism is unclear, the clinical data indicate the significance
of monitoring PLTs in a specific population; patients who suffered
thrombocytosis preoperatively, but recovered following surgery.
In conclusion, a PLT count of 400×109/l
is an ideal threshold value for the definition of thrombocytosis.
Although the incidence (4.0%) was lower than other types of cancer,
thrombocytosis was shown to be associated with a number of
clinicopathological features and function as an independent
prognostic indicator and cancer recurrence monitor.
Acknowledgements
The study was supported by grants from the Zhejiang
Provincial Natural Science Foundation of China (no. Y2100660) and
the Wenzhou Science and Technology Bureau (no. H20100028).
References
|
1
|
Delhommeau F, Jeziorowska D, Marzac C and
Casadevall N: Molecular aspects of myeloproliferative neoplasms.
Int J Hematol. 91:165–173. 2010. View Article : Google Scholar
|
|
2
|
Gungor T, Kanat-Pektas M, Sucak A and
Mollamahmutoglu L: The role of thrombocytosis in prognostic
evaluation of epithelial ovarian tumors. Arch Gynecol Obstet.
279:53–56. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Huang Z, Jiang C, Zhang YM and Yao B:
Analysis of hemogram, iron staining in bone marrow and iron
metabolism in 98 patients with thrombocytosis. Chinese Journal of
Clinical Laboratory Science. 26:49–51. 2008.
|
|
4
|
Tchebiner JZ, Nutman A, Boursi B, et al:
Diagnostic and prognostic value of thrombocytosis in admitted
medical patients. Am J Med Sci. 342:395–401. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Iwasaki A, Hamanaka W, Harnada T, Maekawa
S, Enatsu S and Shirakusa T: Significance of platelet counts in
patients who underwent surgical treatment for lung metastasis. Int
Surg. 92:103–109. 2007.PubMed/NCBI
|
|
6
|
Ikeda M, Furukawa H, Imamura H, et al:
Poor prognosis associated with thrombocytosis in patients with
gastric cancer. Ann Surg Oncol. 9:287–291. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Maráz A, Furák J, Varga Z, Kahán Z,
Tiszlavicz L and Hideghéty K: Thrombocytosis has a negative
prognostic value in lung cancer. Anticancer Res. 33:1725–1729.
2013.PubMed/NCBI
|
|
8
|
Gouin-Thibault I, Achkar A and Samama MM:
The thrombophilic state in cancer patients. Acta Haematol.
106:33–42. 2001. View Article : Google Scholar
|
|
9
|
Riess L: Pathology of the blood. Arch Anat
Physiol Wissensch Med. 39:237–249. 1872.(In German).
|
|
10
|
Ferrigno D and Buccheri G: Hematologic
counts and clinical correlates in 1201 newly diagnosed lung cancer
patients. Monaldi Arch Chest Dis. 59:193–198. 2003.PubMed/NCBI
|
|
11
|
Qiu MZ, Xu RH, Ruan DY, et al: Incidence
of anemia, leukocytosis, and thrombocytosis in patients with solid
tumors in China. Tumour Biol. 31:633–641. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Aminian A, Karimian F, Mirsharifi R, et
al: Significance of platelet count in esophageal carcinomas. Saudi
J Gastroenterol. 17:134–137. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Aoe K, Hiraki A, Ueoka H, et al:
Thrombocytosis as a useful prognostic indicator in patients with
lung cancer. Respiration. 71:170–173. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Brockmann MA, Giese A, Mueller K, et al:
Preoperative thrombocytosis predicts poor survival in patients with
glioblastoma. Neuro Oncol. 9:335–342. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Nather A, Mayerhofer K, Grimm C, et al:
Thrombocytosis and anaemia in women with recurrent ovarian cancer
prior to a second-line chemotherapy. Anticancer Res. 23:2991–2994.
2003.PubMed/NCBI
|
|
16
|
Zwitter M, Kovac V, Smrdel U, Kocijancic
I, Segedin B and Vrankar M: Phase I-II trial of low-dose
gemcitabine in prolonged infusion and cisplatin for advanced
non-small cell lung cancer. Anticancer Drugs. 16:1129–1134. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Cerutti A, Custodi P, Duranti M, Noris P
and Balduini CL: Thrombopoietin levels in patients with primary and
reactive thrombocytosis. Br J Haematol. 99:281–284. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Soonthornthum T, Suraseraneewong V,
Kengsakol K, Wijaithum K, Kasemsan P and Prommatt S: Thrombocytosis
in advanced epithelial ovarian cancer. J Med Assoc Thai.
90:1495–1500. 2007.PubMed/NCBI
|
|
19
|
de Sauvage FJ, Carver-Moore K, Luoh SM, et
al: Physiological regulation of early and late stages of
megakaryocytopoiesis by thrombopoietin. J Exp Med. 183:651–656.
1996.PubMed/NCBI
|
|
20
|
Lidor YJ, Xu FJ, Martínez-Maza O, et al:
Constitutive production of macrophage colony-stimulating factor and
interleukin-6 by human ovarian surface epithelial cells. Exp Cell
Res. 207:332–339. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ceresa IF, Noris P, Ambaglio C, Pecci A
and Balduini CL: Thrombopoietin is not uniquely responsible for
thrombocytosis in inflammatory disorders. Platelets. 18:579–582.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Symbas NP, Townsend MF, El-Galley R, Keane
TE, Graham SD and Petros JA: Poor prognosis associated with
thrombocytosis in patients with renal cell carcinoma. BJU Int.
86:203–207. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Tomita M, Shimizu T, Ayabe T and Onitsuka
T: Prognostic significance of the combined use of preoperative
platelet count and serum carcinoembryonic antigen level in
non-small-cell lung cancer. Gen Thorac Cardiovasc Surg. 58:573–576.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lian L, Li W, Li ZY, et al: Inhibition of
MCF-7 breast cancer cell-induced platelet aggregation using a
combination of antiplatelet drugs. Oncol Lett. 5:675–680.
2013.PubMed/NCBI
|
|
25
|
Palumbo JS, Talmage KE, Massari JV, et al:
Platelets and fibrin(ogen) increase metastatic potential by
impeding natural killer cell-mediated elimination of tumor cells.
Blood. 105:178–185. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
McCarty OJ, Mousa SA, Bray PF and
Konstantopoulos K: Immobilized platelets support human colon
carcinoma cell tethering, rolling, and firm adhesion under dynamic
flow conditions. Blood. 96:1789–1797. 2000.PubMed/NCBI
|
|
27
|
Bachelot T, Ray-Coquard I, Menetrier-Caux
C, Rastkha M, Duc A and Blay JY: Prognostic value of serum levels
of interleukin 6 and of serum and plasma levels of vascular
endothelial growth factor in hormone-refractory metastatic breast
cancer patients. Br J Cancer. 88:1721–1726. 2003. View Article : Google Scholar
|
|
28
|
Wang X, Chen X, Fang J and Yang C:
Overexpression of both VEGF-A and VEGF-C in gastric cancer
correlates with prognosis, and silencing of both is effective to
inhibit cancer growth. Int J Clin Exp Pathol. 6:586–597.
2013.PubMed/NCBI
|