Introduction
Paraquat (N,N′-dimethyl-4,4′-bipyridinium
dichloride; PQ), an effective herbicide that has favorable
environmental characteristics, as well as being cost-effective, was
first synthesized in 1882 and has been used as an herbicide since
1955 (1). PQ is an important
herbicide used in agriculture; however, thousands of individuals
succumb due to PQ intoxication every year in the developing world.
PQ is a highly toxic compound and the fatality rate of PQ ranges
between 60 and 80% (2) due to the
lack of a specific antidote. A PQ dose of 30 mg/kg may be fatal,
which is equivalent to 8–10 ml of the 20% solution sold
commercially (3). PQ has been
shown to cause significant damage to organs, including the lung,
liver, kidneys and myocardium, with the highest concentration of PQ
found in the lungs (4). The
prognosis of patients with multiple organ dysfunction syndrome
(MODS) caused by fulminant poisoning (>40 mg PQ ion per kg of
body weight) is extremely dangerous and patients may succumb within
hours to a few days following ingestion (5,6).
China is an agricultural country and PQ is used
extensively. Since the first reported case of PQ poisoning, studies
have focused on the mechanism and effects of combination therapies
and various agents (7,8). Furthermore, strategies for the
management of PQ poisoning have focused on the modification of the
toxicokinetics of the poison by either decreasing its absorption or
enhancing its elimination (9);
however, studies on comprehensive strategies are rare. We
previously identified a comprehensive treatment strategy against PQ
poisoning, termed the Qilu scheme (10). In the present study, a case of MODS
caused by severe PQ poisoning was treated using multi-target
comprehensive therapy. Furthermore, the present study indicates the
potential and feasibility of the therapy for the treatment of PQ
poisoning. Informed consent was obtained from the patient. The
study was approved by the ethics committee of the Qilu Hospital,
Shandong University (Jinan, China).
Case report
A 42-year-old female, weighing ~60 kg, ingested
>100 ml PQ (20% weight/volume) in an attempted suicide at 12:50
p.m. on September 13, 2012. The patient experienced nausea,
vomiting and discomfort immediately following PQ ingestion and was
sent to a county hospital 20 min later. A gastric lavage was
immediately performed and kaolin (30 g) and mannitol infusion (250
ml) was administered within 1 h following ingestion. Hemoperfusion
therapy was prescribed for 2 h. The dose for methylprednisolone was
1,000 mg/day for the first day. Due to the severity of the
condition, relatives brought the patient to the Department of
Poisoning and Occupational Diseases, Qilu Hospital of Shandong
University at 10:55 a.m. on December 14, 2012. On admission, the
patient’s vital signs were normal, with a body temperature 36.6°C,
pulse 89 beats/min, respiratory rate 19 breaths/min, blood pressure
125/80 mmHg and blood oxygen saturation 98%. Physical examination
was normal, with the exception of painful erosions in the oral
cavity. Based on the typical poison-associated symptoms in the
mouth and the gastrointestinal tract, computed tomography (CT)
manifestations, significantly abnormal results in the main
laboratory test results and the information provided by the patient
and her relatives on admission, the patient was diagnosed with
severe acute PQ poisoning.
Following admission to Qilu Hospital, the patient
was subjected to complete gastrointestinal decontamination using
activated carbon, Smecta and mannitol in order to thoroughly remove
the pesticide residue from the gastrointestinal tract. Furthermore,
other treatments such as an intravenous drip of high doses of
glucocorticoids, anticoagulants, anti-free radical, liver- and
kidney-protecting and water and electrolyte balance-maintaining
agents, and treatment with Chinese herbs (including Xuebijing,
Cordyceps and depside salt from Salvia miltiorrhiza)
were administered to the patient. This was termed the Qilu
therapeutic schedule. The dose for glucocorticoids was 800 mg/day
for the first 4 days and then reduced to 40–80 mg/day. The
patient’s condition was markedly improved following the
comprehensive therapy. Low doses of prednisone were maintained
after 3–6 weeks. After 2 months the patient stopped taking
glucocorticoids; however, the pulmonary damage became aggravated
and recovered again subsequent to treatment with glucocorticoid and
traditional Chinese medicines.
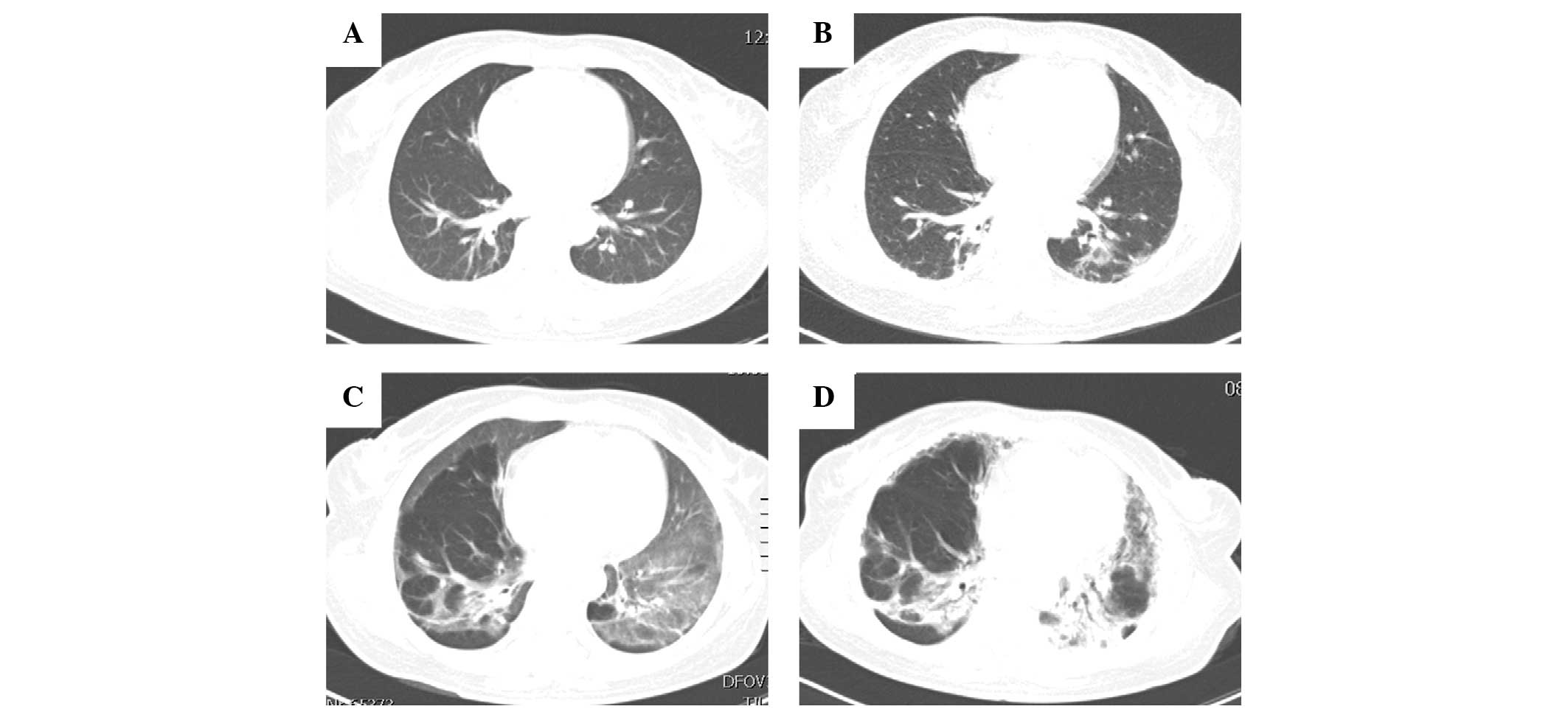
Following multi-target comprehensive therapy, the
dynamic changes in the lung CT scans are shown in Fig. 1 and 2, and the main laboratory test results
are shown in Table I. The liver
and kidney functions were seriously damaged 2 days following
ingestion and the most serious damage was observed 6 days
subsequent to PQ poisoning. However, the liver and kidney functions
gradually recovered 2 weeks later (Table I). The initial CT scan showed that
there was a certain degree of lung injury that occurred after 2
days (Fig. 1A) and gradually
accelerated over the following 3 days (Fig. 1B). Serious lung injury occurred 15
days later (Fig. 1C); however, it
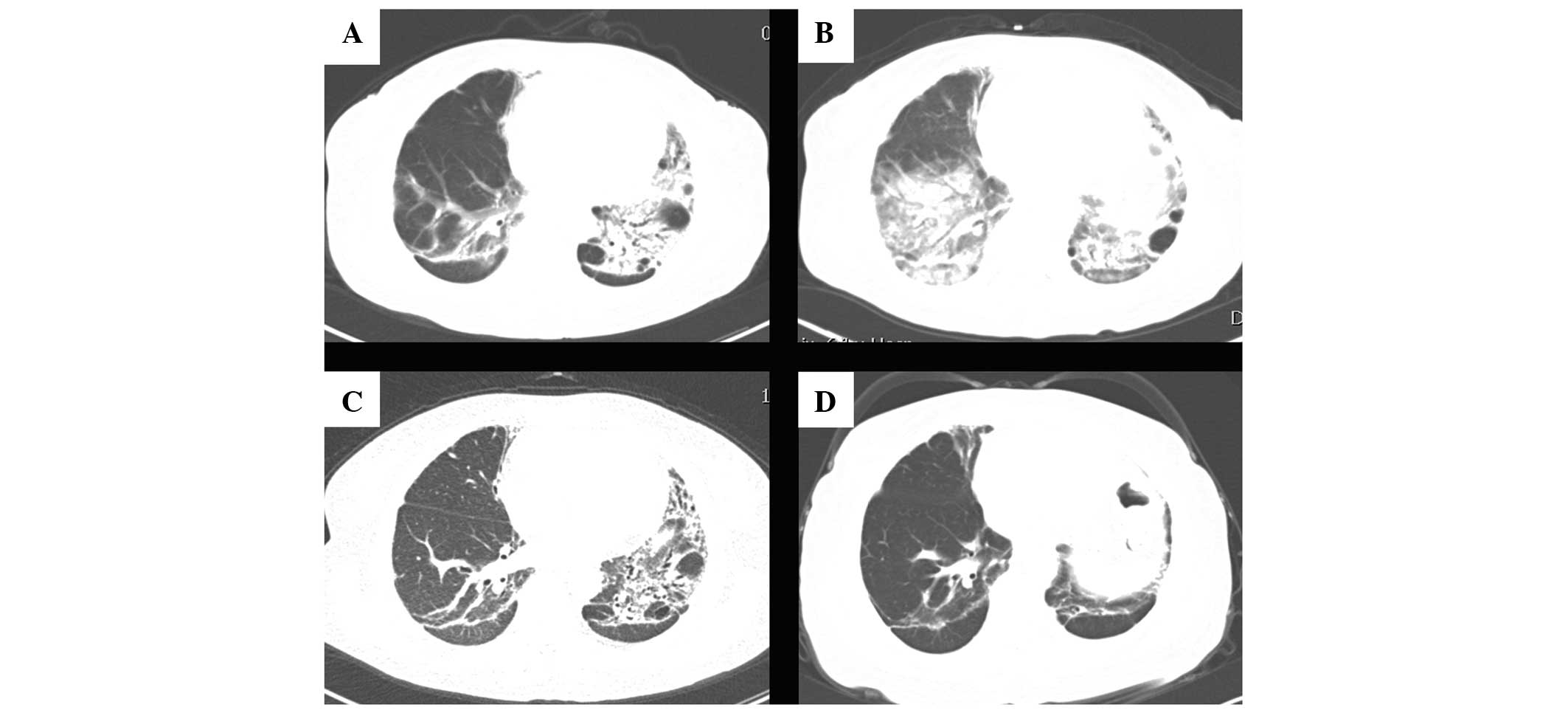
improved gradually during the 6 weeks of treatment (Fig. 1D and Fig. 2A). Treatment was ceased gradually;
however, after 2 months the lung injury re-occurred (Fig. 2B) accompanied by marked liver
dysfunction. Treatment was then resumed and lung function improved
again (Fig. 2C), and the liver
function gradually returned to normal. Eight months following
ingestion, the patient’s lung function was markedly improved
(Fig. 2D). The pulmonary function
test indicated moderate restrictive ventilation dysfunction and a
mild decline of diffuse lung function with the forced vital
capacity, maximum vital capacity, maximum ventilatory volume and
carbon monoxide diffusion capacity accounting for 53.2, 52.1, 67.3
and 54.1% of the expected values, respectively. The patient
continues to be followed up.
 | Table IChanges in the main indicators of
blood, urine, liver and kidney function test results for the
patient 2, 6, 14, 43, 71, 127 and 221 days following ingestion. |
Table I
Changes in the main indicators of
blood, urine, liver and kidney function test results for the
patient 2, 6, 14, 43, 71, 127 and 221 days following ingestion.
| Date | ALT* (U/l) | AST* (U/l) | GGT* (U/l) | Cr (μmol/l) | BUN (mmol/l) | CK-MB* (ng/ml) | CK* (U/l) | DDi* (μg/ml) | WBC
(109/l) | HGB (g/l) | PLT
(109/l) | ESR (mm/h) | PRO |
|---|
| Day 2 | 219 | 212 | 108 | 241 | 13.3 | 4.2 | 410 | 0.79 | 21.05 | 140 | 115 | 16 | 1+ |
| Day 6 | 815 | 304 | 797 | 274 | 23.9 | 2.2 | 117 | 0.85 | 12.79 | 132 | 162 | 44 | 1+ |
| Day 14 | 53 | 39 | 316 | 53 | 5.4 | 5.2 | 75 | 0.70 | 20.76 | 115 | 369 | 69 | 1+ |
| Day 43 | 171 | 82 | 610 | 41 | 5.7 | 2.5 | 29 | 0.16 | 9.08 | 118 | 199 | 40 | − |
| Day 71 | 27 | 24 | 156 | 40 | 1.8 | 1.5 | 28 | 0.64 | 5.95 | 135 | 220 | 27 | +− |
| Day 127 | 29 | 20 | 58 | 57 | 4.4 | 2.0 | 31 | 0.54 | 11.39 | 128 | 236 | 13 | − |
| Day 221 | 23 | 22 | 49 | 60 | 2.6 | 0.8 | 64 | 0.30 | 5.74 | 125 | 207 | 2 | − |
Discussion
PQ is a non-selective herbicide that has been widely
used in agriculture since the 1960s (11). Although it has been found to be
safe for occupational use, PQ poisoning has been observed in
patients who ingest the pesticide either accidentally or
intentionally in an attempt to commit suicide. PQ is banned or
rarely used in the developed world; however, in developing
countries PQ continues to be used and PQ poisoning remains a major
cause of mortality among patients with acute poisoning (12). During acute PQ poisoning, the
pulmonary concentrations of PQ may be higher than the plasma
concentration (13). Therefore,
the primary cause of mortality in PQ poisoning is respiratory
failure due to oxidative damage to the alveolar epithelium with
subsequent obliterating fibrosis (14). In addition to lung damage, PQ
ingestion has been shown to injure other organs, but to a lesser
extent. Severe PQ poisoning is characterized by multi-organ
involvement, primarily affecting the lungs, kidneys, liver,
myocardium and adrenal cortex (15). Therefore, urgent gastric lavage is
required to reduce the absorption of PQ. Extracorporeal
elimination, for example hemoperfusion (HP), is an effective
measure that has previously been used clinically (11). The majority of studies have focused
on the association between HP and the overall prognosis of PQ
poisoning. However, the results from these studies are discouraging
and controversial opinions have arisen on the therapeutic effects
of HP in PQ intoxication treatment (16,17).
The prognosis for patients with severe PQ poisoning, complicated
with multiple organ damage, is extremely poor. Despite numerous
studies into the mechanism of toxicity and the potential
therapeutic treatments for PQ poisoning, at present no specific
therapy has been shown to affect the outcome in controlled clinical
studies (12).
In the present case study, a patient with PQ
poisoning complicated with MODS was successfully treated using
multi-target comprehensive therapy. The patient ingested a high
dose of PQ, resulting in severe liver and kidney damage.
Gastrointestinal procedures were performed to prevent further
absorption of PQ residue, accompanied by glucocorticoid treatment
to reduce cell absorption, promote the elimination of PQ and
control lung inflammation lesions. The mechanism of PQ toxicity has
been previously investigated by Dinis-Oliveira et al
(18). In the present study,
anticoagulant and antioxidant treatments, as well as Chinese
medicine, were administered to the patient to prevent oxidative
damage and to protect other organs against injury. Pulmonary
lesions gradually developed into pulmonary fibrosis; therefore, the
patient was given the immunosuppressant cyclophosphamide. The
patient’s condition was aggravated following the cessation of the
treatment. The lung injury was improved once treatment with
glucocorticoids was resumed, indicating that glucocorticoids may
have an important role in the treatment of pulmonary fibrosis
caused by PQ poisoning. The patient was cured and discharged from
hospital. However, further studies are required to determine an
effective treatment against PQ poisoning.
Acknowledgements
This study was supported by the Natural Science
Foundation of Shandong Province (no. Y2008C123).
References
|
1
|
Yang CJ, Lin JL, Lin-Tan DT, Weng CH, et
al: Spectrum of toxic hepatitis following intentional paraquat
ingestion: analysis of 187 cases. Liver Int. 32:1400–1406. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Weng CH, Hu CC, Lin JL, Lin-Tan DT, et al:
Sequential organ failure assessment score can predict mortality in
patients with paraquat intoxication. PLoS One. 7:e517432012.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Yoon SC: Clinical outcome of paraquat
poisoning. Korean J Intern Med. 24:93–94. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yen TH, Lin JL, Lin-Tan DT, Hsu CW, et al:
Spectrum of corrosive esophageal injury after intentional paraquat
ingestion. Am J Emerg Med. 28:728–733. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Agarwal R, Srinivas R, Aggarwal AN and
Gupta D: Immunosuppressive therapy in lung injury due to paraquat
poisoning: a meta-analysis. Singapore Med J. 48:1000–1005.
2007.PubMed/NCBI
|
|
6
|
Sabzghabaee AM, Eizadi-Mood N, Montazeri
K, Yaraghi A and Golabi M: Fatality in paraquat poisoning.
Singapore Med J. 51:496–500. 2010.PubMed/NCBI
|
|
7
|
Lin JL, Lin-Tan DT, Chen KH, Huang WH, et
al: Improved survival in severe paraquat poisoning with repeated
pulse therapy of cyclophosphamide and steroids. Intensive Care Med.
37:1006–1013. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sun ML, Ma DH, Liu M and Yu YX: Successful
treatment of paraquat poisoning by Xuebijing, an injection
concocted from multiple Chinese medicinal herbs: a case report. J
Altern Complement Med. 15:1375–1378. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Dinis-Oliveira RJ, Sarmento A, Reis P,
Amaro A, et al: Acute paraquat poisoning: report of a survival case
following intake of a potential lethal dose. Pediatr Emerg Care.
22:537–540. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Jian X, Zhang H, Sui H, Guo G, et al: Qilu
Scheme of paraquat poisoning treatment (2014). Chinese Journal of
Industrial Medicine (Chinese). 27:119–121. 2014.(In Chinese).
|
|
11
|
Zhang Z, Jian X, Zhang W, Wang J and Zhou
Q: Using bosentan to treat paraquat poisoning-induced acute lung
injury in rats. PLoS One. 8:e759432013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wilks MF, Fernando R, Ariyananda PL,
Eddleston M, et al: Improvement in survival after paraquat
ingestion following introduction of a new formulation in Sri Lanka.
PLoS Med. 5:e492008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rose MS, Smith LL and Wyatt I: Evidence
for energy-dependent accumulation of paraquat into rat lung.
Nature. 252:314–315. 1974. View
Article : Google Scholar : PubMed/NCBI
|
|
14
|
Suntres ZE: Role of antioxidants in
paraquat toxicity. Toxicology. 180:65–77. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yeo CD, Kim JW, Kim YO, Yoon SA, et al:
The role of pentraxin-3 as a prognostic biomarker in paraquat
poisoning. Toxicol Lett. 212:157–160. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Castro R, Prata C, Oliveira L, Carvalho
MJ, et al: Paraquat intoxication and hemocarboperfusion. Acta Med
Port. 18:423–431. 2005.(In Portuguese).
|
|
17
|
Hampson EC and Pond SM: Failure of
haemoperfusion and haemodialysis to prevent death in paraquat
poisoning. Med Toxicol Adverse Drug Exp. 3:64–71. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Dinis-Oliveira RJ, Duarte JA,
Sánchez-Navarro A, Remião F, et al: Paraquat poisonings: mechanisms
of lung toxicity, clinical features, and treatment. Crit Rev
Toxicol. 38:13–71. 2008. View Article : Google Scholar : PubMed/NCBI
|