Introduction
Synovitis, acne, pustulosis, hyperostosis and
osteitis (SAPHO), is a rare syndrome that is mainly reported in the
West and Japan (1), with few cases
reported in China. Genetic susceptibility and infection with
Propionibacterium acnes are the main pathogenic hypotheses
for the syndrome. Apart from these, proinflammatory cytokines,
including tumor necrosis factor α, are also suspected to be
involved in SAPHO syndrome (1).
SAPHO syndrome is relatively benign and symptomatic treatment is
currently an effective management strategy. Early recognition and
treatment is likely to improve the health and quality of life of
patients with SAPHO. In the present case study, the diagnosis and
management of a Chinese patient with SAPHO syndrome is
described.
Case report
A 42-year-old Chinese male presented with bilateral
psoriasis on the palms for two months without any clear
predisposing cause. The patient later developed skin problems
bilaterally on the ankles and interdigital surfaces of the feet.
Following consultation with doctors in a local hospital, the
patient was prescribed treatment for erythra; however, this did not
lead to much improvement. The patient complained of chest pain and
lumbago for three weeks, and experienced episodes of limited
mobility in the mornings for ~15 min each time. Physical
examination on admission revealed bilateral psoriasis on the palms
and interdigital surfaces of the feet, and pustules on the inner
surfaces of the ankles (Fig. 1).
There was also redness, swelling and tenderness in the left
sternoclavicular joint area and tenderness in the lower back. The
straight-leg raise test for the left leg was positive.
Blood tests revealed an elevation of the erythrocyte
sedimentation rate (49 mm/h, normal range 0–15 mm/h), levels of
C-reactive protein (4.04 mg/dl, normal range <0.80 mg/dl) and
D-dimer (1,080 ng/ml, normal range 0–500 ng/ml). Routine blood
examinations also demonstrated slight increases in the number of
leukocytes (10.14×109/l, normal range
4.00–10.00×109/l), neutrophilic leukocytes
(7.09×109/l, normal range 2.00–7.00×109/l)
and platelets (394×109/l, normal range
100–300×109/l). The rheumatoid factor and human
leukocyte antigen B27 tests were negative. The results for all
other laboratory tests that were carried out were within normal
range.
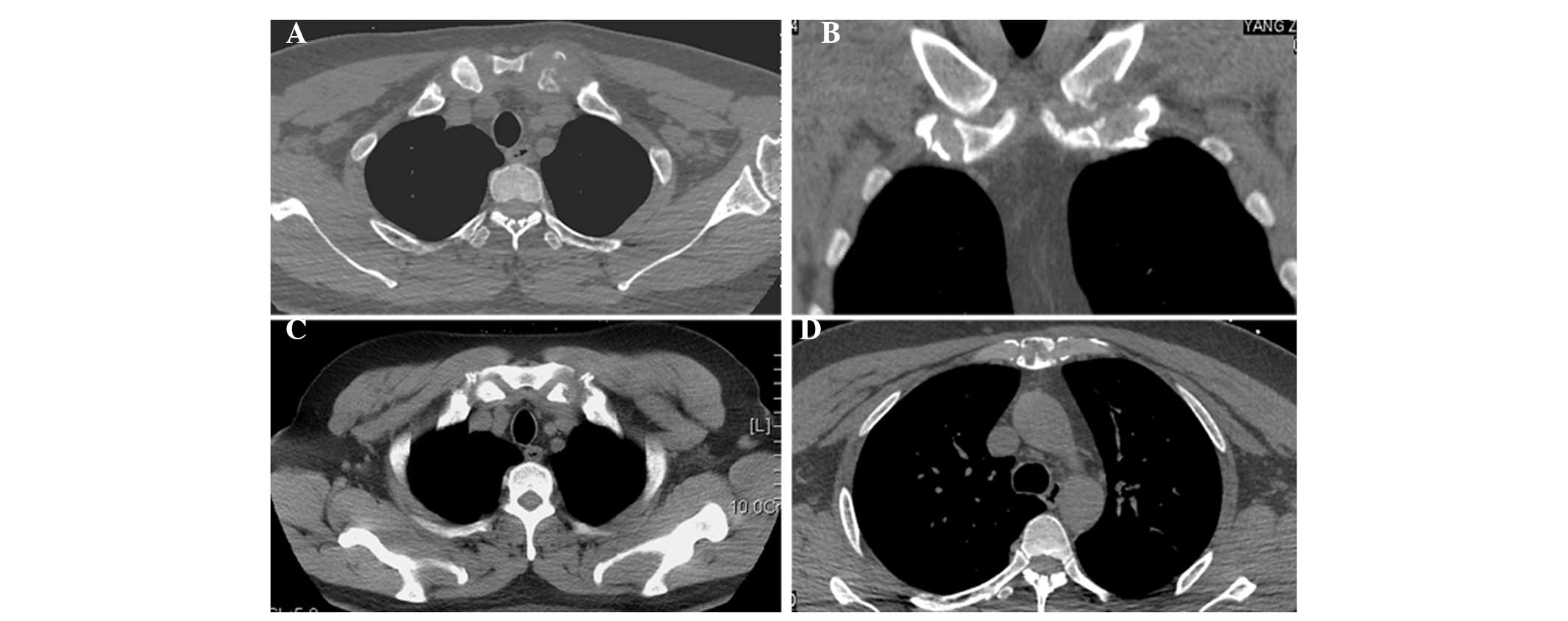
Computerized tomography (CT) scans of the sternum,
sternoclavicular joints and sacroiliac joints revealed osseous
erosions on the left sternoclavicular joint area, manubrium
(Fig. 2) and bilateral sacroiliac
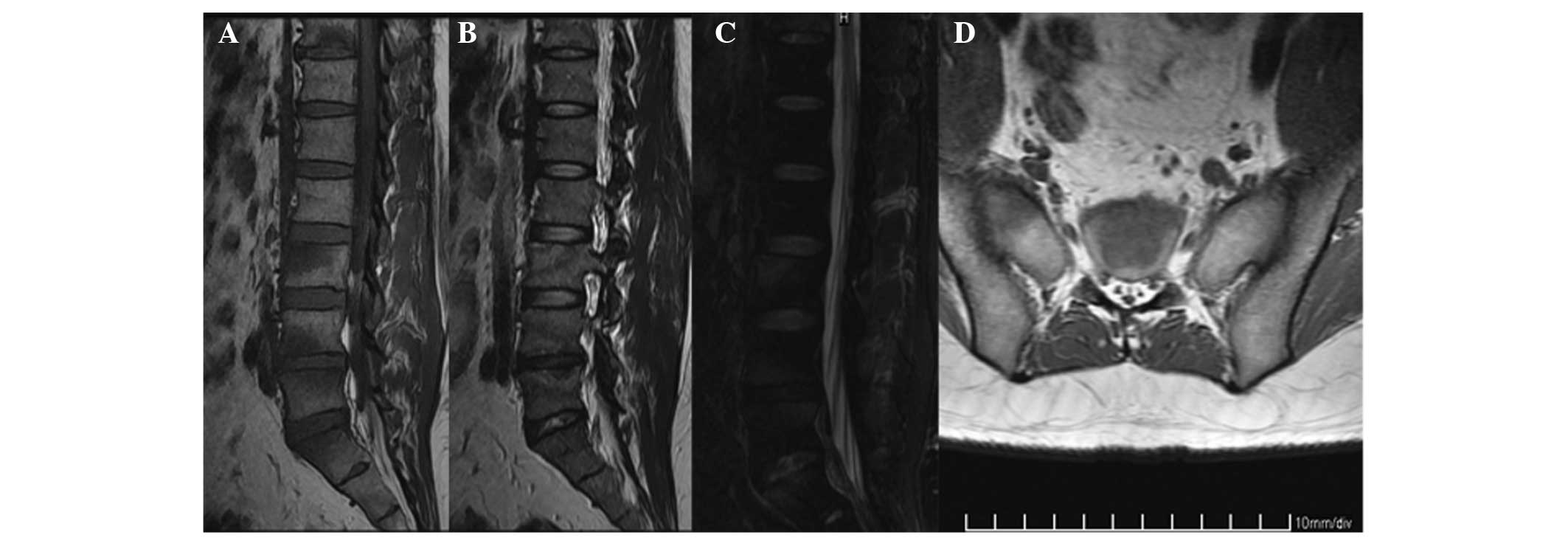
joints. Magnetic resonance imaging (MRI) scans of the lumbar spine
and sacroiliac joints demonstrated bone marrow edema at the levels
of the T11, L3–L5 and S1 vertebra and the bilateral ala of sacrum
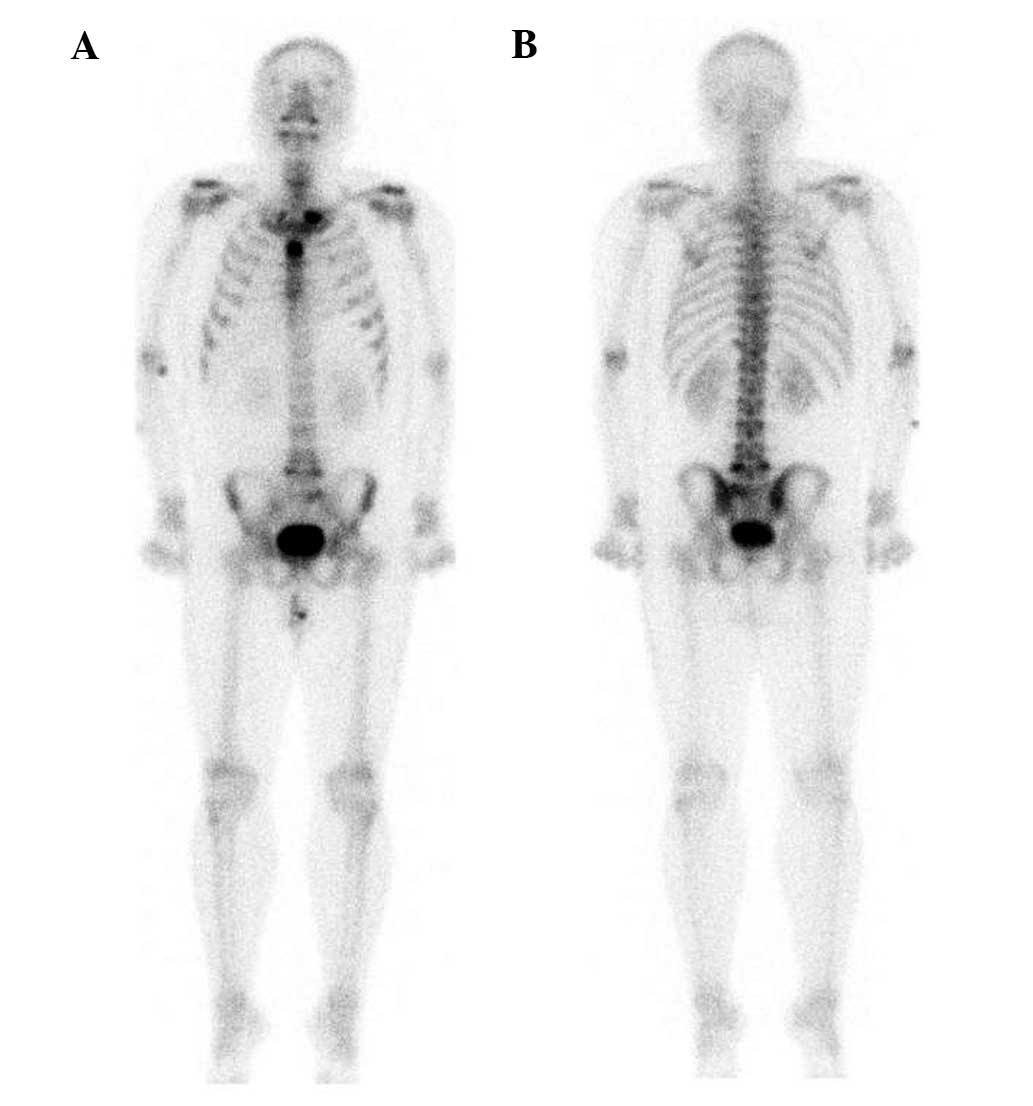
(Fig. 3). To evaluate the
skeleton, a whole body bone scan (WBS) was performed 3 h following
the injection of 25 mCi 99mTc-methylene-diphosphonate.
Anterior and posterior views of the WBS revealed intense uptake at
the proximal end of the left clavicle, manubrium sterni, fifth
lumbar vertebra and right sacroiliac joint (Fig. 4).
A diagnosis of SAPHO syndrome was made according to
the clinical manifestations (skin lesions and osteoarticular
involvement), the results of the CT, MRI and WBS scans, and the
analyses of the laboratory tests. Non-steroidal anti-inflammatory
drugs (NSAIDs), alendronate sodium, leflunomide and steroids were
administered, resulting in a notable remission of the clinical
symptoms and the normalization of serum indices.
A written informed consent was obtained from the
patient prior to publication.
Discussion
The term SAPHO syndrome was first proposed by Chamot
et al in 1987 (2), to
describe a group of conditions that had similar osteoarticular
involvement (osteitis mainly affecting the anterior chest wall) and
that were frequently associated with different forms of
dermatological manifestations. Studies have shown that from its
onset, SAPHO syndrome is associated with an elevated erythrocyte
sedimentation rate and increased C-reactive protein values
(3–5). The etiopathogenetic mechanism of
SAPHO syndrome remains unclear, although several hypotheses have
been proposed involving bacteriologic, immunologic and genetic
factors. By combining bacteriologic, immunologic and genetic data,
Hayem (1) considers SAPHO syndrome
as a ‘reactive osteitis’, namely a pathogenic sequence in which the
opportunistic organism (Propionibacterium acnes) takes
advantage of genetically determined deficiencies in antibacterial
defense mechanisms and subsequently induces auto-amplification of
the inflammatory response, possibly with an autoimmune
component.
The diagnosis of SAPHO syndrome is based on history,
characteristic scintigraphic and radiological results, and skin
manifestations. Any one of the following criteria is regarded as
sufficient to diagnose SAPHO syndrome: i) multifocal osteitis with
or without skin lesions; ii) sterile acute, subacute or chronic
arthritis associated with pustular psoriasis, palmoplantar
pustulosis, acne or hidradenitis suppurativa; and iii) sterile
osteitis combined with one of the skin manifestations (6). However, the dermatological and
skeletal conditions do not always occur in parallel, and they may
be separated by a number of years. Thus, diagnosing SAPHO syndrome
is difficult in certain cases, particularly if the dermatological
manifestations are absent (7).
WBSs using 99mTc-methylene-diphosphonate
are important for the diagnosis of SAPHO syndrome, particularly for
detecting multiple and early bone involvement. Bone scintigraphy is
a sensitive imaging modality that is able to identify uptake in
characteristic regions when changes in radiography are absent or
subtly abnormal (6). The
sternoclavicular junction is the most common site of involvement in
adults, followed by the spine and sacroiliac joints (7). In the present case study, all the
common sites were involved to a certain extent. The radiological
results of SAPHO syndrome consist of osteolysis, osteitis,
hyperostosis and osteosclerosis (8) Osteolysis is occasionally observed,
particularly in the initial stages of the disease (7,9), as
is the case in the current study. CT scans provide a detailed
depiction of the osteoarticular lesions and are the primary imaging
modality of the chest wall, particularly for the sternoclavicular
region. MRI scans are recommended in cases of spondylodiscitis in
SAPHO syndrome in order to provide a better understanding of the
extent of the inflammatory process. This is due to the fact that
chronic sclerotic bone lesions exhibit low signal intensity in T1-
and T2-weighted images, whereas active lesions appear hypointense
on T1- and hyperintense on T2-weighted images (8). MRI results reveal SAPHO vertebral
lesions, including body corner erosions, signal abnormalities in
the contiguous vertebrae and the narrowing of disk spaces (10).
Until now, there have been no treatment guidelines
for SAPHO syndrome. Current treatment of this illness is multimodal
and empirical, and is mainly focused on relieving symptoms. NSAIDs,
with or without antibiotics, are the primary treatment (11). Several studies have supported the
effectiveness of bisphosphonates as a treatment for SAPHO syndrome
as they exhibit a good cutaneous and articular response. These
drugs not only take part in bone remodeling but also have
anti-inflammatory properties that inhibit cytokine secretion by
macrophages (12–14). In the present case study, NSAIDs,
oral bisphosphonates, leflunomide and steroids were prescribed
simultaneously. According to the results observed in the patient,
this combination proved to be effective for the treatment of SAPHO
syndrome, and terminated its rapid onset.
The current study described a rare case of SAPHO
syndrome with skin problems, musculoskeletal involvement of the
anterior thoracic wall, lumbar vertebra and sacroiliac joint
erosion. The present case highlights the importance of using
multiple imaging modalities to produce a definite diagnosis of
SAPHO and indicates that early treatment of SAPHO is vital for a
positive outcome.
References
|
1
|
Hayem G: Valuable lessons from SAPHO
syndrome. Joint Bone Spine. 74:123–126. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chamot AM, Benhamou CL, Kahn MF, et al:
Acne-pustulosis-hyperostosis-osteitis syndrome. Results of a
national survey. 85 cases. Rev Rhum Mal Osteoartic. 54:187–196.
1987.(In French).
|
|
3
|
Colina M, Govoni M, Orzincolo C and Trotta
F: Clinical and radiologic evolution of synovitis, acne,
pustulosis, hyperostosis, and osteitis syndrome: a single center
study of a cohort of 71 subjects. Arthritis Rheum. 61:813–821.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Rosero A, Ruano R, Martin M, Hidalgo C and
Garcia-Talavera J: Acute venous thrombosis as complication and clue
to diagnose a SAPHO syndrome case. A case report. Acta Reumatol
Port. 38:203–206. 2013.PubMed/NCBI
|
|
5
|
Hayem G, Bouchaud-Chabot A, Benali K, Roux
S, Palazzo E, Silbermann-Hoffman O, Kahn MF and Meyer O: SAPHO
syndrome: A long-term follow-up study of 120 cases. Semin Arthritis
Rheum. 29:159–171. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kahn MF and Khan MA: The SAPHO syndrome.
Baillieres Clin Rheumatol. 8:333–362. 1994. View Article : Google Scholar
|
|
7
|
Nguyen MT, Borchers A, Selmi C, et al: The
SAPHO syndrome. Semin Arthritis Rheum. 42:254–265. 2012. View Article : Google Scholar
|
|
8
|
Matzaroglou Ch, Velissaris D, Karageorgos
A, et al: SAPHO syndrome diagnosis and treatment: report of five
cases and review of the literature. Open Orthop J. 3:100–106. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cotten A, Flipo RM, Mentre A, et al: SAPHO
syndrome. Radiographics. 15:1147–1154. 1995. View Article : Google Scholar
|
|
10
|
Laredo JD, Vuillemin-Bodaghi V, Boutry N,
Cotten A and Parlier-Cuau C: SAPHO syndrome: MR appearance of
vertebral involvement. Radiology. 242:825–831. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Olivieri I, Padula A and Palazzi C:
Pharmacological management of SAPHO syndrome. Expert Opin Investig
Drugs. 15:1229–1233. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Pennanen N, Lapinjoki S, Urtti A and
Mönkkönen J: Effect of liposomal and free bisphosphonates on the
IL-1 beta, IL-6 and TNF alpha secretion from RAW 264 cells in
vitro. Pharm Res. 12:916–922. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kopterides P, Pikazis D and Koufos C:
Successful treatment of SAPHO syndrome with zoledronic acid.
Arthritis Rheum. 50:2970–2973. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Amital H, Applbaum YH, Aamar S, Daniel N
and Rubinow A: SAPHO syndrome treated with pamidronate: an
open-label study of 10 patients. Rheumatology. 43:658–661. 2004.
View Article : Google Scholar : PubMed/NCBI
|