Introduction
Acute pancreatitis (AP) is an inflammatory disorder
in which a complex cascade of immunological events develops, which
affects the pathogenesis and clinical course of the disease,
varying from a mild, self-limiting, transient illness to a severe,
fatal outcome (1). Severe AP is
characterized by pancreatic tissue necrosis, as well as
complications including systemic inflammatory response syndrome and
multiple organ dysfunction syndrome. Of the total number of patient
mortalities due to severe AP, >50% are ascribed to acute lung
injury in the early stage (2),
also known as pancreatitis-associated lung injury (PALI).
Previous studies have demonstrated that pulmonary
edema following PALI causes pulmonary swelling, which consequently
produces secondary microvascular leakage, alveolar-capillary
barrier disruption, and even alveolar damage and mortality
(3–5). In severe PALI, pulmonary edema poses
a critical clinical problem due to its association with acute
respiratory function failure (6).
Despite the fact that there have been significant advances in the
understanding of the pathogenesis of alveolar-capillary barrier
disruption and lung edema of PALI, as well as the availability of
existing PALI treatments that attenuate the aforementioned
derangements, the molecular mechanisms underlying this phenomenon
remain poorly understood. The lack of effective drugs to ameliorate
the initiation and progression of PALI-induced alveolar-capillary
barrier disruption and lung edema has led to increased interest in
the role that anti-edematous molecules may serve in alleviating
this phenomenon (4,6–8).
Matrix metalloproteinases (MMPs) have an important
function in the pathophysiology of alveolar-capillary barrier
disruption and lung edema following PALI, and have become viable
candidates for potential pharmacological targets (4,8,9). The
expression of MMPs is crucial in numerous pathological events and
has significant roles in a number of physiological processes,
including remodeling of the extracellular matrix, degradation of
type IV collagen in the basement membrane and migration of
leukocytes during the immune and inflammatory responses (4,8,10,11).
Matrix metalloproteinase-9 (MMP-9), a subgroup of
zinc-dependent endopeptidases, degrades components of the basement
membrane, including collagen type IV, fibronectin and gelatin
(12). Previous studies have
demonstrated that the expression levels of MMP-9 in lung tissues of
PALI model rats are markedly increased compared with those in
healthy rat lungs (13). The
proteolytic cleavage function of MMP-9 results in disruption of the
alveolar-capillary barrier and lung edema (8). When the integrity of the
alveolar-capillary barrier is compromised, vessel permeability
increases and the alveolar-capillary barrier is no longer able to
regulate the passage of molecules between the interstitial and lung
parenchyma. This type of alveolar-capillary barrier dysregulation
leads to an increase in the amount of water in the extracellular
spaces of the lung tissue, namely, edema. In numerous types of lung
pathologies, including PALI, the levels of MMP-9 are markedly
upregulated. Thus, MMP-9 is considered to participate in the
formation and progression of alveolar-capillary barrier disruption
and lung edema (7,8). However, the molecular cascade leading
to the upregulation of the levels of MMP-9 following the
development of PALI has not been elucidated clearly.
Hypoxia-inducible factor 1 (HIF-1) is a highly
conserved transcription factor that is present in almost all types
of cell; it is strictly regulated by O2 availability.
HIF-1 exists as a heterodimer consisting of hypoxia-inducible
factor-1α (HIF-1α) and hypoxia-inducible factor-1β (HIF-1β)
subunits. HIF-1β is ubiquitously expressed, whereas HIF-1α is
observed at low levels under normoxic conditions (14). HIF-1α, an upstream transcription
factor induced by hypoxia, regulates the subsequent expression of
numerous types of proteins in response to the various
pathophysiological conditions induced by hypoxia (4,15).
Although previous studies have shown that the levels of HIF-1α are
upregulated in AP (16,17), a study has also reported that
HIF-1α is associated with augmented pulmonary vascular barrier
disruption (18). However, the
potential role of HIF-1α in lung tissue injury or restoration
following the development of PALI remains unclear. Thus, whether
HIF-1α contributes to the formation of alveolar-capillary
disruption and lung edema by regulating the expression of MMP-9 in
PALI remains to be clarified. The effects of HIF-1α following PALI
also require further elucidation.
The purpose of the present study was to determine
whether a molecular cascade involving HIF-1α and MMP-9 is causally
associated with alveolar-capillary disruption and lung edema
formation in a rodent model of PALI. This study further sought to
provide novel data that may support potential therapeutic targets
within this cascade for the alleviation of alveolar-capillary
disruption and lung edema in PALI.
Materials and methods
Animals
Male Sprague-Dawley rats, 180–220 g in weight, were
supplied by the Experimental Animal Center of Dalian Medical
University (Dalian, China). The animals fasted overnight prior to
the experiment, with water provided ad libitum. This study
was conducted in strict accordance with the recommendations in the
Guide for the Care and Use of Laboratory Animals of the National
Institutes of Health (1st edition, published in 1996). The animal
use protocol was reviewed and approved by the Institutional Animal
Care and Use Committee of Dalian Medical University.
Experimental design
A total of 40 male Sprague-Dawley rats were randomly
divided into the sham surgery group (control group, n=10), in which
the rats only underwent sham surgery, and three PALI groups (n=10
in each group), in which AP was induced by retrograde infusion of
5% sodium taurocholate (1 ml/kg). The PALI groups were as follows:
i) Untreated PALI group; ii) animals treated with the HIF-1α
inhibitor, 2-methoxyestradiol (2ME2; 5 mg/kg body mass; Selleck
Chemicals, Houston, TX, USA); and iii) animals treated with 2ME2
(15 mg/kg body mass). 2ME2 was administered intraperitoneally 1 h
after the induction of AP. All rats were sacrificed by femoral
venous puncture 24 h after the induction of AP. Blood was
immediately extracted from the abdominal aorta of the rats for
blood gas analysis. Both lung tissues were also immediately
collected and put into a freezing tube, which was then placed in
liquid nitrogen and transferred to a refrigerator at −80°C. The
frozen lung tissues were used for RT-PCR and Western blot
evaluation.
Induction of AP
AP was induced in 30 of the rats based on a
previously described method (5),
with minor modifications. Midline sterile laparotomy was performed
under anesthesia with 10% chloral hydrate (Tianjin Kermel Chemical
Reagent Co., Ltd., Tianjin, China) at a dose of 3 ml/kg by
intraperitoneal injection. Sodium taurocholate (≤5%; 1 ml/kg;
Sigma-Aldrich, St. Louis, MO, USA) was retrogradely infused into
the distal end of the bile-pancreatic duct. The proximal bile duct
was temporarily occluded at the hepatic portal by a vascular clamp
for 5 min. Subsequently, the vascular clamp was removed and the
duodenal and abdominal wounds were closed. The 10 rats in the sham
surgery group only underwent a laparotomy.
Serum amylase
In total, 10 rats were sacrificed to test the serum
amylase. Serum was harvested from the collected blood by
centrifugation using a high speed freezing centrifuge at 1,006 × g
for 10 min. The serum was stored at −80°C prior to evaluation of
the serum amylase levels using an automatic chemistry analyzer
(Vitros 3600; Johnson & Johnson, Rochester, NY, USA).
Wet/dry ratio
In total, 10 rats were sacrificed to test the
wet/dry ratio. The magnitude of the pulmonary edema in the rats was
determined by calculating the wet/dry ratio according to the
following formula (7): Wet/dry
ratio (%) = [(wet weight − dry weight)/dry weight] × 100, where the
wet weight is the initial left lung weight and the dry weight is
the weight of the lung following incubation at 72°C for 24 h.
Evans blue dye extravasation
In total, 10 rats were sacrificed to test the Evans
blue dye extravasation. The pulmonary microvascular permeability of
the rats was measured using a modification of the Evans blue dye
(Sigma-Aldrich) extravasation technique as previously described
(19). Briefly, the rats were
injected with 5% Evans blue dye through the internal jugular vein
at a dose of 2 mg/100 g 30 min prior to sacrifice. Immediately
after sacrifice, the lung tissues were collected and washed with
normal saline. The lung tissues were then weighed after drying with
filter paper. The Evans blue dye was extracted following
homogenization in 1 ml deionized formamide and pulverization using
an Ultrasonic Liquid Processor. A further 3 ml deionized formamide
and 1 ml deionized formamide was added, and the mixture was
incubated at 37°C for 48 h. The supernatant was separated by
centrifugation at 1,000 × g for 5 min. The quantity of dye
extracted was determined spectrophotometrically at 620 nm and
calculated from a standard curve established with known amounts of
Evans blue dye. Results are expressed as mg of dye per g of wet
tissue.
ELISA
A total of 10 rats was sacrificed to test the ELISA.
The levels of HIF-1α, MMP-9 and tumor necrosis factor-α (TNF-α) in
the serum were measured using commercially available ELISA kits
(Shanghai Westang Bio-Tech Co., Ltd., Shanghai, China) according to
the manufacturer’s instructions.
Reverse transcription-polymerase chain
reaction (RT-PCR)
Total RNA was extracted from the frozen tissue of
the right lower lung lobe with chloroform and RNAiso Plus reagent
[Takara Biotechnology (Dalian) Co., Ltd., Dalian, China] according
to the manufacturer’s instructions. The lungs were extracted from 8
rats. The total RNA was solubilized in RNase-free water and
quantified by NanoVue spectrophotometric measurement of the nucleic
acids and proteins (GE Healthcare, Little Chalfont, UK). The purity
of the RNA was assured by examining the optical density
(OD)260/OD280 ratio. The RNA (2 μl) was reverse transcribed to
complementary DNA using an RNA PCR kit (AMV) Ver. 3.0 [Takara
Biotechnology (Dalian) Co., Ltd.] according to the manufacturer’s
instructions. The PCR was performed using the primers presented in
Table I. The amplification steps
were as follows: Initial denaturation at 95°C for 3 min, 94°C
denaturation for 30 sec, 51°C annealing for 30 sec and 72°C
extension for 45 sec for 40 cycles, for HIF-1α; initial
denaturation at 95°C for 3 min, 94°C denaturation for 30 sec, 60°C
annealing for 30 sec and 72°C extension for 45 sec for 40 cycles,
for MMP-9; and initial denaturation at 95°C for 3 min, 94°C
denaturation for 30 sec, 52°C annealing for 30 sec and 72°C
extension for 45 sec for 40 cycles, for β-actin. The PCR products
(~5 μl) were electrophoresed using 1.7% agarose gel (Biowest,
Barcelona, Spain) containing ethidium bromide (0.5 μg/ml; Biosharp
Biotech Co., Hefei, China). The gels were visualized under UV
light, and images of the gels were captured. The band intensities
were determined by the ODs with individual PCR product/β-actin
ratios.
 | Table ISequences of the primers. |
Table I
Sequences of the primers.
| Cytokines | Product size
(bp) | Sense primer | Antisense primer |
|---|
| HIF-1α | 670 |
5′-GGCAACGAGAAGAAAAATAGG-3′ |
5′-GAGGAATGGGTTCACAAATC-3′ |
| MMP-9 | 196 |
5′-CCCTGCGTATTTCCATTCATC-3′ |
5′-ACCCCACTTCTTGTCAGCGTC-3′ |
| β-actin | 201 |
5′-CGTTGACATCCGTAAAGAC-3′ |
5′-TGGAAGGTGGACAGTGAG-3′ |
Western blot analysis
A total of 8 rats were used to extract the lungs.
The frozen lung tissues were mechanically processed in lysis buffer
(Nanjing KeyGen Biotech Co., Ltd., Nanjing, China) with protease
inhibitors, phenylmethanesulfonyl fluoride and phosphatase
inhibitor on ice using a protein extraction kit (Nanjing KeyGen
Biotech Co., Ltd.) according to the manufacturer’s instructions.
The total protein concentration was determined by NanoVue
spectrophotometric measurement of the nucleic acids and proteins
(GE Healthcare). Equal volumes (20 μl) of tissue extracts
normalized by protein concentration were separated by
electrophoresis through 10% sodium dodecyl sulfate-polyacrylamide
gel (Bio-Rad Laboratories, Inc., Hercules, CA, USA) and transferred
to polyvinylidene difluoride membranes. The membranes were blocked
with 5% evaporated skimmed milk (BD Biosciences, Sparks, MD, USA)
and then separately incubated with rabbit monoclonal antibody
against HIF-1α (1:1,000; Epitomics Inc., Burlingame, CA, USA) and
rabbit monoclonal antibody against MMP-9 (1:1,000; Epitomics Inc.).
Equal loading of protein was confirmed and adjusted by β-actin
monoclonal antibody (1:1,000; Wuhan Boster Biological Technology,
Ltd., Wuhan, China). These antibodies were incubated with the
membrane at room temperature for 2 h. Following three wash cycles
in Tris-buffered saline with Tween 20, the membrane was incubated
with secondary antibody peroxidase-conjugated AffiniPure goat
anti-rabbit IgG (1:5,000; ZSGB-BIO, Beijing, China). To quantify
the relative expression levels of the target protein, blot images
were captured and analyzed using an image analysis program
(BioSpectrum AC 410; UVP, LCC, Upland, CA, USA). The expression
intensities of the proteins from the different groups were
statistically compared.
Histological examination
In total 8 rats were used to extract the lungs.
Morphological alterations in the lungs and pancreas were examined
in individual rats from each of the four groups. The lungs and
pancreas were fixed with 10% formalin and embedded in paraffin.
Paraffin sections (4 μm thick) were stained with hematoxylin and
eosin (H&E) for examination by light microscopy (model TS100,
Nikon, Japan). A scoring system to grade the degree of lung and
pancreatic injury was employed (20,21).
In this system, the lung injury was assessed from the degree of
edema, inflammatory cell infiltration and bleeding, each of which
was scored on a scale of 0–3, and the pancreatic injury was
assessed from the degree of edema, inflammation, vacuolization and
necrosis, each of which was scored on a scale of 0–4. The grading
was performed by a blinded pathologist. The injury scores were
calculated by adding the individual scores for each category.
Statistical analysis
All data are presented as the mean ± standard
deviation. Statistical analysis was performed with SPSS software
for Windows, version 16.0 (SPSS, Inc., Chicago, IL, USA). The
differences among multiple groups were assessed using χ2
analysis with P<0.05 considered to indicate a statistically
significant difference.
Results
General information
Compared with those of the control group, the levels
of serum amylase, PaCO2 and the wet/dry ratio increased
and PaO2 decreased in the untreated PALI group.
Following the administration of the HIF-1α inhibitor, the levels of
serum amylase, PaCO2 and the wet/dry ratio decreased,
whereas the PaO2 increased, compared with those in the
untreated PALI group. Furthermore, the effect of the larger dose of
the HIF-1α inhibitor was stronger than that of the smaller dose
(Table II).
| Table IIComparison of serum amylase levels,
blood gas analysis and wet/dry weight ratio of lung tissue in the
various groups. |
Table II
Comparison of serum amylase levels,
blood gas analysis and wet/dry weight ratio of lung tissue in the
various groups.
| Groups |
PaO2/mmHg |
PaCO2/mmHg | AMY (U/l) | W/D |
|---|
| Control | 98.05±1.13 | 24.99±2.08 | 1864.5±385.22 | 0.87±0.31 |
| PALI | 74.72±2.30a | 50.34±2.31a |
9428.1±302.80a | 2.86±0.43a |
| PALI + 2ME2 (5
mg/kg) | 83.01±2.83a,b | 40.16±1.10a,b |
7048.1±847.51a,b | 2.45±0.35a,c |
| PALI + 2ME2 (15
mg/kg) | 89.12±2.44a,c | 32.01±1.24a,b |
3923.8±191.12a,c | 1.94±0.28a,c |
Lung permeability
The rats in the untreated PALI group showed a
significant increase in the microvascular capillary permeability of
the lung compared with that of the sham surgery group. Following
the administration of the HIF-1α inhibitor 2ME2 (5 mg/kg), the
capillary leakage was reduced significantly compared with that of
the untreated PALI group. Compared with that of the PALI + 2ME2 (5
mg/kg) group, the blue dye accumulation in the lung parenchyma of
the PALI + 2ME2 (15 mg/kg) group was significantly reduced
(Fig. 1A).
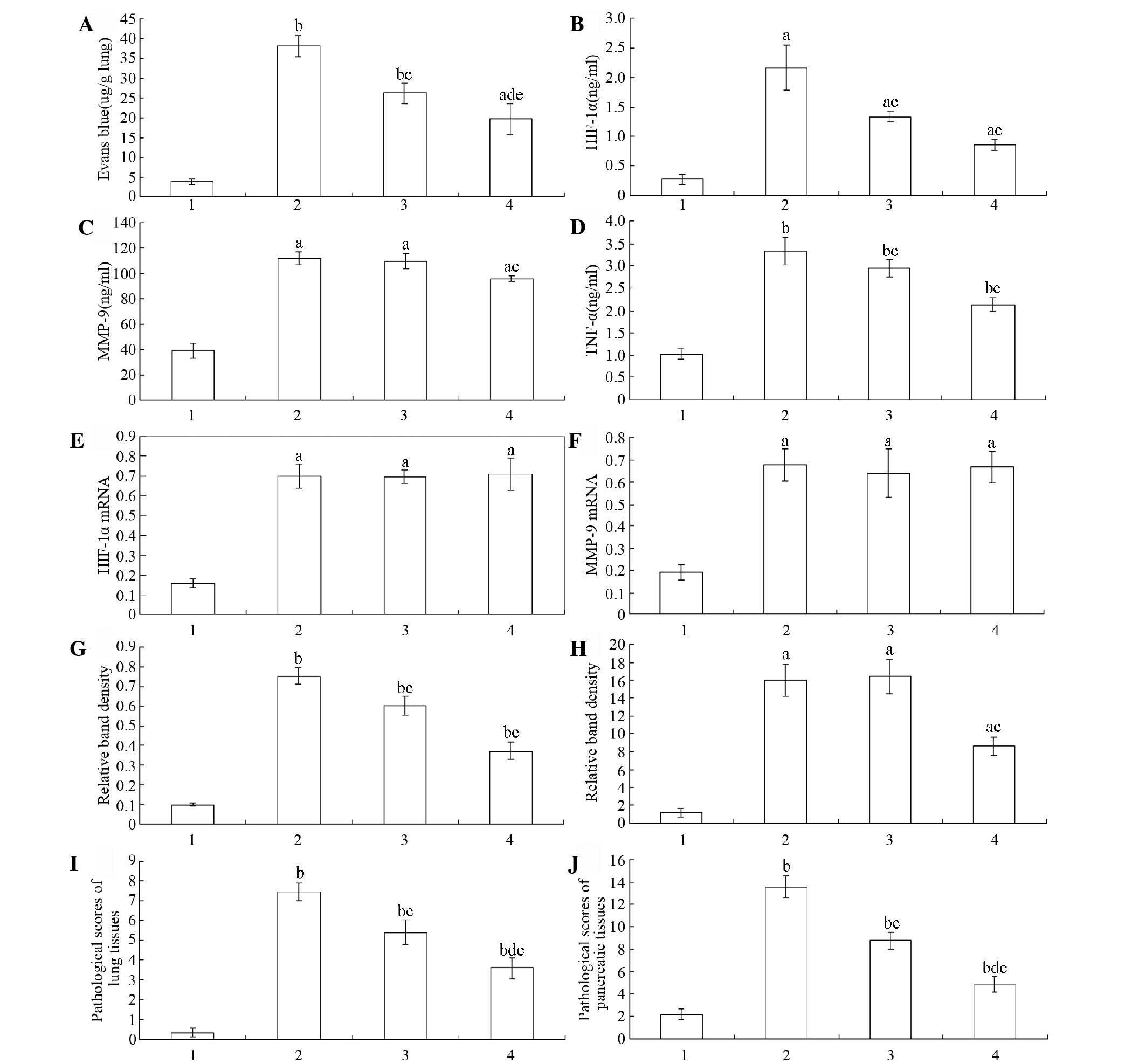 | Figure 1Levels of Evans blue dye
extravasation, active HIF-1α, MMP-9, TNF-α expression, HIF-1α and
MMP-9 mRNA and protein expression, and pathological scores of lung
and pancreatic tissues in the various groups. (A) Capillary
permeability measured by Evans blue dye extravasation in the
various groups. Serum expression levels of (B) active HIF-1α, (C)
MMP-9 and (D) TNF-α in the various groups. Expression levels of (E)
HIF-1α and (F) MMP-9 mRNA in lung tissues and of (G) HIF-1α and (H)
MMP-9 protein in lung tissues. Pathological scores of the (I) lung
and (J) pancreatic tissues in the various groups. Data are
presented as the mean ± standard deviation (n=10). 1, control
group; 2, untreated PALI group; 3, PALI + 2ME2 (5 mg/kg); 4, PALI +
2ME2 (15 mg/kg). aP<0.05, bP<0.01 vs.
the sham surgery group; cP<0.05,
dP<0.01 vs. the PALI group. HIF-1α, hypoxia inducible
factor-1α; MMP-9, matrix metalloproteinase-9; TNF-α, tumor necrosis
factor-α; PALI, pancreatitis-associated lung injury; 2ME2,
2-methoxyestradiol. |
Levels of active HIF-1α, MMP-9 and
TNF-α
For the quantitative determination of the active
levels of HIF-1α, MMP-9 and TNF-α in the serum, a fluorescence
ELISA designed to measure the HIF-1α, MMP-9 and TNF-α activity
levels was used. The results showed that compared with those of the
control group, the levels of HIF-1α, MMP-9 and TNF-α increased in
the untreated PALI group. Following the administration of the
HIF-1α inhibitor, the levels of HIF-1α, MMP-9 and TNF-α decreased
compared with those of the untreated PALI group. Furthermore, the
effect of the larger dose of the HIF-1α inhibitor was stronger than
that of the smaller dose (Fig.
1B–D).
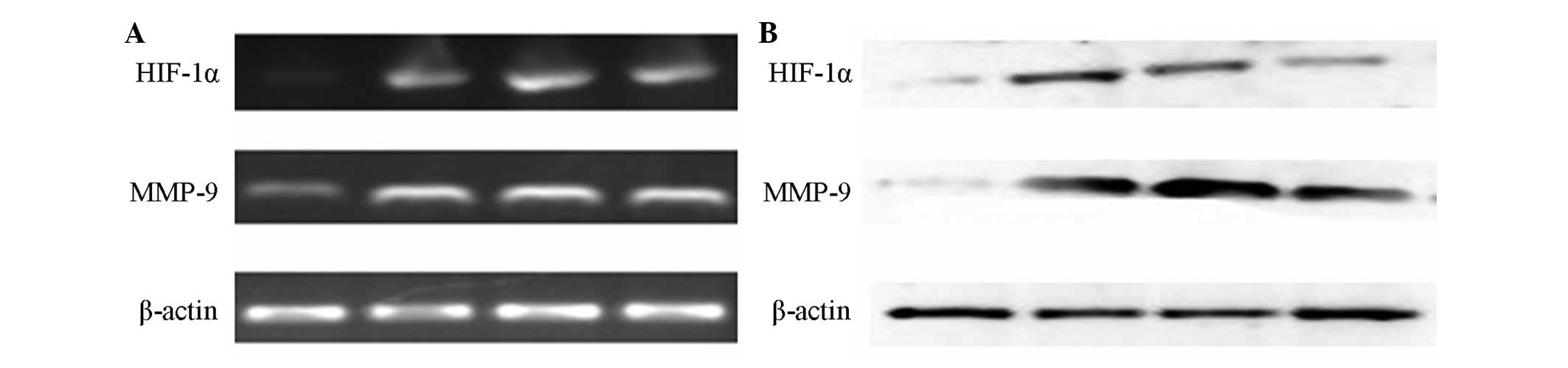
HIF-1α and MMP-9 mRNA expression
levels
The RT-PCR showed that the mRNA expression levels of
HIF-1α and MMP-9 were upregulated significantly in the untreated
PALI group compared with those in the control group. However, the
HIF-1α and MMP-9 mRNA levels in the lung tissues did not exhibit
significant differences between the untreated PALI group and the
two 2ME2 groups (Figs. 1E, 1F and
2A).
HIF-1α and MMP-9 protein expression
levels
HIF-1α expression levels are reportedly upregulated
during AP (16,17). HIF-1α was almost undetectable in
the lung tissues of the rats in the sham surgery group. The HIF-1α
and MMP-9 protein expression levels showed significant increases in
the untreated PALI group compared with those in the control group.
Compared with those in the untreated PALI group, the HIF-1α protein
expression levels were significantly reduced in the PALI + 2ME2 (5
mg/kg) and PALI + 2ME2 (15 mg/kg) groups. However, the difference
in the MMP-9 protein levels between the untreated PALI and PALI +
2ME2 (5 mg/kg) groups was weakly distinguishable, whereas in the
PALI + 2ME2 (15 mg/kg) group, the MMP-9 protein expression levels
were significantly reduced compared with those in the untreated
PALI group (Figs. 1G, 1H and
2B).
Histological examination
The lung and pancreatic tissues were sectioned,
stained with H&E and scored for edema, acinar necrosis,
hemorrhage and fat necrosis, inflammation and perivascular
infiltration (Table III).
| Table IIIRelative levels of the pathological
scores of the lung and pancreatic tissues of the rats in the
various groups. |
Table III
Relative levels of the pathological
scores of the lung and pancreatic tissues of the rats in the
various groups.
| Groups | Lung tissues | Pancreatic
tissues |
|---|
| Control | 0.3±0.23 | 2.15±0.47 |
| PALI | 7.5±0.44a | 13.55±1.01a |
| PALI + 2ME2 (5
mg/kg) | 5.4±0.61a,b | 8.75±0.75a,b |
| PALI + 2ME2 (15
mg/kg) | 3.6±0.52a,c,d | 4.85±0.71a,c,d |
The rats in the untreated PALI group showed
significant increases in pathological scores of lung and pancreatic
tissues compared with those in the sham surgery group. Compared
with those in the PALI + 2ME2 (5 mg/kg) group, the pathological
scores of the lung and pancreatic tissues in the PALI + 2ME2 (15
mg/kg) group were significantly reduced (Figs. 1I and 3A–D, and Figs. 1J and 3E–H for lung and pancreas,
respectively).
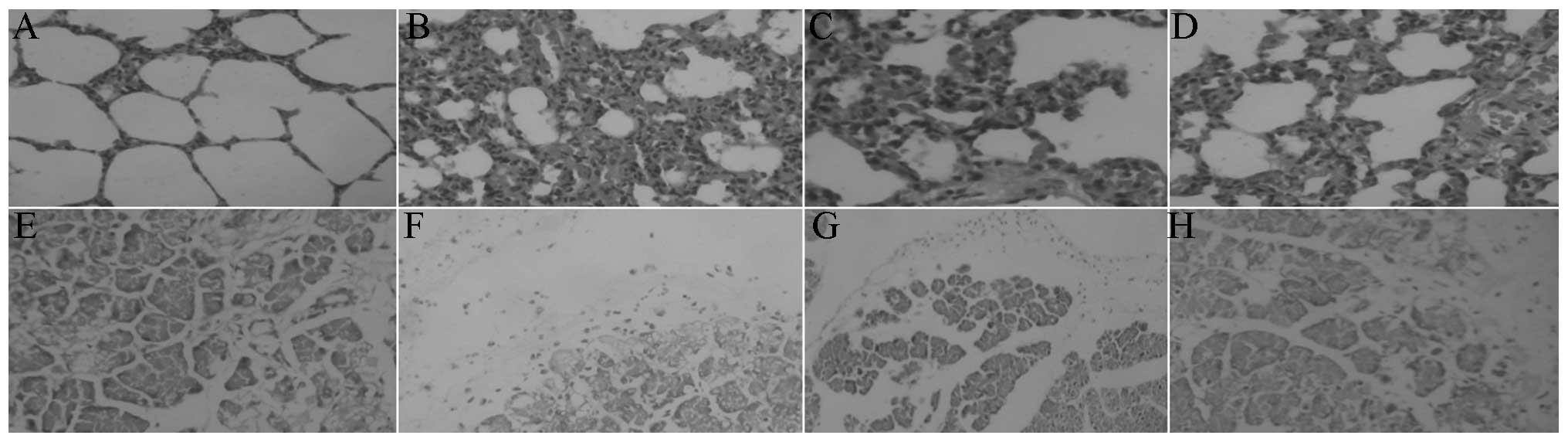 | Figure 3Representative photomicrographs of the
lungs and pancreas in the various groups. The pathology of the lung
(A–D) and pancreatic (E–H) tissues in the (A,E) control group, (B,
F) untreated PALI group, (C, G) PALI + 2ME2 (5 mg/kg) group, and
(D, H) PALI + 2ME2 (15 mg/kg) group. H&E staining;
magnification, ×20. PALI, pancreatitis-associated lung injury;
2ME2, 2-methoxyestradiol, H&E, hematoxylin and eosin. |
Discussion
Previous studies have demonstrated that HIF-1α may
regulate MMP-9 expression in the pathogenesis of blood-brain
barrier disruption and brain edema following brain injury (4,22).
Bai et al (16) observed
that HIF-1α has an important function in the pathogenesis of AP.
Keck et al (13) found that
MMP-9 also participates in the pathogenesis of PALI. Thus, whether
HIF-1α contributes to the formation of lung edema by regulating
MMP-9 requires clarification.
The major finding of the present study is that the
concurrently elevated expression levels of HIF-1α and MMP-9 in the
lung tissues of rat models of PALI temporally coincided with lung
edema formation and alveolar-barrier disruption. In the PALI model
used in the present study, the edema, determined by the wet/dry
ratio, was reduced by the HIF-1α-selective inhibitor, 2ME2,
compared with that in the untreated PALI group. In addition, the
alveolar-barrier disruption determined by Evans blue dye
extravasation was also ameliorated by the inhibition of HIF-1α by
2ME2. At the same time, the inhibition of HIF-1α caused reduced
levels of serum amylase, PaCO2 and pathological scores
of the tissues of the lung and pancreas, as well as increased
PaO2 compared with those in the untreated PALI
group.
The data in the present study further support the
hypothesis that HIF-1α affects the pathogenesis of PALI, which is
consistent with the findings of previous studies (14,16,18).
Blocking HIF-1α expression may prevent the formation of lung edema
and alveolar-capillary barrier disruption, alleviate PALI and
provide a novel approach for the treatment of AP.
Furthermore, the larger dose of the HIF-1α inhibitor
downregulated the protein expression levels of MMP-9 in the PALI
model compared with those in the untreated PALI group. The findings
of the present study suggest a functional interaction linking MMP-9
and HIF-1α, which is possibly dysregulated in PALI. The data also
suggest that HIF-1α regulates the expression levels of MMP-9, which
are crucial in edema formation and alveolar-capillary barrier
disruption in PALI.
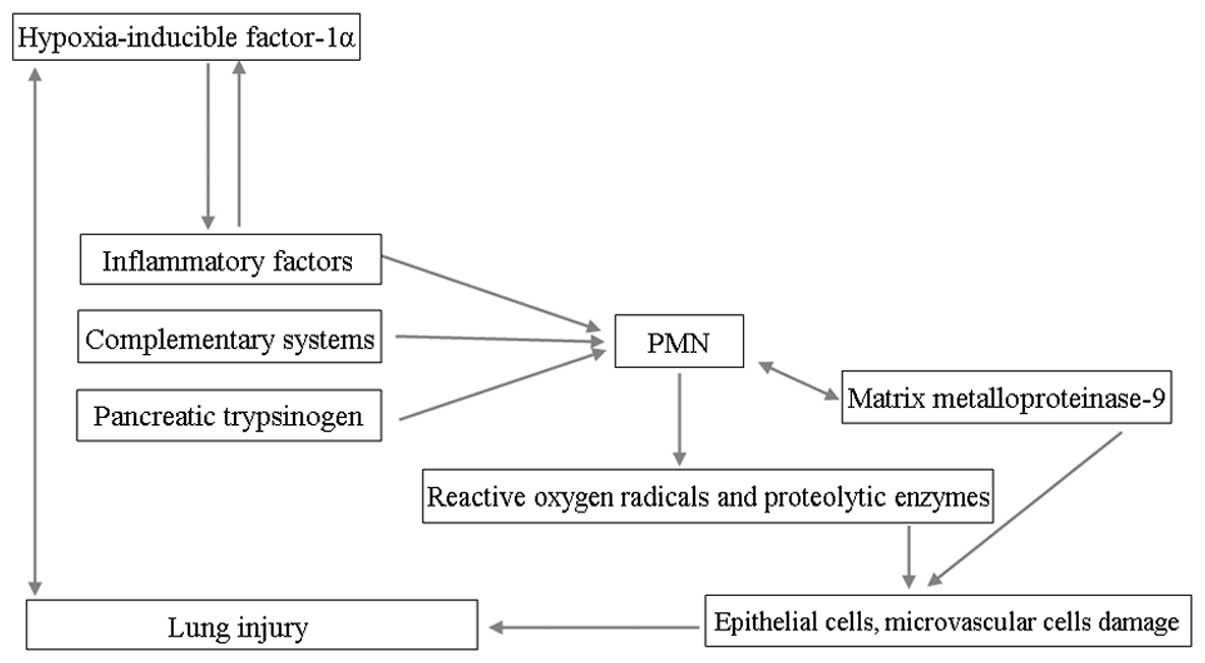
The large quantities of inflammatory factors that
enter the lung tissues in PALI cause damage and necrosis of lung
epithelial cells, microvascular endothelial cells and tight
junctions. Furthermore, pancreatic proteinase activates the
complementary systems, indirectly leading to increased tissue
damage effects and pulmonary transudate, which cause a reduction in
the pulmonary functions of ventilation. Thus, hypoxia may be a
severe consequence of PALI, leading to aberrations in lung function
and repair (15). Hypoxia also
results in damage of the alveolar lining layer, apoptosis of
alveolar epithelial cells, lung edema, increased vascular
permeability and augmented barrier disruption (14,18).
Previous studies have demonstrated that hypoxia
elicits tissue inflammation (23,24).
For example, Hartmann et al (24) demonstrated that exposure to a high
altitude is associated with elevated levels of inflammatory
mediators in humans. Similarly, mice that are exposed to acute
hypoxia (e.g., 8% oxygen over 8 h) develop elevated plasma levels
of cytokines, in conjunction with pulmonary edema and inflammatory
cell accumulation in the lungs and other organs (9,25).
In the inflammatory response, a large dose of cytokines (TNF-α,
IL-1β and IL-8) and serine proteases derived from the pancreas may
activate polymorphonuclear leukocytes (PMNs), which secrete
significant amounts of MMP-9. Subsequently, MMP-9 promotes PMN
migration, alveolar capillary leakage and lung edema (13,26)
(Fig. 4).
2ME2 is a naturally endogenous-occurring metabolite
of estradiol, which post-transcriptionally downregulates the
expression levels of HIF-1α and is an anti-angiogenic and antitumor
agent (27,28). Studies have provided in
vitro and in vivo evidence that 2ME2 has a direct effect
on the inhibition of HIF-1α and the inhibition is not the result of
a ‘side-effect’ of mitotic arrest (29,30).
Furthermore, 2ME2 treatment reduces the levels of nuclear and total
HIF-1α proteins in a dose-dependent manner. The downregulated
expression levels of HIF-1α post-transcription may be the reason
for the absence of statistical significance between the HIF-1 and
MMP-9 mRNA expression levels following the administration of 2ME2
and in the untreated PALI group in the present study. 2ME2 inhibits
HIF-1α translation and nuclear translocation, thereby suppressing
the inflammatory response, PMN activation and MMP-9 expression
(27).
The aforementioned results suggest that HIF-1α may
be an upstream protein that causes the alveolar-capillary barrier
disruption and lung edema formation in PALI through its regulatory
expression of catalytic enzymes, including MMP-9.
In conclusion, the present study demonstrated in a
PALI model that an HIF-1α-MMP-9 signaling cascade exists, wherein
PALI first triggers induction of HIF-1α, which in turn upregulates
MMP-9 expression levels and leads to pathophysiological
alveolar-capillary barrier disruption and lung edema. Inhibition of
HIF-1α may provide novel insights into PALI. These findings enhance
our knowledge of the prevention of acute lung injury secondary to
severe AP.
Acknowledgements
The authors thank The Key Laboratory for Basic
Research of Difficult and Critical Diseases with Integrated
Traditional and Western Medicine of Liaoning Province. This study
was supported by grants from National Natural Science Foundation of
China (81173452).
References
|
1
|
Bhatia M, Wong FL, Cao Y, et al:
Pathophysiology of acute pancreatitis. Pancreatology. 5:132–144.
2005. View Article : Google Scholar
|
|
2
|
Bhatia M: Novel therapeutic targets for
acute pancreatitis and associated multiple organ dysfunction
syndrome. Curr Drug Targets Inflamm Allergy. 1:343–351. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wang G, Chen HL, Ren F, Li J and Li YQ:
Expression of Cav-1, AQP1 and AQP5 in lung of acute
pancreatitis-associated lung injury rats and the therapeutic role
of Qingyitang. Zhonghua Yi Xue Za Zhi. 90:2564–2569. 2010.(In
Chinese).
|
|
4
|
Higashida T, Kreipke CW, Rafols JA, et al:
The role of hypoxia-inducible factor-1α, aquaporin-4, and matrix
metalloproteinase-9 in blood brain barrier disruption and brain
edema after traumatic brain injury. J Neurosurg. 114:92–101.
2011.
|
|
5
|
Gao ZM, Chen HL and Liu XD: Expression and
function of aquaporin-1 in acute lung injury induced by severe
acute pancreatitis in rats. Shi Jie Hua Ren Xiao Hua Za Zhi.
15:453–457. 2007.(In Chinese).
|
|
6
|
Renzulli P, Jakob SM, Täuber M, Candinas D
and Gloor B: Severe acute pancreatitis: Case-oriented discussion of
interdisciplinary management. Pancreatology. 5:145–156. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Chen P, Huang L, Sun Y and Yuan Y:
Upregulation of PIAS1 protects against sodium taurocholate-induced
severe acute pancreatitis associated with acute lung injury.
Cytokine. 54:305–314. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sochor M, Richter S, Schmidt A, Hempel S,
Hopt UT and Keck T: Inhibition of matrix metalloproteinase-9 with
doxycycline reduces pancreatitis-associated lung injury. Digestion.
80:65–73. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Eckle T, Faigle M, Grenz A, Laucher S,
Thompson LF and Eltzschig HK: A2B adenosine receptor dampens
hypoxia-induced vascular leak. Blood. 111:2024–2035. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pirrone F, Pastore C, Mazzola S and
Albertini M: In vivo study of the behaviour of matrix
metalloproteinases (MMP-2, MMP-9) in mechanical, hypoxic and
septic-induced acute lung injury. Vet Res Commun. 33(Suppl 1):
121–124. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kobayashi Y, Matsumoto M, Kotani M and
Makino T: Possible involvement of matrix metalloproteinase-9 in
Langerhans cell migration and maturation. J Immunol. 163:5989–5993.
1999.PubMed/NCBI
|
|
12
|
Martinez-Hernandez A and Amenta PS: The
basement membrane in pathology. Lab Invest. 48:656–677. 1983.
|
|
13
|
Keck T, Balcom JH 4th, Fernández-del
Castillo C, Antoniu BA and Warshaw AL: Matrix metalloproteinase-9
promotes neutrophil migration and alveolar capillary leakage in
pancreatitis-associated lung injury in the rat. Gastroenterology.
122:188–201. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Shimoda LA and Semenza GL: HIF and the
lung: role of hypoxia-inducible fctors in pulmonary development and
disease. Am J Respir Crit Care Med. 183:152–156. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Semenza G: Signal transduction to
hypoxia-inducible factor 1. Biochem Pharmacol. 64:993–998. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bai X, Sun B, Pan S, et al:
Down-regulation of hypoxia-inducible factor-1alpha by hyperbaric
oxygen attenuates the severity of acute pancreatitis in rats.
Pancreas. 38:515–522. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Gomez G, Englander EW, Wang G and Greeley
GH Jr: Increased expression of hypoxia-inducible factor-1alpha,
p48, and the Notch signaling cascade during acute pancreatitis in
mice. Pancreas. 28:58–64. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Becker PM, Alcasabas A, Yu AY, Semenza GL
and Bunton TE: Oxygen-independent upregulation of vascular
endothelial growth factor and vascular barrier dysfunction during
ventilated pulmonary ischemia in isolated ferret lungs. Am J Respir
Cell Mol Biol. 22:272–279. 2000. View Article : Google Scholar
|
|
19
|
Standiford TJ, Kunkel SL, Lukacs NW, et
al: Macrophage inflammatory protein-1 alpha mediates lung leukocyte
recruitment, lung capillary leak, and early mortality in murine
endotoxemia. J Immunol. 155:1515–1524. 1995.PubMed/NCBI
|
|
20
|
Schmidt J, Rattner DW, Lewandrowski K, et
al: A better model of acute pancreatitis for evaluating therapy.
Ann Surg. 215:44–56. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Wang H, Liu JW, Li ZL, et al: Development
of a rat model of severe acute pancreatitis associated lung injury.
Shi Jie Hua Ren Xiao Hua Za Zhi. 21:211–219. 2013.(In Chinese).
|
|
22
|
Chen C, Ostrowski RP, Zhou C, Tang J and
Zhang JH: Suppression of hypoxia-inducible factor-1α and its
downstream genes reduces acute hyperglycemia-enhanced hemorrhagic
transformation in a rat model of cerebral ischemia. J Neurosci Res.
88:2046–2055. 2010.
|
|
23
|
Koeppen M, Eckle T and Eltzschig HK: The
hypoxia-inflammation link and potential drug targets. Curr Opin
Anaesthesiol. 24:363–369. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hartmann G, Tschöp M, Fischer R, et al:
High altitude increases circulating interleukin-6, interleukin-1
receptor antagonist and C-reactive protein. Cytokine. 12:246–252.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Rosenberger P, Schwab JM, Mirakaj V, et
al: Hypoxia-inducible factor-dependent induction of netrin-1
dampens inflammation caused by hypoxia. Nat Immunol. 10:195–202.
2009. View
Article : Google Scholar : PubMed/NCBI
|
|
26
|
Hartwig W, Werner J, Jimenez RE, et al:
Trypsin and activation of circulating trypsinogen contribute to
pancreatitis-associated lung injury. Am J Physiol. 277:G1008–G1016.
1999.PubMed/NCBI
|
|
27
|
Zhou H, Chen X, Zhang WM, Zhu LP and Cheng
L: HIF-1α inhibition reduces nasal inflammation in a murine
allergic rhinitis model. Plos One. 7:e486182012.
|
|
28
|
Mabjeesh NJ, Escuin D, LaVallee TM, et al:
2ME2 inhibits tumor growth and angiogenesis by disrupting
microtubules and dysregulating HIF. Cancer Cell. 3:363–375. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Salama SA, Kamel MW, Botting S, et al:
Catechol-o-methyltransferase expression and 2-methoxyestradiol
affect microtubule dynamics and modify steroid receptor signaling
in leiomyoma cells. PLoS One. 4:e73562009. View Article : Google Scholar
|
|
30
|
Pastor CM, Matthay MA and Frossard JL:
Pancreatitis-associated acute lung injury: new insights. Chest.
124:2341–2351. 2003. View Article : Google Scholar : PubMed/NCBI
|