Introduction
Calcifying aponeurotic fibroma (CAF), also known as
juvenile aponeurotic fibroma, is a rare, benign fibrous tumor that
occurs in the distal extremities, in particular on the palmar
surface of the hand. It usually presents as a slowly growing,
painless, firm mass in children and adolescents, with a slight male
predominance (1). Due to its
infiltrative nature, CAF has a high rate of local recurrence
following surgical excision. Malignant transformation is extremely
rare (2). In the present study, a
case of CAF arising in the little finger of an elderly patient is
presented, as well as a review of the literature.
Case report
A 69-year-old woman presented with a 7-year history
of a slow-growing, painless mass in the radial side of the right
little finger at the proximal interphalangeal joint. There was no
history of antecedent trauma. Physical examination revealed a firm,
immobile, non-tender mass. Neurovascular examinations were normal
and the results from laboratory tests were within the normal
limits, including C-reactive protein levels and white blood cell
counts. The patient’s past medical history was unremarkable.
Plain radiographs revealed a faintly calcified soft
tissue mass without bone involvement (Fig. 1), and computed tomography (CT)
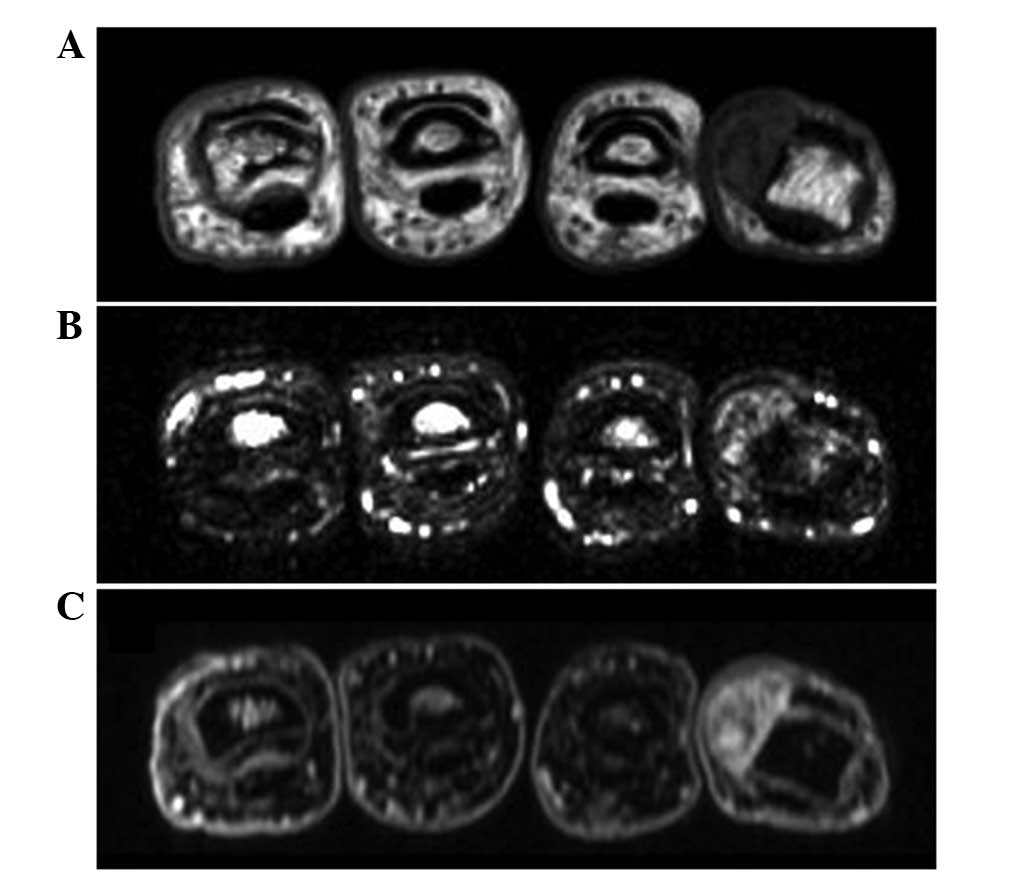
scans confirmed the presence of the lesion (Fig. 2). Magnetic resonance imaging (MRI)
exhibited a relatively well-defined soft tissue mass, 1.2×1.0×0.6
cm in size. The mass showed low to intermediate signal intensity on
T1-weighted images (Fig. 3A) and
heterogeneous high signal intensity with small foci of low signal
intensity on T2-weighted spectral presaturation with inversion
recovery images (Fig. 3B).
Contrast-enhanced fat-suppressed T1-weighted images demonstrated
intense heterogeneous enhancement throughout the mass (Fig. 3C). Based on these findings, the
patient was diagnosed with a benign soft tissue tumor, including
soft tissue chondroma.
An excisional biopsy was performed under general
anesthesia with tourniquet control. A midlateral incision was made
on the radial side of the right little finger. The mass was
adherent to the surrounding fibrous tissues; however, the mass was
fully excised. No adjacent bone involvement was noted.
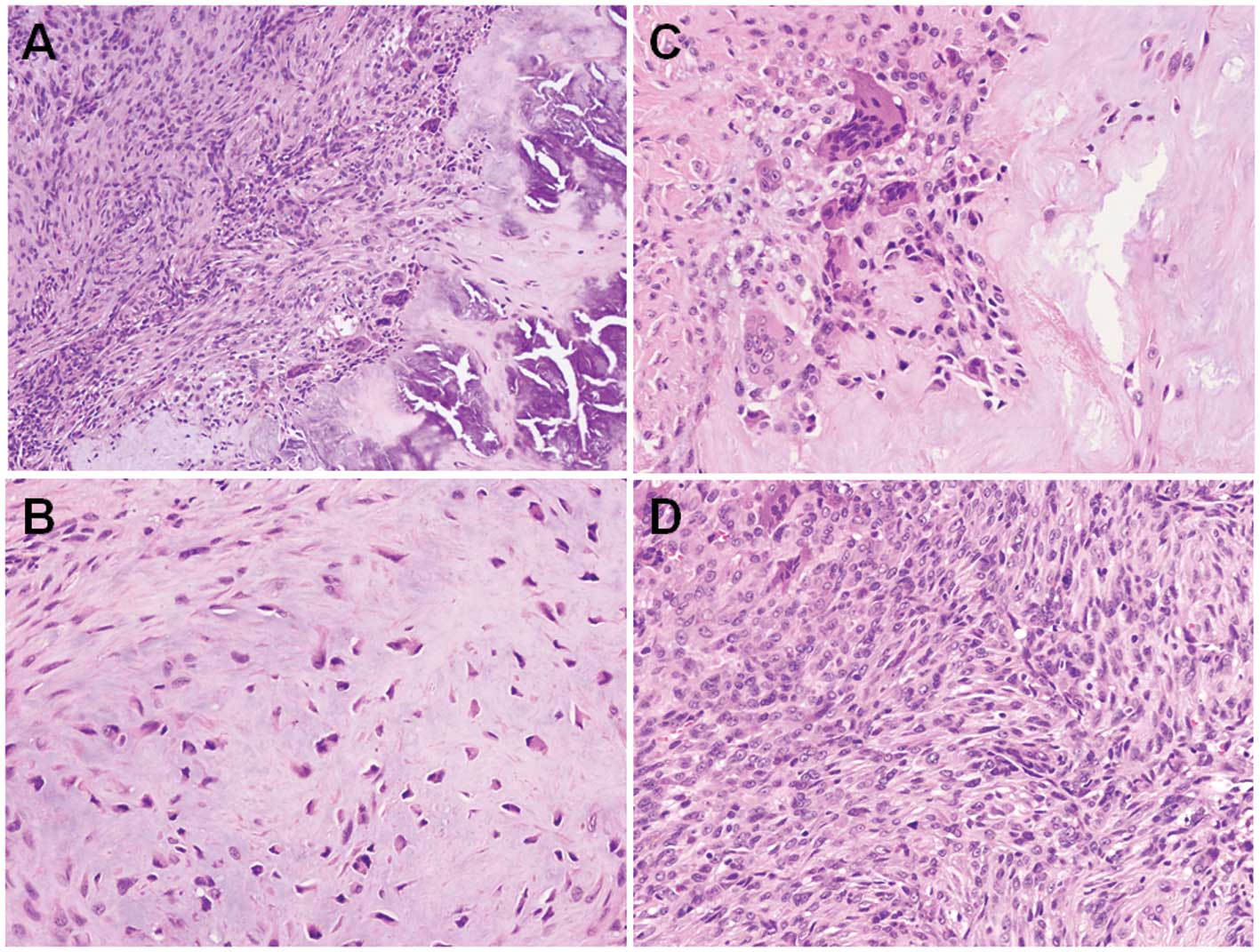
Histologically, the tumor showed a biphasic pattern, composed of a
moderately cellular fibromatosis-like component and irregular
calcified areas with polygonal epithelioid cells (Fig. 4A) and foci of cartilaginous
metaplasia were observed in the calcified areas (Fig. 4B). Multinucleated osteoclast-type
giant cells were found around the calcified areas (Fig. 4C). The proliferating cells did not
exhibit cellular atypia or evident mitotic figures (Fig. 4D). The results from the
histopathological analysis were consistent with CAF.
The postoperative course was uneventful, and there
was no evidence of local recurrence four months following
surgery.
Written informed consent for publication was
obtained from the patient and this study was approved by the
Institutional Review Board (Fukuoka, Japan).
Discussion
CAF occurs in patients over a wide age range;
however, it is most common in children and adolescents (1). The median ages for male and female
patients are 11 and 12 years, respectively (3). To the best of our knowledge, the
present case is the oldest reported case of CAF.
CAF grows in a diffuse, poorly circumscribed manner
and is often attached to the aponeurosis, tendons or fascia.
Complete local excision is the treatment of choice. The
histological examination of the lesion reveals two components: i)
fibromatosis-like spindle-shaped cell elements, and ii) nodules of
calcification, accompanied by more rounded, epithelioid cells
(1). Two phases have been
described in the development of CAF (4); in the initial phase the tumor has an
infiltrative growth and often lacks calcification, whilst in the
later phase the tumor is more compact and nodular and exhibits a
more prominent degree of calcification and cartilage formation, as
seen in the present case.
The pathogenesis of CAF remains uncertain; however,
a fibroblastic/myofibroblastic origin has been suggested (3). It has been previously demonstrated
using immunohistochemistry that the tumor cells usually express
vimentin and smooth muscle actin, but are negative for desmin
(1), and these results are in
accordance with this proposal.
Only a few studies have described the imaging
features of CAF. Plain radiographs may show a nonspecific soft
tissue mass, with a variable extent of finely stippled
calcifications (5), and bone
involvement is rarely observed. CT scans are useful in order to
determine the calcified areas of the lesion and its association
with the adjacent bone. On MRI, CAF typically appears as an
ill-defined subcutaneous mass with intermediate to low signal
intensity on T1-weighted sequences and heterogeneous high signal
intensity on T2-weighted sequences (6). Prominent areas of globular low signal
intensity may be seen on all MR pulse sequences, corresponding with
the presence of calcification. CAF usually demonstrates intense
heterogeneous enhancement following intravenous gadolinium
administration (6). The imaging
results from the present case study were consistent with the
aforementioned findings.
In older patients, the distinction of CAF from soft
tissue chondroma may be difficult. As with CAF, soft tissue
chondroma occurs most commonly in the finger or hand, with no
connection to the underlying bone (7). However, unlike CAF, soft tissue
chondroma is typically well-circumscribed rather than having an
infiltrative border. In addition, soft tissue chondroma is less
likely than CAF to recur. On MRI, soft tissue chondroma usually
appears as a well-defined mass with intermediate signal intensity
on T1-weighted sequences and high signal intensity on T2-weighted
sequences (8). The most important
histological finding distinguishing soft tissue chondroma from CAF
is the presence of infiltrating fascicles of fibroblasts at the
periphery of CAF (9).
In conclusion, in the present case report the
imaging findings of CAF with pathologic correlation in an elderly
patient are described. Although rare, CAF should be considered in
the differential diagnosis of elderly patients with a calcified
soft tissue mass, in particular in the finger or hand.
Acknowledgements
This study was supported in part by the Foundation
for the Promotion of Medical Science.
References
|
1
|
Kilpatrick SE: Calcifying aponeurotic
fibroma. World Health Organization Classification of Tumours of
Soft Tissue and Bone. Fletcher CDM, Bridge JA, Hogendoorn PCW and
Mertens F: 4th edition. IARC Press; Lyon: pp. 632013
|
|
2
|
Lafferty KA, Nelson EL, Demuth RJ, Miller
SH and Harrison MW: Juvenile aponeurotic fibroma with disseminated
fibrosarcoma. J Hand Surg Am. 11:737–740. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Fetsch JF and Miettinen M: Calcifying
aponeurotic fibroma: a clinicopathologic study of 22 cases arising
in uncommon sites. Hum Pathol. 29:1504–1510. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Weiss SW and Goldblum JR: Enzinger and
Weiss’s Soft Tissue Tumors. Calcifying aponeurotic fibroma. 5th
edition. Mosby Elsevier; Philadelphia, USA: pp. 289–293. 2008
|
|
5
|
Murphey MD, Ruble CM, Tyszko SM,
Zbojniewicz AM, Potter BK and Miettinen M: From the archives of the
AFIP: musculoskeletal fibromatoses: radiologic-pathologic
correlation. Radiographics. 29:2143–2173. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Morii T, Yoshiyama A, Morioka H, Anazawa
U, Mochizuki K and Yabe H: Clinical significance of magnetic
resonance imaging in the preoperative differential diagnosis of
calcifying aponeurotic fibroma. J Orthop Sci. 13:180–186. 2008.
View Article : Google Scholar
|
|
7
|
Rosenberg AE and Mandahl N: Soft-tissue
chondroma. World Health Organization Classification of Tumours of
Soft Tissue and Bone. Fletcher CDM, Bridge JA, Hogendoorn PCW and
Mertens F: 4th edition. IARC Press; Lyon: pp. 160–161. 2013
|
|
8
|
Hondar Wu HT, Chen W, Lee O and Chang CY:
Imaging and pathological correlation of soft-tissue chondroma: a
serial five-case study and literature review. Clin Imaging.
30:32–36. 2006.PubMed/NCBI
|
|
9
|
Tai LH, Johnston JO, Klein HZ, Rowland J
and Sudilovsky D: Calcifying aponeurotic fibroma features seen on
fine-needle aspiration biopsy: case report and brief review of the
literature. Diagn Cytopathol. 24:336–339. 2001. View Article : Google Scholar : PubMed/NCBI
|