Introduction
Anti-N-methyl-D-aspartate receptor (anti-NMDAR)
encephalitis is a newly recognized autoimmune disorder that was
first reported as paraneoplastic limbic encephalitis in 2007
(1). It is especially prevalent in
young women with ovarian terotomas (2). However, more recent studies have
revealed that it is not necessarily a paraneoplastic syndrome and
may occur in patients without tumors (3). The clinical presentation of
anti-NMDAR encephalitis includes acute psychiatric symptoms,
cognitive disturbance, new onset of seizures, memory deficits,
dyskinesia, dystonia, rigidity, ataxia and dysautonomia (4). Precise diagnosis may be established
if anti-NMDAR antibodies are detected in the cerebral spinal fluid
(CSF) and blood serum. There are no positive diagnostic features on
brain magnetic resonance imaging (MRI) scans (5). Until recently, few studies have
investigated the application of 18F-fluorodeoxyglucose
positron emission tomography (18F-FDG PET) in the
treatment of anti-NMDAR encephalitis. The present study describes a
case of anti-NMDAR encephalitis that was diagnosed in a young
female who presented subacute encephalitis and psychiatric
manifestation without evidence of malignancy. The study was
approved by the Ethics Committee of Zhejiang Provincial People’s
Hospital (Hangzhou, China) and informed consent was provided by the
patient.
Case report
A 38-year-old female with no significant past
medical history, was admitted to Zhejiang Provincial People’s
Hospital due to the sudden onset of behavioral disturbance, speech
problems and psychiatric symptoms one week previously. The patient
was unable to answer simple questions and responded to all
questions with meaningless answers. The patient also presented
intermittent confusion associated with anxiety and agitation. The
patient denied any problems with her eating and sleeping patterns,
and reported no occurrence of hallucinations or seizures.
On examination, the patient was afebrile with normal
vital signs. However, the patient was unable to answer simple
questions and this was associated with intermittent confusion and
agitation. There was no other evidence of any focal or global
neurological deficit. The results of the patient analyses,
including an MRI brain scan and a routine electroencephalography
(EEG), were all normal. A lumbar puncture was performed to
determine CSF biochemistry, cytology and microbiology. The CSF
revealed an elevated white blood cell count of 25
cells/mm3. The CSF pressure, and the levels of protein
and glucose were within normal range; the bacterial culture was
negative. The patient was hospitalized, empiric treatment for viral
encephalitis was initiated and acyclovir was administered
intravenously.
A week following admission, the patient’s symptoms
deteriorated. The patient was confused and became agitated more
frequently; aggressive behavior towards family members also
developed. The interaction with the surroundings was greatly
reduced and occasionally the patient remained mute. There were
signs of catatonia, including whole body rigidity and psychological
pillow. Insomnia was apparent and the period spent sleeping
decreased to 4 h/day. The patient also presented disturbances of
the movement system, which included intermittent, involuntary
movements of the facial muscles and tongue, and choreiform
movements of the extremities. Lip smacking, lip pursing, chewing,
sucking and teeth grinding was demonstrated. Fine muscle twitches
of the right upper extremity were also observed as well as the
paroxysmal upward gazing of the eyes without evident convulsion or
jerking. The patient lost control of bladder and bowel movement and
autoimmune encephalitis was highly suspected at this stage.
Repeated brain MRI scans enhanced with gadolinium,
fluid-attenuated inversion recovery (FLAIR) and diffusion-weighted
imaging (DWI) all appeared normal. The CSF was analyzed again;
however, CSF biochemistry, cytology and microbiology were all
within normal range. A CSF and serum anti-NMDAR antibody study was
requested. Chest X-ray, computed tomography (CT) and abdominal
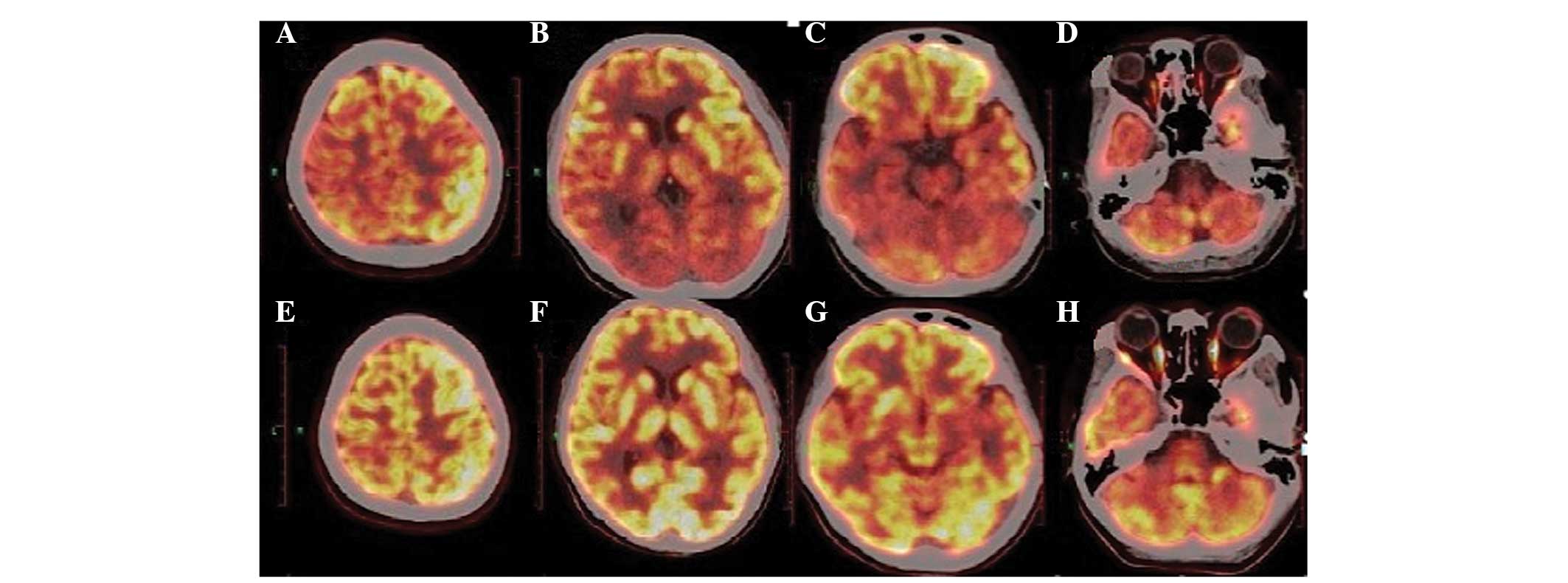
ultrasound scans were unremarkable. The 18F-FDG PET
whole body scan revealed no tumorous focus. However, the
18F-FDG PET brain scan demonstrated hypometabolism in
the bilateral occipital cortex, parietal cortex, thalamus, right
temporal cortex and left cerebellum (Fig. 1). A routine EEG taken immediately
prior to the 18F-FDG PET scan revealed generalized slow
waves with asymmetry in frequency and amplitude. Treatment with a
large dose of intravenously administered methylprednisolone (1,000
mg/day) was initiated. However, the patient did not demonstrate any
improvement within five days of treatment and the results of the
serum and CSF anti-NMDAR antibody experiments returned positive.
Plasmapheresis was subsequently attempted and there was marked
improvement in the patient. The patient regained control of bladder
and bowel movements following the first plasmapheresis treatment.
Following three treatments with plasmapheresis, the patient was
well oriented and able to respond to simple questions with a Mini
Mental State Examination (MMSE) score of 10. Following five courses
of plasmapheresis, the patient demonstrated significant recovery
with a MMSE score of 24. A follow-up 18F-FDG PET scan
revealed that glucose metabolism had returned to normal (Fig. 1). Routine EEG immediately prior to
the 18F-FDG PET scan also demonstrated great
improvement; α-like activity reappeared in the occipital area and
the asymmetry of frequency and amplitude, as observed in previous
EEG tests, had disappeared.
Discussion
Anti-NMDAR encephalitis first was identified in 2007
by Dalmau et al (1), as
treatment-responsive paraneoplastic encephalitis. Since then,
>600 cases of anti-NMDAR encephalitis have been reported. Due to
the acute or subacute onset of the disease, overlap of the stages
and clinical symptoms and signs are extremely common. CSF
biochemistry, cytology and microbiology examinations are either
nonspecific or unremarkable. The MRI brain scan is unremarkable in
50% of cases, with the remainder demonstrating non-specific
changes. EEG may reveal non-specific slowing, disorganized activity
or epileptiform discharge. The diagnosis of anti-NMDAR encephalitis
is highly reliant on clinical awareness and anti-NMDAR antibody
detection in the CSF and serum.
Although the number of published studies on
anti-NMDAR encephalitis has increased markedly since its discovery,
only a few more recent studies have described the application of
18F-FDG PET in the evaluation of anti-NMDAR encephalitis
(6–10). Leypoldt et al (6) revealed a characteristic change in
cerebral glucose metabolism during NMDAR-antibody encephalitis of
an increased frontotemporal-to-occipital gradient; however, no
specific pattern of FDG PET imaging could be identified in the
majority of cases (7–10). The majority of cases demonstrated
various degrees of hyper- or hypometabolism of a particular area of
the brain, which was associated with different stages of the
disease and the different structures involved at each stage.
Certain cases that underwent follow-up FDG PET imaging following
treatment revealed an association between FDG PET imaging and
clinical recovery of the patient. Greiner et al (7) reported the case of an 11-year-old
female with a novel onset of explosive epilepsy. 18F-FDG
imaging at 24 days following the onset of seizure revealed
asymmetric hypermetabolism in the superior right frontal lobe.
Maqbool et al (8) described
a case of anti-NMDAR encephalitis where on day 26 following
admission, 18F-FDG PET imaging demonstrated global
hypometabolism and the presence of a prominent focally intense
hypermetabolic lesion in the right cerebellar cortex. Clinical
signs of improvement were observed following two courses of
intravenous immunoglobulin therapy. A repeat brain FDG-PET scan on
day 46 revealed an overall improvement, with focal hypometabolism
in the right cerebellar cortex. Similar results were observed in
the study by Pillai et al in 2010 (9). 18F-FDG PET images of two
cases, which were taken in the sixth week and fifth month,
respectively, following the onset of disease, demonstrated diffuse
cerebral hypometabolism, including in the bilateral frontal,
parietal, temporal and occipital lobe and thalamus areas.
In the present study, the 18F-FDG PET
images of the patient revealed a general reduction in metabolism in
the bilateral frontal, temporal and occipital lobes, thalamus and
left cerebellum, without an apparent zone of hypermetabolism. The
decreasing levels of metabolism in the left and right hemisphere
were asymmetrical, particularly in the temporal and parietal
cortex. An EEG study carried out immediately prior to the
18F-FDG PET imaging also revealed generalized Δ-θ
slowing with significant frequency and amplitude asymmetry.
Following successful treatment with a high dose of corticosteroids
and subsequently, with five courses of therapeutic plasmapheresis
over two weeks, the current patient improved significantly. A
follow-up 18F-FDG PET image in the seventh week
indicated that the metabolic activity of the cerebral and
cerebellum had returned to normal. Furthermore a follow-up EEG also
revealed great improvement. According to cases analyzed in previous
studies and the case reported in the current study (6,8), the
present authors hypothesize that the changes in the metabolism of
the cerebrum and cerebellum are reversible in anti-NMDAR
encephalitis. Furthermore, if MRI scans are negative,
18F-FDG PET imaging offers maximal efficacy for early
diagnosis and the evaluation of prognosis for anti-NMDAR
encephalitis.
Although no standard of treatment exists for
anti-NMDAR encephalitis, eradication of the associated malignancy
and immunotherapy is recommended. The immunotherapies include
corticosteroids, intravenous immunoglobulin (IVIG), plasmapheresis,
rituximab, cyclophosphamide and azathioprine, with corticosteroids,
IVIG or plasmapheresis constituting the primary approach (11,12).
However, systematic comparisons between the three first-line
modalities are not yet available (12). If the primary therapies are
ineffective, rituximab or cyclophosphamide may be considered as the
second-line therapies. For patients without a malignancy,
first-line therapy may not be effective. Therefore, second-line
immunotherapy is usually required. In the present case study, the
patient achieved considerable improvements following plasmapheresis
initiated in the fourth week, following no effect from steroid
treatment. This was consistent with a study by Pham et al
(13) in which nine cases of
anti-NMDA-R encephalitis were reviewed and two acquired the best
recovery by undergoing plasmapheresis treatment. Thus, the authors
of the current study continue to postulate that early
plasmapheresis treatment may lead to beneficial treatment
results.
In conclusion, 18F-FDG PET imaging is
greatly advantageous in the treatment of anti-NMDAR encephalitis.
The current study presented a special change in PET images during
the overall process of the therapy, which has not been observed in
previous case studies. However, it should be noted that the present
study only analyzed one patient who was treated using
plasmapheresis in combination with 18F-FDG PET. Further
clinical investigations and studies of PET application in the
treatment of anti-NMDAR encephalitis are required to confirm the
results. Furthermore, when the therapeutic effect of steroid
treatment is poor, early plasmapheresis helps to improve the
prognosis of anti-NMDAR encephalitis.
Acknowledgements
The authors are deeply grateful to Professor
Xiangjun Chen of the Department of Neurology at Huashan Hospital
(University of Fudan, Shanghai, China), for assisting in the
measurement of the levels of NMDAR antibodies.
References
|
1
|
Dalmau J, Tüzün E, Wu HY, et al:
Paraneoplastic anti-N-methyl-D-aspartate receptor encephalitis
associated with ovarian teratoma. Ann Neurol. 61:25–36. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Graus F and Dalmau J: Paraneoplastic
neurological syndromes: diagnosis and treatment. Curr Opin Neurol.
20:732–737. 2007.PubMed/NCBI
|
|
3
|
Irani SR, Bera K, Waters P, et al:
N-methyl-D-aspartate antibody encephalitis: temporal progression of
clinical and paraclinical observations in a predominantly
non-paraneoplastic disorder of both sexes. Brain. 133:1655–1667.
2010. View Article : Google Scholar
|
|
4
|
Vincent A and Bien CG: Anti-NMDA-receptor
encephalitis: a cause of psychiatric, seizure, and movement
disorders in young adults. Lancet Neurol. 7:1074–1075. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Florance NR, Davis RL, Lam C, et al:
Anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis in children
and adolescents. Ann Neuro1. 66:11–18. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Leypoldt F, Buchert R, Kleiter I, et al:
Fluorodeoxyglucose positron emission tomography in
anti-N-methyl-D-aspartate receptor encephalitis: distinct pattern
of disease. J Neurol Neurosurg Psychiatry. 83:681–686. 2012.
View Article : Google Scholar
|
|
7
|
Greiner H, Leach JL, Lee KH and Krueger
DA: Anti-NMDA receptor encephalitis presenting with imaging
findings and clinical features mimicking Rasmussen syndrome.
Seizure. 20:266–270. 2011. View Article : Google Scholar
|
|
8
|
Maqbool M, Oleske DA, Huq AH, Salman BA,
Khodabakhsh K and Chugani HT: Novel FDG-PET findings in anti-NMDA
receptor encephalitis: a case based report. J Child Neurol.
26:1325–1328. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Pillai SC, Gill D, Webster R, Howman-Giles
R and Dale RC: Cortical hypometabolism demonstrated by PET in
relapsing NMDA receptor encephalitis. Pediatr Neurol. 43:217–220.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Baumgartner A, Rauer S, Mader I and Meyer
PT: Cerebral FDG-PET and MRI findings in autoimmune limbic
encephalitis: correlation with autoantibody types. J Neurol.
260:2744–2753. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Dalmau J, Lancaster E, Martinez-Hernandez
E, Rosenfeld MR and Balice-Gordon R: Clinical experience and
laboratory investigations in patients with anti-NMDAR encephalitis.
Lancet Neuro1. 10:63–74. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Titulaer MJ, McCracken L, Gabilondo I, et
al: Treatment and prognostic factors for long-term outcome in
patients with anti-NMDA receptor encephalitis: an observational
cohort study. Lancet Neurol. 12:157–165. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Pham HP, Daniel-Johnson JA, Stotler BA,
Stephens H and Schwartz J: Therapeutic plasma exchange for the
treatment of anti-NMDA receptor encephalitis. J Clin Apher.
26:320–325. 2011. View Article : Google Scholar : PubMed/NCBI
|