Introduction
The incidence rate of septic arthritis (SA) has been
increasing over the last few years. Early diagnosis as well as a
prompt and effective treatment are vital in order to avoid severe
outcomes (1). However, the
clinical manifestation of SA is similar to that of non-septic
arthritis, including rheumatoid arthritis (RA), osteoarthritis (OA)
and gouty arthritis (GA), which causes difficulty in the
differentiation of SA from RA, OA and GA in clinics. Currently, the
detection of bacteria in synovial fluid culture remains the primary
index for the diagnosis of SA. However, this has a number of
disadvantages including aseptic surgery, a long turn-around time
and the potential generation of a false positive or negative result
(2,3). Prior to the bacterial culture results
becoming available, several other clinical tests, including X-ray
imaging (4), routine blood tests
(5), erythrocyte sedimentation
rate (ESR) measurements (6),
synovial fluid white blood cell (WBC) count (7) and levels of CRP (C reactive protein)
(8,9) may be used for SA diagnosis. However,
none of these tests are sensitive enough to produce an accurate
diagnosis and they frequently lead to misdiagnosis and/or the delay
of treatment. For example, CRP is another positive predicator in
the diagnosis of SA (10–14); however, the diagnostic accuracy of
CRP is affected by steroids (15).
A quick and sensitive test is thus required.
Procalcitonin (PCT), a precursor of the calcitonin
peptide produced due to bacterial endotoxins, tumor necrosis factor
(TNF)-α and interleukin (IL)-6 (16,17),
is a novel predictor for the diagnosis of bacterial infection
(18,19). As a secondary inflammatory factor,
PCT is not directly involved in initiating the septic process but
may enlarge and aggravate the pathological process of sepsis
(20) and is unresponsive or only
mildly reactive to aseptic inflammation and viral infection
(21). PCT has been used in the
diagnosis of systemic infections or infectious shock (22–27).
Unlike CRP, the diagnostic accuracy of PCT is not affected by
steroids (28). A previous
meta-analysis demonstrated that PCT was more accurate than CRP in
diagnosing systemic bacterial infection, regardless of pathogen
type (29). Despite the widespread
use of PCT in the diagnosis of numerous systemic infectious
diseases, including sepsis and pneumonia (30–33),
the use of PCT in the diagnosis of SA, RA, OA and GA remains
limited. Serum levels of PCT perform better than synovial fluid
levels of PCT in the diagnosis of SA (34). However, PCT levels among
non-infectious types of arthritis (OA, RA and GA) have not, to the
best of our knowledge, been compared, although the level of PCT in
SA has been compared with that of non-inflammatory arthritis in the
current study. The synovial fluid levels of PCT have been reported
to be positive indicators of SA (35). A previous study has demonstrated
that the synovial fluid level of PCT is significantly higher in
patients with SA than in patients with OA, and that CRP levels
differ significantly among patients with SA, RA and OA (36). The serum level of PCT is a specific
marker of SA but with a low sensitivity; serum PCT in association
with CRP has not been useful for the diagnosis of SA (37).
Thus, the applicability of using the levels of PCT
in the serum or synovial fluid as effective indicators for
distinguishing SA from non-infectious forms of arthritis remains
controversial. A study involving patients with SA, RA, OA and GA
would be instrumental in resolving the controversy. The discrepancy
in the effectiveness of applying serum or synovial fluid PCT in
diagnosis may result from the condition of the serum or synovial
fluid samples. The specimens in certain previous studies (34–37)
were frozen for longer than 24 h prior to the experiments being
conducted while the half-life of PCT in the synovial fluid has been
reported to be ~20–24 h (38). The
present study aimed to evaluate whether serum or joint fluid levels
of PCT may be used in the differential diagnosis of SA from RA, OA
and GA using fresh serum and synovial fluid samples.
Materials and methods
Patients
A non-blind method was used for selection of
participants in the present study and subjects volunteered to
become study subjects. All subjects were selected from the
outpatient service of Xiangya Hospital of Central South University
(Changsha, China) from January 2012 to June 2013. The patients were
selected according to the following criteria: i) Patients with
various types of arthritis other than SA, RA, OA or GA were
excluded from the present study. Diagnosis was carried out
according to the criteria set by the American College of
Rheumatology (ACR) and confirmed by bacterial culture of the
patients’ synovial fluid. ii) The patients had not received any
antibiotic or joint puncture treatments prior to enrollment in the
current study. iii) Patients were excluded if the joint(s) being
treated had been subjected to artificial joint surgery. iv) All
patients included in the present study had been evaluated using the
joint fluid bacterial culture test. Patients with SA were excluded
if the result of their bacterial culture test was negative; RA, OA
and GA patients were excluded if the result of their bacterial
culture test was positive. v) Each patient provided informed
written consent and approval from the Institutional Review Board
(IRB) of the Xiangya Hospital was obtained prior to data extraction
and analysis.
Collection of specimens
A total of 5 ml blood was drawn from a vein at the
elbow of each patient followed by centrifugation at 2,756 × g for
10 min. A synovial fluid sample ≥200 μl in volume was aseptically
aspirated from the patellofemoral articular surface. Patients from
which <200 μl synovial fluid was collected were excluded from
the study. If the two knees of a patient exhibited symptoms of SA,
RA, OA or GA, synovial fluid was only drawn from the knee with the
more severe symptoms. All samples were stored at room temperature
(10–25°C) prior to analysis.
Determination of the levels of PCT in the
serum and synovial fluid
Levels of PCT were tested within 24 h after serum
and fluid collection at room temperature (10–25°C) by enzyme linked
fluorescent analysis (ELFA) using a PCT quantitative determination
kit and fluorescence reading machine (Vidas® B.R.A.H.M.S
PCT™; bioMérieux, Marcy l’Etoile, France) according to the
manufacturers’ instructions.
Statistical analysis
All statistical analyses were performed using SPSS
software, version 19.0 (SPSS, Inc., Chicago, IL, USA), unless
otherwise specified. P<0.01 was considered to indicate a
statistically significant difference. Correlations of the serum and
synovial fluid levels of PCT between groups were determined by the
Nemenyi test. Areas under the receiver operating characteristic
(ROC) curve were calculated to evaluate the accuracy of the
correlations.
Results
Patient characteristics
A total of 95 patients were enrolled in the current
study. Of these, 23, 21, 40 and 11 patients had SA, RA, OA and GA,
respectively. The corresponding male/female ratios were 15/8, 6/15,
19/21 and 10/1, respectively, and the corresponding average ages
were 46.6±3.6, 35.0±2.2, 66.2±2.6 and 60.8±5.6 years, respectively
(Table I). The types and number of
pathogenic bacteria of SA are also listed in the table.
 | Table ICharacteristics of the SA, RA, OA and
GA groups. |
Table I
Characteristics of the SA, RA, OA and
GA groups.
| Characteristic | SA | RA | OA | GA |
|---|
| Number of cases | 23 | 21 | 40 | 11 |
| Male/female (n) | 15/8 | 6/15 | 19/21 | 10/1 |
| Average age
(years) | 46.6±3.6 | 35.0±2.2 | 66.2±2.6 | 60.8±5.6 |
| Types and numbers of
pathogenic bacteria |
| Staphylococcus
aureus | 12 | 0 | 0 | 0 |
| Hemolytic
Streptococcus | 5 | 0 | 0 | 0 |
| Tubercle
bacillus | 2 | 0 | 0 | 0 |
| Escherichia
coli | 2 | 0 | 0 | 0 |
| Streptococcus
pneumoniae | 2 | 0 | 0 | 0 |
Levels of PCT in the serum and synovial
fluid
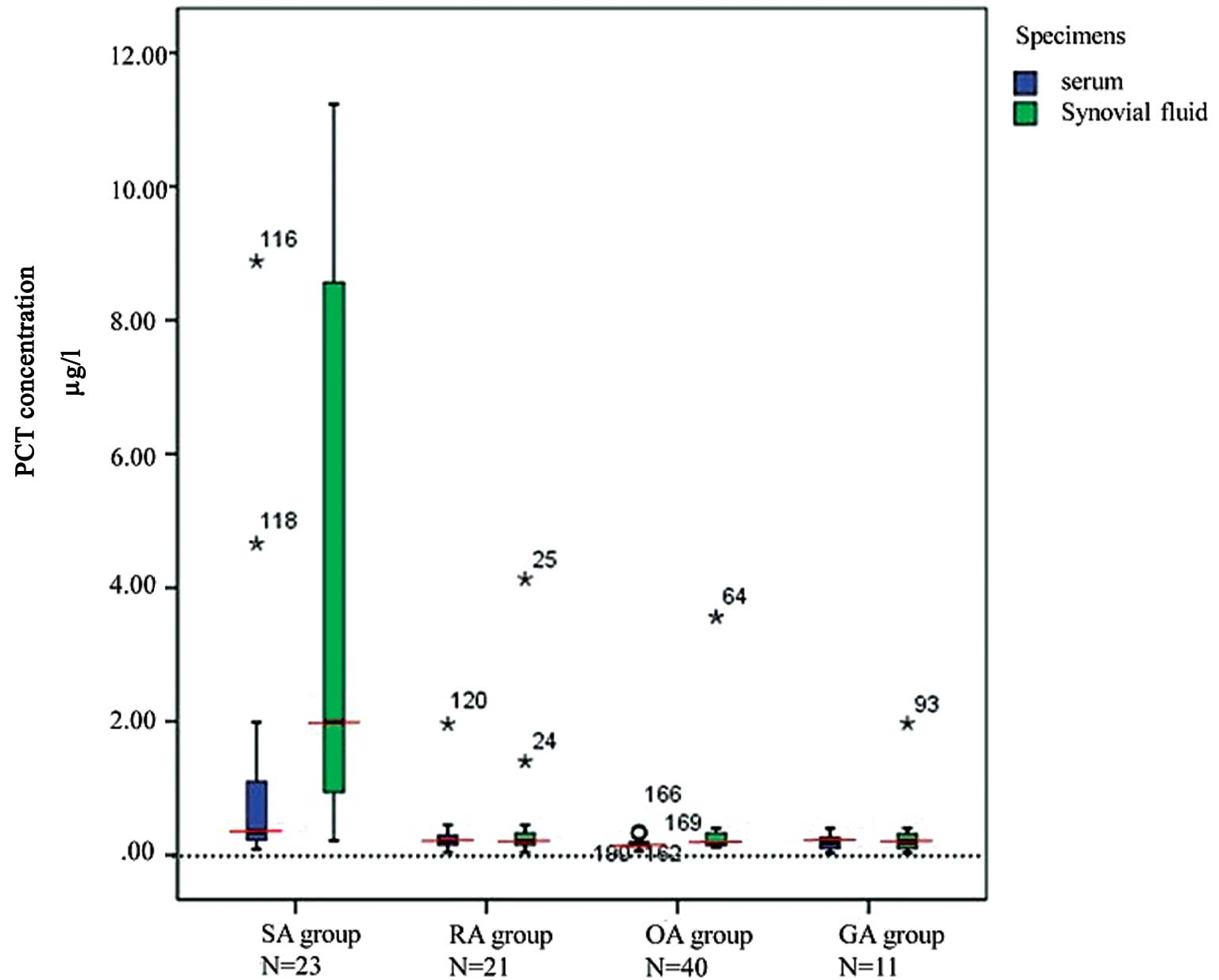
The levels of PCT in the serum and synovial fluid in
the SA group were significantly higher compared with those in the
other three groups (P<0.01). No significant differences in the
levels of PCT in the serum or synovial fluid were observed among
the RA, OA and GA groups (P>0.01; Fig. 1).
Correlation between the levels of PCT in
the serum and synovial fluid and SA, RA, OA and GA
The majority of the serum levels of PCT in the four
groups (SA, 65.2%; RA, 100%; OA, 97.5% and GA, 100%) were <0.5
μg/l. Serum levels of PCT in ~34.8% of patients with SA were in the
range 0.5–10.0 μg/l. The levels of PCT in the synovial fluid in the
majority of patients in the RA, OA and GA groups were <0.5 μg/l
(RA, 95.2%; OA, 95.0% and GA, 90.9%). The levels of PCT in the
synovial fluid of 39.1% and 30.4% of patients in the SA group were
0.5–2 μg/l and 2–10 μg/l, respectively (Table II).
| Table IISerum and synovial fluid levels of PCT
in the knees of patients with SA, RA, OA and GA. |
Table II
Serum and synovial fluid levels of PCT
in the knees of patients with SA, RA, OA and GA.
| SA (n=23) | RA (n=21) | OA (n=40) | GA (n=11) | | |
|---|
|
|
|
|
| | |
|---|
| PCT (μg/l) | Cases | % | Cases | % | Cases | % | Cases | % | χ2 | P-value |
|---|
| Serum |
| <0.5 | 15 | 65.21 | 21 | 100.0 | 39 | 97.50 | 11 | 100.00 | 23.002 | 0.001 |
| 0.5–2.0 | 6 | 26.09 | 0 | 0.00 | 1 | 2.50 | 0 | 0.00 | | |
| 2.0–10.0 | 2 | 8.70 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | | |
| >10.0 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | | |
| Total | 23 | 100.00 | 21 | 100.00 | 40 | 100.00 | 11 | 100.00 | | |
| Synovial fluid |
| <0.5 | 3 | 13.04 | 20 | 95.24 | 38 | 95.00 | 10 | 90.90 | 62.669 | <0.001 |
| 0.5–2.0 | 9 | 39.14 | 0 | 0.00 | 1 | 2.50 | 1 | 9.10 | | |
| 2.0–10.0 | 7 | 30.43 | 1 | 4.76 | 1 | 2.50 | 0 | 0.00 | | |
| >10.0 | 4 | 17.39 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | | |
| Total | 23 | 100.00 | 21 | 100.00 | 40 | 100.00 | 11 | 100.00 | | |
To differentiate SA from the forms of non-infectious
arthritis, serum and synovial fluid levels of PCT <0.5 μg/l had
great specificity, positive predictive value (PPV) and a negative
predictive value (NPV). Synovial fluid levels of PCT <0.5 μg/l
had significantly higher sensitivity compared with serum levels of
PCT. Serum and synovial fluid levels of PCT at 2 or 10 μg/l
revealed great specificity but low sensitivity (Table III).
| Table IIISensitivity, specificity, PPV and PNV
of the serum and joint fluid levels of PCT in the differential
diagnosis of septic arthritis from rheumatoid arthritis,
osteoarthritis and gouty arthritis. |
Table III
Sensitivity, specificity, PPV and PNV
of the serum and joint fluid levels of PCT in the differential
diagnosis of septic arthritis from rheumatoid arthritis,
osteoarthritis and gouty arthritis.
| Serum PCT | Synovial fluid
PCT |
|---|
|
|
|
|---|
| PCT (μg/l) | Sensitivity
(%) | Specificity
(%) | PPV(%) | NPV(%) | Sensitivity
(%) | Specificity
(%) | PPV(%) | NPV(%) |
|---|
| 0.5 | 34.79 | 98.61 | 88.89 | 82.56 | 86.96 | 94.44 | 83.33 | 95.77 |
| 2.0 | 8.70 | 100.00 | 100.00 | 77.42 | 47.83 | 97.22 | 84.62 | 85.37 |
| 10.0 | 0.00 | 100.00 | - | 75.79 | 17.39 | 100.00 | 100.0 | 79.12 |
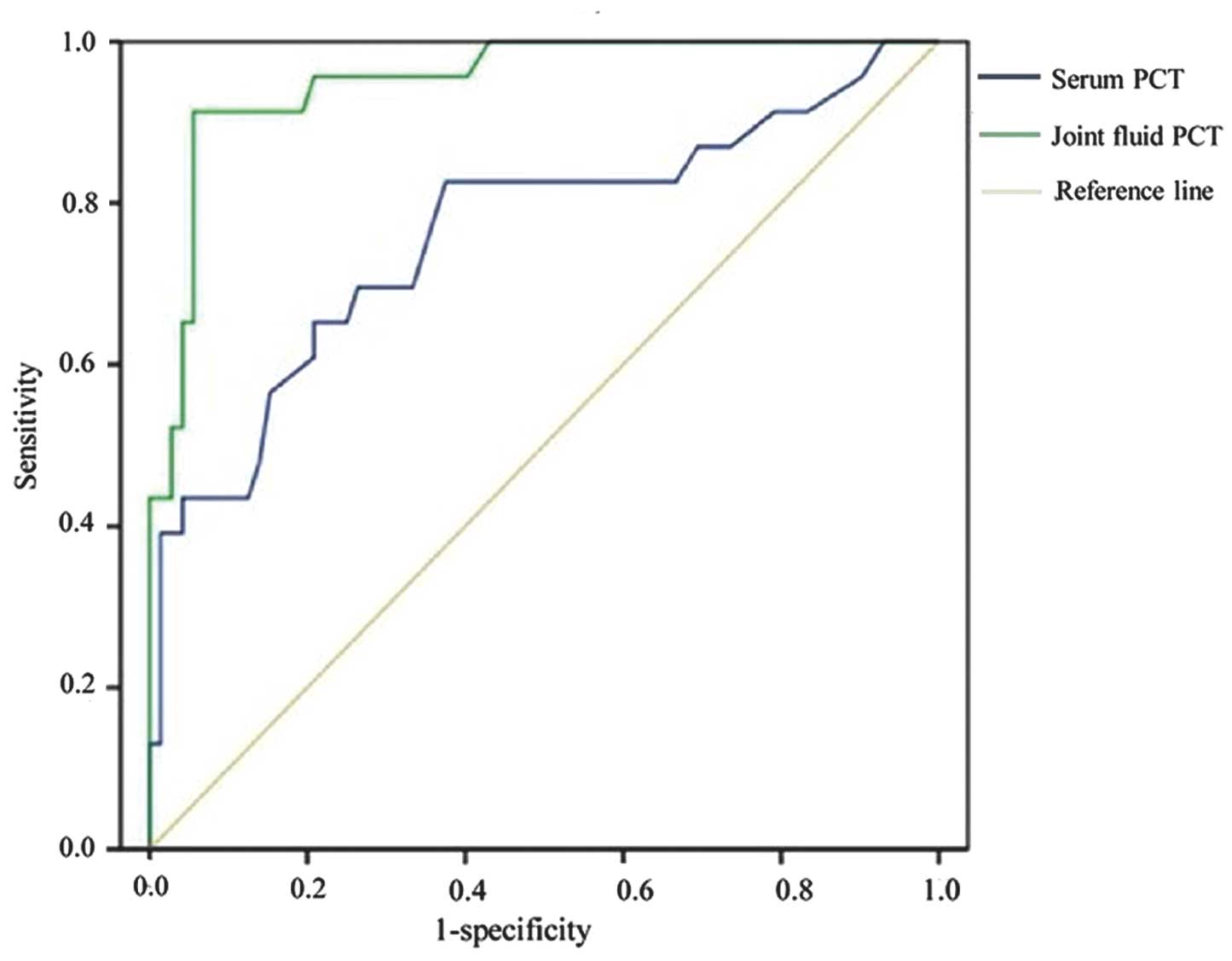
Accuracy of serum and synovial fluid PCT
in discriminating SA from RA, OA and GA
The areas under the ROC curve of the serum and
synovial fluid levels of PCT were calculated and the accuracy of
serum and synovial fluid PCT in discriminating SA from RA, OA and
GA was determined. The area under the ROC curve of the serum levels
of PCT was 0.761 and the area under ROC curve of the synovial fluid
levels of PCT was 0.951 (Fig. 2
and Table IV). The accuracy of
serum PCT was significantly lower compared with that of synovial
fluid PCT in discriminating SA from RA, OA and GA (P<0.01).
| Table IVAccuracy analysis of the serum and
synovial fluid levels of PCT in the differential diagnosis of knee
septic arthritis from rheumatoid arthritis, osteoarthritis and
gouty arthritis. |
Table IV
Accuracy analysis of the serum and
synovial fluid levels of PCT in the differential diagnosis of knee
septic arthritis from rheumatoid arthritis, osteoarthritis and
gouty arthritis.
| | | Asymptotic 95%
confidence interval | |
|---|
| | |
| |
|---|
| Test variables | Area | Standard error | Lower limit | Upper limit | Accuracy
analysis |
|---|
| Serum PCT | 0.761 | 0.064 | 0.635 | 0.887 | Low to
moderate |
| Joint fluid
PCT | 0.951 | 0.023 | 0.905 | 0.996 | Higher |
Discussion
To investigate whether serum and/or joint fluid PCT
can be used in distinguishing SA from RA, OA and GA, the levels of
PCT in fresh serum and synovial fluid samples of patients diagnosed
with SA, RA, OA or GA were measured. The present study demonstrated
that the levels of PCT in the serum and synovial fluid samples from
patients in the SA group were significantly higher compared with
those in the RA, OA, or GA groups. Levels of PCT in the serum and
synovial fluid <0.5 μg/l had high specificity in the
differential diagnosis of SA from RA, OA and GA. The accuracy of
the differential diagnosis of SA from RA, OA and GA using serum PCT
was significantly lower compared with that by synovial fluid
PCT.
To the best of our knowledge, the present study is
the first to simultaneously examine all three non-infectious forms
of arthritis (RA, OA and GA) using serum and synovial fluid not
stored under frozen conditions for >24 h. The levels of PCT in
the two types of sample were compared among the four groups using
the Nemenyi method. The results revealed that the levels of PCT in
the serum and synovial fluid of patients with SA were significantly
higher compared with those in the patients in the other three
groups. No significant difference was observed in the levels of PCT
among the RA, OA and GA groups. A PCT level in the two specimens of
<0.5 μg/l had high specificity, PPV and NPV for the differential
diagnosis of SA from RA, OA and GA; however, the synovial fluid
levels of PCT <0.5 μg/l had significantly higher sensitivity
than those of PCT in the serum at the same level. The results of
the present study are in accordance with certain previous studies
in which synovial levels of PCT were revealed to be positive
indicators of SA (35) and were
able to differentiate SA from OA (36). Serum PCT has previously been
reported as a specific marker of SA but with low sensitivity and
was considered not to be useful for the diagnosis of SA, even in
association with CRP (37).
Nevertheless, serum PCT has been reported to have an improved
performance compared with synovial fluid PCT in the diagnosis of SA
(35) and serum levels of PCT ≥0.3
μg/l have been revealed to have a specificity of 98% in the
differential diagnosis of SA infection from prosthetic joint
infection and a sensitivity of <35% (38–40)
Using ROC curve analysis, the present study
demonstrated that the accuracy of the differential diagnosis of SA
from the three types of non-infectious arthritis using synovial
fluid levels of PCT was significantly higher compared with using
the levels of PCT in the serum. This may be attributed to the fact
that joint SA, RA, OA and GA do not cause systemic inflammation;
therefore, serum levels of PCT are unable to differentiate SA from
RA, OA and/or GA. Certain studies have demonstrated that low levels
of PCT may result from limited inflammation or early infection
(41,42). Other studies have revealed that the
lack of a systemic inflammatory response causes the sensitivity of
serum PCT in the differential diagnosis of infectious prosthesis to
be extremely low (38–40).
In conclusion, the sensitivity and accuracy of
synovial joint fluid PCT at certain levels was significantly higher
than that of the serum levels of PCT. Therefore, the level of
synovial fluid PCT may be used as an alternative indicator in the
differential diagnosis of SA from RA, OA and GA, which may be
valuable in guiding the use of antibiotics to SA. However, further
studies with a larger patient sample size are required to validate
this result. Further work is required to determine the optimal
serum and synovial fluid levels of PCT for the differential
diagnosis of SA from non-infectious arthritis.
References
|
1
|
Favero M, Schiavon F, Riato L, Carraro V
and Punzi L: Septic arthritis: a 12 years retrospective study in a
rheumatological university clinic. Reumatismo. 60:260–267. 2008.(In
Italian).
|
|
2
|
Ma L, Cranney A and Holroyd-Leduc JM:
Acute monoarthritis: what is the cause of my patient’s painful
swollen joint? CMAJ. 180:59–65. 2009.PubMed/NCBI
|
|
3
|
Margaretten ME, Kohlwes J, Moore D and
Bent S: Does this adult patient have septic arthritis? JAMA.
297:1478–1488. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Mathews CJ, Kingsley G, Field M, et al:
Management of septic arthritis: a systematic review. Postgrad Med
J. 84:265–270. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Schiavon F, Favero M, Carraro V and Riato
L: Septic arthritis: what is the role for the rheumatologist?
Reumatismo. 60:1–5. 2008.(In Italian).
|
|
6
|
Buess T and Ludwig C: Diagnostic value of
C-reactive protein in comparison with erythrocyte sedimentation as
routine admission diagnostic test. Schweiz Med Wochenschr.
125:120–124. 1995.(In German).
|
|
7
|
McGillicuddy DC, Shah KH, Friedberg RP,
Nathanson LA and Edlow JA: How sensitive is the synovial fluid
white blood cell count in diagnosing septic arthritis? Am J Emerg
Med. 25:749–752. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Saeed K, Ahmad N, Pallett A, Guiver M and
Marsh P: Specific staphylococcal polymerase chain reaction can be a
complementary tool for identifying causative organisms and guiding
antibiotic management in orthopaedic infections. Curr Ortho Pract.
21:628–631. 2010. View Article : Google Scholar
|
|
9
|
Yang S, Ramachandran P, Hardick A, et al:
Rapid PCR-based diagnosis of septic arthritis by early Gram-type
classification and pathogen identification. J Clin Microbiol.
46:1386–1390. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Caird MS, Flynn JM, Leung YL, Millman JE,
D’Italia JG and Dormans JP: Factors distinguishing septic arthritis
from transient synovitis of the hip in children. A prospective
study. J Bone Joint Surg Am. 88:1251–1257. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Khachatourians AG, Patzakis MJ, Roidis N
and Holtom PD: Laboratory monitoring in pediatric acute
osteomyelitis and septic arthritis. Clin Orthop Relat Res. 186–194.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lorrot M, Fitoussi F, Faye A, et al:
Laboratory studies in pediatric bone and joint infections. Arch
Pediatr. 14(Suppl 2): S86–S90. 2007.(In French).
|
|
13
|
Gupta MN, Sturrock RD and Field M: A
prospective 2-year study of 75 patients with adult-onset septic
arthritis. Rheumatology (Oxford). 40:24–30. 2001.PubMed/NCBI
|
|
14
|
Levine MJ, McGuire KJ, McGowan KL and
Flynn JM: Assessment of the test characteristics of C-reactive
protein for septic arthritis in children. J Pediatr Orthop.
23:373–377. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Monneret G, Labaune JM, Isaac C, Bienvenu
F, Putet G and Bienvenu J: Procalcitonin and C-reactive protein
levels in neonatal infections. Acta Paediatr. 86:209–212. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Altunhan H, Annagür A, Örs R and
Mehmetoğlu I: Procalcitonin measurement at 24 hours of age may be
helpful in the prompt diagnosis of early-onset neonatal sepsis. Int
J Infect Dis. 15:e854–e858. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Reith HB, Mittelkötter U, Debus ES,
Küssner C and Thiede A: Procalcitonin in early detection of
postoperative complications. Dig Surg. 15:260–265. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Caliskan B, Guven A, Ozler M, et al: Ozone
therapy prevents renal inflammation and fibrosis in a rat model of
acute pyelonephritis. Scand J Clin Lab Invest. 71:473–480. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wacker C, Prkno A, Brunkhorst FM and
Schlattmann P: Procalcitonin as a diagnostic marker for sepsis: a
systematic review and meta-analysis. Lancet Infect Dis. 13:426–435.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bohuon C: Inflammatory cascade response to
toxin release: therapeutic perspectives. Ann Pharm Fr. 59:191–197.
2001.(In French).
|
|
21
|
Balog A, Ocsovszki I and Mándi Y: Flow
cytometric analysis of procalcitonin expression in human monocytes
and granulocytes. Immunol Lett. 84:199–203. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Das RR: Should procalcitonin be used as a
routine biomarker of bacterial infection? Infection. 40:713–714.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Giamarellos-Bourboulis EJ, Mega A, Grecka
P, et al: Procalcitonin: a marker to clearly differentiate systemic
inflammatory response syndrome and sepsis in the critically ill
patient? Intensive Care Med. 28:1351–1356. 2002. View Article : Google Scholar
|
|
24
|
Chalupa P, Beran O, Herwald H, Kaspříková
N and Holub M: Evaluation of potential biomarkers for the
discrimination of bacterial and viral infections. Infection.
39:411–417. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lipinska-Gediga M, Mierzchala M and Durek
G: Pro-atrial natriuretic peptide (pro-ANP) level in patients with
severe sepsis and septic shock: prognostic and diagnostic
significance. Infection. 40:303–309. 2012. View Article : Google Scholar
|
|
26
|
Stankovic Stojanovic K, Steichen O,
Lionnet F, et al: Is procalcitonin a marker of invasive bacterial
infection in acute sickle-cell vaso-occlusive crisis? Infection.
39:41–45. 2011.PubMed/NCBI
|
|
27
|
Saeed K, Dryden M, Bourne S, Paget C and
Proud A: Reduction in antibiotic use through procalcitonin testing
in patients in the medical admission unit or intensive care unit
with suspicion of infection. J Hosp Infect. 78:289–292. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Christ-Crain M and Müller B: Procalcitonin
in bacterial infections - hype, hope, more or less? Swiss Med Wkly.
135:451–460. 2005.PubMed/NCBI
|
|
29
|
Simon L, Gauvin F, Amre DK, Saint-Louis P
and Lacroix J: Serum procalcitonin and C-reactive protein levels as
markers of bacterial infection: a systematic review and
meta-analysis. Clin Infect Dis. 39:206–217. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Assicot M, Gendrel D, Carsin H, Raymond J,
Guilbaud J and Bohuon C: High serum procalcitonin concentrations in
patients with sepsis and infection. Lancet. 341:515–518. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Martinez JM, Wagner KE, Snider RH, et al:
Late immunoneutralization of procalcitonin arrests the progression
of lethal porcine sepsis. Surg Infect (Larchmt). 2:193–202. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Sener G, Ozgur E, Rad AY, Uzun L, Say R
and Denizli A: Rapid real-time detection of procalcitonin using a
microcontact imprinted surface plasmon resonance biosensor.
Analyst. 138:6422–6428. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
van Vugt SF, Broekhuizen BD, Lammens C, et
al: GRACE consortium: Use of serum C reactive protein and
procalcitonin concentrations in addition to symptoms and signs to
predict pneumonia in patients presenting to primary care with acute
cough: diagnostic study. BMJ. 346:f24502013.
|
|
34
|
Talebi-Taher M, Shirani F, Nikanjam N and
Shekarabi M: Septic versus inflammatory arthritis: discriminating
the ability of serum inflammatory markers. Rheumatol Int.
33:319–324. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Saeed K, Dryden M, Sitjar A and White G:
Measuring synovial fluid procalcitonin levels in distinguishing
cases of septic arthritis, including prosthetic joints, from other
causes of arthritis and aseptic loosening. Infection. 41:845–849.
2013. View Article : Google Scholar
|
|
36
|
Streit G, Alber D, Toubin MM, Toussirot E
and Wendling D: Procalcitonin, C-reactive protein, and
complement-3a assays in synovial fluid for diagnosing septic
arthritis: preliminary results. Joint Bone Spine. 75:238–239. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Martinot M, Sordet C, Soubrier M, et al:
Diagnostic value of serum and synovial procalcitonin in acute
arthritis: a prospective study of 42 patients. Clin Exp Rheumatol.
23:303–310. 2005.PubMed/NCBI
|
|
38
|
Bottner F, Wegner A, Winkelmann W, Becker
K, Erren M and Götze C: Interleukin-6, procalcitonin and TNF-alpha:
markers of peri-prosthetic infection following total joint
replacement. J Bone Joint Surg Br. 89:94–99. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Randau T, Wimmer M, Kuberra D, et al:
Detection of periprosthetic joint infections: blood infection
markers in patients undergoing revision arthroplasty. Eur Cells
Mater. 21:362011.
|
|
40
|
Worthington T, Dunlop D, Casey A, Lambert
R, Luscombe J and Elliott T: Serum procalcitonin, interleukin-6,
soluble intercellular adhesin molecule-1 and IgG to short-chain
exocellular lipoteichoic acid as predictors of infection in total
joint prosthesis revision. Br J Biomed Sci. 67:71–76. 2010.
|
|
41
|
Butbul-Aviel Y, Koren A, Halevy R and
Sakran W: Procalcitonin as a diagnostic aid in osteomyelitis and
septic arthritis. Pediatr Emerg Care. 21:828–832. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Hügle T, Schuetz P, Mueller B, et al:
Serum procalcitonin for discrimination between septic and
non-septic arthritis. Clin Exp Rheumatol. 26:453–456.
2008.PubMed/NCBI
|