Introduction
With an increasing number of patients receiving
intravascular injections of iodinated contrast media every year
worldwide, contrast-induced nephropathy (CIN) has become the third
leading cause of hospital-acquired acute kidney injury (AKI)
(1). CIN is a serious clinical
problem associated with an increased morbidity and mortality rate,
particularly in high-risk patients who have undergone coronary
angiography and/or percutaneous coronary intervention. A vital step
to lower the number of cases of CIN is to identify patients at risk
and apply proven preventive interventions. A reduction in renal
perfusion and toxic effects on the tubular cells caused by the
direct and indirect effects of contrast media on the kidneys are
generally recognized as important preventive mechanisms.
Furthermore, contrast exposure causes a certain degree of imbalance
between increased renal vasoconstruction and decreased
vasodilatation. This leads to a decrease in renal blood flow and
contraction of the afferent glomerular arteriole, as well as renal
ischemia and cell necrosis (2).
Oxygen radicals released by the ischemia-reperfusion not only
contribute to renal damage but also the apoptosis of the renal
tubular epithelial cells. In the majority of studies, the term CIN
indicates an impairment in renal function, which is defined as an
elevation in the levels of serum creatinine (SCr) following
intravascular administration of the contrast media (3,4).
However, SCr is a relatively inaccurate marker and alterations in
the levels of SCr are not particularly sensitive or specific for
small changes in the estimated glomerular filtration rate (eGFR).
The levels of SCr may also be affected by a number of non-renal
factors including age, ethnicity, muscle metabolism and
nutrition.
A previous study has shown that the activation of
glomerular mesangial cells causes the secretion of interleukin-18
(IL-18), affects the mitosis of the glomerular mesangial cells,
promotes cell proliferation and induces the generation and releases
a series of cytokines, which increases the accumulation of
inflammatory cells within the glomerulus (5). Accumulating evidence indicates that
urinary IL-18 is released in response to injury of the renal
tubules (6,7), and may serve as an early biomarker of
AKI. The present study was designed to investigate whether urinary
IL-18 is an earlier predictive marker than SCr in CIN following
coronary interventional procedures.
Patients and methods
Patient population
The general clinical data of 180 patients who
underwent coronary interventional procedures at the Department of
Cardiology, Affiliated Hospital of Xuzhou Medical College (Xuzhou,
China) from March 1, 2012 to September 31, 2012 were collected in
the study. Among them, 99 were male and 81 were female, with an
average age of 66.5±9.1 years. Exclusion criteria were: i) the use
of drugs with renal toxicity during the preoperative period; ii)
severe hepatic and renal dysfunction, with severe renal dysfunction
defined as eGFR <30 ml/min/1.73 m2; iii) tumors; iv)
New York Heart Association class IV congestive heart failure or
left ventricular ejection fraction (LVEF) <35%; v) thyroid or
adrenal dysfunction; vi) acute or chronic infectious diseases; and
vii) pregnant or breast-feeding females. A nonionic, low osmolality
contrast agent was used in this test. The osmotic concentration was
800 mOsm/kg. All patients were routinely offered antiplatelet,
anticoagulation, antiangina and conventional hydration treatment,
as well as monitoring of lipids, blood pressure and blood
glucose.
The study protocol was in accordance with the
Declaration of Helsinki and was approved by Ethics Committee of the
Affiliated Hospital of Xuzhou Medical College (Xuzhou, China). All
patients provided written informed consent for the procedure.
Laboratory assay
SCr and other biochemical indicators were measured.
Fasting blood specimens were collected prior to and at 24 and 48 h
after the procedure in the biochemical laboratory and subjected to
analysis using an Olympus AU2700 Automatic Biochemistry Analyzer
(Olympus, Center Valley, PA, USA) for determination. Urine
specimens were collected prior to and at 2, 6, 12, 24 and 48 h
after the procedure and immediately centrifuged (1,409 × g, 20 min,
4°C). The supernatant fractions were collected and stored frozen at
−80°C until use. Urinary levels of IL-18 were measured using an
ELISA kit purchased from R&D Systems (Minneapolis, MN, USA).
All procedures were performed strictly following the manufacturer’s
instructions. Renal function was assessed by the eGFR using the
Modification of Diet in Renal Disease formula for Chinese patients
(8): GFR (ml/min/1.73
m2) = 175 × SCr (mg/dl)−1.1549 ×
age−0.2039 (x 0.79 if female). This equation gives a
more accurate assessment of renal function than SCr alone. CIN was
defined as an increase of ≥0.5 mg/dl or ≥25% in SCr concentration
over baseline 24–48 h after the intravascular administration of
contrast medium, without an alternative etiology (9).
Statistical analysis
Statistical analysis was performed by a professional
statistics researcher. Continuous variables are expressed as the
mean ± standard deviation. Student’s t-test and one-way analysis of
variance were used for the comparison of continuous variables.
Categorical data were presented as absolute values and percentages.
The χ2 or the Fisher exact tests were used for the
comparison of categorical variables. Pearson’s correlation analysis
was used to evaluate correlations. All hypothesis testing was
two-tailed. P<0.05 was considered as statistically significant.
The SPSS version 16.0 (SPSS, Inc., Chicago, IL, USA) package was
used for all calculations.
Results
Differences in SCr and eGFR values prior
and subsequent to the procedure
These findings are shown in Table I. A total of 180 patients
undergoing coronary interventional procedure were selected. CIN
occurred in 16 of 180 (8.9%) patients. The 180 patients were
divided into a CIN group (16 patients) and a non-CIN group (164
patients). No significant differences were identified in age,
gender, body mass index, hemoglobin, SCr, eGFR and incidence of
hypertension between the CIN and non-CIN groups. The medications
and hydration volumes used during hospitalization were also not
statistically different. The SCr peak level in the CIN group
(105.94±38.29 μmol/l) was significantly higher than that in the
non-CIN group (67.13±16.32 μmol/l) at 48 h after the procedure
(P<0.05). There were significant differences (P<0.05) in the
eGFR level at 24 and 48 h after the procedure between the CIN and
non-CIN groups.
 | Table IDifferences in the SCr and eGFR values
prior and subsequent to the procedure in the two groups. |
Table I
Differences in the SCr and eGFR values
prior and subsequent to the procedure in the two groups.
| Groups | SCr (μmol/l) | eGFR (ml/min/1.73
m2) |
|---|
| Non-CIN |
| Pre-procedure | 70.04±19.25 | 95.30±22.56 |
| Post-procedure |
| 24 h | 65.92±15.81 | 106.10±23.61 |
| 48 h | 67.13±16.32 | 98.65±23.23 |
| CIN |
| Pre-procedure | 73.06±23.62 | 94.30±31.83 |
| Post-procedure |
| 24 h | 84.04±30.52 | 76.84±23.70a |
| 48 h | 105.94±38.29a | 64.66±28.40a |
Differences in urinary IL-18 level prior
and subsequent to the procedure
These findings are shown in Table II. The urinary IL-18 levels were
elevated 2 h after the procedure in the non-CIN and CIN groups, but
no statistically significant difference was identified (P>0.05).
The urinary IL-18 levels in the CIN group increased significantly
at 6 and 12 h after the procedure compared with those in the
non-CIN group (P<0.01), and began to decline 24 h after the
procedure but remained higher than those in the non-CIN group
(P<0.01). The IL-18 levels had not returned to the normal level
48 h after the procedure.
| Table IIDifferences in the urinary IL-18 level
(pg/ml) prior and subsequent to the procedure in the two
groups. |
Table II
Differences in the urinary IL-18 level
(pg/ml) prior and subsequent to the procedure in the two
groups.
| | Post-procedure |
|---|
| |
|
|---|
| Groups | Pre-procedure | 2 h | 6 h | 12 h | 24 h | 48 h |
|---|
| Non-CIN | 590.80±298.66 | 661.60±297.50 | 782.89±270.52a | 834.82±321.81a | 773.99±264.69a | 664.59±232.73 |
| CIN | 646.62±243.59 | 883.79±181.09 | 998.47±302.43b,c |
1172.13±323.68b,c |
1031.56±369.31b,c | 843.92±284.11d |
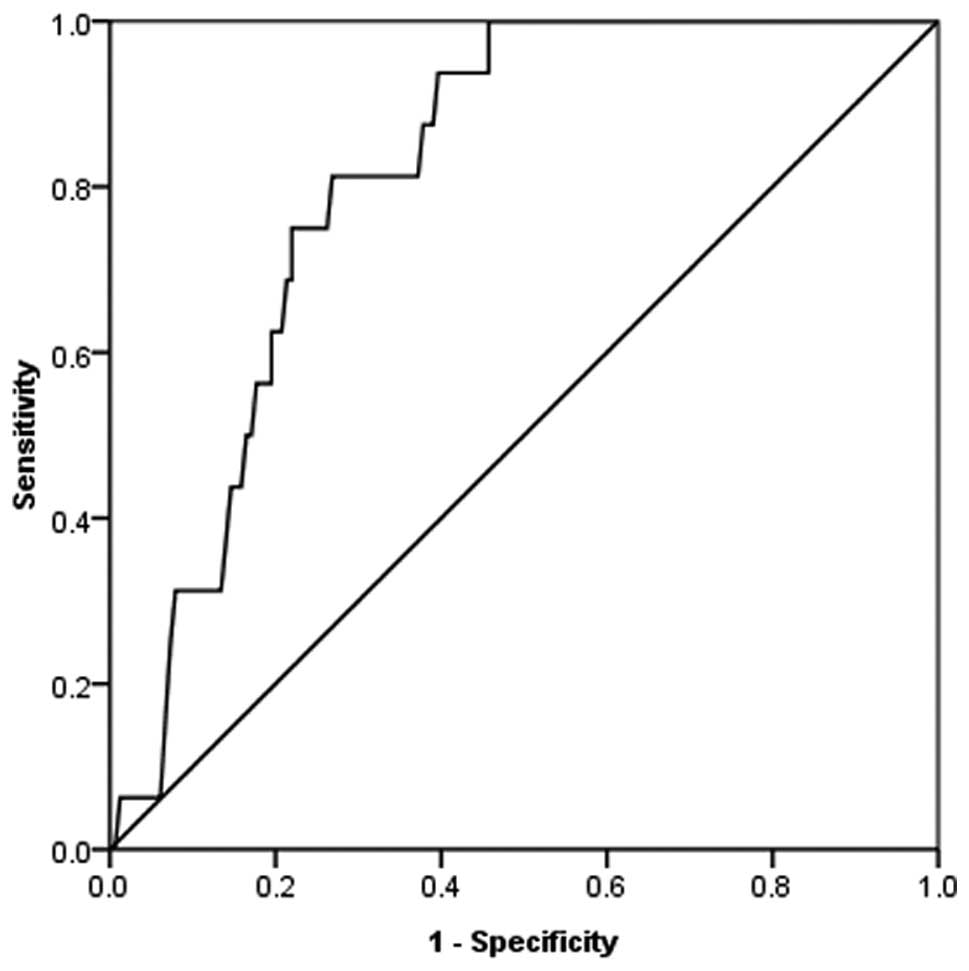
Receiver operating characteristic (ROC)
curve analysis
The ROC curve for urinary IL-18 measured 12 h after
the procedure is shown in Fig. 1.
The area under the ROC curve of urinary IL-18 12 h after the
procedure was 0.811, and the 95% confidence interval of the area
under the curve was 0.735–0.888. If the critical point of the
diagnosis of CIN was 815.61 pg/ml, the sensitivity was 87.5% and
the specificity was 62.2% (P<0.05).
Correlation between urinary IL-18
concentration and SCr
Bivariate analysis shows that the level of IL-18
prior to and within 24–48 h after the procedure positively
correlated with SCr at the same time points. Preoperative urinary
IL-18 and preoperative SCr (r=0.177, P=0.017), postprocedure
24 h urine IL-18 and postoperative 24 h SCr (r=0.174,
P=0.019) and postprocedure 48 h urinary IL-18 and postoperative 48
h SCr (r=0.251, P=0.001) showed positive correlations.
Discussion
With the increasing number of diagnostic and
therapeutic catheterizations each year, particularly among patients
who may have serious conditions predisposing them to CIN, for
example old age, diabetes, renal insufficiency, cardiac
insufficiency and the application of large doses of contrast
medium, the incidence of CIN is likely to continuously increase.
The ability to effectively prevent CIN in high-risk patients should
provide significant public health benefits by potentially reducing
the in-hospital mortality rate, the length of hospital stay and the
subsequent use of chronic hemodialysis. SCr, although used
routinely in clinical practice and in clinical trials, is currently
considered a poor marker of acute renal dysfunction (6). Only when the GFR decreases to <50%
of normal is SCr likely to rise. The detection of acute renal
failure (ARF), which is characterized by a rapid decline in GFR, is
based on an increase in SCr. However, there are limitations in the
application of Cr for evaluating GFR. SCr cannot accurately reflect
GFR in the unsteady state of ARF. Thus, minor changes in Cr, as
observed in early ARF, may reflect a substantial decline in GFR.
Therefore, the early diagnosis of CIN is crucial for prevention
(10).
It is generally accepted that the main mechanism of
CIN, with regard to contrast agent-induced hemodynamic changes and
their effect on renal tubular epithelial cells, is by a direct
toxic effect, with the massive production of free radicals
intensifying the kidney function damage. Urinary IL-18 is an
inflammatory factor expressed in the proximal convoluted tubule. It
comprises 157 amino acid residues and has a molecular weight of
~18.3 kDa. It is activated by caspase-1 in the proximal convoluted
tubule, breaks away from the cell, and is detected in urine
(11). Urinary IL-18 has been
shown to be specific for the diagnosis of ischemic renal injury
(11). A prospective study
involving 138 patients with AKI in an intensive care unit (ICU)
showed that urinary IL-18 was a reliable test for the early
diagnosis of AKI in critically ill patients (6). The pathogenesis of CIN remains
controversial; however, but the main hypothesis is that it involves
renal tubular local ischemia-reperfusion injury (12). Currently the only effective
prevention measure for CIN is hydration therapy (13,14).
Previously, the use of urinary IL-18 as biomarker of AKI has been
investigated in patients in ICUs and in patients following cardiac
surgery and kidney transplantation (6,7,15).
All these studies using urinary IL-18 showed that the biomarker was
able to diagnose AKI much earlier than SCr. The present study
verified that urinary IL-18 could act as an improved early
diagnostic marker for CIN.
The urinary IL-18 concentration and SCr levels were
shown by the correlation analysis to have positive correlations
pre- and postprocedure in the present study. In the CIN group, the
concentration of SCr was statistically significantly different
compared with the preoperative value 48 h after the procedure, the
eGFR was statistically significantly different at 24 h after the
procedure, while the urinary IL-18 level differed significantly 6 h
after the procedure. Studies have also shown that the urinary IL-18
is at its peak 12–24 h after the administration of contrast agents
(7,16). It may be concluded that the urinary
IL-18 level increases earlier than SCr in CIN. Ling et al
(16) examined 150 patients
undergoing a coronary interventional procedure; the urinary IL-18
level increased significantly following the procedure, whereas SCr
exhibited no evident change, compared with that in the non-CIN
group. The study observed that postprocedure urinary IL-18 levels
were clearly increased in the CIN group, which is consistent with
the results of the present study. A study by Bulent et al
(17) compared 15 cases of CIN
with 36 control patients with regard to preoperative and 72 h
postoperative urinary IL-18 concentration, and found no significant
difference in urinary IL-18 concentration in the two groups of
patients. The urinary IL-18 level in kidney injury following
surgery reached a peak 12–24 h postoperatively, and returned to the
baseline level 72 h postoperatively.
Urinary IL-18 can be measured using specific ELISAs,
which are fast, reliable and low-cost, to test urine specimens from
patients. This is a convenient and non-invasive technique, which
therefore can be extended clinically. Postoperative urinary IL-18
is readily monitored, provides an early prediction of the
occurrence of CIN, and enables proactive intervention measures to
be taken to benefit patients. Therefore, the urinary IL-18 level is
an improved indicator for the early prediction of CIN.
The limitations of this study are that the sample
size was small and there were a variety of confounding factors.
Further studies with larger sample sizes and increased monitoring
of serum IL-18 and urine Cr concentrations over the same period,
and the identification and exclusion of certain potential factors
that may also cause increases in IL-18 levels, such as acute
coronary syndrome, are required to validate the findings of the
present study.
Acknowledgements
This study was supported by the Xuzhou Medical
College Science Foundation.
References
|
1
|
Kagan A and Sheikh-Hamad D:
Contrast-induced kidney injury: focus on modifiable risk factors
and prophylactic strategies. Clin Cardiol. 33:62–66. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bartorelli AL and Marenzi G:
Contrast-induced nephropathy. J Interv Cardiol. 21:74–85. 2008.
View Article : Google Scholar
|
|
3
|
Parfrey P: The clinical epidemiology of
contrast-induced nephropathy. Cardiovasc Intervent Radiol. 28(Suppl
2): S3–S11. 2005. View Article : Google Scholar
|
|
4
|
Mehran R and Nikolsky E: Contrast-induced
nephropathy: definition, epidemiology, and patients at risk. Kidney
Int Suppl. (100): S11–S15. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Hardy J, Hambly B, Ko H, et al:
Stimulation of mesangial cells by angiotensin II and
lipopolysaccharide increases expression of interleukin-18, but not
IL-18 receptor. Nephron Exp Nephrol. 116:e63–e71. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Parikh CR, Abraham E, Ancukiewicz M and
Edelstein CL: Urine IL-18 is an early diagnostic marker for acute
kidney injury and predicts mortality in the intensive care unit. J
Am Soc Nephrol. 16:3046–3052. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ma YC, Zuo L, Chen JH, et al: Modified
glomerular filtration rate estimating equation for Chinese patients
with chronic kidney disease. J Am Soc Nephrol. 17:2937–2944. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Malhis M, Al-Bitar S and Al-Deen Zaiat K:
The role of theophylline in prevention of radiocontrast
media-induced nephropathy. Saudi J Kidney Dis Transpl. 21:276–283.
2010.PubMed/NCBI
|
|
9
|
McCullough PA and Soman SS:
Contrast-induced nephropathy. Crit Care Clin. 21:261–280. 2005.
View Article : Google Scholar
|
|
10
|
Melnikov VY, Ecder T, Fantuzzi G, et al:
Impaired IL-18 processing protects caspase-1-deficient mice from
ischemic acute renal failure. J Clin Invest. 107:1145–1152. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Detrenis S, Meschi M, Musini S and Savazzi
G: Lights and shadows on the pathogenesis of contrast-induced
nephropathy: state of the art. Nephrol Dial Transplant.
20:1542–1550. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Trivedi HS, Moore H, Nasr S, et al: A
randomized prospective trial to assess the role of saline hydration
on the development of contrast nephrotoxicity. Nephron Clin Pract.
93:C29–C34. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Thomsen HS: How to avoid CIN: guidelines
from the European Society of Urogenital Radiology. Nephrol Dial
Transplant. 20(Suppl 1): i18–i22. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Parikh CR, Jani A, Mishra J, et al: Urine
NGAL and IL-18 are predictive biomarkers for delayed graft function
following kidney transplantation. Am J Transplant. 6:1639–1645.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Parikh CR, Mishra J, Thiessen-Philbrook H,
et al: Urinary IL-18 is an early predictive biomarker of acute
kidney injury after cardiac surgery. Kidney Int. 70:199–203. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ling W, Zhaohui N, Ben H, et al: Urinary
IL-18 and NGAL as early predictive biomarkers in contrast-induced
nephropathy after coronary angiography. Nephron Clin Pract.
108:c176–c181. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Bulent Gul CB, Gullulu M, Oral B, et al:
Urinary IL-18: a marker of contrast-induced nephropathy following
percutaneous coronary intervention? Clin Biochem. 41:544–547.
2008.PubMed/NCBI
|