Introduction
Papillary thyroid carcinoma (PTC) is the most common
type of primary malignant thyroid cancer, with the incidence rate
increasing in the last decade (1).
Due to the insidious onset and slow development of PTC (2), an early diagnosis is important to
select the correct treatment strategy and improve prognosis
(3). However, in papillary thyroid
microcarcinoma (PTMC), the rates of incorrect and missed diagnoses
are high due to the atypical clinical symptoms and more aggressive
behavior with regional and distant metastases (4,5).
Computed tomography, magnetic resonance imaging and isotope
examination are all ineffective; therefore, ultrasound examination
is the best method of diagnosing PTC (6). However, whether PTMC and papillary
thyroid non-microcarcinoma (non-PTMC) exhibit the same ultrasonic
performances is controversial (2,7). The
aim of the present study was to retrospectively compare the
sonographic features of PTMC and non-PTMC, in order to improve the
diagnostic value of ultrasonography.
Materials and methods
General data
For retrospective analysis, data from a total of 328
patients with PTC, who had undergone thyroid surgery at the Beijing
Friendship Hospital (Beijing, China), were collected between June
2010 and October 2013. Of the cases analyzed, 72 were male and 256
were female, aged between 19 and 83 years, with a mean age of
43.6±12.5 years. The case histories ranged between one day and five
years. All the patients underwent preoperative ultrasonography
within two weeks and a diagnosis of PTC was confirmed by surgery
and pathological examination. The study was conducted in accordance
with the Declaration of Helsinki and with approval from the Ethics
Committee of the Capital Medical University (Beijing, China).
Written informed consent was obtained from all the
participants.
Ultrasound examination
Philips iU22 (Philips Ultrasound, Inc., Bothell, WA,
USA), GE LOGIQ E9 (GE Healthcare, Wauwatosa, WI, USA) and HI VISION
Preirus (Hitachi Medical Corporation, Tokyo, Japan) color
ultrasound diagnostic apparatus were used for analysis, with the
probe frequency set at 5–12 MHz. The patients were placed in a
supine position, exposing the anterior thyroid area, scanning
multi-slice display thyroid nodules, number, size, shape, ratio of
length/width, boundary, echo, peripheral halo ring, calcification
rate, cystic changes, blood flow and accompanying diseases were
observed. A PTMC diagnosis was confirmed if the tumor diameter was
≤10 mm, while non-PTMC cases were confirmed with a tumor diameter
of >10 mm, according to the World Health Organization criteria
(8). The calcification types were
as follows: Microcalcification, ≤2 mm in diameter with punctate
hyperechoic foci, with or without shadow and a scattered or
clustered distribution; and coarse calcifications, >2 mm in
diameter with sheet or shell-like hyperechoic foci and shadow.
Adler flow grading (9) was
determined as follows: Grade 0, no blood flow; grade I, a small
amount of blood with 1–2 punctuate or rod-like blood vessels; grade
II, medium flow with three or four blood vessels, one of which
being longer than the radius of the nodule; grade III, rich in
blood and more than four visible blood vessels or interconnected
angiogenesis, interwoven into a network (9).
Statistical analysis
Data were analyzed using SPSS 17.0 software (SPSS,
Inc., Chicago, IL USA), and measurement data are expressed as the
mean ± standard deviation. Enumeration data were analyzed with the
χ2 test, while the Wilcoxon rank-sum test was used to
analyze the differences in blood flow between the two groups.
P<0.05 was considered to indicate a statistically significant
difference.
Results
Pathological observations
A total of 389 nodules were detected by ultrasound
in the 328 cases. Of these, 167 nodules were located in the left
lobe, 195 were identified in the right lobe and 27 were present in
the isthmus. There were 209 PTMC nodules and 180 non-PTMC nodules.
Of the patients examined, there were 52 (52/328, 15.9%) multifocal
cases where between two and six nodules were identified, of which
37 were cases of PTMC and non-PTMC combined, while the remaining 15
cases were all PTMC. In total, 58.61% (228/389) of the nodules were
found in patients with other thyroid diseases, including
Hashimoto’s thyroiditis (HT; 38.60%; 88/228), nodular goiter
(52.19%; 119/228), adenoma (1.32%; 3/228) and nodular goiter
accompanied with HT or adenoma (7.89%; 18/228); however,
statistically significant differences were not observed when
comparing the PTMC and non-PTMC cases (P>0.05; Table I). There were 57 PTMC (57/209,
27.27%) and 103 non-PTMC (103/180, 57.22%) cases of lymph node
metastasis; the difference between the two groups was statistically
significant (P<0.05).
 | Table IComparison of additional accompanying
thyroid diseases in the patients. |
Table I
Comparison of additional accompanying
thyroid diseases in the patients.
| Group | HT | Nodular goiter | Adenoma | Nodular goiter with
HT | Nodular goiter with
adenoma |
|---|
| PTMC, n | 50 | 57 | 1 | 7 | 3 |
| Non-PTMC, n | 38 | 62 | 2 | 6 | 2 |
| Total, n | 88 | 119 | 3 | 13 | 5 |
Ultrasound observations
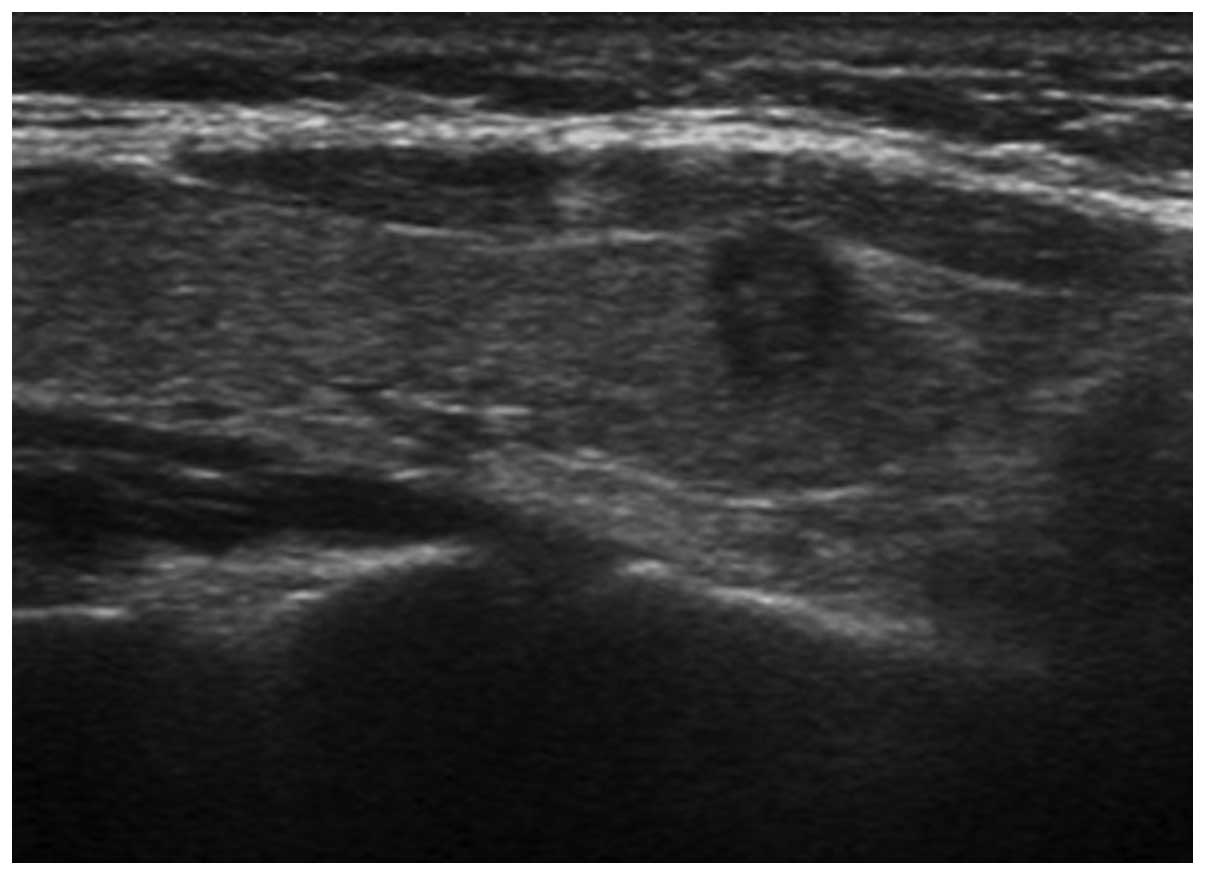
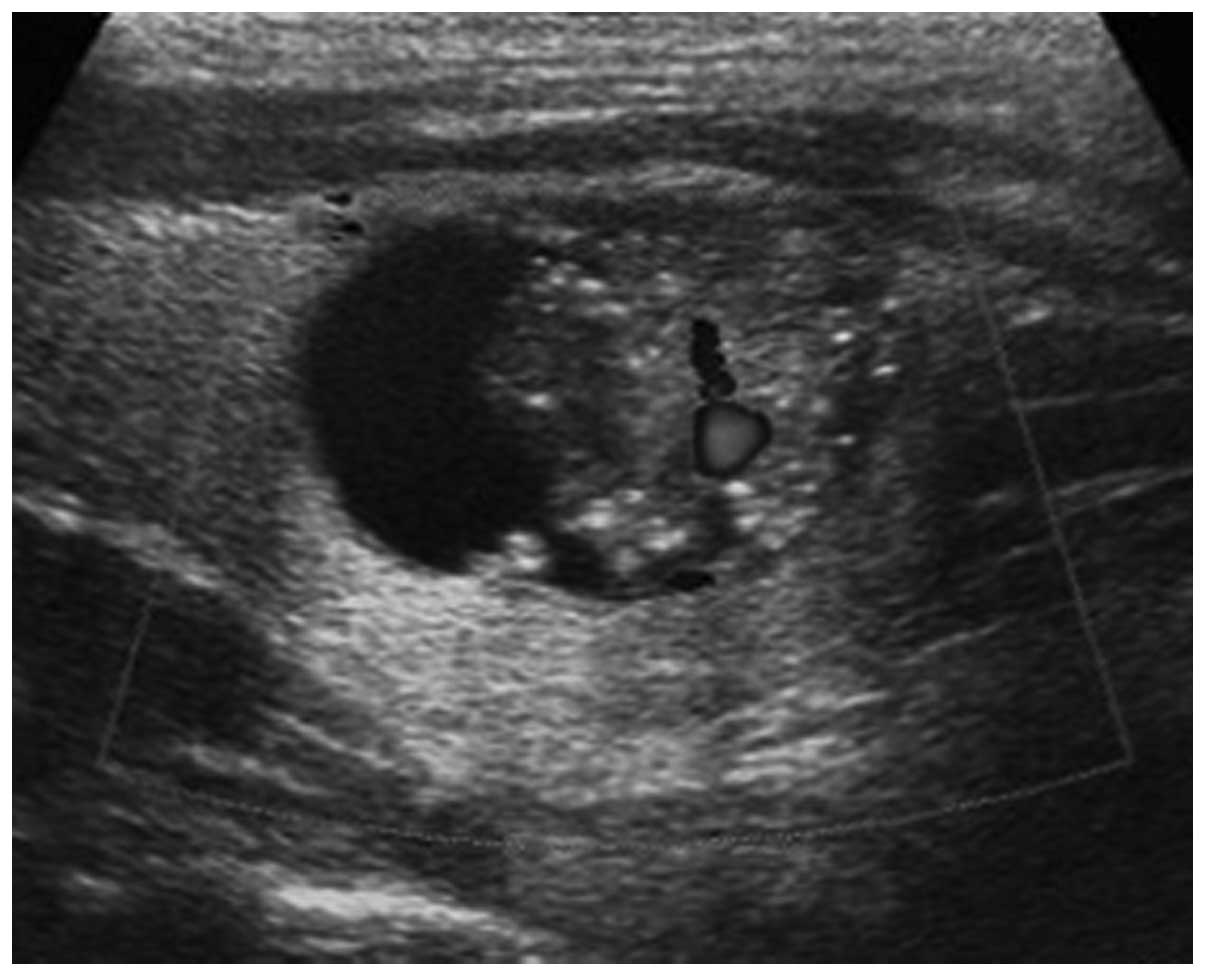
Ultrasound scans detected 371 nodules, ranging in
size between 0.24×0.32 and 5.35×3.86 cm. Of these, 191 were PTMC
nodules and 180 were non-PTMC nodules (Figs. 1–4). The scans missed 18 nodules, which
were all PTMCs with a diameter of ≤3 mm. A total of 57 nodules were
misdiagnosed, including 24 PTMCs and 33 non-PTMCs, of which 52 were
misdiagnosed as nodular goiter and five were misdiagnosed as
adenomas.
With regard to the PTMC nodules, an unclear boundary
and length/width ratio of ≥1 accounted for 87.96% (168/191) and
46.60% (89/191) of cases, respectively. By contrast, in the
non-PTMC nodules, an unclear boundary and length/width ratio of ≥1
accounted for 69.44% (125/180) and 3.89% (7/180) of cases,
respectively. The blood flow in the PTMC nodules was predominantly
grade 0-I, accounting for 81.68% (156/191) of the nodules. In the
non-PTMC nodules, the blood flow was mainly grade II-III,
accounting for 70.00% of the nodules (126/180; Table II).
| Table IIComparisons of the shape, boundary,
ratio of length/width and blood flow. |
Table II
Comparisons of the shape, boundary,
ratio of length/width and blood flow.
| Shape | Boundary | Ratio of
length/width | Blood flowb |
|---|
|
|
|
|
|
|---|
| Group | Regular | Irregular | Clear | Unclear | <1 | ≥1 | 0 | I | II | III |
|---|
| PTMC, n | 31 | 160 | 23 | 168 | 102 | 89 | 52 | 104 | 24 | 11 |
| Non-PTMC, n | 26 | 154 | 55 | 125 | 173 | 7 | 9 | 45 | 84 | 42 |
|
χ2-value | 0.23 | 19.13 | 88.12 | −6.76a |
| P-value | 0.63 | <0.01 | <0.01 | <0.01 |
There were no cystic changes observed in the PTMC
nodules; however, the rate of cystic change in the non-PTMC cases
was ~16.67% (30/180), and the difference between the two carcinoma
types was statistically significant (P<0.05). A total of 63.33%
(19/30) of the non-PTMC cases with cystic changes had
microcalcifications in the solid component. PTMC nodules were
mainly hypoechoic (167/191; 87.43%); however, the echogenicity of
the non-PTMC nodules varied, with 53.89% (97/180) of the nodules
being hypoechoic. The difference in echogenicity between the two
carcinoma types was statistically significant (P<0.05).
Microcalcifications and coarse calcifications were present in
37.70% (72/191) and 18.32% (35/191) of the PTMC nodules,
respectively, and 42.78% (77/180) and 18.33% (33/180) of the
non-PTMC nodules, respectively. No statistically significant
differences in the calcification rate and ratio were observed
between the two groups (P>0.05). Furthermore, the two groups
were rarely accompanied by a peripheral halo ring (Table III).
| Table IIIComparisons of the cystic changes,
echo of solid component, peripheral halo rings and calcification
type. |
Table III
Comparisons of the cystic changes,
echo of solid component, peripheral halo rings and calcification
type.
| Cystic changes | Echo of solid
component | Peripheral halo
ring | Calcification |
|---|
|
|
|
|
|
|---|
| Group | Solid | Cyst-solid | Hypoechoic |
Equal/hyperechoic | With | Without | Without | Micro- | Coarse |
|---|
| PTMC, n | 191 | 0 | 167 | 248 | 12 | 179 | 84 | 72 | 35 |
| Non-PTMC, n | 150 | 30 | 97 | 83 | 11 | 169 | 70 | 77 | 33 |
|
χ2-value | 34.63 | 50.81 | 0.01 | 1.17 |
| P-value | <0.01 | <0.01 | 0.905 | 0.56 |
Discussion
PTC is the most common type of thyroid cancer, with
a low degree of malignancy and a good prognosis. Thyroid
microcarcinoma refers to nodules with a diameter of ≤10 mm, with or
without regional or distant lymph node metastasis. The incidence
rate of PTMC is 2.0–35.6% in autopsy (10). PTMC cases accounted for 53.73%
(209/389) of the total nodules analyzed in the present study. PTMC
presents as isolated nodules that coexist with a larger tumor or
exist in large benign nodules (11). In the current study, 18 cases of
PTMC were missed by ultrasound scans as they were identified as
local carcinogenesis in larger nodules. There is no pathological
difference between PTMC and non-PTMC. At present, more research has
focused on the molecular level (12,13).
The growth of PTMC nodules is slow; a previous study revealed that
the 30-year recurrence rate was 40% in patients of >55
years-old, and the prognosis rate was better in younger individuals
(14).
Multiple nodules are one of the clinical features of
PTC, with a reported occurrence rate of 18–87% (15). The occurrence rate was slightly
lower in the present study, possibly due to a smaller range of
pathological specimens. Pathological examination of the entire
gland may result in a higher incidence due to the fact that
contralateral disease is also detected (15). A previous study observed that there
was a high degree of malignancy in multiple nodules, as well as
cervical lymph node metastasis and a larger proportion of thyroid
infiltration; however, no statistically significant differences
were observed in the disease-specific and total mortality rates
when comparing PTMC and non-PTMC patients (16). Whether the formation of multiple
foci occurs from the gland or is of polyclonal origin remains
controversial. A previous study (17) confirmed that a considerable part of
multifocal PTC is of polyclonal origin. Thus, there are limits to
detecting multifocal nodules by ultrasound scans as they may merge
with other benign thyroid lesions.
PTMC nodules are primarily hypoechoic, which may be
associated with the low degree of differentiation in cancer cells,
fewer interstitial components and a good sound transmission in the
tumor. With nodule growth, blood vessels and fibrous tissue undergo
hyperplasia, causing the echogenicity to vary. As the tumors grow
faster, liquefaction necrosis and cystic changes occur (18). In the present study, cystic changes
were observed in non-PTMC, with more than half of the cases
accompanied by microcalcifications within the solid component. A
previous study demonstrated that microcalcifications in the solid
component of cystic-solid nodules have a higher specificity for the
diagnosis of PTC (19).
Microcalcifications may reflect psammoma bodies,
which are the most specific diagnostic indicators of PTC (20). A previous study (21) revealed that microcalcifications
occur as a result of good growth of autocrine tumor cells, while
coarse calcification occurs as a result of the rapid growth of
cancer cells, tissue hyperplasia, degeneration and then calcium
deposition, known as dystrophic calcification. In the current
study, microcalcifications accounted for 40.16% (149/371) of cases,
while coarse calcifications were present in 18.33% (68/371) of
cases and no calcification was observed in 41.51% (154/371) of the
total nodules detected. No statistically significant difference in
calcification was identified between the groups.
Neovascularization provides nutrients for the growth
of malignant tumors. In the present study, the blood flow of the
PTMC nodules was primarily grade 0-I, whereas the blood flow in the
non-PTMC nodules was mainly grade II-III. This difference may be
due to the fact that there is no neovascularization in non-PTMC or
because low-velocity blood signals were not shown due to improper
adjustment of the instrument.
PTC often coexists with nodular goiter, HT and
adenoma. In the present study, the detection rate of PTC was
significantly lower when the disease was accompanied with nodular
goiter, as atypical nodules may be ignored when scanning multiple
foci. However, the most important reason for misdiagnosis is that
the sonographer may lack knowledge of the local carcinogenesis of
benign nodules. The pathological basis of HT is lymphocytic
infiltration and follicular cell destruction. A previous study
revealed that PTC was accompanied by HT in ~18% of cases (22). HT may destroy follicular cells and
reduce the secretion of thyroid hormones. In addition, feedback
causes increased secretion of thyroid-stimulating hormone, which
stimulates hyperplasia of the follicular epithelium. From
investigations at a molecular level, including investigations into
rearranged during transfection protooncogene/PTC and
cytokeratin-19, certain studies have hypothesized that HT is a
precancerous form of PTC (23,24).
Thus, nodules in HT should be closely followed-up.
In conclusion, ultrasound has an important value in
the diagnosis of PTC. Specific differences exist in the ultrasonic
features between PTMC and non-PTMC; however, the diagnosis of
benign nodules accompanied by the occasional microcancer has
limitations. For cases which are difficult to diagnose, fine-needle
aspiration or ultrasound-guided biopsy should be considered.
References
|
1
|
Londero SC, Krogdahl A, Bastholt L, et al:
Papillary thyroid carcinoma in Denmark 1996–2008: an investigation
of changes in incidence. Cancer Epidemiol. 37:e1–e6. 2013.
|
|
2
|
Ito Y and Miyauchi A: A therapeutic
strategy for incidentally detected papillary microcarcinoma of the
thyroid. Nat Clin Pract Endocrinol Metab. 3:240–248. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sakorafas GH, Giotakis J and Stafyla V:
Papillary thyroid microcarcinoma: a surgical perspective. Cancer
Treat Rev. 31:423–438. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Arora N, Turbendian HK, Kato MA, Moo TA,
Zarnegar R and Fahey TJ III: Papillary thyroid carcinoma and
microcarcinoma: is there a need to distinguish the two? Thyroid.
19:473–477. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lee HS, Park HS, Kim SW, et al: Clinical
characteristics of papillary thyroid microcarcinoma less than or
equal to 5 mm on ultrasonography. Eur Arch Otorhinolaryngol.
270:2969–2974. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Anil G, Hegde A and Chong FH: Thyroid
nodules: risk stratification for malignancy with ultrasound and
guided biopsy. Cancer Imaging. 11:209–223. 2011.PubMed/NCBI
|
|
7
|
Page C, Biet A, Boute P, et al:
‘Aggressive papillary’ thyroid microcarcinoma. Eur Arch
Otorhinolaryngol. 266:1959–1963. 2009.
|
|
8
|
DeLellis RA, Lloyd RV, Heitz PU and Eng C:
World Health Organization Classification of Tumours. Pathology and
Genetics of Tumours of Endocrine Organs. 8. IARC Press; Lyon:
2004
|
|
9
|
Adler DD, Carson PL, Rubin JM and
Quinn-Reid D: Doppler ultrasound color flow imaging in the study of
breast cancer: preliminary findings. Ultrasound Med Biol.
16:553–559. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pazaitou-Panayiotou K, Capezzone M and
Pacini F: Clinical features and therapeutic implication of
papillary thyroid microcarcinoma. Thyroid. 17:1085–1092. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Londero SC, Krogdahl A, Bastholt L, et al:
Papillary thyroid microcarcinoma in Denmark 1996–2008: a national
study of epidemiology and clinical significance. Thyroid.
23:1159–1164. 2013.PubMed/NCBI
|
|
12
|
Antonaci A, Consorti F, Mardente S,
Natalizi S, Giovannone G and Della Rocca C: Survivin and cyclin D1
are jointly expressed in thyroid papillary carcinoma and
microcarcinoma. Oncol Rep. 20:63–67. 2008.PubMed/NCBI
|
|
13
|
Park YJ, Kim YA, Lee YJ, et al: Papillary
microcarcinoma in comparison with larger papillary thyroid
carcinoma in BRAF(V600E) mutation, clinicopathological features,
and immunohistochemical findings. Head Neck. 32:38–45. 2010.
|
|
14
|
Noguchi S, Yamashita H, Uchino S and
Watanabe S: Papillary microcarcinoma. World J Surg. 32:747–753.
2008. View Article : Google Scholar
|
|
15
|
Mazeh H, Samet Y, Hochstein D, et al:
Multifocality in well-differentiated thyroid carcinomas calls for
total thyroidectomy. Am J Surg. 201:770–775. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kuo SF, Lin SF, Chao TC, Hsueh C, Lin KJ
and Lin JD: Prognosis of multifocal papillary thyroid carcinoma.
Int J Endocrinol. 2013:8093822013.PubMed/NCBI
|
|
17
|
Kuhn E, Teller L, Piana S, Rosai J and
Merino MJ: Different clonal origin of bilateral papillary thyroid
carcinoma, with a review of the literature. Endocr Pathol.
23:101–107. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wang Y, Li L, Wang YX, Feng XL, et al:
Ultrasound findings of papillary thyroid microcarcinoma: a review
of 113 consecutive cases with histopathologic correlation.
Ultrasound Med Biol. 38:1681–1688. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Park JM, Choi Y and Kwag HJ: Partially
cystic thyroid nodules: ultrasound findings of malignancy. Korean J
Radiol. 13:530–535. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Trimboli P, Nasrollah N, Amendola S, et
al: Should we use ultrasound features associated with papillary
thyroid cancer in diagnosing medullary thyroid cancer? Endocr J.
59:503–508. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Das DK, Sheikh ZA, George SS, Al-Baquer T
and Francis IM: Papillary thyroid carcinoma: evidence for
intracytoplasmic formation of precursor substance for calcification
and its release from well-preserved neoplastic cells. Diagn
Cytopathol. 36:809–812. 2008. View
Article : Google Scholar
|
|
22
|
Lun Y, Wu X, Xia Q, et al: Hashimoto’s
thyroiditis as a risk factor of papillary thyroid cancer may
improve cancer prognosis. Otolaryngol Head Neck Surg. 148:396–402.
2013.
|
|
23
|
Jankovic B, Le KT and Hershman JM:
Clinical Review: Hashimoto’s thyroiditis and papillary thyroid
carcinoma: is there a correlation? J Clin Endocrinol Metab.
98:474–482. 2013.
|
|
24
|
Flanagan JN, Pineda P, Knapp PE, De Las
Morenas A, Lee SL and Braverman LE: Expression of cytokeratin 19 in
the diagnosis of thyroid papillary carcinoma by quantitative
polymerase chain reaction. Endocr Pract. 14:168–174. 2008.
View Article : Google Scholar : PubMed/NCBI
|