Introduction
Treatment of lung cancer usually involves surgery in
the early stages and radiotherapy or chemoradiotherapy in more
advanced stages of the disease (1). Cancer recurrence may occur in
multiple sites following primary treatment. Although recurrent and
metastatic disease is usually not curable, surgical treatment may
be beneficial in cases where locoregional recurrence is detected
early. Performing 18F-fluorodeoxyglucose positron
emission tomography-computed tomography (18F-FDG PET-CT)
is important in the diagnosis of clinically suspicious recurrent
lung cancer (2). However, the
diagnostic efficiency of PET-CT remains controversial (3,4). A
previous study demonstrated that delayed PET-CT scans enhanced the
variation of FDG uptake between a number of lesions (5). In addition, delayed maximum
standardized uptake values (SUVmax) of >5.5 were shown to
improve the differentiation of hypermetabolic lesions compared with
earlier scans. However, careful interpretation and management are
still required for correct diagnosis. In the present study, a case
of pulmonary tuberculosis, suspected as recurrent lung cancer
following PET-CT scans, was examined.
Case report
A 67-year-old male was admitted to the Surgical
Outpatients Department of The First Affiliated Hospital of Soochow
University (Suzhou, China), with a mass lesion (2×2 cm) on the
right lung (Fig. 1). The lesion
was detected during a routine medical examination. A video-assisted
thoracoscopic lobectomy was performed to remove the mass, and
histopathological examination revealed a lung adenocarcinoma with
visceral pleural invasion. The patient underwent four courses of
adjuvant chemotherapy (75 mg/m2 cisplatin and 100
mg/m2 gemcitabine) and was clinically diagnosed as
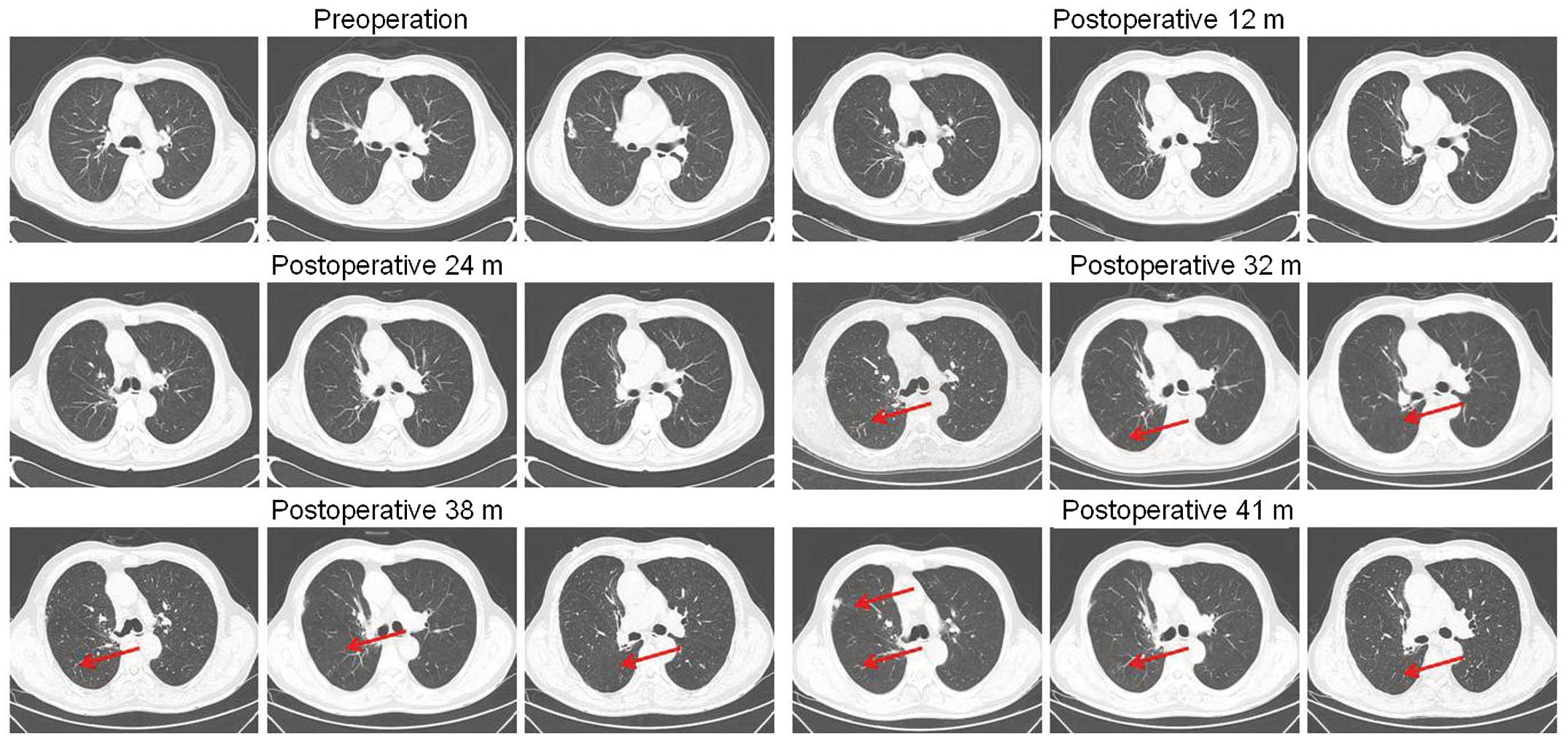
disease free. However, the appearance of multiple patchy shadows on
the right lung was observed in CT scans at 32 months following the
surgery (6). The patient did not
present any evident changes in the chest radiographs and serum
tumor marker tests during the subsequent nine-month follow-up
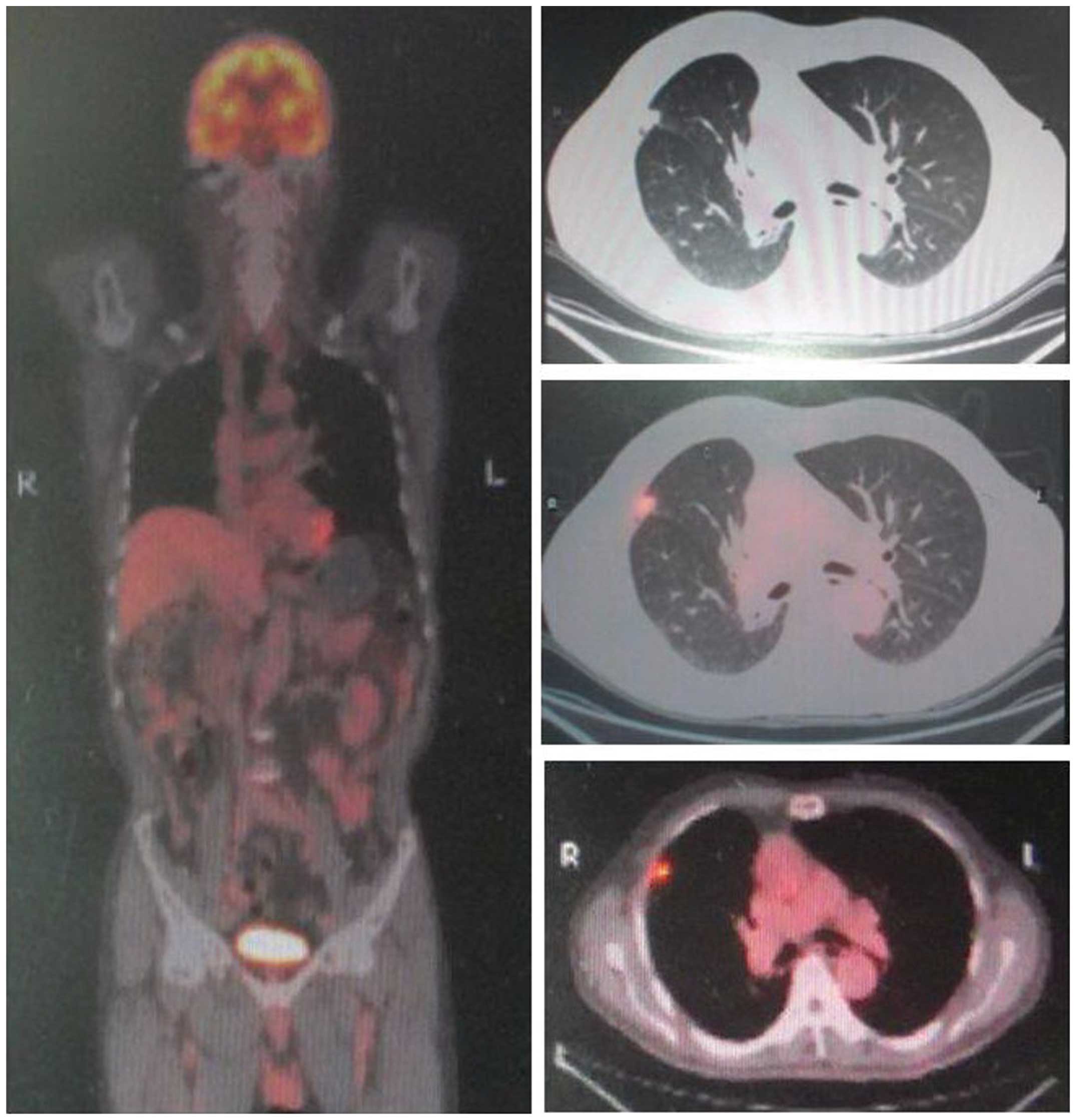
period. After the nine-month period, chest CT scans revealed a
subpleural nodule (0.5×0.5 cm) and a slight enlargement of the
patchy shadow on the right lung (Fig.
2). PET-CT scans revealed that the FDG uptake of the nodule had
a SUVmax of 6.1. A that indicated malignant disease. A
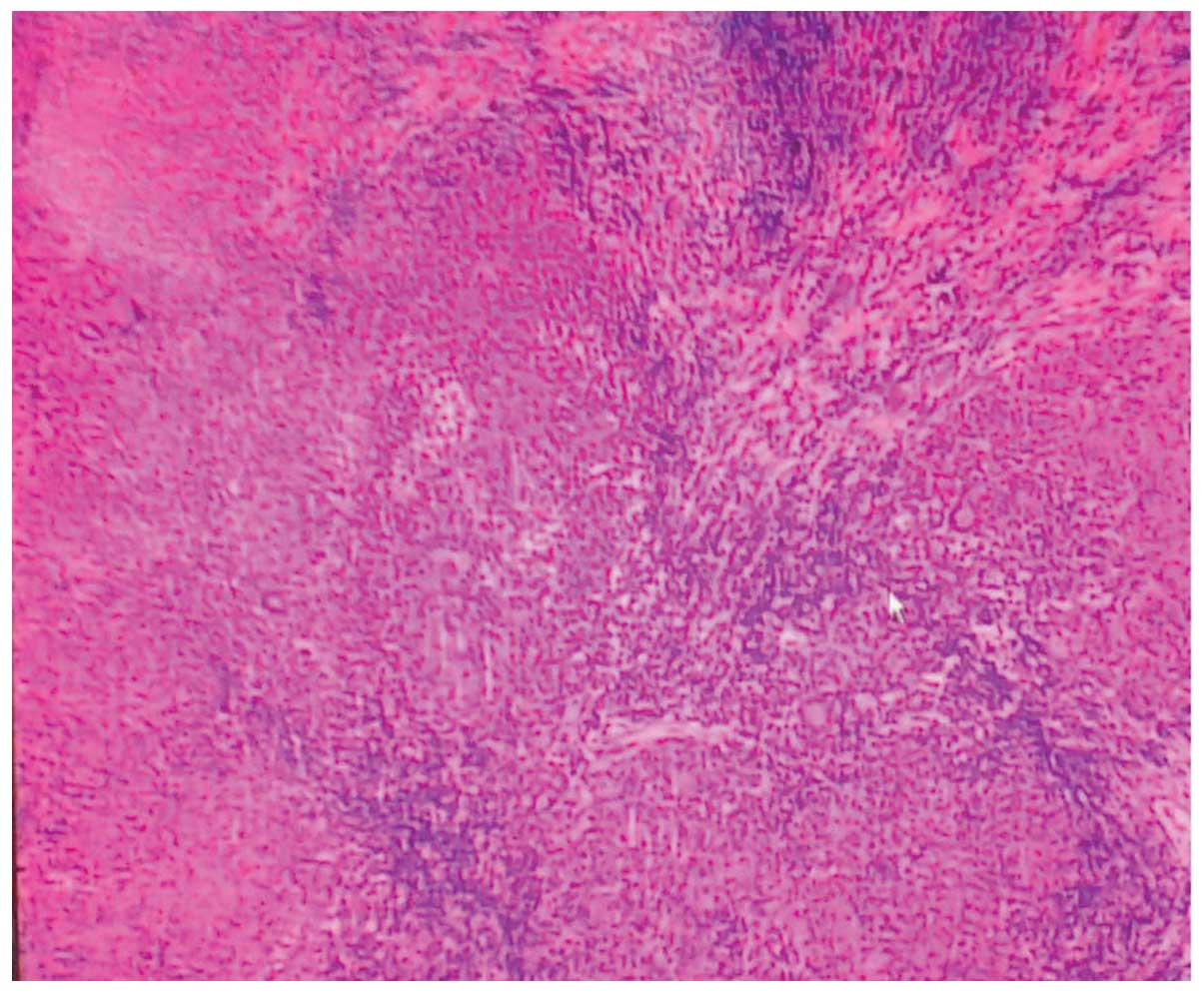
video-assisted thoracoscopic biopsy indicated that the patient
suffered from tuberculosis (Fig.
3). Written informed consent was obtained from the patient.
Discussion
Adenocarcinoma is the predominant histological
subtype of lung carcinoma (7);
however, smear pulmonary tuberculosis appearing on the surgical
site as the recurrence of lung cancer is extremely rare,
particularly during the postoperative follow-up period.
Postoperative recurrence of lung cancer is commonly
diagnosed by CT or PET-CT scans and clinical features, instead of a
rebiopsy. PET-CT is the most sensitive non-invasive imaging method
for the detection of tumor metastases and recurrence, since these
scans enable more accurate assessment of the tumor morphology,
composition, location and extent (8). However, the diagnostic efficiency of
PET-CT remains controversial, since a number of benign lesions may
exhibit increased metabolic activity, leading to a false positive
result. Failure to differentiate between recurrent tumors and
benign lesions may result in inappropriate treatment. Therefore,
previous studies have attempted to evaluate the accuracy of PET-CT
as a diagnostic method, and the characteristics of false negatives
and false positives, to improve specificity and sensitivity
(5,9). Razak et al demonstrated that
early whole body PET-CT may efficiently detect extrapulmonary
tuberculosis lesions, while dual time point imaging may not be able
to determine the lesion type (9).
The present study reports the case of a 67-year-old
male with pulmonary tuberculosis, whose PET-CT images mimicked
recurrent lung cancer. Due to the slow progress of the multiple
patchy shadows on the right lung, along with the increased FDG
uptake in a short-term growing subpleural nodule, the patient was
suspected to suffer from recurrent lung cancer. However, the slow
progress of the multiple patchy shadows and the normality of the
serum tumor markers prompted a video-assisted thoracoscopic
rebiopsy to be performed. Pathological examination confirmed the
inference that the subpleural nodule was due to tuberculosis
instead of recurrent lung cancer. Therefore, further evaluation is
required in all patients with a suspected metastatic and recurrent
carcinoma, and rebiopsy is a valuable method for certain patients,
since other conditions may exist, including a benign disease.
Acknowledgements
The study was supported by grants from the Jiangsu
Provincial Special Program of Medical Science (no. BL2012023), the
Department of Public Health of Jiangsu Province Project (no.
H201208), the Natural Science Foundation of Jiangsu Province
University (no. 13KJB320021) and the National Key Clinical
Specialist Construction Programs of China and Ministry of Health
for Public Projects (no. 201402024).
References
|
1
|
Spiro SG, Gould MK and Colice GL; American
College of Chest Physicians. Initial evaluation of the patient with
lung cancer: symptoms, signs, laboratory tests, and paraneoplastic
syndromes: ACCP evidenced-based clinical practice guidelines (2nd
edition). Chest. 132(3 Suppl): 149S–160S. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Liao S, Penney BC, Wroblewski K, et al:
Prognostic value of metabolic tumor burden on 18F-FDG PET in
nonsurgical patients with non-small cell lung cancer. Eur J Nucl
Med Mol Imaging. 39:27–38. 2012. View Article : Google Scholar
|
|
3
|
Burdick MJ, Stephans KL, Reddy CA, Djemil
T, Srinivas SM and Videtic GM: Maximum standardized uptake value
from staging FDG-PET/CT does not predict treatment outcome for
early-stage non-small-cell lung cancer treated with stereotactic
body radiotherapy. Int J Radiat Oncol Biol Phys. 78:1033–1039.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Li S, Zheng Q, Ma Y, Wang Y, Feng Y, Zhao
B and Yang Y: Implications of false negative and false positive
diagnosis in lymph node staging of NSCLC by means of
18F-FDG PET/CT. PLoS One. 8:e785522013. View Article : Google Scholar
|
|
5
|
Suga K, Kawakami Y, Hiyama A, Sugi K,
Okabe K, Matsumoto T, Ueda K, Tanaka N and Matsunaga N: Dual-time
point 18F-FDG PET/CT scan for differentiation between 18F-FDG-avid
non-small cell lung cancer and benign lesions. Ann Nucl Med.
23:427–435. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Fisher MD and D’Orazio A: Phase II and III
trials: comparison of four chemotherapy regimens in advanced non
small-cell lung cancer (ECOG 1594). Clin Lung Cancer. 2:21–22.
2000. View Article : Google Scholar
|
|
7
|
Tse LA, Mang OW, Yu IT, Wu F, Au JS and
Law SC: Cigarette smoking and changing trends of lung cancer
incidence by histological subtype among Chinese male population.
Lung Cancer. 66:22–27. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ozgül MA, Kirkil G, Seyhan EC, Cetinkaya
E, Ozgül G and Yüksel M: The maximum standardized FDG uptake on
PET-CT in patients with non-small cell lung cancer. Multidiscip
Respir Med. 8:692013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Razak HR, Geso M, Abdul Rahim N and Nordin
AJ: Imaging characteristics of extrapulmonary tuberculosis lesions
on dual time point imaging (DTPI) of FDG PET/CT. J Med Imaging
Radiat Oncol. 55:556–562. 2011. View Article : Google Scholar : PubMed/NCBI
|