Introduction
Ankylosing spondylitis (AS) is a systemic chronic
rheumatic disease that presents with inflammatory back pain,
asymmetrical peripheral arthritis, enthesitis and extra-articular
features (1). Apart from spinal
stiffness and loss of spinal mobility, AS has a considerable impact
on the quality of life (QoL) of patients. Doctors often concentrate
on skeletal damage and measures of pain, whereas most AS patients
focus on feeling well and the capability to live a full life
(2). AS affects patients’
health-related QoL, work life, relationships with family and spouse
and expectations (3). Sexuality
has been described as an essential part of the whole person, and
sexual expression has been cited as a crucial part of an
individual’s self identity (4).
Sexual function plays a significant role in QoL and it is
particularly important for patients with AS as it mainly affects
young individuals.
The effect of rheumatologic diseases, particularly
AS, on sexual function has been explored (5,6). A
previous study demonstrated that patients with erectile dysfunction
(ED) were at a higher risk for AS (odds ratio=2.19) (7). A population-based study demonstrated
that ED was associated with AS (8). However, another study indicated that
the prevalence of ED among AS patients was similar to that of
normal healthy controls (9).
Therefore, whether AS patients harbor an increased risk of sexual
dysfunction when compared to normal population remains
controversial.
The aim of this study was to summarize the existing
evidence and explore the effect of AS on sexual function by
conducting a systematic review and meta-analysis.
Materials and methods
The meta-analysis was reported in accordance with
the recommendations of the Preferred Reporting Items for Systemic
Review and Meta-Analyses (PRISMA) and the Meta-analysis of
Observational Studies in Epidemiology (MOOSE) as closely as
possible (10,11).
Literature search strategy
The following digital databases were searched to
identify relevant trials: PubMed, Embase and the Cochrane Library.
In addition, Chinese databases were searched, including the CNKI
Scholar, VIP, Chinese BioMedicine (CBM) and WanFang databases.
Up-to-date information regarding AS-related sexual function up to
May 2013 was retrieved from these databases.
Different search strategies were combined, as
follows. For the English-language databases, free text such as
‘sexual activity’, ‘sexual function’, ‘impotence’ or ‘erectile
dysfunction’ and ‘Marie-Struempell disease’ ‘Bechterew disease’
‘ankylosing spondylarthritis’ or ‘ankylosing spondylitis’ were
used. For the Chinese databases, free text terms were used,
including the Chinese translations of terms meaning sexual
function, erectile dysfunction and AS. In order to collect an
adequate number of trials, the reference lists of relevant
publications were also searched to identify additional studies.
Inclusion and exclusion criteria
The focus of the analysis was on studies of sexual
function in AS regardless of gender, publication status or
language. Studies were selected for analysis if they satisfied the
following criteria: i) Studies that assessed the association
between sexual function and AS; ii) the subjects enrolled were
diagnosed with AS according to modified New York criteria for AS
(12); and iii) sexual function
was evaluated using the International Index of Erectile Function
(IIEF) (13) or the Female Sexual
Function Index (FSFI) (14)
scoring system. Studies were eliminated if sexual function was
evaluated by other scoring systems.
For repeated studies of the same data, authors of
reports were contacted to clarify ambiguity. If the author could
not be reached, the first published study was considered as
original. Two reviewers selected articles independently. Based on
the PRISMA requirements, a flow diagram of the study selection was
generated.
Data extraction
The relevant data was extracted by two independent
investigators, and discrepancies between the two abstractors were
resolved by consensus, or re-evaluated by a third reviewer. The
validated Newcastle-Ottawa Scale instrument was adopted to
independently assess the quality of each study (15). A star system was applied to
evaluate nonrandomized studies regarding three criteria: Patient
selection (0–4 stars), comparability of study groups (0–2 stars)
and exposure or outcome assessment (0–3 stars). Studies that
achieved a rating of at least six stars were considered to be of
the highest quality (16).
The IIEF index covers five domains: Erectile
function (EF; six questions with a maximum score of 30),
intercourse satisfaction (IS; three questions with a maximum score
of 15), orgasmic function (OF), sexual drive (SD) and overall
satisfaction (OS) (two questions each with a maximum score of 10).
The FSFI index includes domains of sexual desire, arousal,
lubrication, orgasm, satisfaction and pain during sexual
intercourse. In case of vagueness or absence of outcomes in the
articles, the authors were contacted and related data was extracted
by consensus if the authors were unavailable.
Statistical analysis
The correlation of sexual function with AS was
evaluated using Review Manager meta-analysis software (version 5.2;
Cochrane Collaboration, Copenhagen, Denmark). Weighted mean
differences (MDs) and the 95% confidence interval (CI) were
calculated for continuous data. A fixed-effect model was applied to
combine these MDs to get an overall MD, also known as an effect
estimate. A random-effects model was used if heterogeneity across
studies was present. Heterogeneity was evaluated via the
χ2, τ2 and Higgins I2 tests, and a
P level <0.1 was considered significant. A Z score was adopted
to assess the overall effect with significance set at P<0.05.
Publication bias was evaluated by the Egger test and represented
graphically by funnel plots when the number of included trials was
≥5. To minimize the clinical heterogeneity, subgroup analyses for
male sexual function and female sexual function were conducted.
Results
Study selection
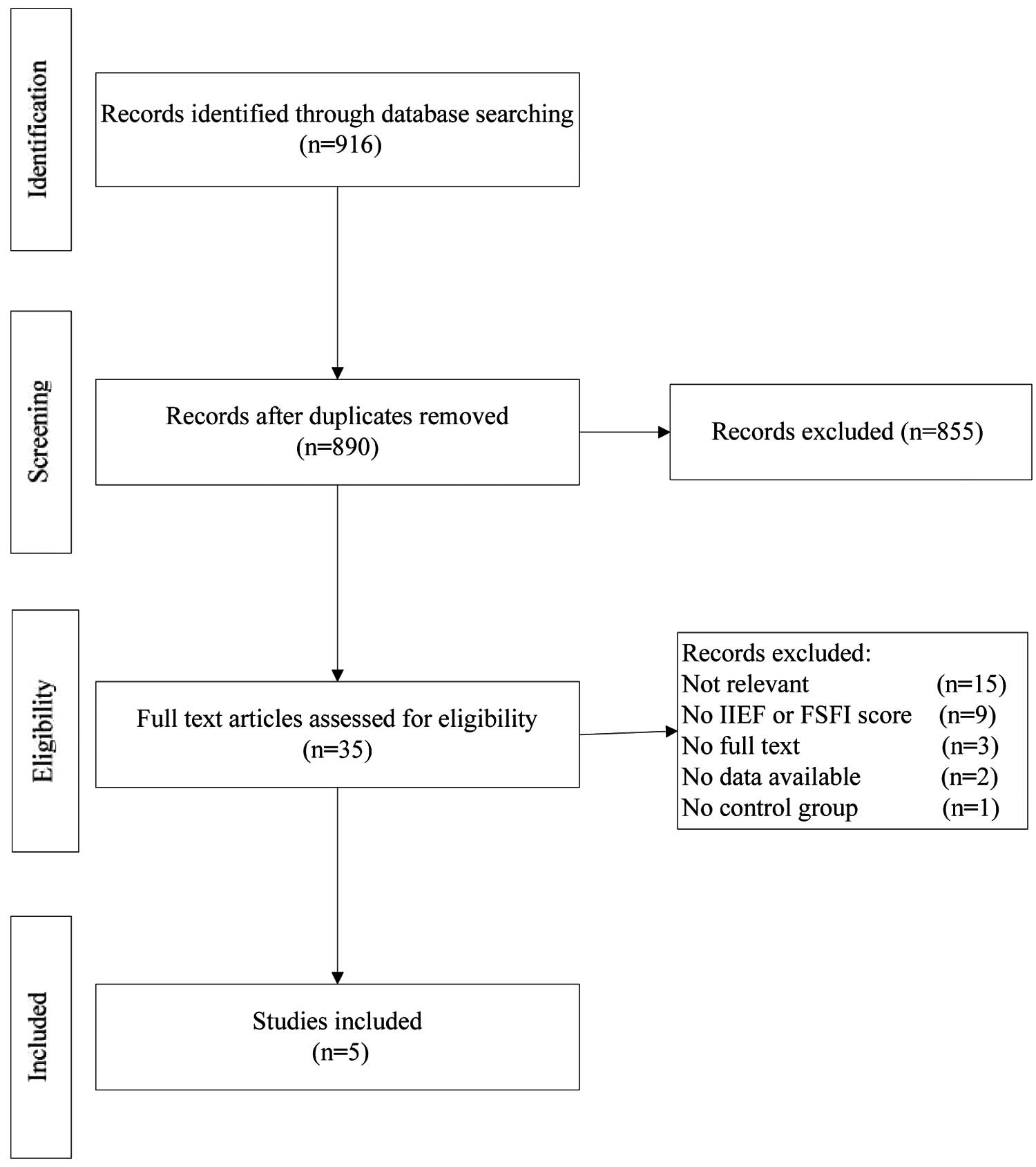
A flowchart of the study selection process is shown
in Fig. 1. One study in which the
data were presented as the median (minimum-maximum) was excluded
(17). According to the selection
criteria defined in Materials and methods, the meta-analysis
finally included five articles, involving a total of 484
participants of which 232 were patients with AS.
Study characteristics
Three studies assessed the impact of AS on male
sexual function, involving a total of 364 participants of which 172
were male patients with AS (9,18,19).
Two studies evaluated sexual function in female patients with AS,
involving a total of 120 participants of which 60 were female
patients with AS (20,21). The clinical and demographic
characteristics of the patients with AS and healthy controls are
summarized in Table I. The
included studies were published as full text between 2004 and 2013.
All studies originated from Turkey and were published in English.
The five included studies were of moderate to high quality.
 | Table IClinical and demographic
characteristics of the patients with AS and healthy controls. |
Table I
Clinical and demographic
characteristics of the patients with AS and healthy controls.
| Author (ref.) | Number of
participants | Age (years) | Characteristics of
patients with AS |
|---|
|
|
|
|---|
| Experimental | Control | Experimental | Control | BASFI | BASDAI | DD (years) | DMS (min) | ESR (mm/h) | CRP (mg/dl) | ASQoL |
|---|
| Pirildar (18) | 65 | 65 | 36.0±8.1 | 37.0±5.2 | 5.29±2.56 | Not reported | 12.2±6.4 | 220±122 | 54±23 | 21±15 | Not reported |
| Bal (9) | 37 | 67 | 42.8±10.8 | 43.6±5.9 | 3.8±2.9 | 3.92a | 10.0±9.0 | 4.7±5.8 | 31.5±19.6 | 13.1±16.5b | Not reported |
| Sariyildiz (19) | 70 | 60 | 36.4±7.4 | 35.2±7.7 | 3.1±2.0 | 2.3±1.9 | 9.9±6.9 | 28.2±33.3 | 18.7±13.7 | 4.5±5.5 | 6.7±5.2 |
| Demir (20) | 23 | 27 | 39.34±6.28 | 37.58±9.58 | 2.16±2.05 | 4.02±2.18 | 8.6±5.0 | Not reported | 24.04±19.19c | 1.48±4.16c | 7.33±4.26 |
| Sariyildiz
(21) | 37 | 33 | 34.1±7.0 | 33.5±6.2 | 3.9±2.3 | 4.5±1.9 | 8.6±7.4 | 32.9±32.4 | 16.5±8.9 | 4.2±6.3 | 6.8±3.1 |
Publication bias
As the number of included studies in each subgroup
was <5, funnel plot analysis and Egger tests were not conducted
to test publication bias.
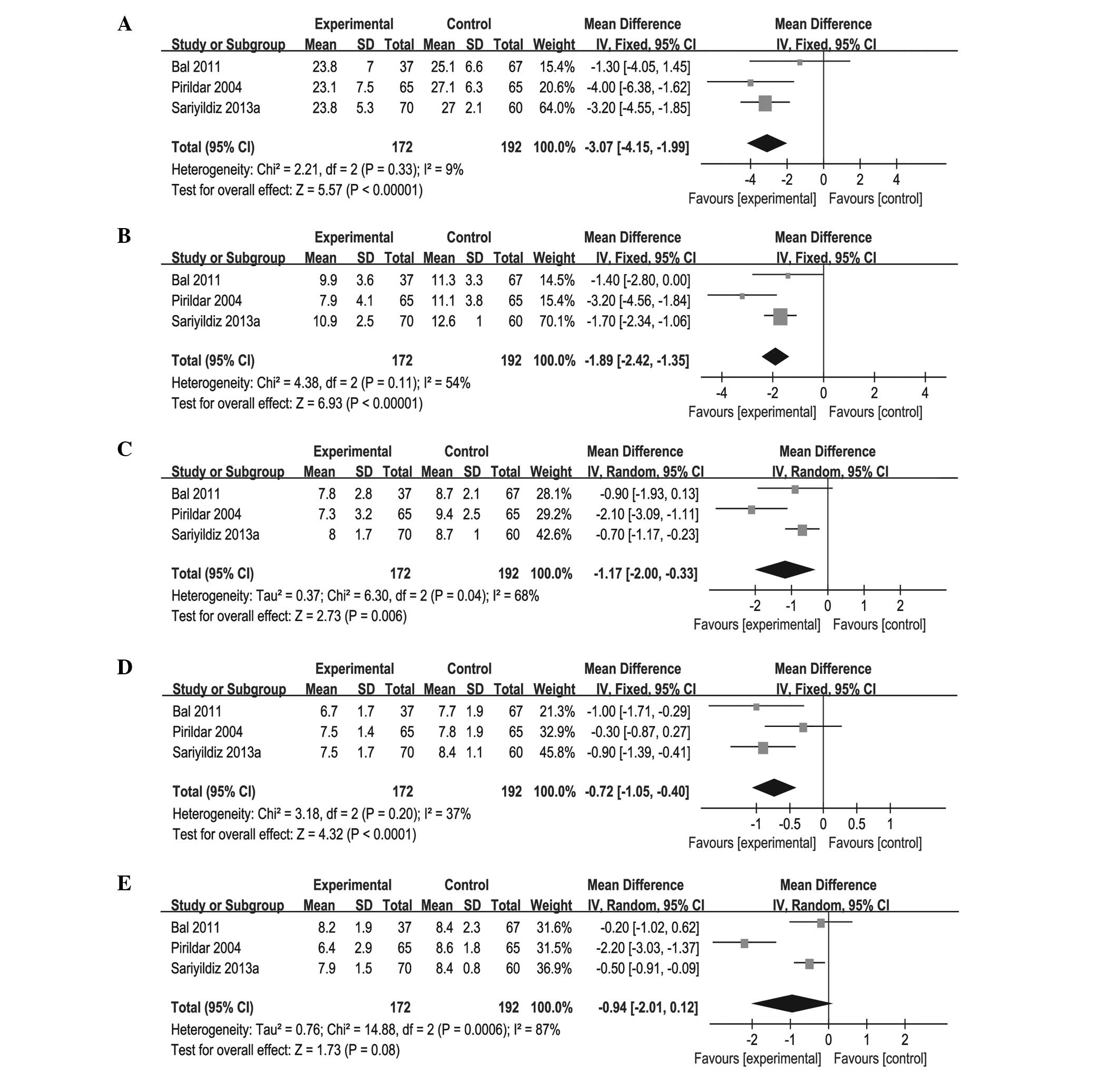
Male sexual function in AS patients and
controls
The number of trial participants with AS ranged from
37 to 70. The statistical heterogeneity among the studies was found
to be significant regarding the results for OF and OS (both
P<0.1). Consequently, the random-effects model was applied to
pool the results. The pooled results displayed statistical
significance with the exception of OS (P=0.08; MD=−0.94; 95% CI:
−2.01 to 0.12). Significant differences were identified in scores
of EF (P<0.00001; MD=−3.07; 95% CI: −4.15 to −1.99), OF
(P=0.006; MD=−1.17; 95% CI: −2.00 to −0.33), SD (P<0.0001;
MD=−0.72; 95% CI: −1.05 to −0.40) and IS (P<0.00001; MD=−1.89;
95% CI: −2.42 to −1.35; Fig. 2;
Table II).
| Table IIResults of meta-analysis for male
sexual function. |
Table II
Results of meta-analysis for male
sexual function.
| Heterogeneity | Test for overall
effect |
|---|
|
|
|
|---|
| Outcomes | χ2 | P-value | I2
(%) | Z | P-value | MD (95% CI) |
|---|
| EF | 2.21 | 0.33 | 9 | 5.57 | <0.00001 | −3.07 (−4.15,
−1.99) |
| IS | 4.38 | 0.11 | 54 | 6.93 | <0.00001 | −1.89 (−2.42,
−1.35) |
| OF | 6.30 | 0.04 | 68 | 2.73 | 0.006 | −1.17 (−2.00,
−0.33) |
| SD | 3.18 | 0.20 | 37 | 4.32 | 0.0001 | −0.72 (−1.05,
−0.40) |
| OS | 14.88 | 0.0006 | 87 | 1.73 | 0.08 | −0.94 (−2.01,
0.12) |
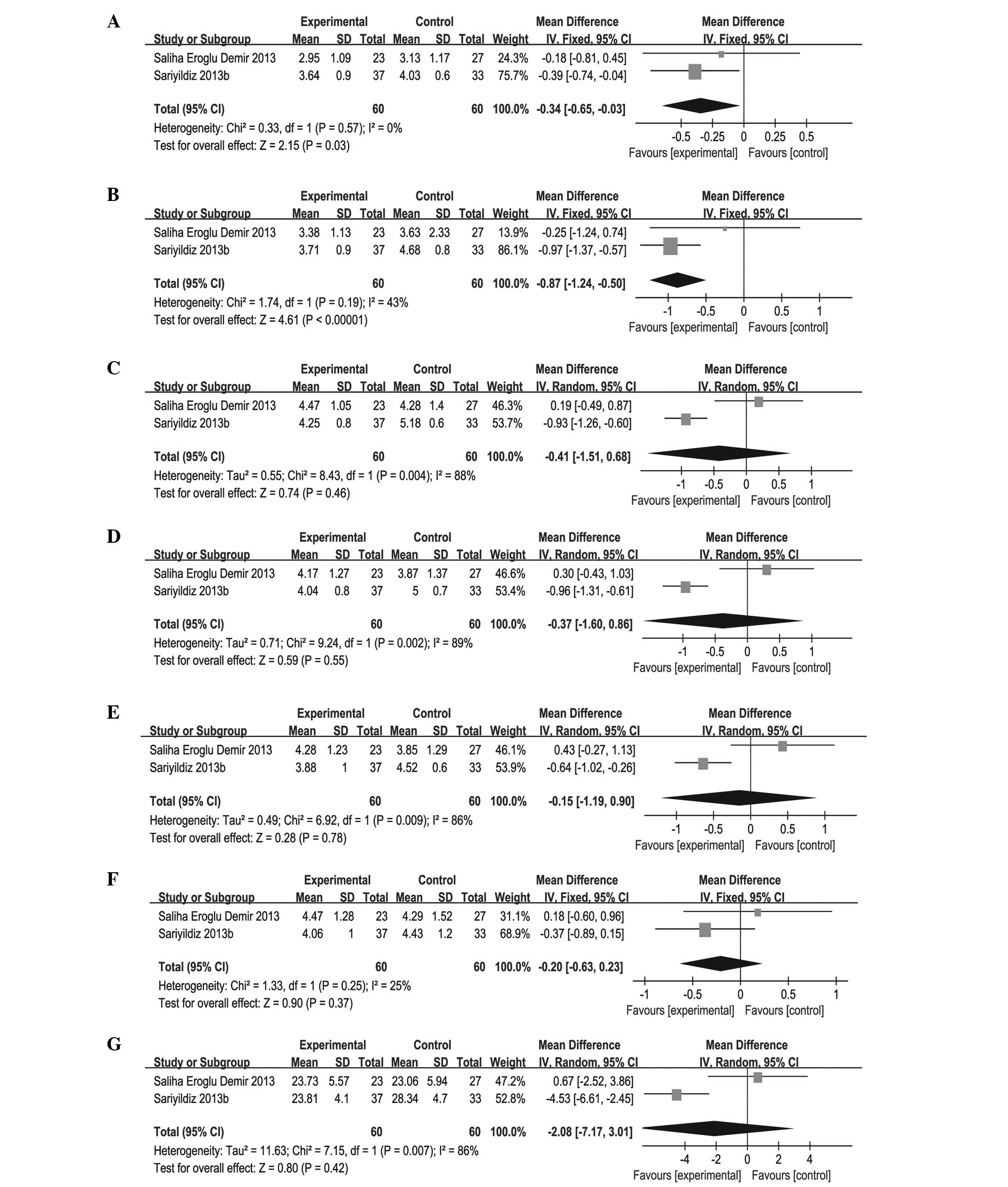
Female sexual function in AS patients and
controls
The number of trial participants with AS ranged from
23 to 37. There was significant heterogeneity in terms of the
domains for total FSFI, lubrication, orgasm and satisfaction (all
P<0.1). Accordingly, the random-effects model was applied to
combine these domains. The pooled results displayed no significant
difference between patients with AS and healthy controls in sexual
function, with the exception of desire (P=0.03; MD= −0.34; 95% CI:
−0.65 to −0.03) and arousal (P<0.00001; MD= −0.87; 95% CI: −1.24
to −0.50). However, no effects were found on total FSFI (P=0.42;
MD= −2.08; 95% CI: −7.17 to 3.01), lubrication (P=0.46; MD= −0.41;
95% CI: −1.51 to 0.68), orgasm (P=0.55; MD= −0.37; 95% CI: −1.60 to
0.86), satisfaction (P=0.78; MD= −0.15; 95% CI: −1.19 to 0.90) and
pain (P=0.37; MD= −0.20; 95% CI: −0.63 to 0.23; Fig. 3; Table III).
| Table IIIResults of meta-analysis for female
sexual function. |
Table III
Results of meta-analysis for female
sexual function.
| Heterogeneity | Test for overall
effect |
|---|
|
|
|
|---|
| Outcomes | χ2 | P-value | I2
(%) | Z | P-value | MD (95% CI) |
|---|
| Desire | 0.33 | 0.57 | 0 | 2.15 | 0.03 | −0.34 (−0.65,
−0.03) |
| Arousal | 1.74 | 0.19 | 43 | 4.61 | <0.00001 | −0.87 (−1.24,
−0.50) |
| Lubrication | 8.43 | 0.004 | 88 | 0.74 | 0.46 | −0.41 (−1.51,
0.68) |
| Orgasm | 9.24 | 0.002 | 89 | 0.59 | 0.55 | −0.37 (−1.60,
0.86) |
| Satisfaction | 6.92 | 0.009 | 86 | 0.28 | 0.78 | −0.15 (−1.19,
0.90) |
| Pain | 1.33 | 0.25 | 25 | 0.90 | 0.37 | −0.20 (−0.63,
0.23) |
| Total FSFI | 7.15 | 0.007 | 86 | 0.80 | 0.42 | −2.08 (−7.17,
3.01) |
Discussion
Increasing evidence indicates that sexual function
as an essential component of QoL is influenced by AS. To the best
of our knowledge, the present meta-analysis is the first
quantitative review analyzing the effect of AS on sexual function.
In the meta-analysis, it was found that AS had a certain impact on
the sexual function of patients, particularly that of male
patients. Five studies with a total of 484 Turkish participants
were included. In comparison with healthy controls, the male
patients with AS had a lower IIEF score in the domains of EF, OF,
SD and IS. The results demonstrated that male patients with AS had
a significant reduction in sexual function scores of EF (−3.07), OF
(−1.17), SD (−0.72) and IS (−1.89). Compared with healthy controls,
female patients with AS have a lower FSFI score in domains of
desire (−0.34) and arousal (−0.87).
AS may have a greater impact on male sexual function
than on that of females. The possible reasons are as follow.
Firstly, it has been reported that males are more often affected by
AS than females (22,23) and pertinent studies concerning
female sexual function are few. Secondly, female patients had a
shorter time of disease duration, older age of disease onset and
lower baseline C-reactive protein level (24). Among patients with longstanding AS,
there are differences in the clinical manifestations of AS between
the genders: Males have significantly more severe radiographic
changes and females may have more peripheral arthritis (25). The probability of enjoying sexual
activity is diminished in female patients with AS (26). Thirdly, sexual problems tend to be
more associated with physical health and aging among males than
females (27). In addition to
these reasons, neurotransmitters, psychosocial and interpersonal
factors (28), and the complexity
of sexual dysfunction in females (29) also contribute to the differences in
sexual response between males and females.
The pathogenesis of sexual problems in patients with
AS is complicated and multifactorial. Several underlying mechanisms
might be involved in the effect of AS on sexual function. Firstly,
tumor necrosis factor α (TNF-α) plays a pivotal role in the
pathogenesis of AS, and TNF-α concentrations are increased in the
circulation (30) and synovial
tissue (31) in patients with AS.
It has been shown that TNF-α acts as a potential candidate in the
pathophysiology of ED (32). In
addition, a pilot study demonstrated that anti-TNF-α therapy may
improve sexual dysfunction in male AS patients (33). Secondly, sexual problems in AS
patients might be associated with joint involvement, increased
disease activity, decreased functionality, declined health quality
and depression (34,35). Poor function, depression, greater
disease activity, unemployment and poor self-efficacy have been
found to be independently associated with a greater impact on the
sexual relationships of patients with AS (36). Bath AS mobility index, impaired
social functioning and Bath AS functionality index have been
identified to be the most significant causes of impaired sexual
function in Chinese AS patients (37). Finally, the toxicity of
disease-modifying antirheumatic drugs could contribute to sexual
problems. Case reports have shown that methotrexate is associated
with reduced libido, ED or impotence (38–40).
Several limitations of the present study should be
noted. Firstly, although the number of participants included in
this meta-analysis is larger than that in an individual study, the
sample size may be not large enough. In the current meta-analysis,
numerous studies were excluded due to inconformity with the IIEF or
FSFI scoring system. Secondly, all the participants were recruited
from Turkish populations. The association of sexual problems and AS
may differ in populations from other ethnic origins. Additionally,
there was a considerable heterogeneity in the subgroup of female
sexual function in AS. It is hypothesized that differences in the
quality of studies, participant characteristics and disease
activity are responsible for the heterogeneity. In view of this,
all of the conclusions require careful consideration.
In conclusion, there is an association between
sexual problems and AS. AS appears to have a greater influence on
the sexual function of males than that of females. Early diagnosis
of sexual dysfunction is essential for AS patients with sexual
problems. Therefore, physicians should be aware of the effect of AS
on sexual health and it is recommended that special attention is
given to all domains of life, not only disease activity and
physical function.
Acknowledgements
The authors acknowledge the authors of the original
studies included in the meta-analysis.
References
|
1
|
Braun J and Sieper J: Ankylosing
spondylitis. Lancet. 369:1379–1390. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Keat A: Sex and the spondylitic.
Rheumatology (Oxford). 48:1337–1338. 2009. View Article : Google Scholar
|
|
3
|
Ozgül A, Peker F, Taskaynatan MA, et al:
Effect of ankylosing spondylitis on health-related quality of life
and different aspects of social life in young patients. Clin
Rheumatol. 25:168–174. 2006. View Article : Google Scholar
|
|
4
|
Hill J, Bird H and Thorpe R: Effects of
rheumatoid arthritis on sexual activity and relationships.
Rheumatology (Oxford). 42:280–286. 2003. View Article : Google Scholar
|
|
5
|
Tristano AG: The impact of rheumatic
diseases on sexual function. Rheumatol Int. 29:853–860. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Gordon D, Beastall GH, Thomson JA and
Sturrock RD: Androgenic status and sexual function in males with
rheumatoid arthritis and ankylosing spondylitis. Q J Med.
60:671–679. 1986.PubMed/NCBI
|
|
7
|
Chung SD, Chen YK, Kang JH, Keller JJ,
Huang CC and Lin HC: Population-based estimates of medical
comorbidities in erectile dysfunction in a Taiwanese population. J
Sex Med. 8:3316–3324. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Chung SD, Chen YK, Liu SP and Lin HC:
Association between ED in ankylosing spondylitis: a
population-based study. Int J Impot Res. 25:229–233. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bal S, Bal K, Turan Y, Deniz G, Gürgan A,
Berkit IK and Sendur OF: Sexual functions in ankylosing
spondylitis. Rheumatol Int. 31:889–894. 2011. View Article : Google Scholar
|
|
10
|
Moher D, Liberati A, Tetzlaff J and Altman
DG; PRISMA Group. Preferred reporting items for systematic reviews
and meta-analyses: the PRISMA statement. Ann Intern Med.
151:264–269. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Stroup DF, Berlin JA, Morton SC, et al:
Meta-analysis of observational studies in epidemiology: a propoal
for reporting. Meta-analysis of observational studies in
Epidemiology (MOOSE) group. JAMA. 283:2008–2012. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
van der Linden S, Valkenburg HA and Cats
A: Evaluation of diagonstic criteria for ankylosing spondylitis. A
proposal for modification of the New York criteria. Arthritis
Rheum. 27:361–368. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rosen RC, Riley A, Wagner G, Osterloh IH,
Kirkpatrick J and Mishra A: The international index of erectile
function (IIEF): a multidimensional scale for assessment of
erectile dysfunction. Urology. 49:822–830. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Rosen R, Brown C, Heiman J, et al: The
female sexual function index (FSFI): a multidimensional self-report
instrument for the assessment of female sexual function. J Sex
Marital Ther. 26:191–208. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wells GA, Shea B, O’Connell D, Peterson J,
Welch V, Losos M and Tugwell P: The Newcastle-Ottawa scale (NOS)
for assessing the quality of nonrandomised studies in
meta-analyses. Ottawa Health Research Institute; 2000
|
|
16
|
Mahid SS, Minor KS, Soto RE, Hornung CA
and Galandiuk S: Smoking and inflammatory bowel disease: a
meta-analysis. Mayo Clin Proc. 81:1462–1471. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Rezvani A, Ök Ş and Demir SE: Assessment
of sexual functions in male patients with ankylosing spondylitis
compared with healthy controls. Turk J Rheumatol. 27:233–240.
2012.
|
|
18
|
Pirildar T, Müezzinoğlu T and Pirildar S:
Sexual function in ankylosing spondylitis: a study of 65 men. J
Urol. 171:1598–1600. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sariyildiz MA, Batmaz I, Dilek B, et al:
Relationship of the sexual functions with the clinical parameters,
radiological scores and the quality of life in male patients with
ankylosing spondylitis. Rheumatol Int. 33:623–629. 2013. View Article : Google Scholar
|
|
20
|
Demir SE, Rezvani A and Ok S: Assessment
of sexual functions in female patients with ankylosing spondylitis
compared with healthy controls. Rheumatol Int. 33:57–63. 2013.
View Article : Google Scholar
|
|
21
|
Sariyildiz MA, Batmaz I, Inanir A, et al:
The impact of ankylosing spondylitis on female sexual functions.
Int J Impot Res. 25:104–108. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Feldtkeller E, Khan M, van der Heijde D,
van der Linden S and Braun J: Age at disease onset and diagnosis
delay in HLA-B27 negative vs. positive patients with ankylosing
spondylitis. Rheumatol Int. 23:61–66. 2003.PubMed/NCBI
|
|
23
|
van der Linden SM, Valkenburg HA, de Jongh
BM and Cats A: The risk of developing ankylosing spondylitis in
HLA-B27 positive individuals. A comparison of relatives of
spondylitis patients with the general population. Arthritis Rheum.
27:241–249. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
van der Horst-Bruinsma IE, Zack DJ,
Szumski A and Koenig AS: Female patients with ankylosing
spondylitis: analysis of the impact of gender across treatment
studies. Ann Rheum Dis. 72:1221–1224. 2013. View Article : Google Scholar
|
|
25
|
Lee W, Reveille JD, Davis JC Jr, Learch
TJ, Ward MM and Weisman MH: Are there gender differences in
severity of ankylosing spondylitis? Results from the PSOAS cohort.
Ann Rheum Dis. 66:633–638. 2007. View Article : Google Scholar
|
|
26
|
Elst P, Sybesma T, van der Stadt RJ, Prins
AP, Muller WH and den Butter A: Sexual problems in rheumatoid
arthritis and ankylosing spondylitis. Arthritis Rheum. 27:217–220.
1984. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Laumann EO, Nicolosi A, Glasser DB, Paik
A, Gingell C, Moreira E and Wang T; GSSAB Investigators’ Group.
Sexual problems among women and men aged 40–80 y: prevalence and
correlates identified in the Global Study of Sexual Attitudes and
Behaviors. Int J Impot Res. 17:39–57. 2004. View Article : Google Scholar
|
|
28
|
Basson R, Berman J, Burnett A, et al:
Report of the international consensus development conference on
female sexual dysfunction: definitions and classifications. J Urol.
163:888–893. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Basson R, Leiblum S, Brotto L, et al:
Definitions of women’s sexual dysfunction reconsidered: advocating
expansion and revision. J Psychosom Obstet Gynaecol. 24:221–229.
2003. View Article : Google Scholar
|
|
30
|
Gratacós J, Collado A, Filella X, et al:
Serum cytokines (IL-6, TNF-α, IL-1β and IFN-γ) in ankylosing
spondylitis: a close correlation between serum IL-6 and disease
activity and severity. Br J Rheumatol. 33:927–931. 1994. View Article : Google Scholar
|
|
31
|
Braun J, Bollow M, Neure L, et al: Use of
immunohistologic and in situ hybridization techniques in the
examination of sacroiliac joint biopsy specimens from patients with
ankylosing spondylitis. Arthritis Rheum. 38:499–505. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Carneiro FS, Webb RC and Tostes RC:
Emerging role for TNF-α in erectile dysfunction. J Sex Med.
7:3823–3834. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Oh JS, Heo HM, Kim YG, Lee SG, Lee CK and
Yoo B: The effect of anti-tumor necrosis factor agents on sexual
dysfunction in male patients with ankylosing spondylitis: a pilot
study. Int J Impot Res. 21:372–375. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Cakar E, Dincer U, Kiralp MZ, et al:
Sexual problems in male ankylosing spondylitis patients:
relationship with functionality, disease activity, quality of life
and emotional status. Clin Rheumatol. 26:1607–1613. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Dincer U, Cakar E, Kiralp MZ and Dursun H:
Assessment of sexual dysfunction in male patients with ankylosing
spondylitis. Rheumatol Int. 27:561–566. 2007. View Article : Google Scholar
|
|
36
|
Healey EL, Haywood KL, Jordan KP, Garratt
AM, Ryan S and Packham JC: Ankylosing spondylitis and its impact on
sexual relationships. Rheumatology. 48:1378–1381. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Shen B, Zhang A, Liu J, Da Z, Xu X and Gu
Z: A primary analysis of sexual problems in Chinese patients with
ankylosing spondylitis. Rheumatol Int. 33:1429–1435. 2013.
View Article : Google Scholar
|
|
38
|
Wylie G, Evans CD and Gupta G: Reduced
libido and erectile dysfunction: rarely reported side-effects of
methotrexate. Clin Exp Dermatol. 34:e2342009. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Aguirre MA, Vélez A, Romero M and
Collantes E: Gynecomastia and sexual impotence associated with
methotrexate treatment. J Rheumatol. 29:1793–1794. 2002.PubMed/NCBI
|
|
40
|
Thomas E, Koumouvi K and Blotman F:
Impotence in a patient with rheumatoid arthritis treated with
methotrexate. J Rheumatol. 27:1821–1822. 2000.PubMed/NCBI
|