Introduction
Multiple myeloma (MM) is caused by the uncontrolled
proliferation of monoclonal plasma cells, resulting in the
production of monoclonal immunoglobulin (Ig) and substantial
immunosuppression and endorgan damage, including direct and
indirect effects on the blood, skeleton, and kidneys (1).
Recent treatment options for MM have led to improved
response rates and increased survival. However, MM is a
heterogeneous disease with variable disease course and response to
therapy, and a survival outcome that ranges from less than 1 year
to more than 10 years (1). Various
clinical characteristics, including age and type of M-component,
have been identified to predict the disease course as well as
outcome in patients with myeloma. In the past ten years, many
factors have been found to impact the prognosis, including stage
according to the International Staging System (ISS) (2), renal function (3), cytogenetics (4) and extramedullary plasmacytoma (EMP)
(5). It is extremely important for
treatment strategies to include the evaluation of prognostic
factors and risk stratification (6).
The present study relates to a special series of
patients with MM. These patients were found to have two different
Ig λ light chains by immunofixation electrophoresis (IFE) at
diagnosis, and they had certain similarities in their clinical
characteristics. However, to the best of our knowledge, there have
been no previous reports associated with such patients. Therefore,
the characteristics of these patients were summarized
retrospectively and their prognosis was analyzed.
Patients and methods
Patients
A total of 483 patients were diagnosed with MM in
Beijing Chaoyang Hospital (Beijing, China) from January 2006 to
June 2012. Among them, 26 patients (5.4%) had two different λ light
chains when analyzed by IFE. Data were collected from the medical
records of such patients. All the patients received baseline
evaluations prior to treatment which included physical examination,
blood counts, hepatic and renal function tests, bone marrow
aspirate and biopsy, serum and urine protein electrophoreses, and
quantitation of serum Igs and urinary light chains, serum β2
microglobulin and C-reactive protein. A chest X-ray and a complete
radiological bone survey were also performed. Detection by
fluorescence in situ hybridization (FISH) of t(4;14),
t(14;16) and del17p was completed prior to treatment.
Treatment strategies
The patients received various treatment strategies.
Some were treated with combination regimens including the PD ± T
regimen (bortezomib and dexamethasone with or without thalidomide)
or the PAD regimen (bortezomib, doxorubicin and dexamethasone).
Other patients were treated with conventional regimens without
bortezomib including the VAD regimen (vindesine, doxorubicin and
dexamethasone), the TAD regimen (thalidomide, doxorubicin and
dexamethasone) or the TD ± CTX regimen (thalidomide, dexamethasone
with or without cyclophosphamide). The patients who were suitable
for autologous stem cell transplantation (SCT) received autologous
SCT. Local radiotherapy was used for the patients with
extramedullary plasmacytoma (EMP) following total therapy.
In addition to antimyeloma treatment, all patients
received intensive supportive care including intravenous hydration,
alkalinization of urine, correction of hypercalcemia and the
discontinuation of all potential nephrotoxic agents. Renal dialysis
was offered to patients with severe renal dysfunction.
Statistical analysis
All statistical analyses were performed with SPSS
13.0 statistical software (SPSS, Inc., Chicago, IL, USA). The
efficacy was evaluated by Chi-square test. Survival analysis was
performed with a life-table and Kaplan-Meier survival curve. A
P-value of <0.05 was considered significant for all statistical
calculations. Response was evaluated following the international
uniform response criteria for multiple myeloma defined by the
International Myeloma Working Group (7). The main indices were overall remission
(OR), complete remission (CR), very good partial remission (VGPR)
and partial remission (PR) rates, in which OR is equal to the sum
of CR, VGPR and PR. Overall survival (OS) and duration of remission
(DOR) were used to establish the durability of response in this
study. The OS is the duration from diagnosis of the disease to
mortality (regardless of cause of mortality) or loss to follow-up.
The DOR is the duration from the first observation of PR to the
time of disease progression or mortality from a cause other than
disease progression (regardless of the nature of this cause),
whichever occurred first.
Results
Patient characteristics
There were 23 males and 3 females with a median age
of 59 years (range, 48–76 years) in this study (Table I). All the patients were found to
have two different λ light chains following IFE tests (Fig. 1). Among these patients, IgG MM was
found in 14 patients (53.8%), IgA in 7 patients (26.9%) and IgD in
5 patients (19.2%). Seventeen patients (65.4%) had renal
dysfunction, 12 patients (46.2%) in the group received hemodialysis
and 10 patients (38.5%) had extramedullary plasmacytoma (EMP) at
diagnosis. Twenty-two patients (84.6%) had stage III disease
according to the ISS. Five patients had hypercalcemia at diagnosis.
Ten patients (38.5%) had t(4;14), t(14;16) or del17p abnormalities
by FISH analysis. Other characteristics are presented in Table I.
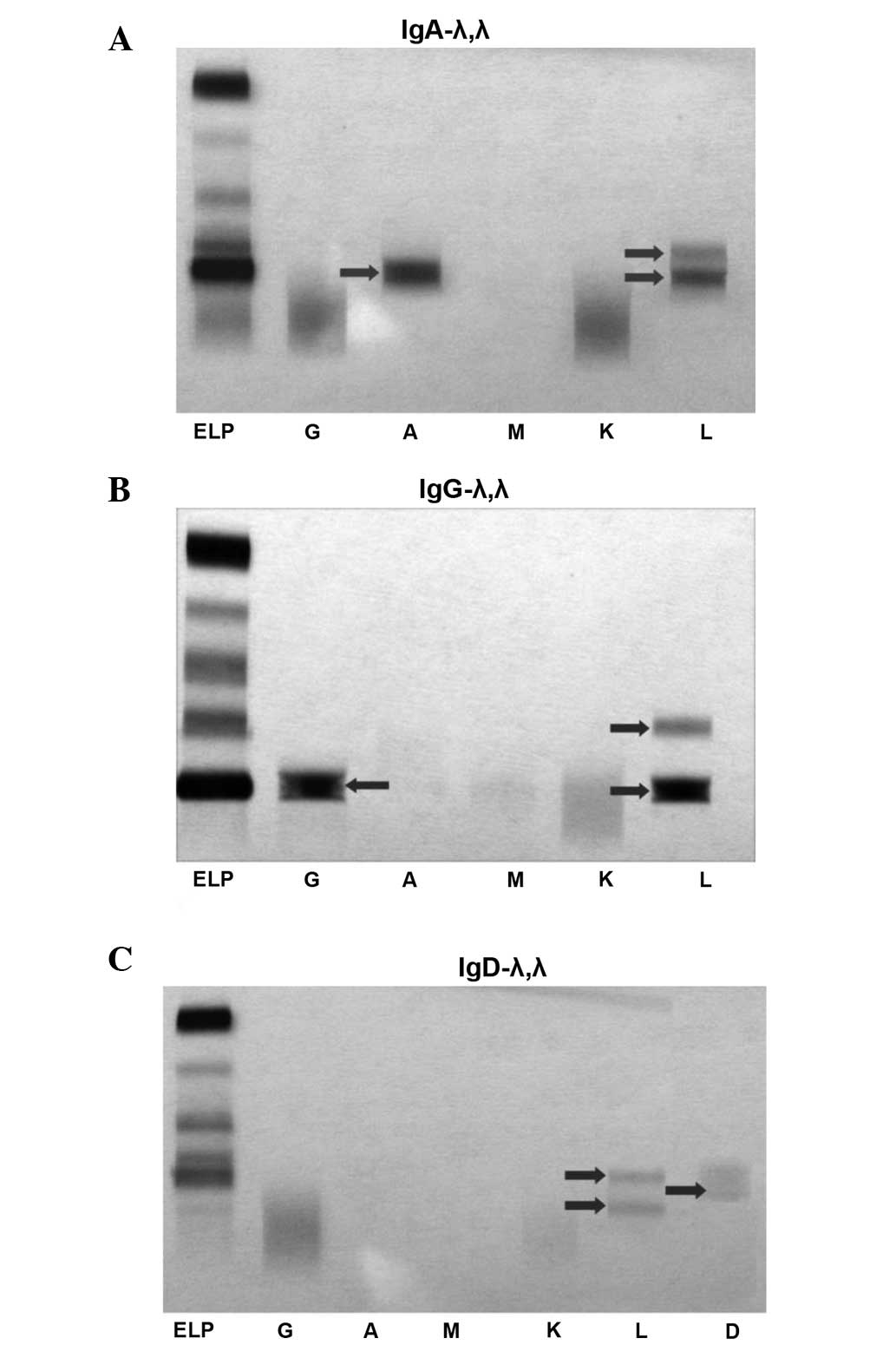 | Figure 1.Two bands for the immunoglobulin (Ig)
λ light chain by immunofixation electrophoresis (IFE). (A) IgA-λ,λ,
(B) IgG-λ,λ and (C) IgD-λ,λ. Lane ELP, serum protein
electrophoresis; lane G, IgG; lane A, IgA; lane M, IgM; lane K, κ
light chain; lane L, λ light chain; lane D, IgD. |
 | Table I.Characteristics of the patients with
multiple myeloma at diagnosis. |
Table I.
Characteristics of the patients with
multiple myeloma at diagnosis.
| Characteristics | Values |
|---|
| Number of
patients | 26 |
| Gender, n (%) |
|
| Male | 23 (88.5) |
|
Female | 3 (11.5) |
| Median age, years
(range) | 59 (48–76) |
| Type of M-component,
n (%) |
|
| IgG-λ,
λ | 14 (53.8) |
| IgA-λ,
λ | 7 (26.9) |
| IgD-λ,
λ | 5 (19.2) |
| Durie-Salmen stage, n
(%) |
|
| IIa | 2 (7.7) |
| IIIa | 7 (26.9) |
| IIIb | 17 (65.4) |
| ISS stage, n (%) |
|
| I | 1 (3.8) |
| II | 3 (11.5) |
| III | 22 (84.6) |
| WBC
(×109/l), median (range) | 5.6 (2.2–7.9) |
| Hb (g/l), median
(range) | 68 (52–119) |
| PLT
(×109/l), median (range) | 89 (43–201) |
| Serum album (g/l),
median (range) | 24 (17–38) |
| Serum creatinine
(µmol/l), median (range) | 342 (67–1455) |
| Plasma cell (BM, %),
median (range) | 41.5 (11.0–85.0) |
| Extramedullary
plasmacytoma, n (%) | 10 (38.5) |
| Hypercalcemia n
(%) | 5 (19.2) |
| Abnormalities by
FISH, n (%) |
|
|
del17p | 2 (7.7) |
|
t(14;16) | 3 (11.5) |
|
t(4;14) | 5 (19.2) |
| None of
the above | 16 (61.5) |
| Serum β2
microglobulin (mg/l), median (range) | 6.0 (3.1–18.6) |
Response analysis
Three patients (11.5%) achieved CR, 6 patients
(23.1%) VGPR, 6 patients (23.1%) PR and the OR rate was 57.7%
(15/26). Fourteen patients received chemotherapy with bortezomib
and five of them continued to receive autologous SCT. Twelve
patients received chemotherapy without bortezomib and four of them
proceeded to receive autologous SCT. The results are presented in
Table II.
| Table II.Efficacy of the different treatment
strategies. |
Table II.
Efficacy of the different treatment
strategies.
| Regimen | No. | CR (n) | VGPR (n) | PR (n) | OR rate (%) |
|---|
| Bortezomib without
auto-SCT | 9 | 1 | 3 | 2 |
66.7 |
| Bortezomib with
auto-SCT | 5 | 2 | 2 | 1 |
100.0 |
| No bortezomib without
auto-SCT | 8 | 0 | 0 | 2 |
25.0 |
| No bortezomib with
auto-SCT | 4 | 0 | 1 | 1 |
50.0 |
| Total | 26 | 3 | 6 | 6 |
57.7 |
The OR rate of the 14 patients who received
chemotherapy with bortezomib was superior to that of the 12
patients who received chemotherapy without bortezomib (78.6% vs.
33.3%, respectively; P<0.05). The OR rate of the 9 patients who
received autologous SCT was superior to that of the 17 patients who
did not receive autologous SCT (77.8% vs. 47.1%, respectively;
P<0.05).
Ten patients (10/26, 38.5%) had t(4;14), t(14;16) or
del17p cytogenetic abnormalities by FISH in this study. Seven of
them received chemotherapy with bortezomib and two of them received
autologous SCT. Their OR rate was 60.0% and the OR rate of the
patients without abnormality by FISH was 56.3% (P>0.05).
Among the patients with EMP (n=10), five received
chemotherapy with bortezomib and one received autologous SCT. One
of these patients achieved CR, two achieved VGPR and two achieved
PR. There was no statistically significant difference on the OR
rate between the patients with EMP and the patients without EMP
(50.0% vs. 62.5%, respectively; P>0.05).
Prognosis
The endpoint of follow-up was patient mortality,
loss to follow-up or October 31, 2012. No case in the study was
lost during the period of follow-up. At the time of analysis, 6/26
patients (23.1%) were alive, with a median follow-up of 24 months.
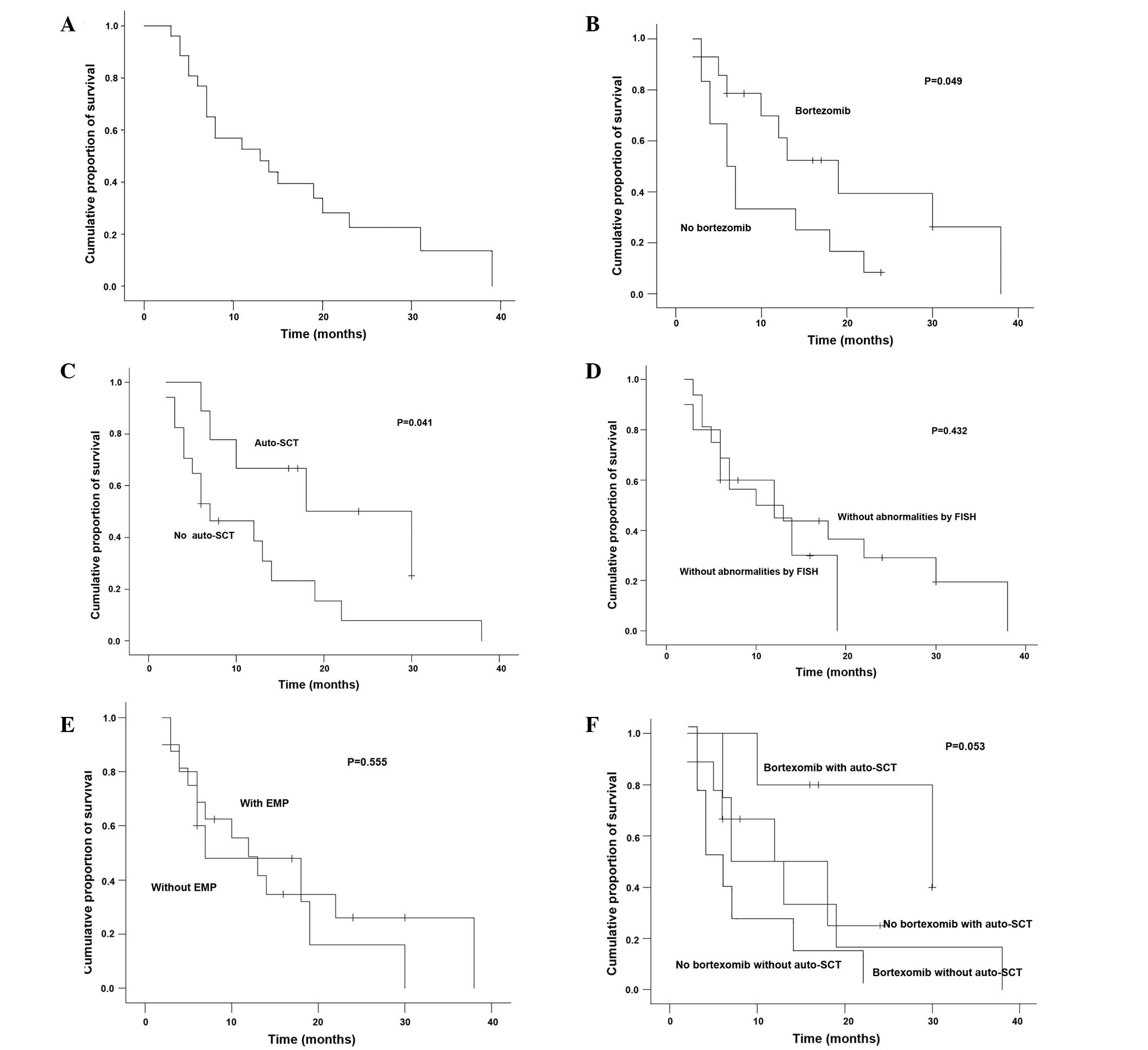
The median OS was 12.6 months (range, 2–38 months; Fig. 2A). The patients who received
chemotherapy with bortezomib had a significantly longer median OS
as compared with the patients who received chemotherapy without
bortezomib (19 vs. 6 months, respectively; P=0.049; Fig. 2B). The patients who received
autologous SCT (n=9) also had a significantly longer median OS as
compared with the patients who did not receive autologous SCT (18
vs. 7 months, respectively; P=0.041; Fig. 2C). However, the patients with
abnormalities by FISH had similar median OS as compared with the
patients without abnormalities by FISH (18 vs. 10 months,
respectively; P=0.432; Fig. 2D).
There was no statistically significant difference on median OS
between the patients with EMP and those without EMP (7 vs. 12
months, respectively; P=0.555; Fig.
2E). From Fig. 2F, it may be
observed that the patients who received chemotherapy combined with
bortezomib and autologous SCT had a longer median OS, the patients
who received only chemotherapy without bortezomib had a shorter
median OS and other patients had an intermediate OS. However, there
was no statistical difference among these differently treated
patients (P=0.053).
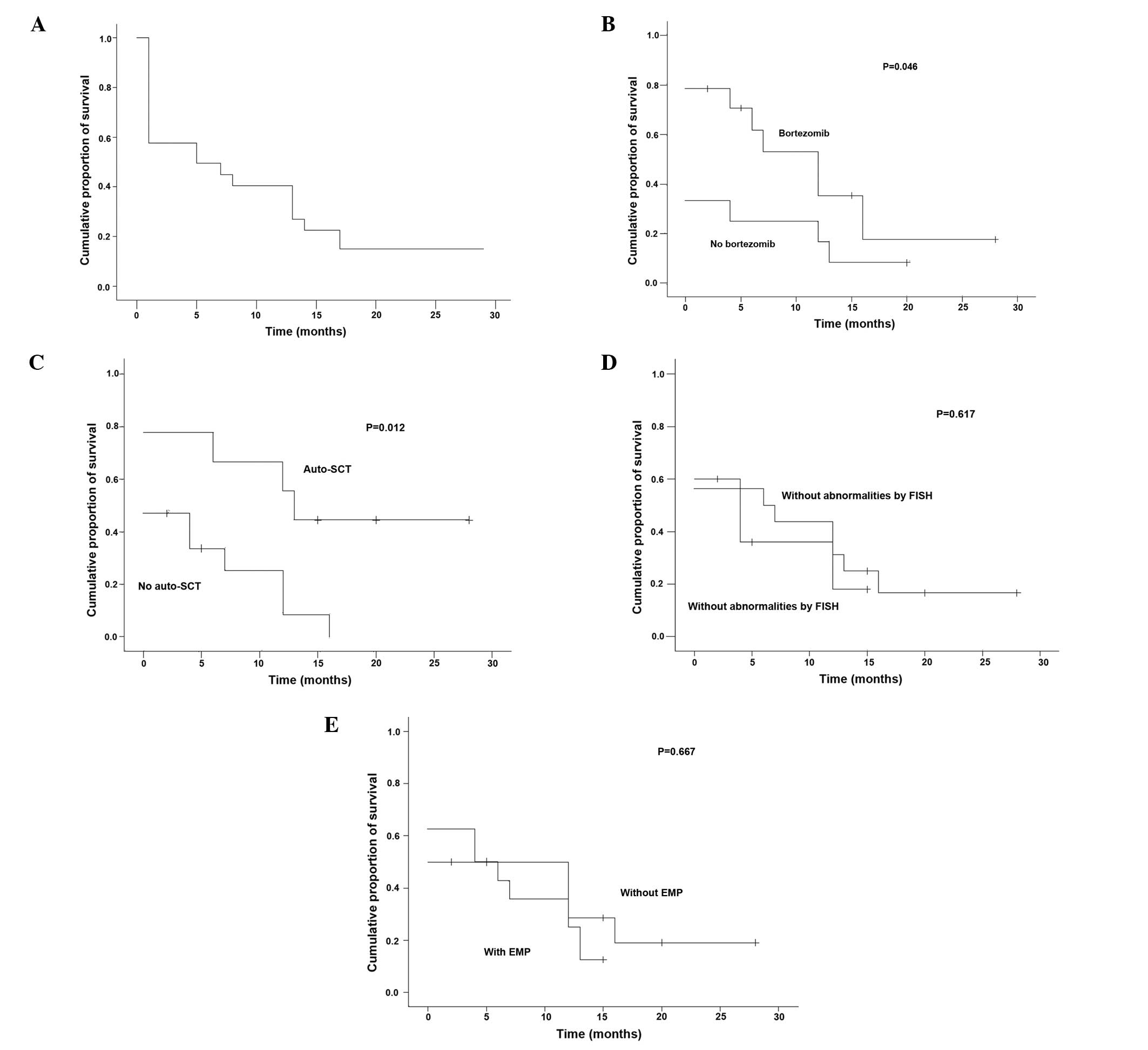
The median DOR was 5 months (range, 0–28 months)
(Fig. 3A). The patients who received
bortezomib or autologous SCT had a significantly longer median DOR
than those who did not (P=0.046 and P=0.012, respectively; Table III, Fig.
3B and C). However, the patients with abnormalities by FISH had
a median DOR similar to that of the patients without abnormalities
by FISH, and there was no statistically significant difference in
median DOR between the patients with EMP and the patients without
EMP (P=0.617 and P=0.667, respectively; Table III, Fig.
3D and E).
| Table III.DOR of the patients affected by
different factors. |
Table III.
DOR of the patients affected by
different factors.
| Factor | Number of
patients | Median DOR
(months) | P-value |
|---|
| Bortezomib |
|
|
|
| Yes | 14 | 11 | 0.046 |
| No | 12 | 4 |
|
| Auto-SCT |
|
|
|
| Yes | 9 | 16 | 0.012 |
| No | 17 | 4.5 |
|
| Abnormality by
FISH |
|
|
|
| Yes | 10 | 6 | 0.617 |
| No | 16 | 9 |
|
| EMP |
|
|
|
| Yes | 10 | 6.5 | 0.667 |
| No | 16 | 9 |
|
Discussion
In the present study, a series of patients with MM
who were revealed to have rare double M-components by IFE were
investigated. The two λ light chains, as shown in Fig. 1, had different velocities during IFE;
therefore, they should rationally have different molecular weights.
It may be concluded that the two chains are different. It is
noteworthy that the light chains of all the patients are λ light
chains. Such patients had a very poor prognosis with a median OS
only 12.6 months and, therefore, it is recommended that these
patients should receive particular attention.
Renal dysfunction is a common symptom that
negatively affects the quality of life of the patient and their
prognosis. With the clinical application of novel strategies and
agents such as autologous SCT and bortezomib, this situation has
improved (8). In the present study,
17 patients (65.4%) had renal dysfunction and 12 patients (46.2%)
in the group received hemodialysis. The rates of renal dysfunction
and severe renal dysfunction were higher than those reported in
previous studies (3,8). The pathogenesis is unknown. The
pathophysiology of the most common types of renal injury observed
in myeloma is closely linked to the renal handling of light chains
(9). It may be concluded that the
renal function of the patients is likely to be affected severely by
the presence of two different λ light chains.
EMP is not a rare manifestation of MM and its
incidence is 9–13% (5,10). Notably, IgD MM is associated with a
higher frequency of EMP. In a study by Bladé et al, EMP was
reported in 15–20% of patients at diagnosis and in an additional
15% of patients during follow-up (11). Another study described a series of 72
patients with MM aged <40 years with a high incidence of EMP
(12). A high incidence of EMP may
be associated with younger age or IgD MM. In the present study, the
median age of all patients was 59 years old and IgD MM accounted
for 19.2% (5/26) of cases. However, the incidence of EMP at
diagnosis was 38.5% (10/26). This observation may explain the
interesting phenomenon that MM in patients with two different λ
light chains appears to have a stronger extramedullary invasive
ability.
The patients in the present study had a poor
prognosis with a median OS of 12.6 months. Renal dysfunction, EMP
and abnormalities by FISH are all known to be poor prognostic
factor (3,5,8,13). However, neither EMP nor the
abnormalities identified by FISH were observed to affect the
prognosis in the present study. The identification of two different
λ light chains by IFE at diagnosis could be an independent poor
prognostic factor. To the best of our knowledge, no relevant
studies concerning the therapy of such patients have been reported
previously. In the present study, bortezomib and autologous SCT
were found to be superior to conventional chemotherapy in the
treatment of these patients.
In conclusion, patients with MM and two different λ
light chains as identified by IFE may be a special group that is
affected by a high incidence of renal dysfunction and EMP. They
have a poor prognosis, and novel therapies including bortezomib and
autologous SCT may increase the chances of survival of such
patients.
References
|
1
|
Rajkumar SV: Treatment of multiple
myeloma. Nat Rev Clin Oncol. 8:479–491. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Greipp PR, San Miguel J, Durie BG, Crowley
JJ, Barlogie B, Bladé J, et al: International staging system for
multiple myeloma. J Clin Oncol. 23:3412–3420. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Morabito F, Gentile M, Ciolli S, et al:
Safety and efficacy of bortezomib-based regimens for multiple
myeloma patients with renal impairment: a retrospective study of
Italian Myeloma Network GIMEMA. Eur J Haematol. 84:223–228. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Liu N, Zhou H, Yang G, Geng C, Jian Y, Guo
H and Chen W: Retrospective analysis of genetic abnormalities and
survival in 131 patients with multiple myeloma. Oncol Lett.
9:930–936. 2015.PubMed/NCBI
|
|
5
|
Varettoni M, Corso A, Pica G, et al:
Incidence, presenting features and outcome of extramedullary
disease in multiple myeloma: a longitudinal study on 1003
consecutive patients. Ann Oncol. 21:325–330. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Fonseca R, Monge J and Dimopoulos MA:
Staging and prognostication of multiple myeloma. Expert Rev
Hematol. 7:21–31. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Durie BG, Harousseau JL, Miguel JS, et al:
International Myeloma Working Group: International uniform response
criteria for multiple myeloma. Leukemia. 20:1467–1473. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yang GZ and Chen WM: Bortezomib-based
regimen for the treatment of 110 multiple myeloma patients.
Zhonghua Yi Xue Za Zhi. 90:2671–2674. 2010.[(In Chinese)].
PubMed/NCBI
|
|
9
|
Dimopoulos MA, Kastritis E, Rosinol L,
Bladé J and Ludwig H: Pathogenesis and treatment of renal failure
in multiple myeloma. Leukemia. 22:1485–1493. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Chen HF, Wu TQ, Li ZY, et al:
Extramedullary plasmacytoma in the presence of multiple myeloma:
clinical correlates and prognostic relevance. Onco Targets Ther.
5:329–334. 2012.PubMed/NCBI
|
|
11
|
Bladé J, Lust JA and Kyle RA:
Immunoglobulin D multiple myeloma: presenting features, response to
therapy, and survival in a series of 53 cases. J Clin Oncol.
12:2398–2404. 1994.PubMed/NCBI
|
|
12
|
Bladé J, Kyle RA and Greipp P: Presenting
features and prognosis in 72 patients with multiple myeloma who
were younger than 40 years. Br J Haematol. 93:345–351. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Dimopoulos M, Kyle R, Fermand JP, et al:
International Myeloma Workshop Consensus Panel 3: Consensus
recommendations for standard investigative workup: report of the
International Myeloma Workshop Consensus Panel 3. Blood.
117:4701–4705. 2011. View Article : Google Scholar : PubMed/NCBI
|