Introduction
The prevalence of chronic kidney disease (CKD) is
high in the general population and increases significantly with age
(1). As reported in the National
Health and Nutrition Examination Survey, the prevalence of a
reduced estimated glomerular filtration rate (GFR; <60
ml/min/1.73 m2) was 37.8% among participants aged >70
years (1). However, the clinical
implications of a low GFR in elderly individuals remains
controversial, particularly among the Chinese population. Certain
studies have proposed that a gradual decline in the GFR is an
expected consequence of aging, and that rigid cutoffs of the GFR
result in the arbitrary ‘labeling’ of individuals with disease,
particularly when the GFR is considered to indicate mild CKD (45–59
ml/min/1.73 m2) (2,3).
However, this estimate of the GFR is cumbersome and susceptible to
record errors in elderly individuals (4). An additional approach for evaluating
the significance of a low GFR in the elderly population is to
assess the association between a lower GFR and metabolic disorders,
typically observed in patients with CKD (5). Furthermore, anemia is common in CKD
(6); however, it remains unknown
whether hemaglobin (Hb) levels may be used to discriminate the
stages of CKD in elderly patients, and whether Hb can be used as a
biomarker to assess the severity of CKD. The association of CKD and
anemia in elderly Chinese patients is not well studied and thus
further investigation is necessary. Studies on the above mentioned
gaps would yield valuable information for elderly Chinese patients
with chronic kidney disease, particularly those with different
hematocrit levels and anemia. Therefore, the aim of the present
study was to investigate the prevalence of CKD in elderly Chinese
individuals, and subsequently the associations with stages of CKD
and complications of anemia.
Materials and methods
Study population
The present study was approved by the Ethics
Committee of Capital Medical University (Beijing, China), and
written informed consent was obtained from all of the patients. In
total, 2,258 subjects (male, 1,138; female, 1,120; age, 30–99
years; mean age, 62.3±12.0 years), admitted to Beijing Tongren
Hospital affiliated to Capital Medical University, were recruited
for the study based on their 99 mTc-DTPA renal clearance value.
Patients were categorized into six groups according to their age:
30–39, 40–49, 50–59, 60–69, 70–79 and ≥80 years-old. Young and
elderly groups were assigned using a cutoff value of 60 years,
according to the latest standards of the World Health Organization
(WHO). CKD was diagnosed according to the National Kidney
Foundation-Kidney Disease Outcomes Quality Initiative (K/DOQI)
clinical practice guidelines; subjects were classified into five
CKD stages according to the K/DOQI guidelines (7). Information was collected as part of the
routine care. All subjects were ambulatory without active
comorbidities, and were under regular control and in a stable
condition. For subjects with multiple samples, only the sample with
the lowest serum creatinine (SCr) value was used for analysis.
Subjects with edema, pleural effusion or ascites, heart failure,
skeletal muscle atrophy, malnutrition, amputation, ketoacidosis or
acute kidney function deterioration were excluded from the study.
In addition, subjects who were receiving any form of renal
replacement therapy or had been administered recombinant human
erythropoietin were excluded.
Blood sampling
Biochemical profiles included those for Hb, the
hematocrit (HCT) and SCr (i-STAT 04J60-20; Abbott Diagnostics Inc.,
Abbott Park, IL, USA). The levels of Hb and SCr, and the HCT value,
were determined in a single laboratory at Beijing Tongren Hospital
using a Stanbio 900900SP (Stanbio Laboratory, Boerne, TX, USA).
Blood samples were obtained simultaneously with the reference GFR
(rGFR) measurement.
Measurement of the rGFR
GFRs were calculated based on the
99mTc-DTPA-clearance rate, with the rGFR. The 99mTc-DTPA-clearance
rate was assayed using a radionuclide imaging method, known as the
modified Gates' method (8), which
was performed using a GE SPECT Millennium VG Hawkeye Nuclear
Medical System (GE Healthcare Life Sciences, Little Chalfont, UK).
Following Gates' method, the subjects were asked to drink 300–500
ml water after breakfast, which was 20 min prior to the
investigation. Between 2–3 min following the arrival of the
radiotracer in the kidneys, the fractional renal uptake of the
intravenously administered 99mTc-DTPA is proportional to the GFR.
The GFR was computed from the scintigraphic determination of the
99mTc-DTPA uptake within the kidneys, and modified according to the
Chinese population (9). Results
obtained from the rGFR method were corrected for the body surface
area (BSA; m2) as follows: rGFR (ml/min/1.73
m2) = GFR/standard BSA. The BSA was calculated according
to the method outlined by Du Bois and Du Bois (10).
Statistical analysis
All statistical analyses were conducted using SPSS
version 16.0 (SPSS, Inc., Chicago, IL, USA). Descriptive statistics
for continuous variables were presented as the mean ± standard
deviation, while categorical variables (number and percentage) were
used to characterize the study population. Levels of Hb and SCr,
the HCT and the rGFR were assessed for the young and elderly
individuals separately, across the various CKD stages. Analysis of
variance was used to assess the effect of aging on the CKD stages,
and the effect of CKD severity on the Hb level and number anemia
cases. In addition, comparisons were performed for the prevalence
rates of significant anemia cases among subjects with an rGFR of
<30, 30–44, 45–59 and >60 ml/min/1.73 m2. The
associations among anemia, rGFR and age were also analyzed based on
the WHO definitions of Hb (females, <120 g/l; males, <130
g/l) (11). P<0.05 was considered
to indicate a statistically significant difference.
Results
Subjects and their
characteristics
Baseline characteristics of all the participants are
shown in Table I. The mean rGFR was
91.19±23.81 ml/min/1.73 m2 in the young group and
64.84±23.60 ml/min/1.73 m2 in the elderly group. The
prevalence of a rGFR of <60 ml/min/1.73 m2 was higher
in the elderly group compared with the young group (Table I). As shown in Table II, the number of patients with stage
3 CKD increased with aging, with the number of stage 3 CKD cases
>50% in the ≥80 years age group. With regard to the percentage
of cases of CKD stage 3a or higher, there was a small difference
between the young and elderly groups. However, statistically
significant differences were observed in the percentage of CKD
among the different decade of age groups.
 | Table I.Clinical and demographic
characteristics of the study population (n=2,258) at the
baseline. |
Table I.
Clinical and demographic
characteristics of the study population (n=2,258) at the
baseline.
| Patient
characteristics | Young group | Elderly group | P-value |
|---|
| Subjects, n | 989 | 1,269 |
|
| Age, years | 51.17±6.34 | 70.95±7.32 | <0.001 |
| Gender |
|
|
|
| Male, n
(%) | 508 (51.4) | 630 (49.6) | 0.421 |
| Creatinine,
mg/dl | 0.96±0.83 | 1.20±0.94 | <0.001 |
| Hb, g/l | 136.63±18.35 | 124.80±18.26 | <0.001 |
| HCT | 0.40±0.05 | 0.37±0.05 | <0.001 |
| GFR, ml/min/1.73
m2 | 91.19±23.81 | 64.84±23.60 | <0.001 |
| ≥60,
% | 90.6 | 59.3 |
|
| 45–59,
% | 5.1 | 20.3 |
|
| 30–44.99,
% | 2.2 | 12 |
|
| <30,
% | 2 | 8.4 |
|
| Table II.Distribution of subjects according to
their rGFR stage and age group. |
Table II.
Distribution of subjects according to
their rGFR stage and age group.
|
|
|
| CKD stage, n (%) |
|---|
|
|
|
|
|
|---|
| Age, years | Cases, n | GFRa, ml/min/1.73 m2 | CKD 1–2 | CKD 3a | CKD 3b | CKD 4–5 |
|---|
| 30–39 | 59 | 100.61±26.21 | 54 (91.5) | 4 (6.8) | 0 (0) | 1 (1.7) |
| 40–49 | 275 |
96.75±24.36 | 254 (92.4) | 13 (4.7) | 2 (0.7) | 6 (2.2) |
| 50–59 | 655 |
88.00±22.70 | 588 (89.8) | 34 (5.2) | 20 (3.0) | 13 (2.0) |
| 60–69 | 550 |
74.67±22.06 | 416 (75.6) | 80 (14.6) | 37 (6.7) | 17 (3.1) |
| 70–79 | 558 |
60.49±21.69 | 297 (53.2) | 131 (23.5) | 75 (13.4) | 55 (9.9) |
| ≥80 | 161 |
46.37±19.16 | 40 (24.8) | 47 (29.2) | 40 (24.8) | 34 (21.2) |
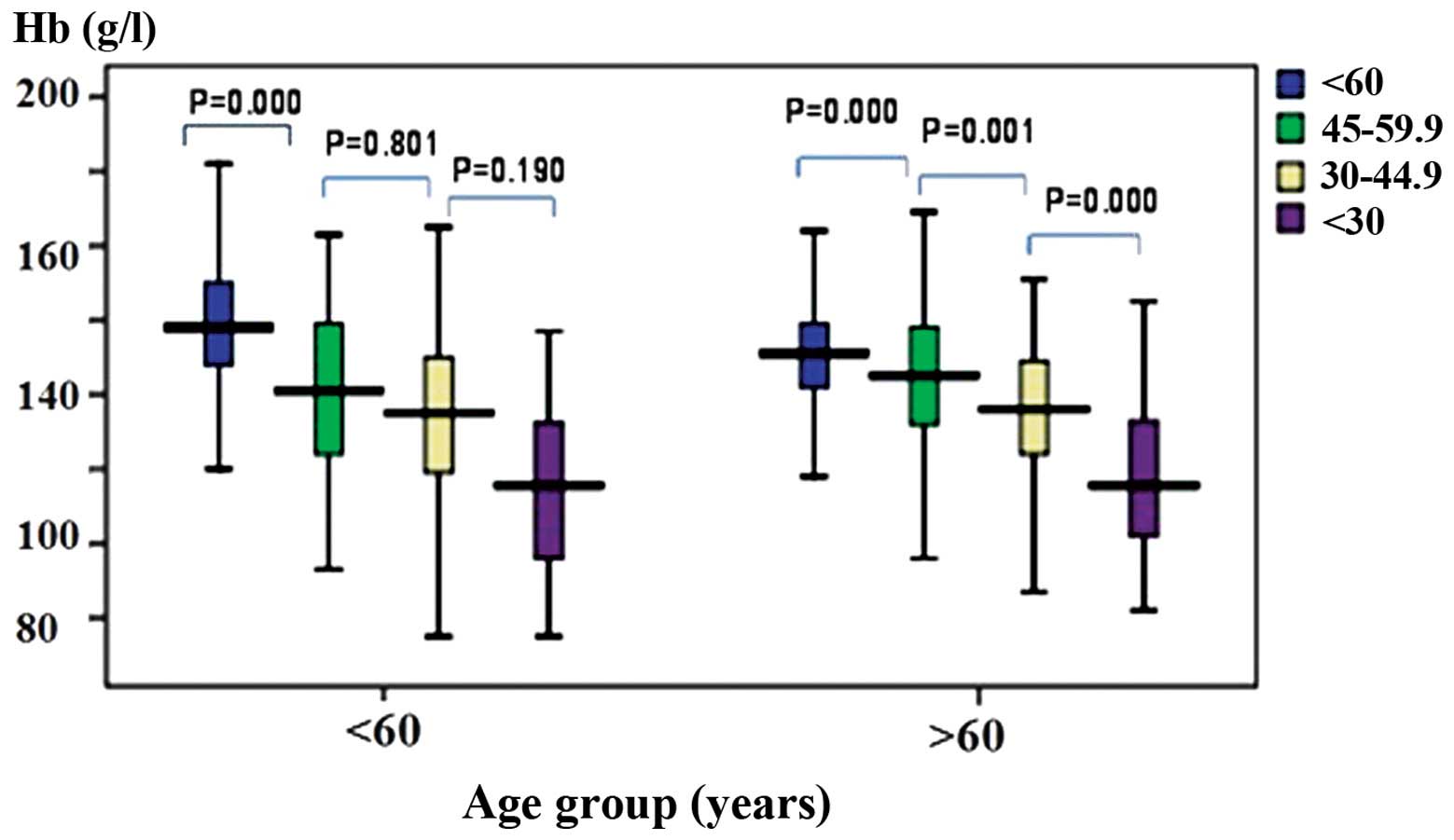
rGFR and anemia
In the young and elderly groups, the Hb
concentration was shown to decrease and anemia was shown to
deteriorate with increasing CKD stage (Table III). A rGFR of 45 ml/min/1.73
m2 was an important cutoff, particularly in the elderly
group. In the young group, there were no statistically significant
differences in the Hb concentration or number of anemia cases
between the patients with CKD of stage 3a and 3b. However, in the
elderly group, the Hb levels were significantly higher and the
number of anemia cases was alleviated in patients with stage 3a
CKD, as compared with patients with CKD of stage 3b (Fig. 1).
| Table III.Hb concentration and anemia are
associated with the reduced rGFR in the two age groups. |
Table III.
Hb concentration and anemia are
associated with the reduced rGFR in the two age groups.
| Group | Parameters | CKD 1–2 | CKD 3a | CKD 3b | CKD 4–5 | P-value |
|---|
| Young | Hb, g/l | 139.01±15.72 | 120.53±22.81 | 114.18±23.33 | 95.7±24.37 | <0.001 |
|
| Anemia, n (%) | 138 (15.4) | 28 (54.9) | 13 (59.1) | 16 (80) | <0.001 |
| Elderly | Hb, g/l | 131.00±13.02 | 124.32±17.50 | 113.66±18.31 | 97.93±19.88 | <0.001 |
|
| Anemia, n (%) | 206 (27.4) | 131 (50.8) | 103 (67.8) | 92 (86.8) | <0.001 |
Discussion
In 2002, the K/DOQI proposed a CKD definition and
staging system, which is now regarded as the millstone of CKD
development. The study focused attention towards CKD in the public
and for non-nephrology physicians, moved the research on the
epidemiology of CKD forward, and had a significant impact on the
policy of public health (12).
However, there was limited evidence-based therapy available at that
time. With the development of clinical practice and increasing
evidence-based treatment, much controversy has been aroused
(13,14). One major focus is the K/DOQI
definition and staging, based on the epidemiology survey. The
prevalence of CKD is between 6 and 16% in the elderly population
(15). The increasing population of
CKD patients are predominantly classified as stage 3, particularly
within the elderly population. The results of the present study
revealed that the prevalence of CKD increases with age. In the
elderly group, 40.7% of the subjects had a GFR of <60
ml/min/1.73 m2, among which 20.3% were classified as CKD
stage 3a, indicating that >50% of patients with stage 3 CKD are
at stage 3a. In subjects aged between 70 and 79 years, almost 50%
had a GFR of <60 ml/min/1.73 m2, while for those aged
>80 years, ∼75% had a GFR of <60 ml/min/1.73 m2.
These observations are consistent with previously published results
(16), indicating that this is a
common finding in the elderly population.
Anemia is very common in CKD and an independent
predictor for cardiovascular complications of CKD. Not only does
anemia affect the life quality of patients, the condition worsens
their kidney function. Patients at any stage of CKD may be
accompanied with different degrees of anemia. The common causes are
inadequate erythropoietin levels due to kidney disease, the
metabolic products of renal dysfunction, and the toxins produced by
uremia, which are renal-derived (17). However, anemia caused by nutritional
insufficiency is more common in stages 1 and 2 CKD (18). A positive correlation between the
degree of anemia and the degree of kidney insufficiency has been
previously reported (19,20). The results of the present study
indicated that the level of Hb decreased with decreasing renal
function. Using a GFR of 60 ml/min/1.73 m2 as the cutoff
point, in the young group, a statistically significant difference
was observed in the level of Hb, with higher values observed in
those with a higher GFR. There was no statistically significant
difference in the level of Hb between patients with stage 3 and 4
CKD. However, in the elderly group, statistically significant
differences were observed in the Hb level between patients with
stages 1–5 of CKD. Furthermore, a statistically significant
difference was observed between patients with stage 3a and 3b CKD,
demonstrating the importance of staging in this age group.
Compared with the Hb level, the prevalence of anemia
appears to be more important clinically. The present study
demonstrated that in the young group, there was a significantly
higher prevalence of anemia cases in those with stage 3b compared
with stage 3a CKD, when the GFR was >60 ml/min/1.73
m2. However, no statistically significant difference was
observed when the GFR cutoff was set at 45 ml/min/1.73
m2. In the elderly group, the prevalence of anemia
differed between patients with stage 3a and 3b CKD, regardless of
the GFR cutoffs. This observation indicated that in an elderly
population, a GFR cutoff of 45 ml/min/1.73 m2 may be
more successful for use in clinical practice.
However, there are limitations to the present study.
Although the current study used a large patient population,
including more patients is likely to improve the accuracy of the
results. In addition, as the focus of the study was Hb and anemia,
the associations among metabolic acidosis, electrolytes,
parathyroid function, proteinuria and other factors were not
evaluated and require further investigation.
In conclusion, the results of the present study
demonstrated that Hb levels can be used to discriminate stages of
CKD in elderly Chinese patients. Therefore, Hb may be used as a
biomarker to assess the severity of CKD.
Acknowledgements
The study was funded by a grant from the Research
Project of Beijing Healthcare (grant no. Jing 11-04). The authors
thank all the subjects who participated in the study, as well as
all the staff and faculty member in the departments that provided
assistance during the study.
References
|
1
|
Coresh J, Astor BC, Greene T, Eknoyan G
and Levey AS: Prevalence of chronic kidney disease and decreased
kidney function in the adult US population: Third National Health
and Nutrition Examination Survey. Am J Kidney Dis. 41:1–12. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Glassock RJ and Winearls C: An epidemic of
chronic kidney disease: fact or fiction? Nephrol Dial Transplant.
23:1117–1121. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Woodard T, Sigurdsson S, Gotal JD, et al:
Mediation analysis of aortic stiffness and renal microvascular
function. J Am Soc Nephrol. Oct 7–2014.(Epub ahead of print).
PubMed/NCBI
|
|
4
|
Carnevale V, Pastore L, Camaioni M, et al:
Estimate of renal function in oldest old inpatients by MDRD study
equation, Mayo Clinic equation and creatinine clearance. J Nephrol.
23:306–313. 2010.PubMed/NCBI
|
|
5
|
Van Pottelbergh G, Vaes B, Jadoul MC, et
al: The prevalence and detection of chronic kidney disease
(CKD)-related metabolic complications as a function of estimated
glomerular filtration rate in the oldest old. Arch Gerontol
Geriatr. 54:e419–e425. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Chen TK, Estrella MM, Astor BC, Greene T,
Wang X, Grams ME and Appel LJ: Longitudinal changes in hematocrit
in hypertensive chronic kidney disease: Results from the
African-American Study of Kidney Disease and Hypertension (AASK).
Nephrol Dial Transplant. Mar 27–2015.(Epub ahead of print).
View Article : Google Scholar
|
|
7
|
National Kidney Foundation, . K/DOQI
clinical practice guidelines for chronic kidney disease:
evaluation, classification, and stratification. Am J Kidney Dis. 39
(2 Suppl 1):S1–S266. 2002.PubMed/NCBI
|
|
8
|
Gates GF: Split renal function testing
using Tc-99m DTPA. A rapid technique for determining differential
glomerular filtration. Clin Nucl Med. 8:400–407. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Li Q, Zhang CL, Fu ZL, et al: Development
of formulae for accurate measurement of the glomerular filtration
rate by renal dynamic imaging. Nucl Med Commun. 28:407–413. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Du Bois D and Du Bois EF: A formula to
estimate the approximate surface area if height and weight be
known. 1916. Nutrition. 5:303–313. 1989.PubMed/NCBI
|
|
11
|
McLean E, Cogswell M, Egli I, et al:
Worldwide prevalence of anemia, WHO Vitamin and Mineral Nutrition
Information System, 1993–2005. Public Health Nutr. 12:444–454.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Patel SS, Kimmel PL and Singh A: New
clinical practice guidelines for chronic kidney disease: a
framework for K/DOQI. Semin Nephrol. 22:449–458. 2002.PubMed/NCBI
|
|
13
|
Zhang L, Zhang P, Wang F, et al:
Prevalence and factors associated with CKD: a population study from
Beijing. Am J Kidney Dis. 51:373–384. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hallan SI, Ritz E, Lydersen S, et al:
Combining GFR and albuminuria to classify CKD improves prediction
of ESRD. J Am Soc Nephrol. 20:1069–1077. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
McMurray JJ, Uno H, Jarolim P, et al:
Predictors of fatal and nonfatal cardiovascular events in patients
with type 2 diabetes mellitus, chronic kidney disease, and anemia:
an analysis of the Trial to Reduce cardiovascular Events with
Aranesp (darbepoetin-alfa) Therapy (TREAT). Am Heart J.
162:748–755. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
McClellan WM, Resnick B, Lei L, et al:
Prevalence and severity of chronic kidney disease and anemia in the
nursing home population. J Am Med Dir Assoc. 11:33–41. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Coresh J, Turin TC, Matsushita K, et al
CKD Prognosis Consortium: Decline in estimated glomerular
filtration rate and subsequent risk of end-stage renal disease and
mortality. JAMA. 311:2518–2531. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Babitt JL and Lin HY: Mechanisms of anemia
in CKD. J Am Soc Nephrol. 23:1631–1634. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Drawz PE, Babineau DC and Rahman M:
Metabolic complications in elderly adults with chronic kidney
disease. J Am Geriatr Soc. 60:310–315. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bowling CB, Inker LA, Gutiérrez OM, et al:
Age-specific associations of reduced estimated glomerular
filtration rate with concurrent chronic kidney disease
complications. Clin J Am Soc Nephrol. 6:2822–2828. 2011. View Article : Google Scholar : PubMed/NCBI
|