Introduction
Since Marshall (1)
initially reported the use of a flexible cystoscope to visualize a
ureteric stone, there have been marked technical advancements in
the flexible ureteroscope, which has revolutionized the treatment
of upper urinary tract calculi. However, the conventional
integrated flexible ureteroscope is fragile and costly, and the
ongoing maintenance and repair costs are expensive. Afane et
al (2) assessed four flexible
ureteroscopes and reported that repair of flexible ureteroscopes
was mandatory after an average of 6–15 uses or 3–13 h. Similarly,
Landman et al (3) evaluated
the durability of the ACMI DUR-8 ureteroscope and noted continued
function in 25 cases prior to repair. Carey et al (4) reported 40–48 uses for four flexible
ureteroscopes, including ACMI DUR-8, DUR-8 Elite, and Storz Flex-X,
prior to the first repair. In addition, Canales et al
(5) reported the average repair cost
for flexible ureteroscopes to be 4,597 USD, which may have since
risen.
Flexible ureteroscopes also require backup
equipment, due to possible malfunction, which necessitates further
financial commitment. All of these disadvantages have tempered the
enthusiasm of both surgeons and institutions for widespread
popularization of this technique. Therefore, in order to promote
the application of flexible ureteroscopes, an inexpensive, small
caliber, single-use flexible ureteroscope, with similar deflection
capabilities as conventional integrated flexible ureteroscopes, may
be a cost-effective option since it eliminates the associated
repair costs and need for backup instruments.
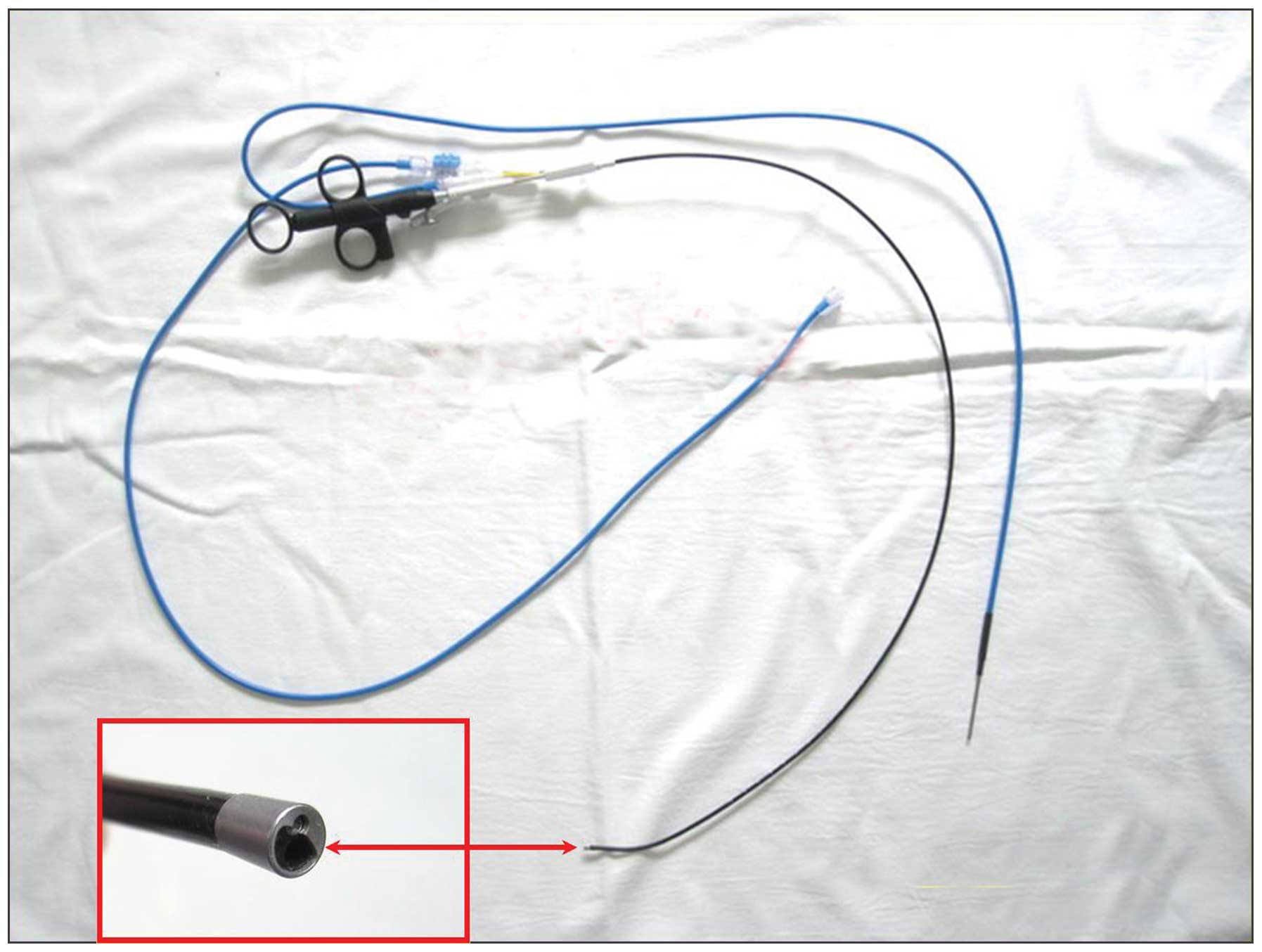
The PolyScope™ (PolyDiagnost GmbH,
Pfaffenhofen, Germany) is a disposable, modular design, flexible
ureteroscope, which consists of a single-use flexible multilumen
catheter and a separate, reusable optical fiber (Fig. 1). This system has been described in
detail by Bader et al (6) and
Johnson et al (7). Laser
lithotripsy is an established endourological modality. Holmium
lasers have broadened the applications for ureteroscopic stone
treatment to include larger stone sizes throughout the entire upper
urinary tract. The present study aimed to analyze the combined use
of the PolyScope™ and holmium laser lithotripsy for the
treatment of renal and proximal ureteral calculi, in order to
further evaluate the clinical value of this instrument. To the best
of our knowledge, the present study represents the largest
single-surgeon experience, in which there was uniformity of
technique and treatment algorithms.
Materials and methods
Ethics statement
This study was approved by the ethics board of the
First Hospital of Ningbo, Ningbo University (Ningbo, China).
Written informed consent was not obtained, since all patient
records were anonymized and de-identified prior to analysis.
Patients
A retrospective review of 691 procedures performed
at the First Hospital of Ningbo, Ningbo University for renal and
proximal ureteral calculi between June 2010 and June 2013 was
conducted. The present study identified 382 consecutive patients
with renal and proximal ureteral calculi who had undergone
PolyScope™ and laser lithotripsy by a single surgeon (Dr
Yue Cheng). A chart review was used to obtain patient, stone, and
treatment parameters. The inclusion criteria for ureteroscopy in
this series were: Renal and proximal ureteral calculi that failed
extracorporeal shock wave lithotripsy (ESWL), obesity (>30
kg/m2), poor candidates for percutaneous procedures, and
patient preference. The exclusion criteria included severe
hydronephrosis, stones in a calyceal diverticulum, and
non-dependently draining collecting system (i.e., high insertion of
the ureter, horseshoe kidney). All patients were offered ESWL and
percutaneous nephrolithotomy (PNL) as alternative treatment
options, and the final decision regarding the treatment was made by
the patients themselves. Informed consent included specific mention
of the possible need for numerous ureteroscopic procedures,
residual stones and stent placement, and was obtained from all
patients.
All patients underwent preoperative urine culture
sensitivity tests, serum biochemistry and routine blood tests, a
non-contrast spiral computed tomography (CT) urogram (to define
total stone burden), and an intravenous urography. Patients with
positive urine cultures were adequately treated with appropriate
antibiotics, with all patients having a negative urine culture
prior to surgery.
Surgical Procedures
All of the procedures were performed by a single
surgeon (Fig. 2). Patients were
administered intravenous preoperative antibiotics. Procedures for
153 patients were performed under spinal anesthesia, whereas 229
patients were operated on under general anesthesia. All procedures
were carried out in the dorsal lithotomy position. A 22 F
cystoscope was inserted into the bladder via the urethra, and the
ureteral orifice was cannulated with an open-ended 5F catheter and
a 0.038-inch hydrophilic guidewire. A 6/7.5F or 8/9.8F semi-rigid
ureteroscope (Richard Wolf GmbH, Knittlingen, Germany) was passed
over a guidewire using fluoroscopic guidance until it reached the
proximal ureter or renal pelvis. This enabled dilation of the
ureteral orifice and facilitated easier instrument passage during
the flexible ureteroscopy. Subsequently, a ureteral access sheath
(12/14 F or 14/16 F; Cook Medical, Inc., Bloomington, IN, USA) was
placed in order to allow optimal visualization, maintain low
intrarenal pressure, and to facilitate stone fragment extraction.
If the ureteral access sheath could not be placed in patients with
a tight ureter or ureteral stricture, a double-J stent was placed
instead and the procedure was performed 2–6 weeks later. An 8 F
PolyScope™ and a 200 or 365 µm laser fiber were used for treatment.
Irrigation was conducted using a 60 ml syringe with normal saline
connected to a 3-way stopcock with arterial line tubing. The
holmium laser (Powersuite 100 W; Lumenis, Inc., San Jose, CA, USA)
was set to an energy level of µ0.8–1.5 J and at a rate of 15–30 Hz.
Following lithotripsy, stone fragments were retrieved using a
1.9-Fr nitinol basket (Zero-Tip; Boston Scientific Japan Co. Ltd.,
Tokyo, Japan) if necessary. A double-J ureteral stent was routinely
left in all patients, and the stent was removed 2–4 weeks
postoperatively, when it was decided that the stent was no longer
necessary.
A plain kidney, ureter, and bladder X-ray (KUB) was
performed on postoperative day 1 in all cases, in order to assess
the residual stone fragments and position of the double-J stent. A
total of 1–2 weeks following the procedure, residual stone
fragments were assessed again using a renal ultrasound, plain KUB
film, and/or a CT scan. If necessary, a second-look procedure was
scheduled 2–4 weeks following the first procedure. The operative
time was calculated from the time of cystoscope insertion to the
completion of stent placement. Stone-free status was defined as no
fragments or asymptomatic, or the presence of clinically
insignificant residual fragments ≤4 mm, based on the European
Association of Urology Guidelines 2013 (8).
Statistical analysis
Data are presented as the mean ± standard deviation,
the median and range for continuous variables, and the number and
percentage for categorical variables. Data were recorded using
Microsoft Excel 2010 software (Microsoft Corporation, Redmond, WA,
USA).
Results
Table I presents
patient demographics: 382 patients were eligible for the present
study; 215 males and 167 females. The average age was 49.1±15.0
years (range, 17–84 years).
 | Table I.Patient demographics. |
Table I.
Patient demographics.
| Characteristics | Values |
|---|
| Gender (n) |
|
| Male | 215 (56.3%) |
|
Female | 167 (43.7%) |
| Age (y) | 49.1±15.0 |
| BMI
(kg/m2) | 23.6±2.2 |
| Previous ESWL
(n) | 274 (71.7%) |
The stone demographics and operative data are shown
in Table II. The mean stone size
was 11.6±3.8 mm (range, 5–28 mm), and the mean total stone burden
was 16.7±5.7 mm (range, 8–46 mm). A total of 305 patients (79.8%)
had a stone burden ≤20 mm, and 77 patients (20.2%) had a stone
burden >20 mm. Overall, 284 patients underwent one procedure, 87
patients underwent two procedures and 11 patients underwent three
treatments, not including the final ureteroscopic inspection at the
time of double-J stent removal. This equates to 491 primary
procedures for 382 patients, a mean of 1.3±0.2 primary procedures
for each patient. The mean operative time per procedure was
67.1±19.2 min (range, 35–116 min). Of all the 491 procedures, 121
multilumen catheters were used. The mean repeat usage of a
multilumen catheter was 4.1 (range, 1–6). The stone-free rates
following the first and the second procedures were 74.3 and 86.9%,
respectively. The overall stone-free rate was 86.9%. Of the 11
patients who underwent a third procedure, none were rendered
stone-free. The mean postoperative hospital stay following each
procedure was 2.9±1.0 days (range, 2–6 days).
| Table II.Stone demographics and operative
data. |
Table II.
Stone demographics and operative
data.
| Variables | Values |
|---|
| Mean stone size
(mm) | 11.6±3.8 |
| Mean stone burden
(mm) | 16.7±5.7 |
| Cumulative stone
burden (n) |
|
| ≤20
mm | 305 |
| >20
mm | 77 |
| Stone location
(n) |
|
| Renal
pelvis | 115 |
| Upper
calyx | 96 |
| Middle
calyx | 81 |
| Lower
calyx | 43 |
| Proximal
ureter | 29 |
| Multiple
calyx | 18 |
| Mean number of
procedures per patient | 1.3±0.2 |
| Mean operative time
per procedure (min) | 67.1±19.2 |
| Mean repeat usage of
the multilumen catheter | 4.1±1.5 |
| Overall SFR (%) | 86.9 |
| SFR after first
treatment (%) | 74.3 |
| SFR after second
treatment (%) | 86.9 |
| SFR after third
treatment (%) | 86.9 |
| Major complication
rate (%) | 2.1 |
| Minor complication
rate (%) | 6 |
| Mean postoperative
hospital stay (d) | 2.9±1.0 |
Table III presents
stone clearance rates according to stone burden and location. The
highest clearance rates were observed for proximal ureteral stones
(100%) and renal pelvic stones (88.7%), whereas the lowest
clearance rates were observed for lower calyx stones (76.7%) and
multiple calyx stones (77.8%). The higher the stone burden, the
lower the postoperative stone-free rate (≤20 vs. >20.0 mm; 89.8%
vs. 75.3%).
| Table III.Stone-free rates for patients with
various stone burdens and locations. |
Table III.
Stone-free rates for patients with
various stone burdens and locations.
| Variables | Number | Overall SFR (%) |
|---|
| Cumulative stone
burden |
|
|
| ≤20
mm | 305 | 274 (89.8) |
| >20
mm | 77 | 58
(75.3) |
| Stone location |
|
|
| Renal
pelvis | 115 | 102 (88.7) |
| Upper
calyx | 96 | 84
(87.5) |
| Middle
calyx | 81 | 70
(86.4) |
| Lower
calyx | 43 | 33
(76.7) |
| Proximal
ureter | 29 | 29
(100) |
| Multiple
calyx | 18 | 14
(77.8) |
Ureteral perforation occurred in one patient,
resulting in the discontinuation of the procedure following the
placement of a double-J stent. This patient underwent a second
treatment one month later (Clavien-Dindo grade III) (9). A follow-up CT urogram one month after
double-J stent removal documented no stricture formation. Five
patients exhibited significant bleeding, which resulted in poor
visibility and led to discontinued procedures. However, no
transfusions were necessary (Clavien-Dindo grade I). These five
patients underwent an uncomplicated second treatment 2 weeks later,
and no other major intraoperative complications (Clavien-Dindo
grade III or greater), such as ureteral avulsion and renal rupture,
were identified. Postoperative high-grade fever >38.5°C was
observed in 25 patients (Clavien-Dindo grade II), including two
patients who developed sepsis (considered as a postoperative major
complication). These patients were conservatively treated with
parenteral administration of antibiotics.
Discussion
Rapid advances in distal-tip deflection,
miniaturization of flexible ureteroscopes and corresponding
accessories, have allowed the potential application of these
instruments in not only diagnostic, but also therapeutic,
procedures. However, the ongoing problems faced by surgeons with
the conventional integrated flexible ureteroscope, including its
low cost-effectiveness and fragility, ultimately limit the clinical
application of these instruments (10,11).
To decrease the overall cost of ureteroscopy by
eliminating repair costs, a novel flexible ureteroscope
(PolyScope™) has been produced. The
PolyScope™ is a flexible ureteroscope with a
semi-disposable and modular design. The instrument has a separate
optical system, which consists of a 10,000-pixel fiber optic (0.77
mm diameter) and an angle of view of 120°, therefore the image can
be transmitted clearly and stably. The multilumen catheter of this
instrument has an outer diameter of 8F (2.65 mm), a
working/irrigation channel of 3.5 F (1.2 mm), and a length of 85
cm. The steering component is rotatable, which has a luer-lock
mechanism for deflection of the steerable tip of the catheter. The
tip deflection angle is >240°, even when the 365 µm laser fiber
or the 3 F basket is inserted into the working channel. Bagley and
Rittenberg (12) noted that a mean
range of 140° (104–175°) of deflection is sufficient to reach the
lower calyx. Therefore, theoretically, the PolyScope™ is
able to check all calyxes. The ocular, camera, and light cables are
separated from the endoscopic catheter outside the sterile field
and are mounted on a four-joint arm, which allows for easy
positioning of the non-sterile components relative to the operating
side. As the separate image fiber does not come into direct contact
with the patient, it does not require sterilization following each
use. Therefore, the subsequent procedures can be performed
immediately, simply by changing the multilumen catheter.
Bader et al (6) examined the clinical outcome of 32
patients with renal stones who were treated using the
PolyScope™, and reported a stone-free rate of 87.5%. In
addition, Bansal et al (13)
diagnosed and treated 22 patients with the PolyScope™;
of which six patients with undiagnosed hematuria were diagnosed
with transitional-cell carcinoma, and 16 patients had stones (<1
cm) removed using a Dormia basket. Three PolyScope™
multilumen catheters were used to complete all of the procedures,
indicating that the disposable catheters can be sterilized and
reused. Gu et al (14)
evaluated the clinical value of the PolyScope™ endoscope
system in the treatment of 86 patients with upper urinary calculi
with a diameter <2 cm. Lithotripsy was successful in 77 patients
and the mean duration of the surgery was 42 min.
In the present study, PolyScope™ and
holmium laser lithotripsy were used to treat 382 patients with
renal and proximal ureteral calculi; a total of 491 procedures were
performed with 121 multilumen catheters, and the mean repeat usage
of a multilumen catheter was 4.1. The stone-free rate following the
first and the second procedures was 74.3 and 86.9%, respectively.
The third procedure did not improve the stone-free rate. The
overall complication rate was 8.1%. Six (1.6%) intraoperative
complications arose: One patient suffered from a ureteral
perforation and five patients exhibited significant bleeding, which
led to early discontinuation of the procedure. A total of 25
patients had postoperative high-grade fever >38.5°C. All of the
patients fully recovered after appropriate treatment and no other
severe complications were observed. The results of the present
study are comparable with the conventional integrated flexible
ureteroscope efficacy for treatment of upper urinary tract stones
(15,16). As for lower calyx calculi,
theoretically there are no blind spots due to the excellent
deflection of the instrument. However, due to anatomical
particularities, the bending angle of the PolyScope™ was
reduced following insertion of the auxiliary instruments; therefore
some lower calyx calculi may not be reached. Therefore, the overall
stone-free rate of lower calyx calculi was lower, as compared with
that in the upper and middle calyx calculi. In addition, the
overall stone-free rate was low in calculi with a cumulative stone
burden >20 mm. Dasgupta et al (17) performed flexible ureterorenoscopy in
105 patients over a 9-month period, and obtained overall success in
72.3%. A successful outcome was achieved in 72% with a stone size
≤10 mm, 80% for 11–20 mm, and 50% for >20 mm. Two or more
procedures were required in eight patients; thus suggesting that
the flexible ureteroscope is more suitable for stones <20 mm.
However, due to the minimally invasive nature of flexible
ureteroscopy, staged procedure for the treatment of large stones is
a practical option. In the present study, the stone-free rate was
74.3% after the first procedure, which increased to 86.9% after the
second procedure. In a comparable study, Riley et al
(18) used retrograde flexible
ureteroscopy with holmium laser lithotripsy to treat 22 patients
with stones >2.5 cm, the average number of procedures was 1.82,
and overall stone-free rate was 90.9%; thus suggesting that planned
staged flexible ureteroscopy is a viable option for the treatment
of renal stones >2.5 cm, with excellent stone-free results.
These findings are consistent with the results of the present
study.
According to the present study, the following points
were particularly important for achieving higher stone-free results
and minimizing complications: i) Prior to each flexible
ureteroscopy, a semi-rigid ureteroscopy was performed to exclude
ureteral stricture or other pathological findings. This enabled
dilation of the ureteral orifice and facilitated enhanced
instrument passage during the procedure; ii) following the
semi-rigid ureteroscopy, a ureter access sheath was inserted at the
level of the ureteropelvic junction to enable optimal
visualization, allow numerous passages of the
PolyScope™, maintain low intrarenal pressure and
facilitate stone fragment extraction. In the case of a ureteral
stricture or tight ureter, the ureteral access sheath could not be
inserted; instead a double-J stent was placed for 2–6 weeks to
passively dilate the ureter; iii) once the PolyScope™
was inserted into the pelvis, the operator identified the
ureteropelvic junction as a mark, gradually distinguished the upper
calyx, middle calyx and lower calyx, and then searched for stones
calyx by calyx; iv) in general, the holmium laser lithotripsy was
set at a maximum power of 20–45 W (0.8–1.5 J/15–30 Hz). The laser
energy and frequency of pulsation varied according to different
stone densities and stone burdens. In order to convert the stone
center to small fragments and fine dust, higher settings were
employed initially; however, the settings were decreased to
minimize kinetic forces and emphasize mechanical fragmentation once
the residual mass became mobile.
There are some limitations to the present study. The
present study is a retrospective review from a single institution.
In addition, a single-surgeon experience obviously has limitations
with regards to the reproducibility of the results.
In the present study, the modular flexible
ureteroscope (PolyScope™) proved its safety, utility and
efficacy, and we suggest that modular flexible ureteroscopy with
holmium laser lithotripsy may be considered the primary method for
the diagnosis and treatment of renal and proximal ureteral calculi
in select patients. Notably, the modular design of the
PolyScope™ avoids high maintenance costs associated with
the conventional integrated flexible ureteroscope, making the
PolyScope™ a superior and more cost-effective option for
clinical use. Nevertheless, further clinical studies over a longer
period of time, with a larger patient cohort and at different
centers, are required to validate the perceived advantages of this
device.
Acknowledgements
A research grant was provided by the Ningbo Social
Development Projects Foundation (No. 2011C50065).
References
|
1
|
Marshall VF: Fiber optics in urology. J
Urol. 91:110–114. 1964.PubMed/NCBI
|
|
2
|
Afane JS, Olweny EO, Bercowsky E, Sundaram
CP, Dunn MD, Shalhav AL, McDougall EM and Clayman RV: Flexible
ureteroscopes: A single center evaluation of the durability and
function of the new endoscopes smaller than 9Fr. J Urol.
164:1164–1168. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Landman J, Lee DI, Lee C and Monga M:
Evaluation of overall costs of currently available small flexible
ureteroscopes. Urology. 62:218–222. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Carey RI, Gomez CS, Maurici G, Lynne CM,
Leveillee RJ and Bird VG: Frequency of ureteroscope damage seen at
a tertiary care center. J Urol. 176:607–610. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Canales BK, Gleason JM, Hicks N and Monga
M: Independent analysis of Olympus flexible ureteroscope repairs.
Urology. 70:11–15. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bader MJ, Gratzke C, Walther S, Schlenker
B, Tilki D, Hocaoglu Y, Sroka R, Stief CG and Reich O: The
PolyScope: A modular design, semidisposable flexible
ureterorenoscope system. J Endourol. 24:1061–1066. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Johnson MT, Khemees TA and Knudsen BE:
Resilience of disposable endoscope optical fiber properties after
repeat sterilization. J Endourol. 27:71–74. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tiselius HG, Ackermann D, Allen P, Buck C,
Conort P and Gallucci M: Working Party on Lithiasis, European
Association of Urology: Guidelines on urolithiasis. Eur Urol.
40:362–371. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mitropoulos D, Artibani W, Graefen M,
Remzi M, Rouprêt M and Truss M: European Association of Urology
Guidelines Panel: Reporting and grading of complications after
urologic surgical procedures: An ad hoc EAU guidelines panel
assessment and recommendations. Eur Urol. 61:341–349. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Defidio L, De Dominicis M, Di
Gianfrancesco L, Fuchs G and Patel A: Improving flexible
ureterorenoscope durability up to 100 procedures. J Endourol.
26:1329–1334. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sooriakumaan P, Kaba R, Andrews HO and
Buchholz NP: Evaluation of the mechanisms of damage to flexible
ureteroscopes and suggestions for ureterorenoscopy preservation.
Asian J Androl. 7:433–438. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bagley DH and Rittenberg MH: Percutaneous
antegrade flexible ureteroscopy. Urology. 27:331–334. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Bansal H, Swain S, Sharma GK, Mathanya M,
Trivedi S, Dwivedi US and Singh PB: Polyscope: A new era in
flexible ureterorenoscopy. J Endourol. 25:317–321. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Gu SP, Huang YT, You ZY, Zhou X, Lu YJ, He
CH and Qi J: Clinical effectiveness of the PolyScope™ endoscope
system combined with holmium laser lithotripsy in the treatment of
upper urinary calculi with a diameter of less than 2 cm. Exp Ther
Med. 6:591–595. 2013.PubMed/NCBI
|
|
15
|
Breda A, Ogunyemi O, Leppert JT and
Schulam PG: Flexible ureteroscopy and laser lithotripsy for
multiple unilateral intrarenal stones. Eur Urol. 55:1190–1196.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cohen J, Cohen S and Grasso M:
Ureteropyeloscopic treatment of large, complex intrarenal and
proximal ureteral calculi. BJU Int. 111:E127–E131. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Dasgupta P, Cynk MS, Bultitude MF, Tiptaft
RC and Glass JM: Flexible ureterorenoscopy: Prospective analysis of
the Guy's experience. Ann R Coll Surg Engl. 86:367–370. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Riley JM, Stearman L and Troxel S:
Retrograde ureteroscopy for renal stones larger than 2.5 cm. J
Endourol. 23:1395–1398. 2009. View Article : Google Scholar : PubMed/NCBI
|