Introduction
Mesial temporal lobe epilepsy (MTLE) is the most
common type of medically refractory epilepsy syndrome in
adolescents and adults. MTLE usually presents at the inner aspect
of the temporal lobe, and typically affects the hippocampus,
parahippocampal gyrus and amygdala (1,2). The
pathophysiological substrate of this disease is usually hippocampal
sclerosis (HS) (3). However, certain
cases of MTLE present without the typical changes of mesial
temporal sclerosis or other abnormalities on magnetic resonance
imaging (MRI) scans (MRI-negative), and the seizure outcome is poor
(4). Previous studies have
demonstrated that surgery is a more effective therapeutic approach
for epilepsy compared with anti-epileptic drugs (AEDs) in the
majority of patients with MTLE (5–7). For
this reason, certain scholars consider surgery to be the first
choice of treatment for MTLE. Anterior temporal lobectomy (ATL) is
the most commonly used surgical technique for treating MTLE.
McIntosh et al (6) provided a
systematic review summarizing 126 articles published between 1991
and 2001, and demonstrated that 60–70% of patients with MTLE were
free of seizures following ATL surgery. However, the remaining ~30%
of patients continue to experience seizures to a certain extent,
the cause of which remains unclear. The primary goal of epilepsy
surgery is to achieve the long-term prevention of seizures.
However, numerous studies have reported that the long-term
prognosis is relatively poor compared with the short-term prognosis
(6–15). The causes for long-term worsening of
the surgical outcome are also unknown and the predictive factors of
short-term and long-term prognosis may differ.
Therefore, it is crucial to investigate the
predictive indicators of long-term outcome in patients with MTLE,
which may improve general understanding of the causes of surgical
failure. However, few studies have evaluated the influence of
pre-surgical factors including medical history, clinical features
of seizures, MRI and video-electroencephalography (EEG) monitoring
results on the efficacy of epilepsy surgery, particularly on the
long-term prevention of seizures. Accordingly, it is necessary to
understand how to predict the prognosis from pre-surgical factors
and select patients for surgery in order to improve the
seizure-free rate in patients with MTLE. Therefore, in the present
study, the clinical data of 121 patients with MTLE who underwent an
ATL was analyzed, with at least 1 year of follow-up. Patients were
allocated into different groups according to Engel seizure
classification in order to evaluate the surgical results in terms
of seizure outcomes, and to further analyze the potential value of
predictive factors associated with long-term efficacy.
Subjects and methods
Subjects and inclusion criteria
A total of 162 patients with medically refractory
temporal epilepsy syndrome that underwent ATL in Tiantan Hospital
(Beijing, China) were recruited between January 2005 and December
2008. The inclusion criteria were as follows: i) All patients
presented the clinical characteristics of MTLE for >1 year and
had adequate trial of at ≥3 first-line antiepileptic drugs for
>2 years, but continued to suffer from seizures; ii) continuous
non-invasive 32-channel video scalp EEG monitoring (including
sphenoidal electrodes to determine ictal and interictal focal
activity for ≥7 days) supported the characteristics of MTLE; iii)
MRI (1.5T scanners) and/or histopathological findings were
characteristic of HS. The histopathological findings associated
with HS were neuronal loss and glial proliferation in the
hippocampal subfields CA1 and CA3 or in the dentate gyrus (16–18). The
MRI findings associated with HS were decreased hippocampal volume
secondary to neuronal loss, and increased hippocampal T2 signal
secondary to gliosis (16–18). This study was supported by the ethics
committee of Tsinghua University (Beijing, China). Informed consent
was obtained from the patients for the use of their data.
Pre-surgical evaluation
The pre-surgical evaluation program was as follows:
i) Medical histories included perinatal anoxia, family history of
seizure, febrile seizures, intracranial infection and traumatic
brain injury; ii) clinical data included gender, pre-surgical
duration, auras, age at seizure onset, duration of seizure, types
of seizure, seizure frequency per month prior to surgery, location
of surgery and age at surgery; iii) diagnostic examination included
MRI and video-EEG via scalp/sphenoidal electrodes, single photon
emission computed tomography or positron emission tomography or
magnetoencephalography of relevant areas of patients.
Surgical procedure
Following an ipsilateral frontotemporal craniotomy,
all patients underwent cerebral cortex and deep EEG monitoring. The
surgical approach adopted ATL during which the anterior 4–5 cm of
the temporal tip for the dominant hemisphere and 5–6 cm for the
non-dominant one were resected, as were the mesial structures
including the areas of amygdala, hippocampus and parahippocampal
gyrus. The extent of resection was adjusted on the basis of
intraoperative electrocorticogram (ECoG) monitoring. All surgeries
were performed by the same neurosurgeon and no patients underwent a
second surgery.
Follow-up
Postoperative follow-up data regarding seizure
outcomes, including clinical auras, seizure frequency and duration
of seizure, were obtained via standardized telephone interviews
performed by one of the authors. Patients were assigned to outcome
classes in relation to seizure control based on the Engel seizure
classification, which was as follows: Class I, free of disabling
seizures; class II, rare disabling seizures, almost seizure-free;
class III, worthwhile improvement; and class IV, no worthwhile
improvement.
Data collection and statistical
analysis
The pre-surgical seizure duration was grouped as
<10 years and ≥10 years. According to the international
classification of epileptic seizures (19), seizure types were divided into simple
complex partial seizures (CPS), frequent CPS and frequent
generalized tonic-clonic seizures (GTCS) based on whether the CPS
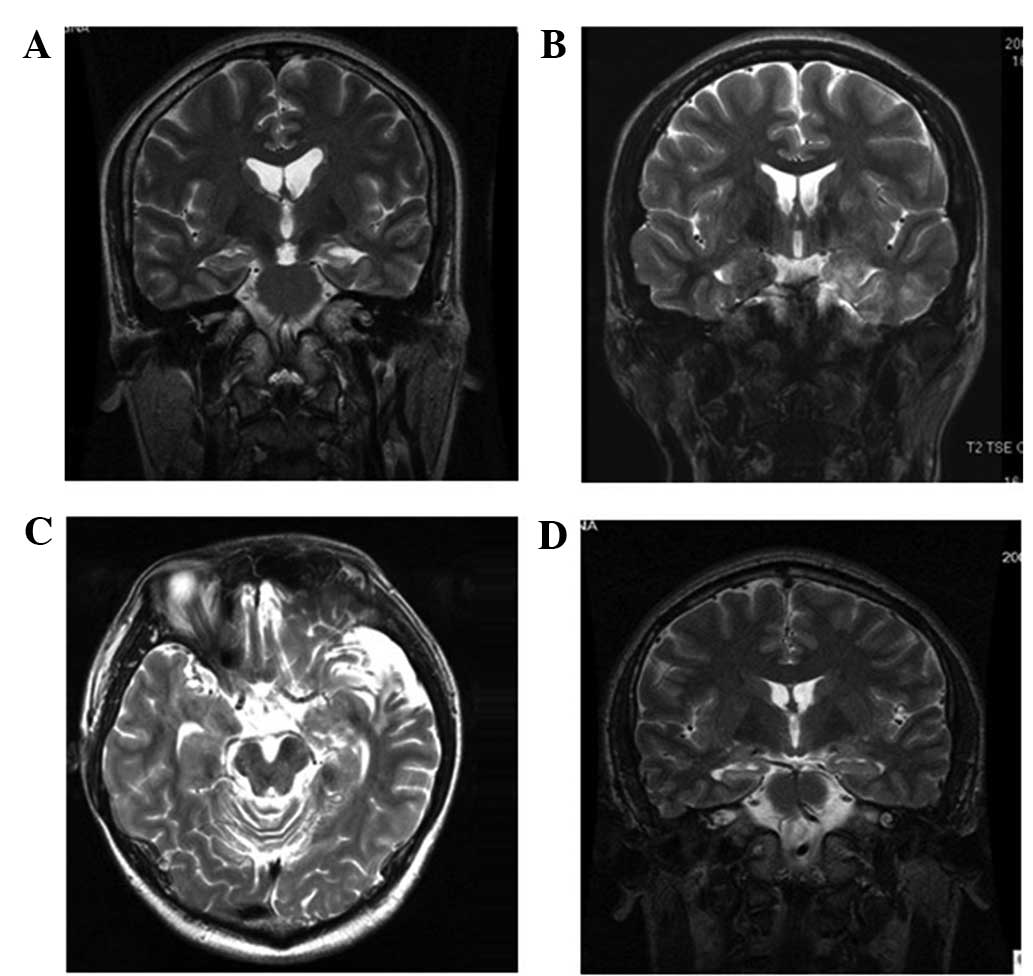
was accompanied by GTCS or not. The MRI data were classed as
positive and negative according to whether HS was present or not
(Fig. 1). Patients were further
classified as exhibiting unilateral local lobe, unilateral
multi-lobe or bilateral lobe seizures, based on the characteristics
of the video-EEG.
Regarding seizure outcome, patients were divided
into two categories: Seizure-free group (Engel classification, I)
and seizure group (Engel classification, II–IV). Patients with
non-disabling auras, but without seizures, were considered to be
seizure-free. Seizure freedom was defined as those patients that
were seizure-free from the day of surgery to the last outcome
assessment, or were seizure-free for >2-years post surgery.
An independent sample t-test or Rank sum test was
used to analyze the quantitative variables: Age at seizure onset,
pre-surgical duration, duration of seizure, seizure frequency per
month prior to surgery and age at surgery. A Pearson's
χ2, continuity correction or Fisher's exact test was
used to analyze the following qualitative variables: Gender,
presence of auras, history of perinatal anoxia, family history of
seizure, febrile seizures, intracranial infection and traumatic
brain injury, location of surgery and MRI data. Row × Column (RxC)
contingency table χ2 and subdivided RxC table
independence tests were used for the analysis of seizure types and
distributing range of spikes in the video-EEG. Backward stepwise
multiple logistic regression analysis was used to assess the
possible predicting factors of prognosis. Using SPSS software,
version 16.0 (SPSS, Inc., Chicago, IL, USA) P<0.017 was
considered to indicate a statistically significant difference in
the subdividing RxC table tests, and P<0.025 was considered to
indicate a statistically significant difference for the other
statistical methods.
Results
Patient characteristics
Among the total of 162 patients with ATL, 123
(75.9%) exhibited MTLE/HS, 14 (8.6%) gliomas, 4 (2.5%) heterotopic
gray matter, 5 (3.1%) cavernous malformation, 8 (4.9%) cerebral
dysgenetic lesions and 8 (4.9%) arachnoid cysts. A total of 121
patients (98.4%, 63 men and 58 women) among the 123 patients with
MTLE/HS were adequately followed-up. The mean follow-up period was
3.33±0.89 years (range, 1–5 years). The mean patient ages at
seizure onset and at surgery were 16.35±12.29 years (range, 4–34
years) and 27.55±11.58 years (range, 5–54 years), respectively. The
mean patient pre-surgical seizure period was 10.90±7.50 years
(range, 2–35 years). Among the 121 patients that received
follow-up, 83 cases possessed a history relating to seizures,
including 63 cases with febrile seizures (including 43 simple
febrile seizures without secondary diseases, 7 cases secondary to
intracranial infection and 13 cases secondary to traumatic brain
injury), 19 cases with traumatic brain injury, 7 cases with
intracranial infection, 12 cases with perinatal anoxia and 2 cases
with a family history of seizures. The numbers of patients that
underwent ATL on the left and right side were 61 (50.4%) and 60
(49.6%), respectively (Table I).
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
| Parameter | Value |
|---|
| Gender, M/F | 63/58 |
| Follow-up period,
years |
|
|
Mean | 3.33±0.89 |
|
Range | 1–5 |
| Age at seizure
onset, years |
|
|
Mean | 16.35±12.29 |
|
Range | 4–34 |
| Age at surgery,
years |
|
|
Mean | 27.55±11.58 |
|
Range | 5–54 |
| Pre-surgical
seizure duration, years |
|
|
Mean | 10.90±7.50 |
|
Range | 2–35 |
| History associated
with seizure, n (%) | 83 (68.6) |
| Febrile
seizures, n (%) | 63 (52.1) |
|
Traumatic brain injury, n
(%) | 19 (15.7) |
|
Intracranial infection, n
(%) | 7
(5.8) |
|
Perinatal anoxia, n (%) | 12 (9.9) |
| Family
history of seizures, n (%) | 2
(1.7) |
| Surgery location, n
(%) |
|
| Left
side | 61 (50.4) |
| Right
side | 60 (49.6) |
| Clinical auras, n
(%) | 57 (47.1) |
| Gastric
gas | 11 (9.1) |
|
Palpitation | 13 (10.7) |
|
Headache | 7 (5.8) |
|
Fear | 17 (14.0) |
|
Déjà-vu | 6 (5.0) |
|
Euphoria | 1 (0.8) |
|
Sadness | 2 (1.7) |
| Automatism, n
(%) | 53 (43.8) |
|
Oroalimentary | 22 (18.2) |
|
Gestural | 25 (20.7) |
|
Verbal | 6 (5.0) |
| Seizure types, n
(%) |
|
| Single
CPS | 30 (24.8) |
|
Frequent CPS | 72 (59.5) |
|
Frequent GTCS | 19 (15.7) |
| Video-EEG results,
n (%) |
|
|
Unilateral lobe | 90 (74.4) |
|
Unilateral multi-lobe | 17 (14.0) |
|
Bilateral lobes | 14 (11.6) |
| Evidence of HS, n
(%) |
|
|
MRI | 101 (83.5) |
|
Histopathology | 115 (93.4) |
Among the 57 patients with auras, 11 cases presented
with adverse rising of gastric gas, 13 cases had palpitations, 7
cases suffered from headache, 17 cases experienced fear, 6 cases
had déjà-vu, 1 case experienced euphoria and 2 cases exhibited
sadness, as observed by the doctor. In addition, 53/121 patients
(43.8%) had automatism, including 22 cases of oroalimentary
automatism, 25 cases of gestural automatism and 6 cases of verbal
automatism. With regard to seizures, there were 30 patients (24.8%)
with CPS, 72 patients (59.5%) with frequent CPS and 19 patients
(15.7%) with frequent GTCS. The results of the video-EEG showed
that in 90 patients (74.4%) the unilateral local lobe was involved
in the seizure onset, 17 patients (14.0%) had unilateral multi-lobe
involvement and 14 patients (11.6%) had bilateral lobe involvement.
Among the 121 patients, 101 cases (83.5%) presented with
indications of HS under MRI examination, and 115 cases (93.4%) had
a diagnosis of HS confirmed by histopathological analysis (the
remaining 6 patients were not available for histopathological
examination but were confirmed to have HS using MRI). Therefore,
all patients received a confirmed diagnosis of HS using MRI or
histopathological analysis, including 20 patients in whom MRI did
not reveal HS, and 95 patients (78.5%) in whom HS was confirmed by
MRI and histopathological results (Table
I).
Engel classification
In total, 87 patients (71.9%) received an Engel
classification of class I and formed the seizure-free group. In
addition, 3 (2.5%), 18 (14.9%) and 13 patients (10.7%) were
categorized as Engel class II, III and IV, respectively, and were
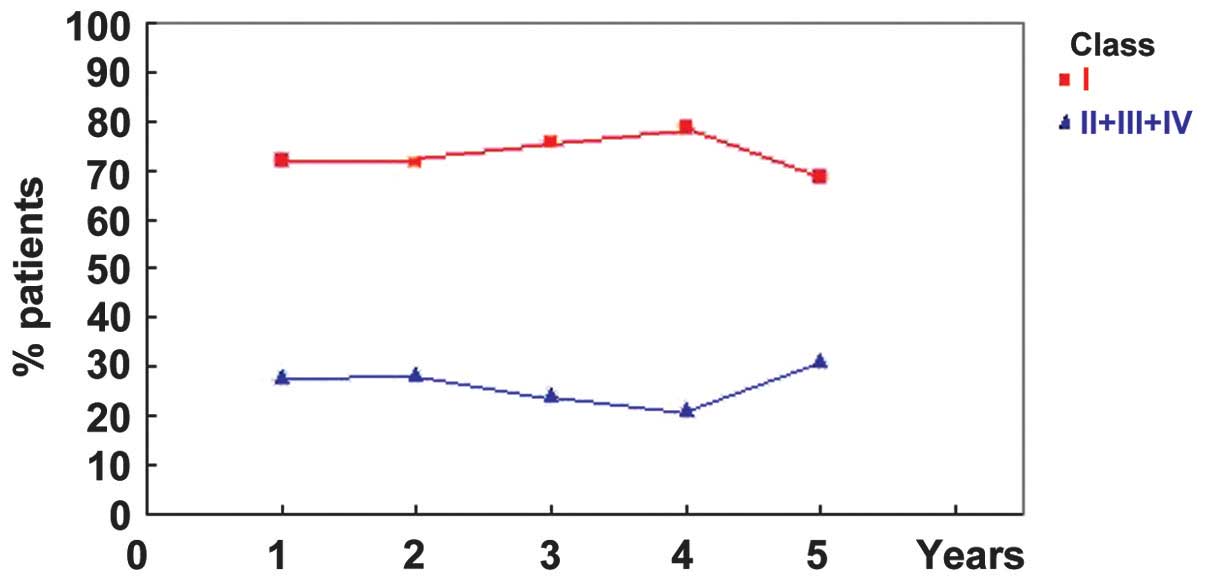
grouped together as the seizure group. Furthermore, 87/121 (71.9%),
83/116 (71.6%), 69/91 (75.8%), 41/52 (78.8%) and 11/16 (68.8%)
patients satisfied the criteria of Engel Class I at years 1–5 of
follow-up, respectively. Year-by-year seizure outcomes based on
Engel's classification are presented in Table II and Fig. 2.
| Table II.Year-by-year seizures by Engel
class. |
Table II.
Year-by-year seizures by Engel
class.
|
| Patients, n
(%) |
|---|
|
|
|
|---|
| Follow-up | Class I | Classes II–IV |
|---|
| 1 year | 87/121 (71.9) | 34/121 (28.1) |
| 2 years | 83/116 (71.6) | 33/116 (28.4) |
| 3 years | 69/91
(75.8) | 22/91
(24.2) |
| 4 years | 41/52
(78.8) | 11/52
(21.2) |
| 5 years | 11/16
(68.8) |
5/16 (31.2) |
Identification of variables
distinguishing between seizure and seizure-free groups
Univariate analysis indicated no statistically
significant difference between the seizure and seizure-free groups
in gender, age at onset of seizures, age at surgery, history of
traumatic brain injury, perinatal anoxia, intracranial infection,
family history of seizures, presence of auras and site of surgery.
By contrast, significant differences were detected in pre-surgical
duration <10 years, history of febrile seizures, seizure type,
MRI and video-EEG results between the two groups. The outcomes of
analyses between the seizure-free and seizure groups are presented
in Tables III–V.
| Table III.Analysis of identifying variables
between seizure-free and seizure groups. |
Table III.
Analysis of identifying variables
between seizure-free and seizure groups.
| Quantitative
variables | Seizure-free
(n=87) | Seizure (n=34) | P-value |
|---|
| t-test |
|
|
|
| Age at
surgery (years) | 26.97±11.70 | 29.21±11.81 | 0.347 |
| Age at
onset of seizure (years) | 16.44±12.33 | 16.12±12.37 | 0.897 |
|
Pre-surgical duration
(years) | 10.39±7.56 | 11.89±7.61 | 0.329 |
| Rank sum test |
|
|
|
|
Duration of seizures
(sec) | 136.67±170.44 | 146.67±218.20 | 0.908 |
| Seizure
frequency (n/month) | 23.37±46.34 | 40.94±83.81 | 0.935 |
| Table V.Analysis of identifying variables
between seizure-free and seizure groups. |
Table V.
Analysis of identifying variables
between seizure-free and seizure groups.
| Qualitative
variables | Seizure-free
(n=87) | Seizure (n=34) | P-value |
|---|
| Video-EEG
results |
|
| 0.003 |
|
Bilateral lobes | 7 | 7 |
|
|
Unilateral multi-lobes | 8 | 9 |
|
|
Unilateral local lobe | 72 | 18 |
|
| Seizure types |
|
| 0.001 |
|
Frequent GTCS | 7 | 12 |
|
|
Frequent CPS | 57 | 15 |
|
| Simple
CPS | 23 | 7 |
|
The Rank sum test indicated no statistically
significant difference between the seizure and seizure-free groups
with regard to duration of seizures and seizure frequency prior to
surgery. However, the RxC χ2 test revealed a
statistically significant difference in video-EEG results and
seizure types between the two groups. Furthermore, the subdividing
RxC table test showed that the seizure outcomes for unilateral
local lobe involvement differed in comparison with those for
multiple lobe involvement (including unilateral multi-lobes and
bilateral lobes) and that seizure outcomes involving CPS differed
from those of frequent CPS and frequent GTCS (Table V).
On the basis of a backward stepwise multiple
logistic regression analysis, the presence of a number of
pre-surgical risk factors, including pre-surgical seizure duration,
history of febrile seizures, seizure types, MRI and video-EEG
results were associated with poor prognosis. However, other
factors, including gender, presence of auras, age at seizure onset,
age at surgery, duration of seizures, seizure frequency per month
prior to surgery, history of perinatal anoxia, intracranial
infection or traumatic brain injury, and a family history of
seizure were not associated with prognosis (Table VI).
| Table VI.Backward stepwise multiple logistic
regression. |
Table VI.
Backward stepwise multiple logistic
regression.
|
| Engel
classification |
|---|
|
|
|
|---|
| Parameter | Regression
coefficient | P-value |
|---|
| Pre-surgical
seizure duration <10 years |
1.100 | 0.019 |
| History of febrile
seizures |
1.755 | 0.002 |
| Seizure types |
1.232 | 0.017 |
| Video-EEG
findings |
1.321 | 0.012 |
| MRI (positive) |
1.441 | 0.005 |
| Constant | −7.500 | 0.001 |
Discussion
MTLE is the most common type of temporal lobe
epilepsy (TLE), and surgery is the most effective treatment
available at present for this condition (1,2,5,6,20). Since the causes of surgical failure
are not understood, epilepsy surgery is underutilized. Surgical
approaches include ATL, amygdalohippocampectomy and
lesionectomy/corticectomy. Various alternative methods of resecting
MTLE have been discussed since ATL was first developed by Falconer
and Taylor (21). However, at
present ATL remains the predominant surgical option for MTLE
(5–7)
and the seizure outcomes following ATL have been extensively
studied (6–8,18).
Prognostic factors for the long-term surgical outcomes of MTLE
include early postoperative seizures (22,23),
duration of seizures (24,25), age at surgery (24–26),
history of febrile seizures (11,27),
concordant interictal epileptiform abnormalities (20,28,29) and
GTCS or the presence of status epilepticus prior to surgery
(7,10,29,30).
However, there are few systematic studies regarding the prediction
of long-term seizure-free outcome following ATL. In addition, the
previous studies regarding the surgical outcomes of MTLE are
conflicting. The discrepancies in these predictive factors may be
associated with the differences in the pathological substrates used
and methodological problems of the study population (6,31).
The aim of the present study was to identify
prognostic factors that are able to predict the surgical outcome in
patients with MTLE at 1–5 years after ATL, according to the
well-established Engel classification system. The results of 121
patients that had undergone a range of pre-surgical evaluations,
including medical history, clinical presentation, MRI and video-EEG
observations, are reported. Among these patients, 71.9% with MTLE
became seizure free and the remaining 28.1% patients continued to
exhibit seizure symptoms at the first follow-up period, which was
consistent with the results of previous studies (6,7,26). Seizure relief rates have ranged
between 67 and 84% for the surgical treatment of MTLE in recent
studies (6,7,26) with a
median rate of ~70% (6). This
outcome may further support the use of early ATL for the treatment
of MTLE. However, in the present study, the seizure-free rate of
the patients had decreased by 5 years after surgery and the
seizure-free rates >5 years after surgery are unknown.
Therefore, the therapeutic efficacy of surgery after 5 years cannot
be predicted. Furthermore, certain predictors of the long-term
surgical outcomes following ALT for MTLE may differ from the
variables that predict short-term outcome. In the present study,
univariate and multivariate analyses indicated that factors
including pre-surgical seizure duration, history of febrile
convulsions, seizure types, MRI and video-EEG results exhibited
statistically significant differences between the seizure and
seizure-free group, and these factors were associated with the
surgical outcomes of the patients.
In the present study, of the 64 patients with a
seizure duration <10 years, 41 (64%) were in the seizure-free
group and 23 (36%) were in the seizure-free group. Of the 57
patients with a pre-surgical seizure duration of ≥10 years, 46
patients (80.7%) belonged to the seizure-free group and 11 patients
(19.3%) were in the seizure group. The Pearson's χ2 test
indicated a statistically significant difference in seizure outcome
between the two groups (P=0.042). Backward stepwise logistic
regression further demonstrated that a pre-surgical duration of
<10 years predicted a seizure-free 5-year outcome. In addition,
previous studies have demonstrated that patients with a longer
pre-surgical seizure duration exhibit a poor outcome, and are more
likely to exhibit large epileptogenic zones and more diffuse
lesions, which are difficult to eradicate with surgery (32,33). On
the basis of these observations, it was hypothesized for the
purposes of the present study that epilepsy duration may be a key
predictive factor of long-term surgical outcome.
In addition, it was observed that a history of
febrile seizures was a predictor for surgical outcome following ALT
according to backward logistic analysis. Among the 121 patients
were followed up, 63 cases (52.1%) had a history of febrile
seizures while 58 (47.9%) had no history of febrile seizures, which
is consistent with a previous study by Pavlidou et al
(34), in which patients with a
history of febrile seizures comprised ~40% of TLE cases,
particularly in children aged <4 years (34). Among the 63 patients with a history
of febrile seizures, 58 (92.1%) were classified as seizure-free,
which was significantly different from the rate among the 58
patients with no history of febrile seizures (29/58, 50.0%). This
observation indicates that the structural and functional anatomy of
the brain was altered, becoming more susceptible to intractability
following febrile seizures (11,27,34).
On the basis of univariate and multivariate
analysis, seizure types were found to be associated with long-term
surgical outcome evaluated ≤5 years following surgery. A
χ2 test revealed statistically significant differences
in seizure outcome between simple CPS and frequent CPS or frequent
GTCS. Furthermore, it was observed that 19 patients (15.7%)
exhibited frequent GTCS, including 7 patients (36.8%) that had a
good outcome and 12 patients (63.2%) with a poor outcome. These
results indicate that GTCS was associated with a worse outcome.
Theoretically, patients with CPS would be expected to exhibit an
improved outcome compared with patients with frequent CPS, based on
previous studies (13,22). By contrast, it was observed that
57/72 patients (79.2%) with frequent CPS were seizure-free, while
23/30 patients (76.7%) with simple CPS exhibited improved seizure
control. This result may be due to epileptogenic zones in patients
with GTCS being difficult to localize and resect, resulting in the
postoperative formation of a residual epileptogenic area.
With respect to video-EEG results, 72/90 patients
(80.0%) with unilateral local lobe involvement, 8/17 patients
(47.1%) with unilateral multi-lobe involvement and 7/14 patients
(50.0%) with bilateral lobe involvement exhibited a seizure-free
outcome. Furthermore, positive video-EEG results were a predictor
of surgical outcome, which indicates that patients with unilateral
lobe involvement may expect an improved outcome compared with
patients with bilateral lobe involvement. Therefore, the present
study detected a significant predictive contribution of video-EEG
data, particularly in patients with MTLE or with normal MRI
results, which is similar to the findings of previous studies
(7,10,14,32).
However, in other studies, discrepancies between video-EEG and MRI
results indicated a poor surgical outcome, which may be due to the
existence of bilateral HS or multi-lobe foci (16,35).
Finally, 77/101 patients (76.2%) with positive MRI
were seizure-free and 24/101 patients (23.8%) were in the seizure
group, indicating that MRI may be useful for the pre-surgical
evaluation of epilepsy patients. On the basis of multiple logistic
regression analysis, it was determined that the presence of MRI
abnormalities was highly predictive of long-term patient outcome.
Furthermore, various MRI results, particularly the presence of
mesial temporal sclerosis, were identified as predictive of
surgical outcomes, which is consistent with previous studies that
reported a poor outcome for patients that exhibited no signs of
MTLE under MRI (33,36–39). In
addition, discrepancies between MRI and histopathological results
regarding MTLE may be due to the fact that current MRI protocols
only provide accurate information in patients with severe bilateral
HS or with a significant difference in the bilateral hippocampus.
Therefore, the majority of patients with mild unilateral HS and
severe contralateral HS are diagnosed with unilateral HS, while
patients with mild bilateral HS are considered to be normal
(31,35). Although these patients underwent
preoperative MRI examinations, for the majority of patients MRI
results were not available for each year during the follow-up
period. Thus, the structural changes occurring in the brain
following surgery are unknown, particularly with respect to the
residual hippocampal tissue following ATL, which was a common cause
of recurrent seizures, and further studies are required to
investigate this in the future.
In the present study, it was demonstrated that the
majority of patients with MTLE may be treated effectively with an
ATL. A number of pre-surgical factors, including pre-surgical
seizure duration, history of febrile convulsion, seizure type, MRI
and video-EEG results may be used as predictors of surgical
outcomes. Thus, postoperative remission may be achieved in patients
with MTLE via the accurate collection of patient information and
adequate pre-surgical evaluation. Further studies are required that
include a larger group of patients with a longer follow-up period,
in order to analyze the rate of late seizure recurrence after an
initial seizure-free period. In addition, year-by-year MRI
examination and comparisons between MRI and video-EEG results may
aid in ascertaining surgical outcomes.
Acknowledgements
The authors thank Wenhan Hu and Ning Chen for
collecting the data from the archive, as well as Chao Zhang for
technical help.
References
|
1
|
Engel J Jr: The timing of surgical
intervention for mesial temporal lobe epilepsy: A plan for a
randomized clinical trial. Arch Neurol. 56:1338–1341. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wieser HG: ILAE commission on neurosurgery
of epilepsy: ILAE commission report. Mesial temporal lobe epilepsy
with hippocampal sclerosis. Epilepsia. 45:695–714. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Engel J Jr: Mesial temporal lobe epilepsy:
What have we learned? Neuroscientist. 7:340–352. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wieser HG and Hane A: Antiepileptic drug
treatment in seizure-free mesial temporal lobe epilepsy patients
with hippocampal sclerosis following selective
amygdalohippocampectomy. Seizure. 13:534–536. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Berkovic SF, McIntosh AM and Kalnins RM:
Preoperative MRI predicts outcome of temporal lobectomy: An
actuarial analysis. Neurology. 45:1358–1363. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
McIntosh AM, Wilson SJ and Berkovic SF:
Seizure outcome after temporal lobectomy: current research practice
and findings. Epilepsia. 42:1288–1307. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Radhakrishnan K, So EL, Silbert PL, et al:
Predictors of outcome of anterior temporal lobectomy for
intractable epilepsy: A multivariate study. Neurology. 51:465–471.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Blume WT, Desai HB, Girvin JP, McLachlan
RS and Lemieux JF: Effectiveness of temporal lobectomy measured by
yearly follow-up and multivariate analysis. J Epilepsy. 7:203–214.
1994. View Article : Google Scholar
|
|
9
|
Guldvog B, Løyning Y, Hauglie-Hanssen E,
Flood S and Bjørnas H: Predictive factors for success in surgical
treatment for partial epilepsy: A multivariate analysis. Epilepsia.
35:566–578. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hennessy MJ, Elwes RD, Rabe-Hesketh S,
Binnie CD and Polkey CD: Prognostic factors in the surgical
treatment of medically intractable epilepsy associated with mesial
temporal sclerosis. Acta Neurol Scand. 103:344–350. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Janszky J, Schulz R and Ebner A: Clinical
features and surgical outcome of medial temporal lobe epilepsy with
a history of complex febrile convulsions. Epilepsy Res. 55:1–8.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Specht U, May T, Schulz R, et al:
Cerebellar atrophy and prognosis after temporal lobe resection. J
Neurol Neurosurg Psychiatry. 62:501–506. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Semah F, Picot MC, Adam C, et al: Is the
underlying cause of epilepsy a major prognostic factor for
recurrence? Neurology. 51:1256–1262. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Schulz R, Lüder HO, Hoppe M, Tuxhorn I,
May T and Ebner A: Interictal EEG and ictal scalp EEG propagation
are highly predictive of surgical outcome in mesial temporal lobe
epilepsy. Epilepsia. 41:564–570. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Spencer SS, Berg AT, Vickrey BG, et al:
Initial outcomes in the multicenter study of epilepsy surgery.
Neurology. 61:1680–1685. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bote RP, Blázquez-Llorca L, Fernández-Gil
MA, Alonso-Nanclares L, Muñoz A and De Felipe J: Hippocampal
sclerosis: Histopathology substrate and magnetic resonance imaging.
Semin Ultrasound CT MR. 29:2–14. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Camacho DLA and Castillo MMR: Imaging of
temporal lobe epilepsy. Semin Ultrasound CT and MRI. 28:424–436.
2007. View Article : Google Scholar
|
|
18
|
Tanriverdi T, Olivier A, Poulin N,
Andermann F and Dubeau F: Long-term seizure outcome after mesial
temporal lobe epilepsy surgery: Corticalamygdalohippocampectomy
versus selective amygdalohippocampectomy. J Neurosurg. 108:517–524.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Bancaud J, Henriksen O, Rubio-Donnadieu F,
Seino M, Dreifuss FE and Penry JK: Commission on the Classification
and Terminology of the International League Against Epilepsy:
Proposal for revised clinical and electroencephalographic
classification of epileptic seizures. Epilepsia. 22:489–501. 1981.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wiebe S, Blume WT, Girvin JP and Eliasziw
M: Effectiveness and efficiency of surgery for temporal lobe
epilepsy study group. A randomized, controlled trial of surgery for
temporal-lobe epilepsy. N Engl J Med. 345:311–318. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Falconer MA and Taylor DC: Surgical
treatment of drug-resistant epilepsy due to mesial temporal
sclerosis: Etiology and significance. Arch Neurol. 19:353–361.
1968. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
McIntosh AM, Kalnins RM, Michell LA and
Berkovic SF: Early seizures after temporal lobectomy predict
subsequent seizure recurrence. Ann Neurol. 57:283–288. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Tezera FI, Akalanb N, Oguzc KK, Karabulut
E, Dericioglu N, Ciger A and Saygi S: Predictive factors for
postoperative outcome in temporal lobe epilepsy according to two
different classifications. Seizure. 17:549–560. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Clusmann H, Schramm J, Kral T, et al:
Prognostic factors and outcome after different types of resection
for temporal lobe epilepsy. J Neurosurg. 97:1131–1141. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zentner J, Hufnagel A, Wolf HK, et al:
Surgical treatment of temporal lobe epilepsy: Clinical,
radiological and histopathological findings in 178 patients. J
Neurol Neurosurg Psychiatry. 58:666–673. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Jeong SW, Lee SK, Kim KK, Kim H, Kim JY
and Chung CK: Prognostic factors in anterior temporal lobe
resections for mesial temporal lobe epilepsy: Multivariate
analysis. Epilepsia. 40:1735–1739. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Behrens E, Zentner J, van Roost D,
Hufnagel A, Elger CE and Schramm J: Subdural and depth electrodes
in the presurgical evaluation of epilepsy. Acta Neurochir (Wien).
128:84–87. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Foldvary N, Nashold B, Mascha E, et al:
Seizure outcome after temporal lobectomy for temporal lobe
epilepsy: A Kaplan-Meier survival analysis. Neurology. 54:630–634.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ho SS, Berkovic SF, McKay WJ, Kalnins RM
and Bladin PF: Temporal lobe epilepsy subtypes: Differential
patterns of cerebral perfusion on ictal SPECT. Epilepsia.
37:788–795. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Clusmann H, Kral T, Fackeldey E, et al:
Lesional mesial temporal lobe epilepsy and limited resections:
Prognostic factors and outcome. J Neurol Neurosurg Psychiatry.
75:1589–1596. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Schramm J: Temporal lobe epilepsy surgery
and the quest for optimal extent of resection: A review. Epilepsia.
49:1296–1307. 2008.PubMed/NCBI
|
|
32
|
Holmes MD, Born DE, Kutsy RL, Wilensky AJ,
Ojemann GA and Ojemann LM: Outcome after surgery in patients with
refractory temporal lobe epilepsy and normal MRI. Seizure.
9:407–411. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Sperling MR, Saykin AJ, Glosser G, et al:
Predictors of outcome after anterior temporal lobectomy: The
intracarotid amobarbital test. Neurology. 44:2325–2330. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Pavlidou E, Tzitiridou M, Kontopoulos E
and Panteliadis CP: Which factors determine febrile seizure
recurrence? A prospective study. Brain Dev. 30:7–13. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Vinton AB, Carne R, Hicks RJ, et al: The
extent of resection of FDG-PET hypometabolism relates to outcome of
temporal lobectomy. Brain. 130:548–560. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Antel SB, Li LM, Cendes F, et al:
Predicting surgical outcome in temporal lobe epilepsy patients
using MRI and MRSI. Neurology. 58:1505–1512. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Clusmann H: Predictors, procedures and
perspective for temporal lobe epilepsy surgery. Semin Ultrasound CT
MR. 29:60–70. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Gilliam F, Bowling S, Bilir E, et al:
Association of combined MRI, interictal EEG, and ictal EEG results
with outcome and pathology after temporal lobectomy. Epilepsia.
38:1315–1320. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Pillai JJ, Williams HT and Faro S:
Functional imaging in temporal lobe epilepsy. Semin Ultrasound CT
MR. 28:437–450. 2007. View Article : Google Scholar : PubMed/NCBI
|