Introduction
Chronic kidney disease (CKD), a worldwide problem
with a high incidence, is commonly accompanied by inflammation and
anemia. Between 6.5 and 10% of the population in developed
countries suffer from various renal diseases (1). CKD is a condition, which is
characterized by chronic inflammation and is hypothesized to be
promoted by cytokines and oxidation reactions. The inflammation can
be induced by toxins, immune complexes, microorganisms, chemical
agents and complement, and is activated by the monocyte-macrophage
system during which tumor necrosis factor (TNF)-α, interleukin
(IL)-6 and other agents are released (1). However, the underlying pathogenesis of
the numerous forms of CKD remains unclear.
Expression of resistin, a cysteine-rich secretory
plasma protein (molecular weight, ~12.5 kDa), is correlated with
the expression of TNF-α, IL-6, lipoprotein-associated phospholipase
A2 and other factors, which indicates that it may be involved in
various inflammatory events. A number of studies have identified
that resistin was involved in insulin resistance and metabolic
syndromes in renal diseases (1–3) and CKD
patients on maintenance hemodialysis often succumbed to
cardiovascular and cerebrovascular complications (4). Elevation of resistin levels may serve
as a marker of atherosclerosis (AS) in patients exhibiting a
metabolic syndrome, indicating that resistin may be key in the
occurrence and development of coronary AS (1–3) as well
as demonstrating that there may be a correlation between resistin
levels and heart disease in CKD patients.
Anemia often occurs in CKD patients and is closely
associated with a high incidence of cardiovascular disease.
Recombinant human erythropoietin (EPO) has been administered to CKD
patients presenting with anemia in addition to undergoing
hemodialysis. However, there is evidence that a high dose of EPO
may be associated with an increased rate of mortality. Boyraz et
al (2) demonstrated that
administration of a high dose of EPO to treat anemia may lead to an
increase in mortality. Chen et al (3) reported that EPO responses and targeted
hemoglobin (Hb) values may serve as markers of mortality risk.
Therefore, prescribing an excessive dose of EPO for CKD patients
may increase mortality. Moreover, EPO was involved in inflammation
(2) and the inflammation inhibited
the activity of EPO and, thus, erythropoiesis of CKD patients,
which indicated that there may be a correlation between
inflammation and EPO responsiveness in CKD patients. As changes in
the levels of EPO and resistin may be involved in the occurrence
and progression of CKD, the correlation between serum resistin and
variability to EPO responsiveness, in tissue samples obtained from
CKD patients, was investigated in the present study.
Materials and methods
Materials
An enzyme-linked immunosorbent assay (ELISA) kit for
detecting human resistin was obtained from Quantikine (Minneapolis,
MN, USA) and IL-6 was purchased from Invitrogen Life Technologies
(Carlsbad, CA, USA). Recombinant EPO was purchased from Life
Sciences Advanced Technologies (St. Petersburg, FL, USA) and
additional reagents were purchased from Sigma-Aldrich (St. Louis,
MO, USA).
Patients
The CKD patients (n=138) and healthy control
subjects (n=16) were recruited from the First Hospital Affiliated
to Bethune Medical College of Jilin University (Changchun, China)
between May 2009 and May 2012. Ethical approval was obtained from
the institutional review committee of Jilin University (Changchun,
China) and informed consent was obtained from the participants
according to the Declaration of Helsinki (4). The samples were analyzed by routine
blood tests to determine coagulation, liver and renal function, as
well as the levels of blood sugar, blood lipids (high density
lipoproteins and low density lipoproteins), ions and parathyroid
hormone. In addition, gender, age, dialysis duration, systolic and
diastolic blood pressure and cardiac functional grades were
recorded.
Patient grouping
One hundred and thirty-eight CKD patients were
divided into two groups; one group did not receive hemodialysis and
the second group did. The healthy subjects served as a control
group and the patients in the second group (the hemodialysis
group), were randomly selected. The patients of the third group, a
subset of the second group, were subjected to hemodialysis for
>3 months in addition to intravenous EPO therapy to maintain a
Hb level of 11.0 g/l.
The CKD groups without dialysis were designated as
CKD3, 4 and 5. The CKD3 group comprised of six males and five
females (mean age, 39.8±4.9 years), the CKD4 group comprised of six
males and six females (mean age, 48.0±4.9 years) and the CKD3 group
comprised of eight males and six females (mean age, 38.9±17.5
years).
The CKD patients, who received dialysis, were
divided into two groups as described above; the first group
included 21 males and 18 females (mean age, 47.5±23.8 years) and
the second group included 33 males and 29 females (mean age,
53.5±21.9 years) with a dialysis time of 39.8±15.7 months. The
first group was dialyzed three times per week for four hours each
time using a 4008s dialysis machine (Fresenius Medical Care,
Waltham, MA, USA). Blood flow was measured at 200–220 ml/min using
bicarbonate as the dialysate and a dialysis rate of 500 ml/min.
The patients in the second CKD group, who underwent
dialysis, received dialysis and treatment for >3 months and were
injected with EPO to maintain Hb levels of 11.0 g/l. The patients
that were receiving dialysis were also administered with ferrous
sulfate and oral folic acid to maintain serum ferritin levels at
>100 ng/ml and transferrin saturation (TSAT) at >20%.
The CKD patients, who received hemodialysis, were
administered with ferrous sulfate and folate to maintain serum
ferritin levels at >100 ng/ml and TSAT at >20%. When the
serum ferritin levels were <100 ng/ml and TSAT <20%, the
patients who were subjected to 10 continuous cycles of hemodialysis
were administered with 100 mg iron hydroxide or were removed from
the study (1–3). In addition, when serum ferritin levels
were ≥800 ng/ml and TSAT ≥50%, the patients were excluded from the
study.
The healthy control group included nine males and
seven females (mean age, 37.6±10.5 years).
Blood preparation
Blood was drawn from a vein in the arm and mixed
with sodium citrate, which served as an anti-coagulant. The blood
was sent to the clinical laboratory from the First Hospital
Affiliated to Bethune Medical College of Jilin University for
further experiments. The samples were centrifuged at 460 × g
(Allegra X-15 R centrifuge, Beckman Coulter, Brea, CA, USA) for 8
min at room temperature and the supernatant was obtained and
subjected to determine the levels of serum creatinine (SCr), blood
urea nitrogen and serum albumin.
ELISA
All of the samples were subjected to routine blood
analysis. The levels of SCr, serum C-reactive protein (CRP), serum
total cholesterol, triglycerides, IL-6 and serum resistin were
detected in all of the groups using sandwich ELISA. ELISA assays
were performed as previously reported (5). Briefly, 100 µl diluent was added to
each well of an RD1-19 plate (Sigma, St. Louis, MO, USA) in
addition to 100 µl standard solution, control solution and sample.
The wells were blocked using a rubber sealing bar and the mixture
was incubated for 2 h at room temperature. Each well was washed
three times with four repetitions each time and 200 µl resistin
conjugating agent was added. The wells were blocked an additional
time, using a rubber-sealing bar and incubated for 2 h at room
temperature. Subsequent to washing each well again, a substrate
solution was added and the reactions were conducted in the dark for
30 min at room temperature. Stopping buffer (50 µl) was added and
the solutions were gently mixed, the change in the color of the
solution in each well from blue to yellow, indicated that the
reaction was finished. The light intensity of each well was
measured after 30 min using an ELISA reader (Sigma) with an
absorbance of 450 nm.
The measurement of CRP was conducted using a
fully-automated DADE Behring BN ProSpec (Beckman Coulter) using
ancillary reagents. Immunosuppressant rate nephelometry was used
according to the manufacturer's instructions.
The level of human IL-6 was measured via an ELISA
method with an ELISA kit (Invitrogen Life Technologies) according
to the manufacturer's instructions.
The estimated glomerular filtration rate (eGFR) was
calculated using the following revised equation, termed the
modification of diet in renal disease (6): eGFR = 186 × (SCr)−1.154 ×
(age)−0.203 × 0.742 (for females). Where the units are:
eGFR, ml/min/1.73 m2; SCr, mg/dl and age, years.
The EPO resistance index (ERI) was defined as: EPO
dose/Hb unit/body weight/week.
Data analysis
Data are presented as means ± standard deviation and
the statistical significance between the means was analyzed using
one-way analysis of variance and the χ2 test and
Student's t-test were performed using SPSS 16.0 software (SPSS
Inc., Chicago, IL, USA). Fisher's exact test was used to analyze
the correlations between the levels of resistin and variability to
EPO responsiveness in the CKD patients. P<0.05 and P<0.01
were considered to indicate statistically significant
differences.
Results
Clinical data
The clinical data and demographics of the study
participants, including gender, age and length of dialysis are
shown in Table I.
 | Table I.Clinical data of study
participants. |
Table I.
Clinical data of study
participants.
|
| CKD group without
hemodialysis | Hemodialysis CKD
group |
|
|---|
|
|
|
|
|
|---|
| Variable | CKD3 | CKD4 | CKD5 | 1 | 2 | group |
| Case number | 11 | 12 | 14 | 39 | 62 | 16 |
| Gender (m/f) | 6/5 | 6/6 | 8/6 | 21/18 | 33/29 | 9/7 |
| Age (years) |
39.8±4.9 |
48.0±4.9 |
38.8±17.5 |
47.5±23.8 |
53.5±21.9 |
37.6±10.5 |
| BMI |
25.1±3.7 |
23.3±4.7 |
23.5±3.4 |
23.2±3.7 |
23.0±4.3 |
22.0±3.1 |
| Dialysis time |
|
|
|
|
|
|
| (months) | – | – | – |
40.1±15.9 |
39.8±15.7 | – |
| Hb (g/l) |
128±22 |
107±14 |
92.7±19.4 |
87.5±17.6 |
104±7 |
123±20 |
| HCT |
0.36±0.02 |
0.28±0.05 |
0.26±0.08 |
0.21±0.09 |
0.30±0.02 |
0.42±0.03 |
| Alb (g/l) |
37.5±4.3a |
35.0±5.2a |
33.9±5.3a |
30.4±8.2a |
31.0±4.4a |
47.9±4.2 |
| TC (mmol/l) |
4.59±1.02a |
4.88±1.10a |
5.04±1.19 |
5.28±1.37a |
5.37±1.36 |
4.27±1.41 |
| TG (mmol/l) |
2.29±1.79a |
1.91±0.73a |
1.73±0.94a |
2.83±0.71a |
2.96±0.81a |
1.34±0.51 |
| HDL (mmol/l) |
1.23±0.41a |
1.09±0.34a |
0.99±0.15a |
0.75±0.09a |
0.80±0.02a |
1.42±0.63 |
| LDL (mmol/l) |
2.57±0.74a |
2.39±0.87a |
2.34±0.81a |
2.57±0.64a |
2.53±0.68a |
2.34±0.46 |
| SCr (µmol/l) |
231±69a |
564±96a |
1280±311a |
793±296a |
776±258a |
60.8±10.6 |
| CRP (mg/l) |
4.28±4.84a |
5.30±4.24a |
7.06±4.31a |
4.94±2.73ab |
5.23±3.19ab |
1.89±0.47 |
| IL-6 (ng/ml) |
2.05±1.03a |
2.21±1.37a |
3.17±1.05a |
5.61±5.13ab |
5.42±5.53ab |
1.57±0.91 |
| EPO (IU) |
1.58±0.22 |
1.76±0.68 |
1.83±1.12 |
1.91±1.37 |
1.97±1.23 |
1.45±1.02 |
| Resistin
(ng/ml) |
9.48±4.11a |
14.1±6.7a |
19.3±7.1a |
23.1±4.2ab |
22.6±5.6ab |
8.72±2.32 |
Levels of resistin in CKD samples
The serum resistin levels in the patients in the CKD
groups who were not dialyzed, and in those in the hemodialysis CKD
group were identified to be significantly higher than those in the
control group (P<0.01). The levels of serum resistin in the
hemodialysis CKD group were higher than those observed in the CKD
groups without dialysis (P<0.01). There was a marked difference
between the hemodialysis patient groups 1 and 2 with regards to
level of resistin (P<0.05; Table
I).
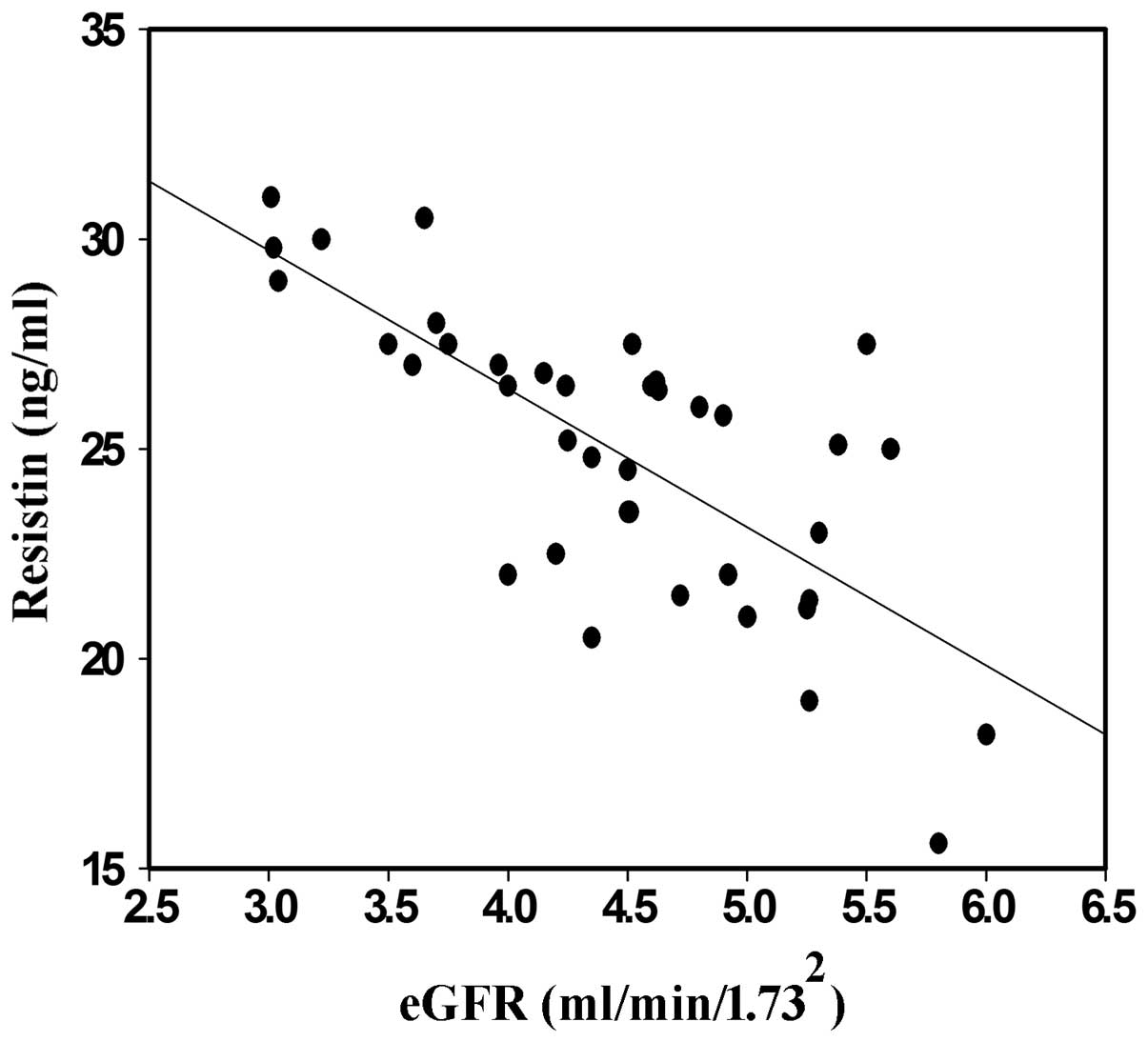
Correlation between resistin and
eGFR
The kidneys of the CKD patients and the control
subjects were subjected to eGFR analysis via an enzymatic method
and the correlation analysis was performed using resistin. The
level of resistin increased in the CKD3, 4 and 5 groups without
dialysis and statistically significant differences were identified
between these three groups. However, no significant difference was
identified among the groups with dialysis. These data indicated
that serum resistin and eGFR were correlated (Fig. 1).
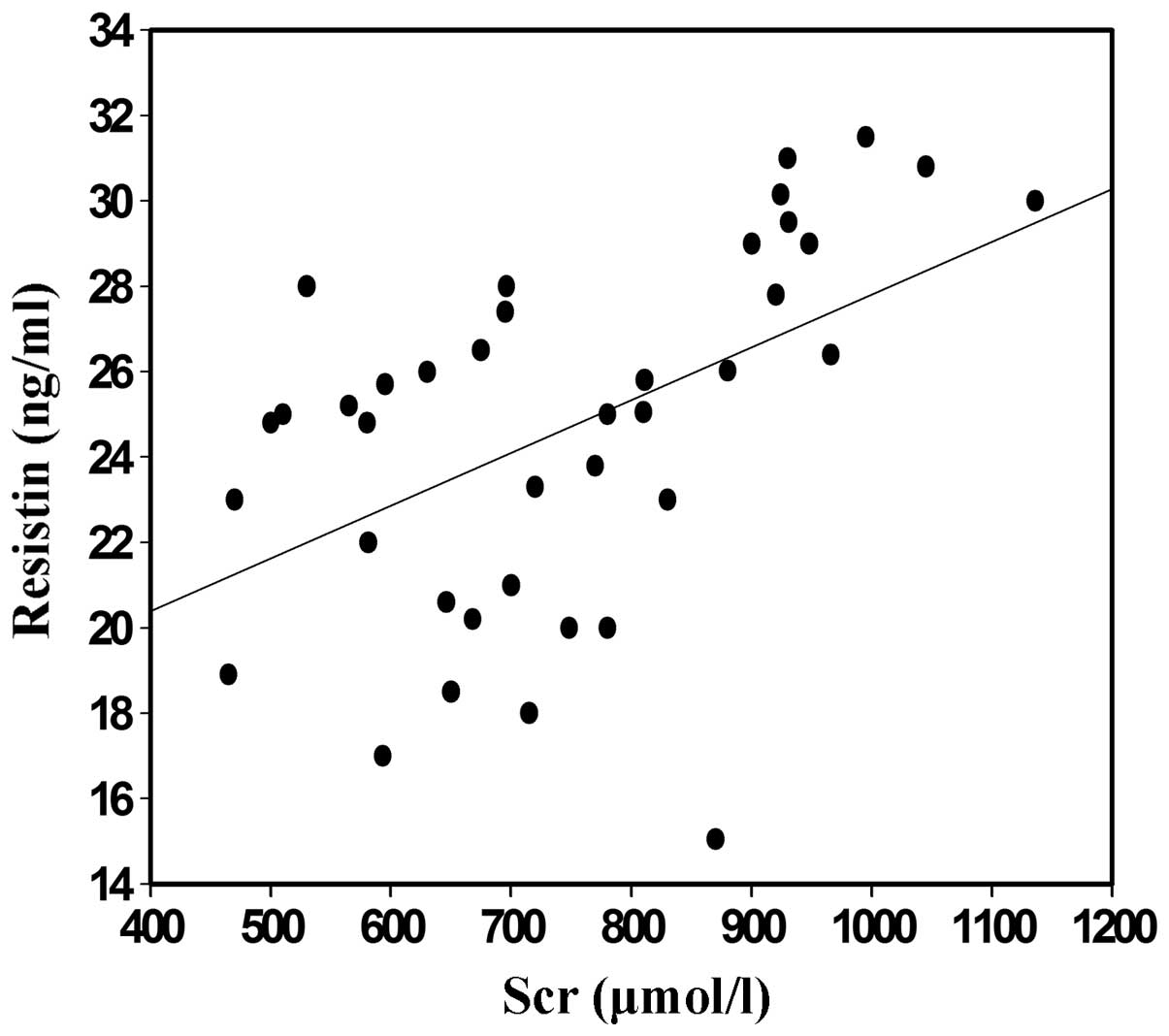
Correlation between resistin and
SCr
The blood samples of the CKD patients and the
control subjects were collected and subjected to ELISA analysis.
The levels of serum resistin in the randomly selected CKD group
with hemodialysis indicated positive correlation with the levels of
SCr (P<0.05; Fig. 2).
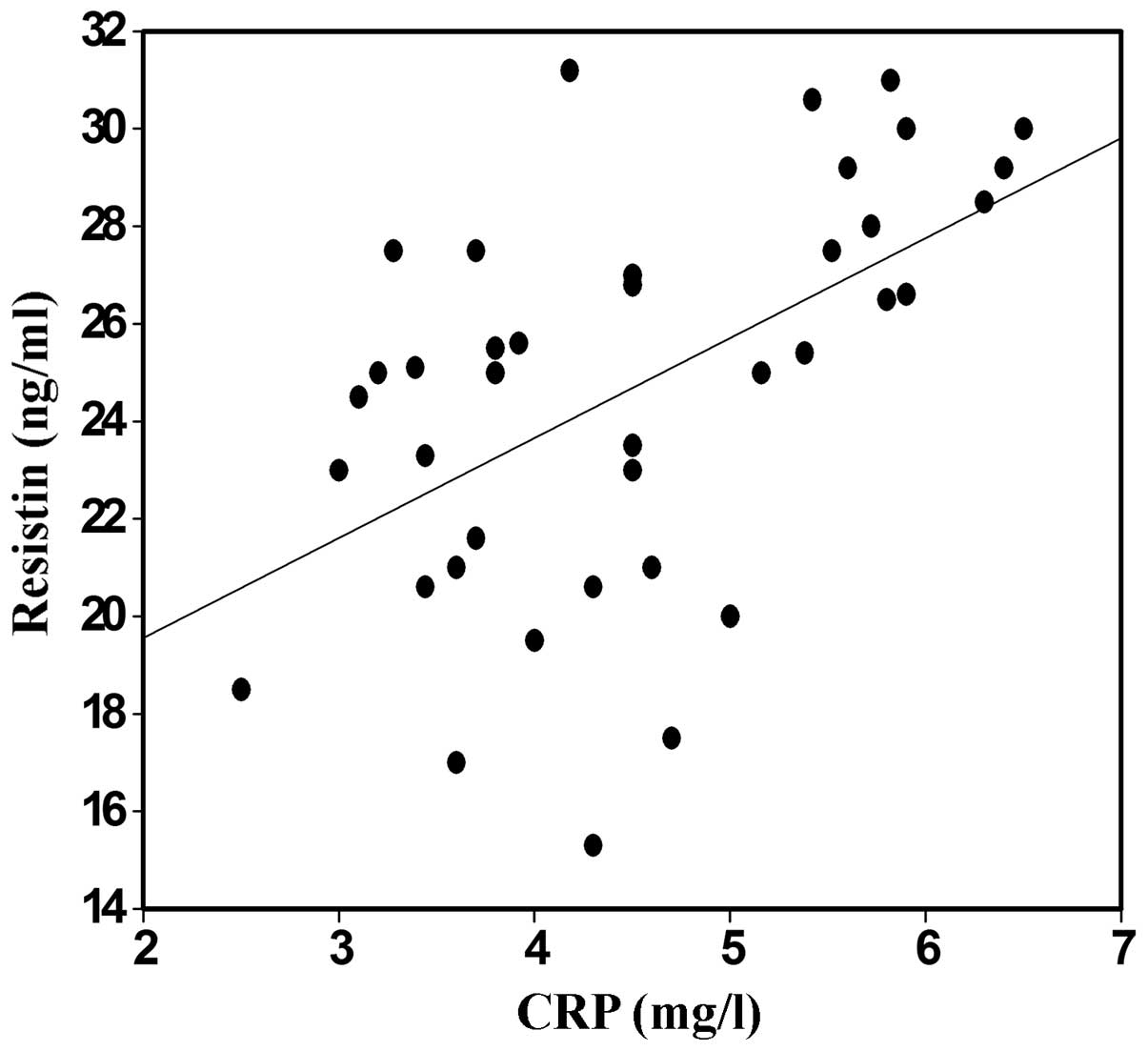
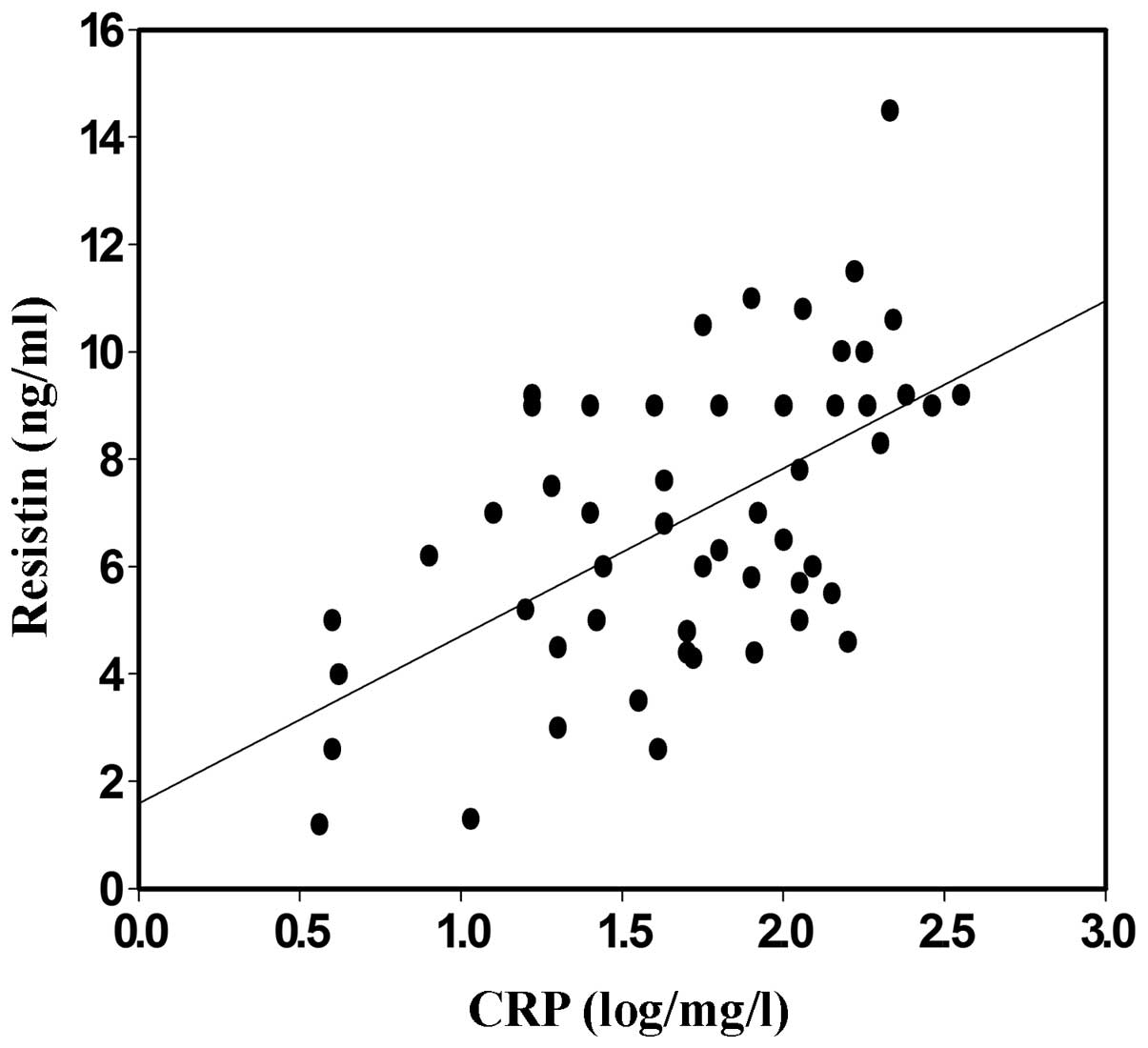
Correlation between resistin and
CRP
To investigate the clinical correlation between the
highly sensitive CRP and serum resistin in the CKD patients treated
with EPO, the levels of CRP were detected and compared with those
of resistin. The serum levels of resistin in the randomly selected
CKD group with hemodialysis were positively correlated with the
levels of CRP (Figs. 3 and 4; P<0.05).
Discussion
In the present study, the data demonstrated that the
serum resistin levels correlated with the variability in EPO
responsiveness that was observed in CKD patients, indicating that
serum resistin may serve as a marker for the occurrence and
development of CKD. This conclusion is supported by numerous lines
of evidence; the levels of serum resistin in CKD groups with and
without hemodialysis were significantly higher than those observed
in the normal control group (P<0.01). Furthermore, the levels of
serum resistin in the hemodialysis CKD group were higher than those
of the CKD group without dialysis (P<0.01). No marked difference
was identified between the two groups of hemodialysis patients
regarding the levels of resistin (P>0.05). Moreover, the levels
of serum resistin in the randomly selected CKD group with
hemodialysis were positively correlated with the duration of the
dialysis period, the levels of SCr and CRP (P<0.05); however,
they were negatively correlated with eGFR. ERI was observed to be
correlated with body mass index (BMI) and CRP and resistin levels.
In addition, EPO reactivity was determined by BMI and CRP and
resistin levels. Finally, a correlation between the level of
resistin and ERI was demonstrated.
CKD, specifically in end-stage renal disease, is a
condition in which chronic inflammation is present and one that is
hypothesized to be promoted by cytokines and oxidation reactions.
The inflammation is induced by various factors and is associated
with cytokines, such as TNF-α and IL-6 (6). In a previous study, the levels of CRP
and IL-6 were observed to be higher in CKD patients than in the
healthy control subjects, indicating that there was a
micro-inflammatory state in the CKD patients (4).
Resistin, which was initially identified in obese
diabetic patients, is a signaling molecule secreted by adipose
cells (7). Previous studies have
revealed that resistin is involved in insulin resistance and that
there is a correlation between the level of plasma resistin and
pro-inflammatory cytokines, whereas there is a negative correlation
between the level of resistin and eGFR, in CKD patients. Patients
who were on maintenance hemodialysis predominantly succumbed to
cardiovascular and cerebrovascular complications (8). Elevation of the resistin level may
serve as a marker of AS in patients who exhibit metabolic
syndromes, indicating that resistin may be key in the occurrence
and development of coronary AS. The present results supported the
conclusion of Díez et al (9),
who demonstrated a correlation between resistin and heart disease
in patients with end-stage renal disease.
Anemia commonly occurs in CKD patients and is
closely associated with a high incidence of cardiovascular disease.
Recombinant human EPO has been used in hemodialysis to treat anemia
patients in clinical applications and EPO is a mainstay in treating
anemia in CKD patients. However, there are EPO-sensitive patients
and the variability in EPO responsiveness in these patients is
considerable. Moreover, although the levels of Hb were in the
normal range, it was reported that high-dose EPO was involved in
increased instances of mortality, indicating that EPO
responsiveness and the targeted value of Hb may serve as markers
for mortality risk. Therefore, it is necessary to investigate the
variability of EPO responsiveness. It is possible that the
administration of EPO to CKD patients may increase the risk of
various diseases, and EPO and resistin may be involved in the
occurrence and progression of CKD; therefore, the correlation
between serum resistin and the variability of EPO responsiveness in
CKD patients was investigated in the present study.
Resistin is highly expressed in normal fetal liver,
adult bone, umbilical cord blood and peripheral blood cells, which
indicates that the distribution of human resistin may be associated
with hematopoiesis (10). In
addition, granulocyte colony stimulating factor (G-CSF) induces the
secretion of resistin in adipose cells in vitro and G-CSF
treatment markedly increases the levels of serum resistin (11). G-CSF is critical in inhibiting
erythropoiesis and anemia (12).
Thus, these data demonstrated a correlation between the levels of
secreted resistin and a decreased number of erythrocytes,
indicating that there may be a correlation between the level of
resistin and EPO responsiveness. The level of resistin was
previously shown to be increased in patients exhibiting insulin
resistance (9,13) and in a previous study, EPO was shown
to reverse insulin resistance by curing anemia in uremic patients
(14). Furthermore, EPO treatment
decreased the iron stores within the body to reduce the insulin
resistance and improved the chronic inflammatory state in CKD
patients (15).
The negative correlation between resistin and eGFR
may be applied to the diagnosis of CKD patients. In the second
stage of CKD (eGFR=60–89 mol/min/1.73 mm−2) (2,16–20), the
level of resistin increased markedly, whereas other polypeptide
substances were freely filtered by the kidneys. In addition, the
level of resistin was observed to increase with decreasing levels
of eGFR in CKD patients. In the present study, the level of
resistin increased in the patients in the CKD3, 4 and 5 groups
without dialysis and there was a statistically significant
difference observed among these three groups. However, there was no
difference identified among the two groups with dialysis. Moreover,
data was obtained, which indicated that the level of resistin in
CKD patients was negatively correlated with eGFR. In the present
study, the level of resistin in patients with end-stage renal
disease was higher than that of the healthy control subjects and
the level of resistin in the groups with hemodialysis was higher
than that of the renal failure groups without hemodialysis. The
present results showed that resistin was positively correlated with
dialysis time and SCr, whereas, it was negatively correlated with
eGFR. This indicated that resistin was associated with an
inflammatory state in the patients with end-stage renal disease and
was correlated with the function of the remnant kidney.
BMI has been reported to be negatively associated
with the control of anemia (19,20) and
in the present study, EPO responsiveness was negatively correlated
with BMI. However, previous studies have demonstrated that BMI was
independent of the EPO response (21). Kotanko et al (22) reported that CKD patients exhibiting a
high proportion of adipose tissue and subcutaneous fatty tissue
required less EPO and exhibited less EPO resistance. More than 100
molecules, including cytokines that are secreted by adipose tissue,
may be involved in the response to EPO. Adipose tissue participates
in energy regulation, inflammation and the immune response, in
addition to being a component of the hematopoietic
microenvironment. In the present study, there was a high
correlation observed between ERI and CRP, indicating that EPO
responsiveness is involved in inflammation. Moreover, resistin is
secreted by adipose tissue, thus, there may be a correlation
between the levels of resistin and EPO responsiveness.
In conclusion, a correlation was observed between
the levels of serum resistin and the variability of EPO
responsiveness in CKD patients, which may aid in clarifying the
underlying mechanism of CKD and may provide an improved method for
diagnosing CKD.
Acknowledgements
The present study was supported by grants from the
National Natural Science Foundation of China.
References
|
1
|
Ota T: Chemokine systems link obesity to
insulin resistance. Diabetes Metab J. 37:165–172. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Boyraz M, Cekmez F, Karaoğlu A, Cinaz P,
Durak M and Bideci A: Relationship of adipokines (adiponectin,
resistin and RBP4) with metabolic syndrome components in pubertal
obese children. Biomark Med. 7:423–428. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chen XY, Zhang JH, Liu F, Liu HM, Song YY
and Liu YL: Association of serum resistin levels with metabolic
syndrome and early atherosclerosis in obese Chinese children. J
Pediatr Endocrinol Metab. 26:855–860. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Drouet L, Bal Dit and Sollier C:
Fibrinogen: factor and marker of cardiovascular risk. J Mal Vasc.
27:143–156. 2002.(In French). PubMed/NCBI
|
|
5
|
Kim KH, Lee K, Moon YS and Sul HS: A
cysteine-rich adipose tissue-specific secretory factor inhibits
adipocyte differentiation. J Biol Chem. 276:11252–11256. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Imai E, Horio M, Nitta K, et al:
Modification of the Modification of Diet in Renal Disease (MDRD)
Study equation for Japan. Am J Kidney Dis. 50:927–937. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Steppan CM, Bailey ST, Bhat S, et al: The
hormone resistin links obesity to diabetes. Nature. 409:307–312.
2001. View
Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ren W, Pan H, Wang P, et al: Clinical
analysis of pulmonary infection in hemodialysis patients. Exp Ther
Med. 7:1713–1717. 2014.PubMed/NCBI
|
|
9
|
Díez JJ, Iglesias P, Fernández-Reyes MJ,
et al: Serum concentrations of leptin, adiponectin and resistin,
and their relationship with cardiovascular disease in patients with
end-stage renal disease. Clin Endocrinol (Oxf). 62:242–249. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Briana DD and Malamitsi-Puchner A: The
role of adipocytokines in fetal growth. Ann NY Acad Sci.
1205:82–87. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lago F, Dieguez C, Gómez-Reino J and
Gualillo O: The emerging role of adipokines as mediators of
inflammation and immune responses. Cytokine Growth Factor Rev.
18:313–325. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Papaldo P, Ferretti G, Di Cosimo S, et al:
Does granulocyte colony-stimulating factor worsen anemia in early
breast cancer patients treated with epirubicin and
cyclophosphamide? J Clin Oncol. 24:3048–3055. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Anderson PD, Mehta NN, Wolfe ML, et al:
Innate immunity modulates adipokines in humans. J Clin Endocrinol
Metab. 92:2272–2279. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Borissova AM, Djambazova A, Todorov K,
Dakovska L, Tankova T and Kirilov G: Effect of erythropoietin on
the metabolic state and peripheral insulin sensitivity in diabetic
patients on haemodialysis. Nephrol Dial Transplant.
8:931993.PubMed/NCBI
|
|
15
|
Rasic-Milutinovic Z, Perunicic-Pekovic G,
Cavala A, Gluvic Z, Bokan L and Stankovic S: The effect of
recombinant human erythropoietin treatment on insulin resistance
and inflammatory markers in non-diabetic patients on maintenance
hemodialysis. Hippokratia. 12:157–161. 2008.PubMed/NCBI
|
|
16
|
National Kidney Foundation: K/DOQI
clinical practice guidelines for chronic kidney disease:
evaluation, classification, and stratification. Am J Kidney Dis.
39(2 Suppl 1): S1–S266. 2002.PubMed/NCBI
|
|
17
|
Nüsken KD, Kratzsch J, Wienholz V, Stöhr
W, Rascher W and Dötsch J: Circulating resistin concentrations in
children depend on renal function. Nephrol Dial Transplant.
21:107–112. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ridker PM, Pare G, Parker A, et al: Loci
related to metabolic-syndrome pathways including LEPR, HNF1A, IL6R,
and GCKR associate with plasma C-reactive protein: the Women's
Genome Health Study. Am J Hum Genet. 82:1185–1192. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Takeda A, Toda T, Shinohara S, Mogi Y and
Matsui N: Factors contributing to higher hematocrit levels in
hemodialysis patients not receiving recombinant human
erythropoietin. Am J Kidney Dis. 40:104–109. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Di Iorio B, Cirillo M, Bellizzi V,
Stellato D and De Santo NG: Campania Dialysis Registry Research
Group: Prevalence and correlates of anemia and uncontrolled anemia
in chronic hemodialysis patients - the Campania Dialysis Registry.
Int J Artif Organs. 30:325–333. 2007.PubMed/NCBI
|
|
21
|
Locatelli F, Andrulli S, Memoli B, et al:
Nutritional-inflammation status and resistance to erythropoietin
therapy in haemodialysis patients. Nephrol Dial Transplant.
21:991–998. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kotanko P, Thijssen S and Levin NW:
Association between erythropoietin responsiveness and body
composition in dialysis patients. Blood Purif. 26:82–89. 2008.
View Article : Google Scholar : PubMed/NCBI
|