Introduction
Sporadic Creutzfeldt-Jakob disease (sCJD) is a rare,
transmissible and ultimately fatal prion disease of the brain,
characterized by rapidly progressing dementia. This is often
accompanied by myoclonus, multiple symptoms of neurological
dysfunction and a periodic electroencephalogram pattern (1,2). sCJD is
typically characterized by prominent neurological symptoms,
including myoclonus, visual or cerebellar disturbance,
pyramidal/extrapyramidal dysfunction and akinetic mutism (3), but less commonly with early psychiatric
manifestation. There are a number of reports suggesting that
psychiatric manifestations may occur as a symptom during the
development of sCJD (2,4), but early psychiatric manifestations as
an initial or sole symptom of sCJD are relatively rare. The present
study describes a 67-year-old woman who first presented with
anxiety symptoms but, following initial diagnosis with adjustment
disorder and anxiety, was subsequently diagnosed with probable
sCJD. Diffusion-weighted images (DWIs) supported this diagnosis of
sCJD.
Case report
A 67-year-old woman was admitted to the inpatient
psychiatric service of the Second Affiliated Hospital of Zhejiang
University School of Medicine (Hangzhou, China) with anxiety and
insomnia, which had begun a month prior to admission, and had been
initiated by family issues. The patient was admitted to the
neurology clinic 2 weeks later due to dizziness, but the
neurological examination results and brain magnetic resonance
imaging (MRI) T1-weighted images (T1WIs) and T2-weighted images
(T2WIs) were normal [captured using a Sonata 1.5T MRI scanner
(Siemens AG, Munich, Germany)]. The patient reported that the
symptoms of anxiety subsequently increased, and that she became
increasingly dependent on others, but remained able to perform
normal activities. The patient had experienced similar anxiety
symptoms a year previously, following a bereavement; however, the
patient fully recovered after 1 month of treatment with the
anxiolytic drugs citalopram (20 mg, daily) and lorazepam (0.5 mg,
at bedtime). The patient had no history of alcohol or drug abuse,
memory problems, surgery or any other noteworthy prior medical
history. Furthermore, there was no reported family history of any
neuropsychiatric diseases.
An initial neurological examination revealed a
bilateral mild fluctuating tremor in the hands, which was not
apparent when the patient was relaxed or distracted. Upon
examination of mental status, the patient appeared anxious and
restless, but exhibited no disorientation, hallucinations or
delusions. Psychological testing using the Hamilton Anxiety Rating
Scale (HAM-A) revealed a score of 23, indicative of moderate
anxiety (5). Furthermore, the
patient exhibited no clear cognitive impairment; the patient
recorded a Mini Mental Status Examination (MMSE) score of 26/30 and
a Wechsler Adult Intelligence Scale-Revised by China (WAIS-RC)
score of 90 (6,7). Initial electroencephalogram (EEG;
sourced from Shanghai Nuocheng Electric Appliance Co., Ltd.,
Shanghai, China) analysis demonstrated mildly abnormal brain
activity, with slowed alpha rhythms.
The initial diagnosis was of adjustment disorder and
anxiety, and the patient was prescribed citalopram (20 mg, daily)
and alprazolam (0.4 mg, at bedtime) to relieve anxiety. Upon
assessment 10 days later, the psychiatric symptoms had improved and
the HAM-A score had reduced to 11; however, the patient had become
increasingly forgetful and demonstrated slowed performance in daily
functioning. Cognitive appraisal revealed a deterioration in
cognition, with an MMSE score of 18/30 and a WMS-CR score of 55.
The patient had a staggering gait and occasional choreic movement
of the upper extremities. An EEG revealed moderately abnormal brain
activity, with enhanced theta activity. A lumbar puncture was
performed; an analysis of cerebrospinal fluid (CSF) demonstrated no
marked alterations. However, examination of 14-3-3 protein and tau
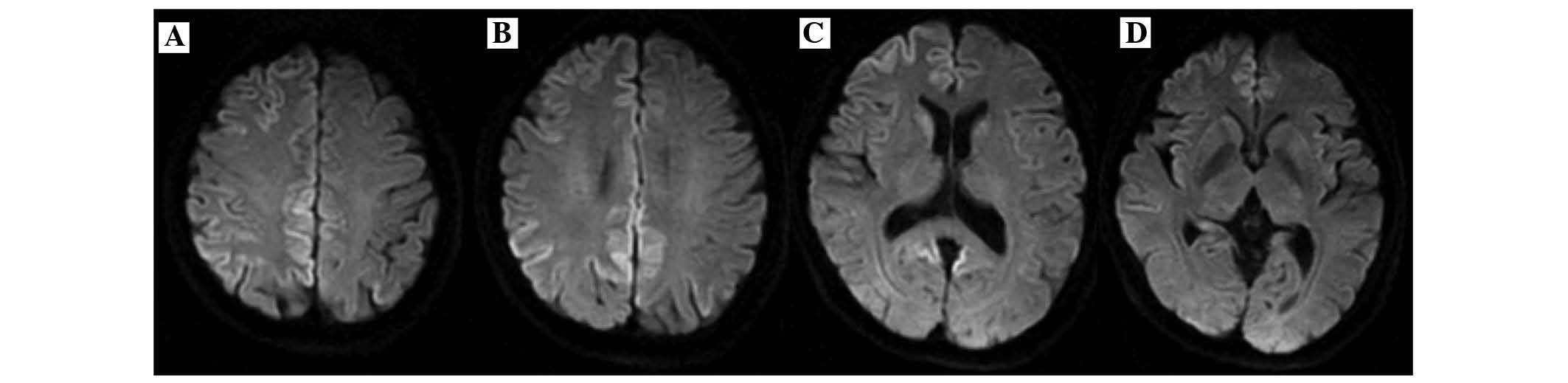
protein was not possible in the current hospital. When examined by
MRI, no abnormality was detected on the brain T1WI and T2WI
sequences, but DWI revealed abnormally high, ribbon-like cortical
signal intensity within numerous brain regions, particularly within
the bilateral cingulate cortex (Fig.
1). Following consultation with a neurologist, the patient was
diagnosed with possible sCJD and transferred as an inpatient to the
neurology department. The patient was monitored and treated with
acyclovir (1,500 mg, daily) and citicoline (500 mg, daily) but
developed increasing confusion, dysphasia, tremors, myoclonus and
ataxia. A neurological examination revealed cogwheel rigidity,
bilaterally increased deep tendon reflexes and positive Babinski
reflexes. A severe deterioration of the patient's cognition was
observed, with an MMSE score of 4/30. Serial EEG demonstrated
periodic sharp-wave complexes. In accordance with the World Health
Organization criteria (3), the
patient was diagnosed with probable sCJD 2 weeks after diagnosis
with possible sCJD. Following this, the patient deteriorated
rapidly, experiencing progressive confusion, ataxia, myoclonus and
frequent convulsions. The patient became bedbound and succumbed to
inhalational bronchopneumonia 5 months after the onset of anxiety.
A postmortem was not performed upon the request of relatives.
Discussion
In the current report, anxiety was presented as the
sole initial symptom of sCJD in an elderly woman with a history of
anxiety disorder, which was misdiagnosed as the primary psychiatric
disorder and delayed the diagnosis of sCJD. The initial
presentation of sCJD is quite variable, and the two most recognized
cardinal features of sCJD are rapidly progressing dementia and
myoclonus (8,9). A previous cohort study of 114 patients
with sCJD revealed that 20% of patients may present with
‘behavioral symptoms’, typically agitation, irritability and
depression (10). However, reports
of early psychiatric manifestations as an initial or sole symptom
of sCJD are relatively rare. Wall et al (2) previously reported upon 2 patients with
sCJD who were concerned regarding their health prior to the
development of severe dementia. Jardri el al (11) reported a sCJD case demonstrating
early depressive disorder with psychotic symptoms, which delayed
the diagnosis of sCJD (11). Based
on the incidence of psychiatric symptoms in the present and
previous reports, it can be concluded that a number of patients may
appear to have psychiatric symptoms prior to diagnosis of sCJD, and
therefore are initially treated for psychiatric illness.
In the present case, the patient expressed anxiety
due to an identifiable stressor during the prodromal phase of sCJD,
and this anxiety persisted during the onset phase and cognitive
deterioration. This anxiety prompted the patient to seek medical
attention, and anxiolytic drugs were effective in its treatment.
These symptoms were initially hypothesized to have psychogenic
origin due to the reported history of anxiety and the absence of
additional neurological symptoms. However, the progressive
deterioration of cognitive and neurological symptoms raised
suspicions of the presence of sCJD. Stressful life events have been
established to be risk factors associated with several neurological
and psychiatric diseases, and it is possible that brain lesions may
act together with stressful events to lead to the manifestation of
these diseases (12). In the present
case, this suggests that increased anxiety, triggered by a
stressful experience, may act together with brain legions to
present as anxiety symptoms in patients with sCJD.
Thorough neurological, cognitive and psychiatric
examinations are important for observation of the clinical features
of sCJD. However, a definitive diagnosis of sCJD is reliant upon
the neuropathological results of a brain biopsy, which presents
substantial risks to the patient; furthermore, there is also an
added risk of false-negative results associated with sampling error
(13). Available tests include EEG
examinations and the detection of 14-3-3 protein in the CSF, but
neither test is specific or able to provide early detection of sCJD
(9,14). As sCJD results from prion
proliferation within the central nervous system, with cortical and
subcortical manifestations, the guidelines from the University of
California, San Francisco have advocated the use of MRI in the
diagnosis of sCJD (15). Use of
brain MRI provides a radiological method of sCJD diagnosis, and
supports amendment of the current clinical diagnostic criteria for
sCJD; use of DWI additionally increases the diagnostic sensitivity
of MRI in the detection of sCJD (16,17).
Bahn and Parchi (18) reported on 4
patients with sCJD demonstrating isolated to diffuse cortical
ribbons using DWI, suggesting that DWI was a more sensitive method
than T2WI for detecting gray matter abnormalities in sCJD
sequences. Yaguchi et al (19) have previously suggested that
standardizing DWI is useful in the early diagnosis of CJD. A
multi-center international study aiming to improve the clinical
diagnostic criteria for sCJD proposed that high signal
abnormalities in the caudate nucleus and putamen or >2 cortical
regions (in the parietal-temporal-occipital regions) using DWI may
support a diagnosis of sCJD, and that the sensitivity of the
criteria for the sCJD spectrum would improve from 92% (WHO
criteria) to 98% (MRI-CJD Consortium) (17). In the current case, compared with the
normal T1WI and T2WI sequences, the hyperintensities detected
within the basal ganglia and cortical regions using DWI temporally
preceded changes revealed using EEG to support the diagnosis of
sCJD.
Evidence from brain imaging indicates that specific
brain structures, such as the amygdaloid complex and the cingulate
and prefrontal cortices, are mediators of the broad range of
behavioral and physiological responses associated with anxiety
(20). The examination of patients
suffering from anxiety using functional MRI has demonstrated
increased activity in the inferior frontal cortex, hippocampus and
throughout the anterior and posterior cingulate cortices, which
provides support for the hypothesis that the limbic circuit is
involved in the pathophysiology of anxiety (21). In the present study, DWI revealed
remarkably restricted diffusion amongst multiple brain regions,
particularly in the bilateral cingulate cortices. As the cingulate
cortex is a section of the limbic lobe involved with generation of
emotions, it is possible that the gray matter abnormality of
bilateral cingulate cortex may be associated with the etiology of
anxiety symptoms.
In conclusion, the present case demonstrates that
sCJD may affect moods in its early stages, and present anxiety as
the first symptom. The importance of secondary causes of anxiety
symptoms in elderly patients should be noted, however, and a global
approach and differential diagnosis are additionally required in
the evaluation of primarily psychiatric syndromes. Brain DWI is a
non-invasive and useful adjuvant examination for the early
diagnosis of sCJD, which may present with initial psychiatric
symptoms.
Acknowledgements
The present study was supported by a grant from
Zhejiang Science and Technology Research Fund in China (grant no.
2012C33119) and Zhejiang Traditional Medical Science Research Fund
in China (grant no. 2010ZB059).
References
|
1
|
Brown P, Gibbs CJ Jr, Rodgers-Johnson P,
Asher DM, Sulima MP, Bacote A, Goldfarb LG and Gajdusek DC: Human
spongiform encephalopathy: The National Institutes of Health series
of 300 cases of experimentally transmitted disease. Ann Neurol.
35:513–529. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wall CA, Rummans TA, Aksamit AJ, Krahn LE
and Pankratz VS: Psychiatric manifestations of Creutzfeldt-Jakob
disease: A 25-year analysis. J Neuropsychiatry Clin Neurosci.
17:489–495. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
World Health Organization (WHO): Global
surveillance, diagnosis and therapy of human Transmissible
Spongiform Encephalopathies: Report of a WHO consultation. Geneva,
Switzerland: 9–11–February;1998.Available from. simpleapps.who.int/iris/bitstream/10665/65516/1/WHO_EMC_ZDI_98.9.pdf
|
|
4
|
Chuang DT, O'Dowd MA, Frieder A, Haut SR
and Robbins MS: Delayed diagnosis of sporadic Creutzfeldt-Jakob
disease in a patient with schizophrenia. Psychosomatics.
53:392–396. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Hamilton M: The assessment of anxiety
states by rating. Br J Med Psychol. 32:50–55. 1959. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rovner BW and Folstein MF: Mini-mental
state exam in clinical practice. Hosp Pract (Off Ed). 22:99–103,
106, 110. 1987.PubMed/NCBI
|
|
7
|
Gong YX: Revision of Wechsler Adult
Intelligence Scale in China. Acta Psychologica Sinica. 15:362–369.
1983.
|
|
8
|
Appleby BS, Appleby KK and Rabins PV: Does
the presentation of Creutzfeldt-Jakob disease vary by age or
presumed etiology?. A meta-analysis of the past 10 years. J
Neuropsychiatry Clin Neurosci. 19:428–435. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Moellentine CK and Rummans TA: The varied
neuropsychiatric presentations of Creutzfeldt-Jakob disease.
Psychosomatics. 40:260–263. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Rabinovici GD, Wang PN, Levin J, Cook L,
Pravdin M, Davis J, DeArmond SJ, Barbaro NM, Martindale J, Miller
BL and Geschwind MD: First symptom in sporadic Creutzfeldt-Jakob
disease. Neurology. 66:286–287. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Jardri R, DiPaola C, Lajugie C, Thomas P
and Goeb JL: Depressive disorder with psychotic symptoms as
psychiatric presentation of sporadic Creutzfeldt-Jakob disease: A
case report. Gen Hosp Psychiatry. 28:452–454. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Esch T, Stefano GB, Fricchione GL and
Benson H: The role of stress in neurodegenerative diseases and
mental disorders. Neuro Endocrinol Lett. 23:199–208.
2002.PubMed/NCBI
|
|
13
|
Tartaro A, Fulgente T, Delli Pizzi C,
Bonomo L, Bocola V and Onofrj M: MRI alterations as an early
finding in Creutzfeld-Jakob disease. Eur J Radiol. 17:155–158.
1993. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Collins SJ, Sanchez-Juan P, Masters CL,
Klug GM, van Duijn C, Poleggi A, Pocchiari M, Almonti S,
Cuadrado-Corrales N, de Pedro-Cuesta J, et al: Determinants of
diagnostic investigation sensitivities across the clinical spectrum
of sporadic Creutzfeldt-Jakob disease. Brain. 129:2278–2287. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Geschwind MD: Rapidly progressive
dementia: Prion diseases and other rapid dementias. Continuum
(Minneap Minn). 16:31–56. 2010.PubMed/NCBI
|
|
16
|
Young GS, Geschwind MD, Fischbein NJ,
Martindale JL, Henry RG, Liu S, Lu Y, Wong S, Liu H, Miller BL and
Dillon WP: Diffusion-weighted and fluid-attenuated inversion
recovery imaging in Creutzfeldt-Jakob disease: High sensitivity and
specificity for diagnosis. AJNR Am J Neuroradiol. 26:1551–1562.
2005.PubMed/NCBI
|
|
17
|
Zerr I, Kallenberg K, Summers DM, Romero
C, Taratuto A, Heinemann U, Breithaupt M, Varges D, Meissner B,
Ladogana A, et al: Updated clinical diagnostic criteria for
sporadic Creutzfeldt-Jakob disease. Brain. 132:2659–2668. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Bahn MM and Parchi P: Abnormal
diffusion-weighted magnetic resonance images in Creutzfeldt-Jakob
disease. Arch Neurol. 56:577–583. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yaguchi M, Yaguchi H and Kanaya T: Early
lesion of Creutzfeldt-Jakob disease detected by standardizing
diffusion-weighted images. Intern Med. 48:1717–1718. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Davidson RJ: Anxiety and affective style:
Role of prefrontal cortex and amygdala. Biol Psychiatry. 51:68–80.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bystritsky A, Pontillo D, Powers M, Sabb
FW, Craske MG and Bookheimer SY: Functional MRI changes during
panic anticipation and imagery exposure. Neuroreport. 12:3953–3957.
2001. View Article : Google Scholar : PubMed/NCBI
|