Introduction
Chronic liver disease comprises a process of
progressive destruction and regeneration of the liver parenchyma
(1). Liver fibrosis is known to
result from chronic liver damage in conjunction with the excessive
accumulation of extracellular matrix proteins, a characteristic of
the majority of chronic liver disease types (2). Chronic infection with hepatitis B virus
(HBV) remains the predominant cause of chronic liver disease and
liver-related morbidity worldwide (3). Asia and the Western Pacific have the
highest proportion of global chronic hepatitis B (CHB) cases, with
75% of all CHB patients concentrated in these countries (4). CHB is considered to be the major risk
factor for cirrhosis, end-stage liver disease and hepatocellular
carcinoma (2,5). In the hepatic tissues of patients with
CHB, the accumulation of extracellular matrix proteins distorts the
hepatic architecture by forming a fibrous scar (6). The subsequent development of nodules of
regenerating hepatocytes eventually leads to liver cirrhosis
(5). Therefore, it is crucial to
achieve an accurate and timely diagnosis of liver fibrosis in order
to prevent its development to liver cirrhosis.
Liver biopsy is a diagnostic procedure, which
involves the examination of a small liver tissue sample for liver
disease, and is considered to be the gold standard for the
diagnosis of liver fibrosis (7).
However, due to its invasiveness and high-cost, the application of
liver biopsy in the evaluation of liver fibrosis is limited. The
liver tissue samples obtained for liver biopsy comprise only
~1/50,000 of the entire liver tissue (8), and therefore may not reflect the
condition of the entire liver. In previous studies, liver biopsies
conducted using tissue samples 15–25 mm in length were consistent
with histopathological examination results in 65–75% of cases
(9,10).
Liver stiffness measurement (LSM) using Fibroscan is
a non-invasive, rapid, quantitative and low-cost transient
elastographic method of assessing the degree of liver fibrosis
(11). Briefly, vibrations of mild
amplitude and low frequency are transmitted by the transducer, and
induce an elastic shear wave that is propagated within the liver.
Pulseecho ultrasonic acquisitions are performed in order to follow
the shear wave and measure its speed, which is directly associated
with the tissue stiffness (the harder the tissue, the faster the
shear propagates). Results are expressed in Kilopascals (Kpa) and
correspond to the median value of ten validated measurements
ranging from 2.5 to 75 Kpa (12).
However, the results of LSM may be influenced by factors other than
fibrosis, including necroinflammatory activity, obesity,
extrahepatic cholestasis and sampling location (13–16). The
efficacy of transient elastography has been validated in patients
with chronic hepatitis C; however, limited data are available for
its use in patients with other forms of liver disease, particularly
patients with CHB and alanine aminotransferase (ALT) <2 times
the upper normal limit. A previous study has suggested that the
diagnostic accuracy of liver fibrosis as measured by Fibroscan may
be influenced by the elevated ALT concentration (17).
Measurement of serum ALT levels is widely used for
the assessment of liver diseases (18). The upper limit of normal ALT is
considered to be a reliable standard to assess liver function
(19). In the present study, the
diagnostic accuracy of Fibroscan for liver fibrosis development in
patients with CHB with ALT levels <2 times the upper normal
limit was investigated.
Materials and methods
Patients
A total of 263 patients (160 males and 103 females;
age range, 16–67 years; average age, 33.48±11.36 years) with CHB
from the Department of Infectious Diseases at the Sichuan Academy
of Medical Sciences & Sichuan Provincial People's Hospital
(Chengdu, China) were enrolled in the present study between October
2010 and August 2013. The inclusion criteria were as follows: i)
Tested positively for the Hepatitis B surface antigen (HBsAg); ii)
ATL levels were sustained <2 times the normal upper limit for 6
months and did not receive drugs for the reduction of ALT levels
(0–80 U/L); iii) received no antiviral therapy; and iv) were
willing to undergo liver biopsy. The exclusion criteria were as
follows: i) Infected with hepatitis A, C or E virus; ii) infected
with the human immunodeficiency virus; iii) suffered from a type of
chronic liver disease other than CHB; iv) total serum bilirubin
level >34.2 µM (normal range, 1.71–17.10 µM); and v) suffered
from liver cirrhosis, as indicated by diagnostic imaging. Prior
written and informed consent was obtained from each patient. The
study was approved by the Ethics Review Board of the Sichuan
Academy of Medical Sciences & Sichuan Provincial People's
Hospital.
LSM assay
LSM assays were conducted according to the
instructions provided by the manufacturer of FibroScan 502 Touch
(Echosens; Paris, France) using an M probe attachment. Briefly,
measurements were performed following an overnight period of
fasting. Mild amplitude and low-frequency vibrations (50 Hz) were
transmitted to the liver of each patient, inducing an elastic shear
wave propagating through the underlying liver tissue. The velocity
of the wave directly correlated to the tissue stiffness. The tip of
the transducer was covered with a drop of gel and placed
perpendicularly in the intercostal space of the patient, who was
required to lie in the dorsal decubitus position with the right arm
on maximal abduction. Scanning was conducted in a region
encompassing the 6th, 7th and 8th intercostal spaces between
anterior axillary and midaxillary lines. The number of successfully
detections per case was required to be ≥10, as LSM may be
considered reliable when 10 valid measurements are obtained, with a
success rate of ≥80% and an interquartile range/median LSM ≤30%
(20–22). The median value, expressed in kPa,
was recorded as representative of the liver stiffness.
Liver biopsy
Liver biopsies were performed percutaneously
following 2–3 ml local anesthetic with 1% lidocaine, and samples
were obtained using a biopsy instrument with a 16 G needle
(BARD® MAGNUM®, Bard Biopsy Systems, Tempe,
AZ, USA). The samples were fixed in formalin and embedded in
paraffin. The embedded tissues were cut into 4-µm sections and
stained with hematoxylin and eosin and Masson's trichrome stains
(both Beisen, Inc., Nanjing, China). Liver fibrosis was
semi-quantitatively evaluated according to the Batts-Ludwig scoring
system (7). The activity grade
referred to the grades of hepatic necroinflammatory activity as
follows: G0, no activity; G1, minimal activity; G2, mild activity;
G3, moderate activity; and G4, severe activity. Liver fibrosis in
liver tissues was graded as follows: S0, no fibrosis, normal
connective tissue; S1, portal fibrosis, fibrous portal expansion);
S2, periportal fibrosis, periportal or rare portal-portal septa;
S3, septal fibrosis, fibrous septa with architectural distortion,
no obvious cirrhosis; and S4, cirrhosis (7).
HBsAg and DNA assay
HBsAg was detected using the HBsAg enzyme-linked
immunosorbent assay (ELISA) kit (Wanti BioPharm, Inc., Beijing,
China), according to the manufacturer's protocol. Serum HBV DNA
levels were measured using Diagnostic kit for Quantification of HBV
DNA (PCR-Fluorescence) (DaAn Gene Co., Ltd., Guangzhou, China) with
a lower limit detection of 1,000 copies/ml, according to the
manufacturer's instructions.
ALT detection assay
Peripheral blood was collected from patients with
CHB with ATL levels <2 times the normal upper limit. ALT was
detected using the enzymatic method as described by Reitman and
Frankel (23), using ALT detection
reagents obtained from Zhongsheng Beikong Reagent, Co., Ltd.
(Beijing, China). ALT levels were measured using the Automatic
Biochemistry analyzer (AU2700; Olympus Corporation, Tokyo,
Japan).
Statistical analysis
All results are expressed as the mean ± standard
deviation. All statistical analyses were performed using the SPSS,
version 18.0 software (SPSS, Inc., Chicago, IL, USA). Receiver
operating characteristic (ROC) analysis was used to determine the
ability of LSM to predict the development of liver fibrosis in
patients with CHB. The area under the curve was a calculated as an
overall assessment of the predictive ability of LSM. Bivariate
Spearman rank correlation coefficient was used to analyze the
correlation between the LSM and histological fibrosis grade.
P<0.05 was considered to indicate statistically significant
difference.
Results
General data of patients with CHB
According to the inclusion and exclusion criteria, a
total of 263 patients (160 males and 103 females) with CHB were
enrolled in the present study. The age range of the patients was
16–67 years, with an average age of 33.48±11.36 years. The general
data of liver enzyme levels of these patients are presented in
Table I. The ALT level range of the
patients was 12–79 U/l, with an average level of 44.07±16.84 U/l.
Among the 263 patients, 120 had ALT levels of ≤40 U/l and 143 had
an ALT level range of 41–80 U/l. The aspartate aminotransferase
(AST) level range was 7–77 U/l, with an average level of
38.57±10.81 U/l. Among the 263 patients, 161 had AST levels of ≤40
U/l and 102 had an AST level range of 41–80 U/l. As shown in
Table II, with regard to the grade
of necroinflammatory activity, 125 cases (47.5%) had mild portal
inflammatory infiltrates (G2). According to the stage of liver
fibrosis, 207 cases (78.7%) had mild liver fibrosis (S1).
 | Table I.Liver enzyme levels in patients with
chronic hepatitis B. |
Table I.
Liver enzyme levels in patients with
chronic hepatitis B.
| Liver enzyme | Range (U/l) | Levels (U/l) | Cases with levels ≤40
U/l (n) | Cases with levels
41–80 U/l (n) |
|---|
| Alanine
aminotransferase | 12–79 | 44.07±16.84 | 120 | 143 |
| Aspartate
aminotransferase | 7–77 | 38.57±10.81 | 161 | 102 |
| Table II.Grade of necroinflammatory activity
and liver fibrosis stage in patients with chronic hepatitis B. |
Table II.
Grade of necroinflammatory activity
and liver fibrosis stage in patients with chronic hepatitis B.
| Necroinflammatory
activity | Liver fibrosis |
|---|
|
|
|---|
| Grade | Cases (%) | Stage | Cases (%) |
|---|
| G0 | 0 (0) | S0 | 17 (6.5) |
| G1 | 79 (30.0) | S1 | 207 (78.7) |
| G2 | 125 (47.5) | S2 | 25 (9.5) |
| G3 | 52 (19.8) | S3 | 11 (4.2) |
| G4 | 7 (2.7) | S4 | 3 (1.1) |
| Total | 263 (100) | Total | 263 (100) |
Correlation analysis between LSM
values and liver fibrosis stage
In order to investigate the association between LSM
values and the stage of liver fibrosis for the diagnosis of liver
fibrosis in patients with CHB and ATL levels <2 times the normal
upper limit, Bivariate Spearman rank correlation analysis was
performed. The LSM values, which were measured by Fibroscan,
positively correlated with the stage of liver fibrosis (r=0.522,
P<0.001), as well as the grade of necroinflammatory activity
(r=0.461, P<0.001). The stage of liver fibrosis positively
correlated with the grade of necroinflammatory activity (r=0.705,
P<0.001). These results indicate that the LSM values positively
correlated with the degree of liver fibrosis and necroinflammatory
activity.
ROC analysis for the prediction of
liver fibrosis development in patients with CHB
In order to determine the diagnostic accuracy of
Fibroscan for the prediction of liver fibrosis development in
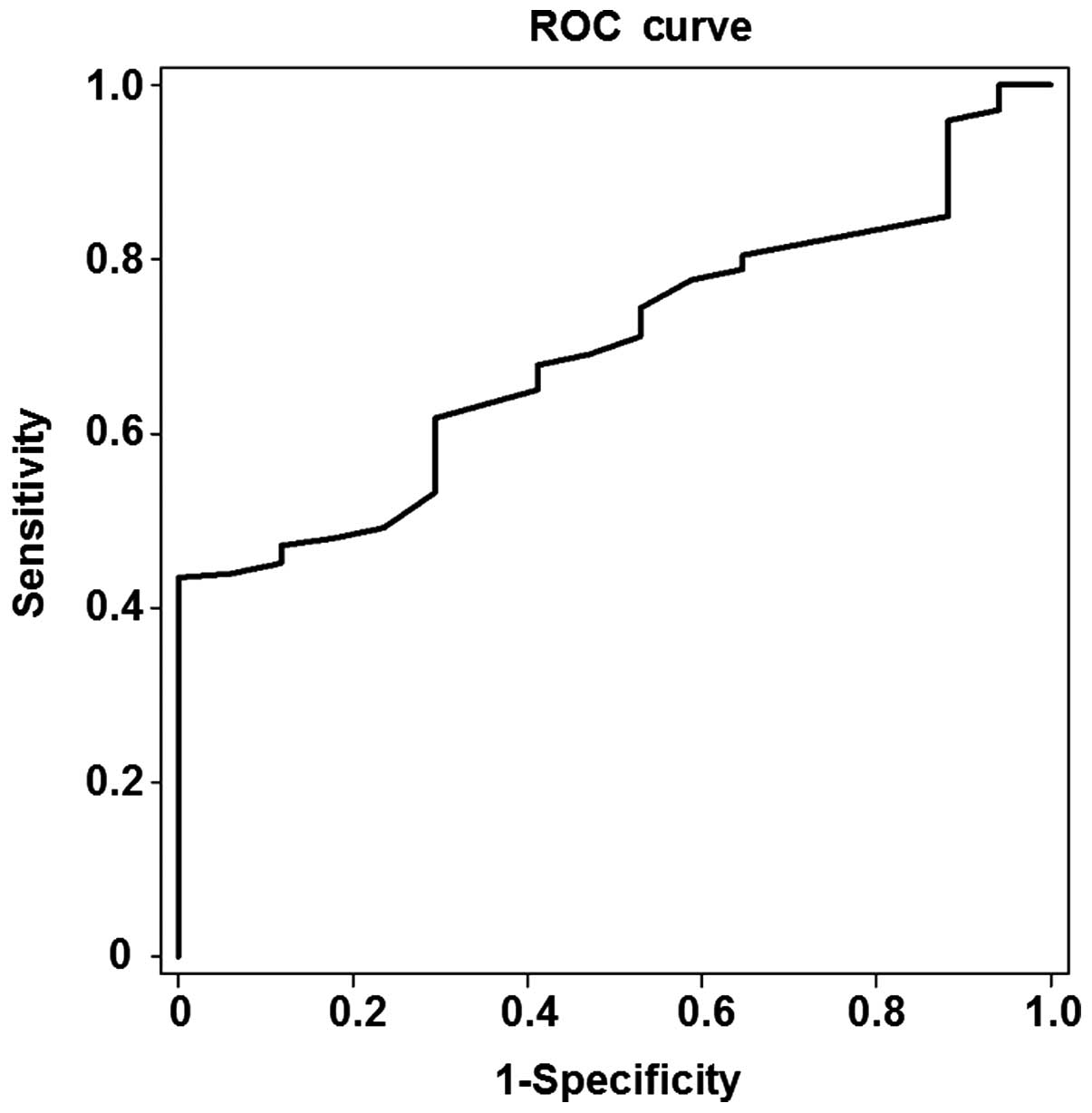
patients with CHB, ROC analysis was performed. Among the 263
patients, 246 were found to have stage S1-S4 liver fibrosis and 17
had stage S0 liver fibrosis. As shown in Fig. 1, the area under the ROC curve for the
prediction of liver fibrosis development was 0.696, and the optimal
cut-off value was 5.55 kPa in the patients with stage S1 liver
fibrosis (P<0.05). The threshold of the optimal cut-off value
had a sensitivity of 61.8% and a specificity of 70.6%.
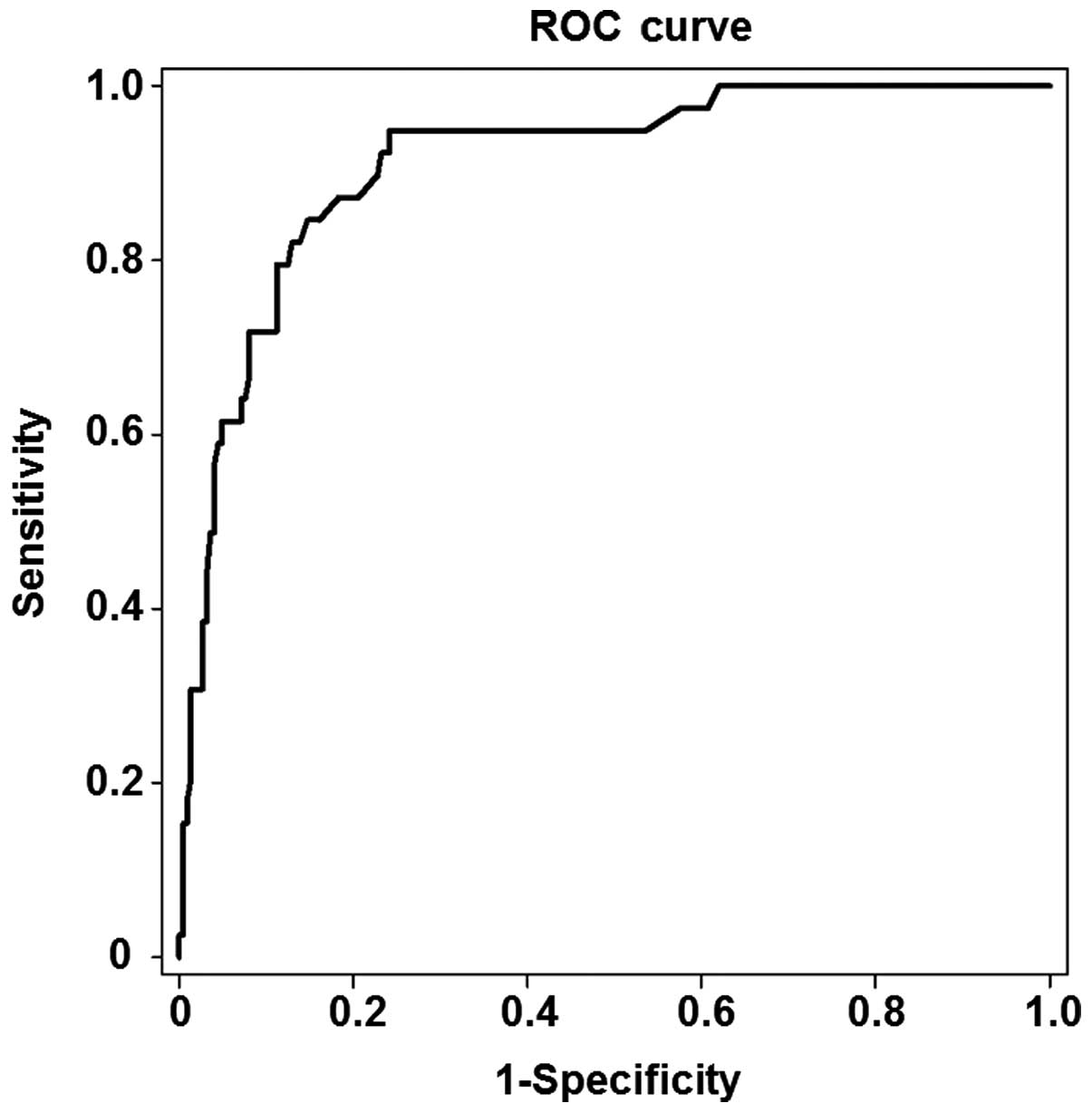
Among the 263 patients, 39 were found to have stage
S2-S4 liver fibrosis and 224 stage S0-S1 liver fibrosis. As shown
in Fig. 2, the area under the ROC
curve for the prediction of liver fibrosis development was 0.911,
and the optimal cut-off value was 8.0 kPa in the patients with
stage S2 liver fibrosis (P<0.05). The threshold of the optimal
cut-off value had a sensitivity of 86.4% and a specificity of
85.3%.
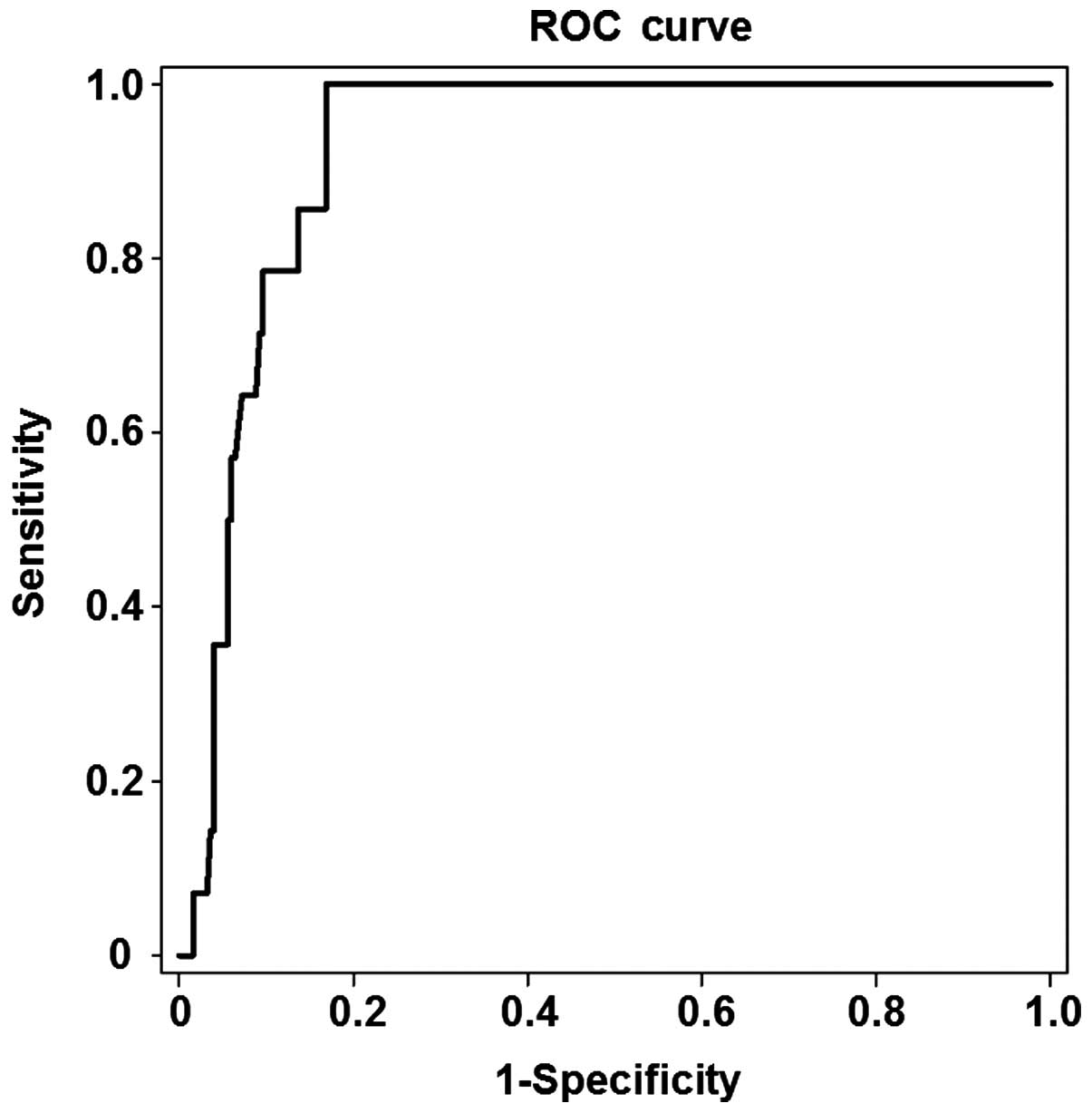
Among the 263 patients, 14 were found to have stage
S3-S4 and 249 stage S0-S2 liver fibrosis. As shown in Fig. 3, the area under the ROC curve for the
prediction of liver fibrosis development was 0.923, and the optimal
cut-off value was 10.95 kPa in the patients with stage S3 liver
fibrosis (P<0.05). The threshold of the optimal cut-off value
had a sensitivity of 78.6% and a specificity of 90.4%. These
results indicated that the stage of liver fibrosis can be
accurately predicted by LSM in patients with CHB with ALT levels
<2 times the normal upper limit. In addition, the specificity of
prediction is increased with the progression of liver fibrosis.
Discussion
Liver fibrosis is known to be primarily caused by
CHB viral infection (24). Timely
and accurate diagnosis of liver fibrosis is essential to the
prevention and treatment for chronic liver disease. Liver biopsy
has been considered to be the most reliable method for diagnosing
liver fibrosis; however, liver biopsy cannot reflect the conditions
of the entire liver, due to the small size of the tissue samples
(25). Although numerous patients
with CHB may be persuaded to undergo a first biopsy, the majority
will be reluctant to accept follow-up biopsies for the evaluation
of disease progression or response to treatment (26). Non-invasive methods of assessing
liver fibrosis in a range of chronic liver diseases are currently
being investigated (27). Principal
among these methods are transient elastography and the use of serum
markers, which have already been evaluated in patients with CHB
(22). The detection capacity of
Fibroscan is ~100-fold greater compared with that of liver biopsy,
despite the fact that the accuracy of Fibroscan may be influenced
by various factors other than fibrosis, including necroinflammatory
activity, obesity, ascites, extrahepatic cholestasis and sampling
location (13–15). Previous studies have shown that the
area under the ROC curve in patients with CHB with significant
fibrosis, advanced fibrosis and cirrhosis were 0.78–0.87, 0.87–0.93
and 0.84–0.96, respectively (28–30). The
diagnosis of liver fibrosis and cirrhosis using LSM based on
transient elastography has been shown to be superior to the
enhanced liver fibrosis test, acoustic radiation force impulse
imaging, Forns fibrosis index, Fibrosis-4 index and enhanced liver
fibrosis algorithm (22,30–32).
In the present study, LSM was performed with
Fibroscan in patients with CHB with ATL levels <2 times the
normal upper limit. The results indicated that the stage of liver
stiffness measured by Fibroscan was positively correlated with the
degree of liver fibrosis and necroinflammatory activity measured by
liver biopsy. The optimal cut-off values in patients with stage S1,
S2 and S3 liver fibrosis were 5.5 kPa, 8.0 kPa, and 10.95 kPa,
respectively. The area under the ROC curve for the prediction of
liver fibrosis development in patients with stage S1, S2 and S3
liver fibrosis was 0.696, 0.911 and 0.923, respectively. In
patients with stage S2 and S3 liver fibrosis, Fibroscan was shown
to have a higher diagnostic accuracy. The optimal cut-off value
exhibited a higher sensitivity and specificity in patients with
stage S1, S2 and S3 liver fibrosis, as did the threshold of the
optimal cut-off value.
In conclusion, Fibroscan examination is a
quantitative analysis technique, which improves the diagnostic
sensitivity of liver fibrosis in patients with CHB with ALT levels
<2 times the normal upper limit.
Acknowledgements
This study was supported by a project of the Sichuan
Provincial Health Department (grant no. 110161).
References
|
1
|
Williams MJ, Clouston AD and Forbes SJ:
Links between hepatic fibrosis, ductular reaction, and progenitor
cell expansion. Gastroenterology. 146:349–356. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Friedman SL: Liver fibrosis-from bench to
bedside. J Hepatol. 38(Suppl 1): S38–S53. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lok AS and McMahon AJ: Chronic hepatitis
B. Hepatology. 45:507–539. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Croagh CM and Lubel JS: Natural history of
chronic hepatitis B: Phases in a complex relationship. World J
Gastroenterol. 20:10395–10404. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ginès P, Cárdenas A, Arroyo V and Rodés J:
Management of cirrhosis and ascites. N Engl J Med. 350:1646–1654.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hernandez-Gea V and Friedman SL:
Pathogenesis of liver fibrosis. Annu Rev Pathol. 6:425–456. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Rockey DC, Caldwell SH, Goodman ZD, Nelson
RC and Smith AD: American Association for the Study of Liver
Diseases: Liver biopsy. Hepatology. 49:1017–1044. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Regev A, Berho M, Jeffers LJ, Milikowski
C, Molina EG, Pyrsopoulos NT, Feng ZZ, Reddy KR and Schiff ER:
Sampling error and intraobserver variation in liver biopsy in
patients with chronic HCV infection. Am J Gastroenterol.
97:2614–2618. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bravo AA, Sheth SG and Chopra S: Liver
biopsy. N Engl J Med. 344:495–500. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bedossa P, Dargère D and Paradis V:
Sampling variability of liver fibrosis in chronic hepatitis C.
Hepatology. 38:1449–1457. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sharma P, Dhawan S, Bansal R, Tyagi P,
Bansal N, Singla V, Kumar A, Matin A and Arora A: The usefulness of
transient elastography by FibroScan for the evaluation of liver
fibrosis. Indian J Gastroenterol. 33:445–451. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Castera L, Forns X and Alberti A:
Non-invasive evaluation of liver fibrosis using transient
elastography. J Hepatol. 48:835–847. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Enomoto M, Morikawa H, Tamori A and Kawada
N: Noninvasive assessment of liver fibrosis in patients with
chronic hepatitis B. World J Gastroenterol. 20:12031–12038. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sporea I, Gilja OH, Bota S, Şirli R and
Popescu A: Liver elastography - an update. Med Ultrason.
15:304–314. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lee S and Kim Do Y: Non-invasive diagnosis
of hepatitis B virus-related cirrhosis. World J Gastroenterol.
20:445–459. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wu T, Li L, Wang H, Luo X and Ning Q:
Transient elastography in hepatitis B virus infection. Liver
stiffness discrepancy due to sampling location. Saudi Med J.
35:554–560. 2014.PubMed/NCBI
|
|
17
|
Bota S, Sporea I, Peck-Radosavljevic M,
Sirli R, Tanaka H, Iijima H, Saito H, Ebinuma H, Lupsor M, Badea R,
et al: The influence of aminotransferase levels on liver stiffness
assessed by acoustic radiation force impulse elastography: A
retrospective multicentre study. Dig Liver Dis. 45:762–768. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Pratt DS and Kaplan MM: Evaluation of
abnormal liver-enzyme results in asymptomatic patients. N Engl J
Med. 342:1266–1271. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Prati D, Taioli E, Zanella A, Della Torre
E, Butelli S, Del Vecchio E, Vianello L, Zanuso F, Mozzi F, Milani
S, et al: Updated definitions of healthy ranges for serum alanine
aminotransferase levels. Ann Intern Med. 137:1–10. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zarski JP, Sturm N, Guechot J, Paris A,
Zafrani ES, Asselah T, Boisson RC, Bosson JL, Guyader D, Renversez
JC, et al: Comparison of nine blood tests and transient
elastography for liver fibrosis in chronic hepatitis C: The ANRS
HCEP-23 study. J Hepatol. 56:55–62. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Degos F, Perez P, Roche B, Mahmoudi A,
Asselineau J, Voitot H and Bedossa P: FIBROSTIC Study Group:
Diagnostic accuracy of FibroScan and comparison to liver fibrosis
biomarkers in chronic viral hepatitis: A multicenter prospective
study (the FIBROSTIC study). J Hepatol. 53:1013–1021. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Trembling PM, Lampertico P, Parkes J,
Tanwar S, Viganò M, Facchetti F, Colombo M and Rosenberg WM:
Performance of enhanced liver fibrosis test and comparison with
transient elastography in the identification of liver fibrosis in
patients with chronic hepatitis B infection. J Viral Hepat.
21:430–438. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Reitman S and Frankel S: A colorimetric
method for the determination of serum glutamic oxalacetic and
glutamic pyruvic transaminases. Am J Clin Pathol. 28:56–63. 1957.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Cohen-Naftaly M and Friedman SL: Current
status of novel antifibrotic therapies in patients with chronic
liver disease. Therap Adv Gastroenterol. 4:391–417. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lefkowitch JH: Liver biopsy assessment in
chronic hepatitis. Arch Med Res. 38:634–643. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Cadranel JF, Rufat P and Degos F:
Practices of liver biopsy in France: Results of a prospective
nationwide survey. For the Group of Epidemiology of the French
Association for the Study of the Liver (AFEF). Hepatology.
32:477–481. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Papastergiou V, Tsochatzis E and Burroughs
AK: Non-invasive assessment of liver fibrosis. Ann Gastroenterol.
25:218–231. 2012.PubMed/NCBI
|
|
28
|
Chen YP, Liang XE, Dai L, Zhang Q, Peng J,
Zhu YF, Wen WQ, Chan HL and Hou JL: Improving transient
elastography performance for detecting hepatitis B cirrhosis. Dig
Liver Dis. 44:61–66. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Chan HL, Wong GL, Choi PC, Chan AW, Chim
AM, Yiu KK, Chan FK, Sung JJ and Wong VW: Alanine
aminotransferase-based algorithms of liver stiffness measurement by
transient elastography (Fibroscan) for liver fibrosis in chronic
hepatitis B. J Viral Hepat. 16:36–44. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Stebbing J, Farouk L, Panos G, Anderson M,
Jiao LR, Mandalia S, Bower M, Gazzard B and Nelson M: A
meta-analysis of transient elastography for the detection of
hepatic fibrosis. J Clin Gastroenterol. 44:214–219. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Liu Y, Dong CF, Yang G, Liu J, Yao S, Li
HY, Yuan J, Li S, Le X, Lin Y, et al: Optimal linear combination of
ARFI, transient elastography and APRI for the assessment of
fibrosis in chronic hepatitis B. Liver Int. 35:816–825. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Lee MH, Cheong JY, Um SH, Seo YS, Kim DJ,
Hwang SG, Yang JM, Han KH and Cho SW: Comparison of surrogate serum
markers and transient elastography (Fibroscan) for assessing
cirrhosis in patients with chronic viral hepatitis. Dig Dis Sci.
55:3552–3560. 2010. View Article : Google Scholar : PubMed/NCBI
|