Introduction
Chronic malignant pain is often managed using opioid
medication. However, opioid-associated adverse effects have also
increased with the widespread usage of opioids. Constipation,
sedation, nausea, vomiting, respiratory depression, and physical
dependence are some of the most well-established side-effects of
opioid treatment.
Previous studies have demonstrated that opioids
alter endocrine function (1,2). Opioid-induced endocrinopathy is a
common consequence of prolonged opioid therapy, yet is infrequently
diagnosed (3). Opioids have been
reported to decrease the levels of gonadal sex hormones, growth
hormones, cortisol and dehydroepiandrosterone sulfate (4,5). Opioids
are known to exert detrimental effects on the endocrine system,
including the hypothalamic-pituitary-adrenal (HPA) axis (6,4). The
mechanisms underlying this interference are unknown, but it has
been hypothesized that opioids inhibit the HPA axis via the
µ-opioid receptor (7). Endogenous
and exogenous opioids also exert an inhibitory effect on
gonadotropin-releasing hormone (3).
The preclinical study conducted by Adams et
al (8) demonstrated that opioids
decrease testosterone secretion. The present study aimed to
investigate the occurrence of endocrine dysfunction in patients
with cancer pain treated with opioids.
Materials and methods
Data collection and study design
The study included 20 patients with
cancer-associated pain. All data were obtained from patients with
malignant tumors who were diagnosed and followed up at the Oncology
Clinic of Akdeniz University Hospital (Antalya, Turkey) between May
2009 and December 2013. The study was designed to be a
retrospective study. Serum samples had been measured to determine
the levels of free testosterone and total testosterone
(predominantly in men), the levels of follicle-stimulating hormone
(FSH), luteinizing hormone (LH), and estradiol (predominantly in
women), as well as the levels of growth hormone (GH), serum free
thyroxine (fT4), thyroid-stimulating hormone (TSH), prolactin,
adrenocorticotropic hormone (ACTH) and serum cortisol. The blood
samples were taken at 8:00 a.m. Patients with a history of cranial
radiation, cranial surgery, pituitary tumors, adrenal metastasis,
brain metastasis, anxiety, major depressive disorder, alcoholism,
acute or chronic infection, cachexia, obesity, uncontrolled pain
management or hormone replacement therapy were excluded from the
present study, due to the fact that these conditions may affect the
HPA axis or endocrine system. In addition, patients that were
receiving medication that may interfere with pituitary function or
the endocrine system, such as megestrol acetate, continuous steroid
usage for three weeks, tamoxifen, anastrozole, metoclopramide or
psychiatric drugs were not included in the study. The inclusion
criteria were chronic cancer-associated pain, and daily treatment
with a morphine equivalent daily dose (MEDD) ≥25 mg/dl for ≥1
month. None of the patients in the current study were >80 years
old.
Pain was measured using the visual analog score
(VAS). All patients had a VAS of <2, which indicated mild to no
pain. Obesity was classified according to body mass index (BMI).
Patients with a BMI of >30 were not included in the study. In
addition, patients with an Eastern Cooperative Oncology Group score
of >2 were also not included in the study. The levels of
procalcitonin and C-reactive peptide were used to exclude patients
with infections. Daily opioid use was recorded, and MEDD was
calculated using the equianalgesic conversion table listed in the
study conducted by Cepeda et al (9).
Statistical analysis
The data were presented as means ± standard
deviations for normally distributed variables. The variables were
investigated using visual (histograms and probability plots) and
analytical methods (Kolmogorov-Simirnov and Shapiro-Wilk's tests),
in order to determine whether the data were normally distributed
(including MEDD scores, and levels of ACTH, cortisol, prolactin,
TSH, fT4, FSH, LH, testosterone and free testosterone). Independent
predictors were examined using logistic regression analysis.
Statistical analyses were performed using SPSS software, version
20.0 (IBM SPSS, Armonk, NY, USA). P<0.05 was considered to
indicate a statistically significant result.
Results
The present study evaluated the data of 20 patients
with cancer who were diagnosed and followed-up at the Akdeniz
University Hospital between May 2009 and December 2013. All
patients received opioid treatment for ≥1 month for pain
management.
The median follow-up period was 9.4 months. The
median age of the patients was 50 years (range, 24–72 years). Of
the patients, 65% were male and 35% were female. A total of 15
patients (75%) had metastatic cancer. The demographic data of the
patients are summarized in Table
I.
 | Table I.Characteristics of the patients
(n=20). |
Table I.
Characteristics of the patients
(n=20).
| Characteristic | Value |
|---|
| Gender, n (%) |
|
|
Female | 7
(35) |
| Male | 13 (65) |
| Age, years |
|
|
Median | 50 |
|
Range | 24–72 |
| Metastases location,
n (%) |
|
| None | 5
(25) |
|
Visceral | 10 (50) |
| Bone | 3
(15) |
| Bone and
visceral | 2
(10) |
| ECOG score, n
(%) |
|
| 0 | 10 (50) |
| 1 | 8
(40) |
| 2 | 2
(10) |
Serum TSH levels (normal range, 0.2–4.2 µIU/ml) were
>4.2 µIU/ml in 20% of the patients, and <0.2 µIU/ml in 5% of
the patients (Table II). Serum fT4
levels (normal range, 0.9–1.7 pg/ml) were <0.9 pg/ml in 5.2% of
patients, and none of the patients exhibited serum fT4 levels
higher than the upper limit of the normal range (>1.7 pg/ml;
Table II). Serum cortisol
concentrations (normal range, 4.3–22.4 µg/dl) were lower than the
normal range in 15% of patients and higher than the normal range in
40% of patients (Table II). Serum
total testosterone levels (male normal range, 1.9–5.4 ng/ml; female
normal range, 0.06–0.8 ng/ml) were lower than the normal range in
68.7% of patients, and serum free testosterone levels (male normal
range, 4.9–21.6 pg/ml; female normal range, 0–2.6 pg/ml) were lower
than the normal range in 57.1% of patients (Table II). Serum FSH levels (male normal
range, 1.5–12.4 mIU/ml; female normal range, 3.5–12.5 mIU/ml) were
lower than the normal range in 30% of patients, and higher in 45%
of patients. Serum LH levels (male normal range, 1.7–8.6 mIU/ml;
female, 2.4–12.6 mIU/ml) were lower than the normal range in 30% of
patients and higher in 40% of patients. Serum GH concentrations
were within the normal range (0–8 ng/ml) in 94.8% of patients.
Serum prolactin concentrations (normal range, 4.1–18.4 ng/ml) were
above normal values in 42.9% of patients, but none of the patients
had concentrations below the normal range (Table II). Serum ACTH concentrations
(normal range, 0–65 pg/ml) were within the normal range in 94.5% of
patients (Table II). Lastly serum
estradiol levels (normal range, 24–195 pg/ml) were lower in 25% of
patients and higher in 12.5% of patients (Table II).
| Table II.Hormonal status of the patients. |
Table II.
Hormonal status of the patients.
|
|
| Hormone levels of
patients, n (%) |
|---|
|
|
|
|
|---|
| Hormone | Normal range | Lower | Normal | Higher |
|---|
| TSH (n=20),
µIU/ml | 0.2–4.2 | 1 (5) | 15 (75) | 4 (20) |
| fT4 (n=19),
pg/ml | 0.9–1.7 | 1 (5.2) | 18 (94.8) | 0 (0) |
| ACTH (n=18),
pg/ml | 0–65 | 1 (5.5) | 17 (94.5) | 0 (0) |
| Cortisol (n=20),
µg/dl | 4.3–22.4 | 3 (15) | 9 (45) | 8 (40) |
| FSH (n=20),
mIU/ml | Female: 3.5–12.5 | 6 (30) | 5 (25) | 9 (45) |
|
| Male: 1.5–12.4 |
|
|
|
| LH (n=20),
mIU/ml | Female: 2.4–12.6 | 6 (30) | 6 (30) | 8 (40) |
|
| Male: 1.7–8.6 |
|
|
|
| Total testosterone
(n=16), ng/ml | Male: 1.9–5.4 | 11 (68.7) | 5 (31.3) | 0 (0) |
|
| Female: 0.06–0.8 |
|
|
|
| Free testosterone
(n=14), pg/ml | Male: 4.9–21.6 | 8 (57.1) | 6 (42.9) | 0 (0) |
|
| Female: 0–2.6 |
|
|
|
| GH (n=19), ng/ml | 0–8 | 0 (0) | 18 (94.8) | 1 (5.2) |
| Estradiol (n=8),
pg/ml | Female: 24–195 | 2 (25) | 5 (62.5) | 1 (12.5) |
|
|
Male:
13.5–59.5 |
|
|
|
| Prolactin (n=14,
ng/ml | 4.1–18.4 | 0 (0) | 8 (57.1) | 6 (42.9) |
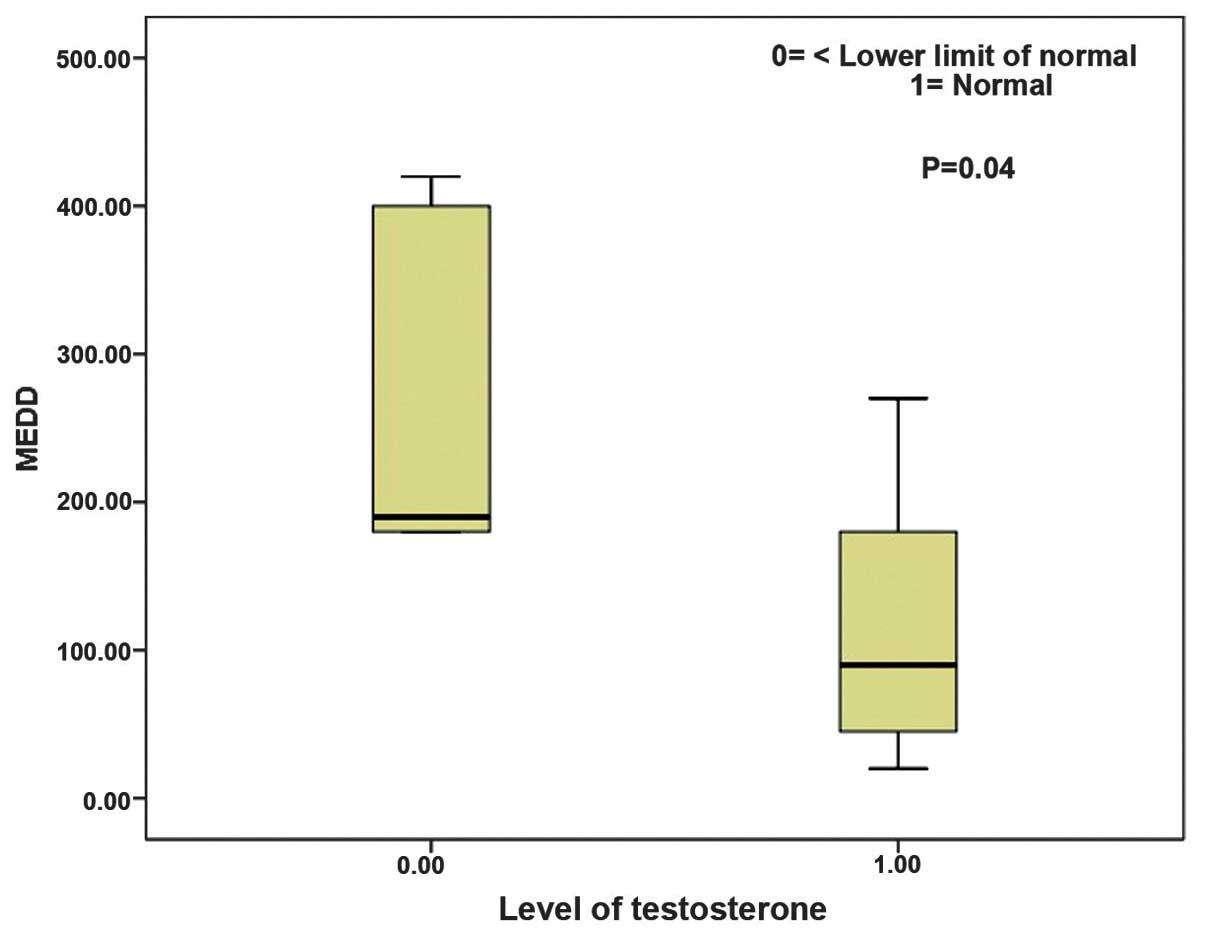
The median MEDD of the patients was 180 (range,
10–420). Independent predictors of the MEDD were evaluated using
logistic regression analysis, but no significant association was
found between MEDD and gender, or the levels of ACTH, cortisol,
prolactin, TSH, fT4, FSH or LH. However, the levels of testosterone
(P=0.040) and the levels of free testosterone (P=0.041) were
significantly affected by MEDD (Fig.
1). These results indicate that as the MEDD increases the
testosterone and free testosterone levels decrease (Fig. 1). Conversely, prolactin levels were
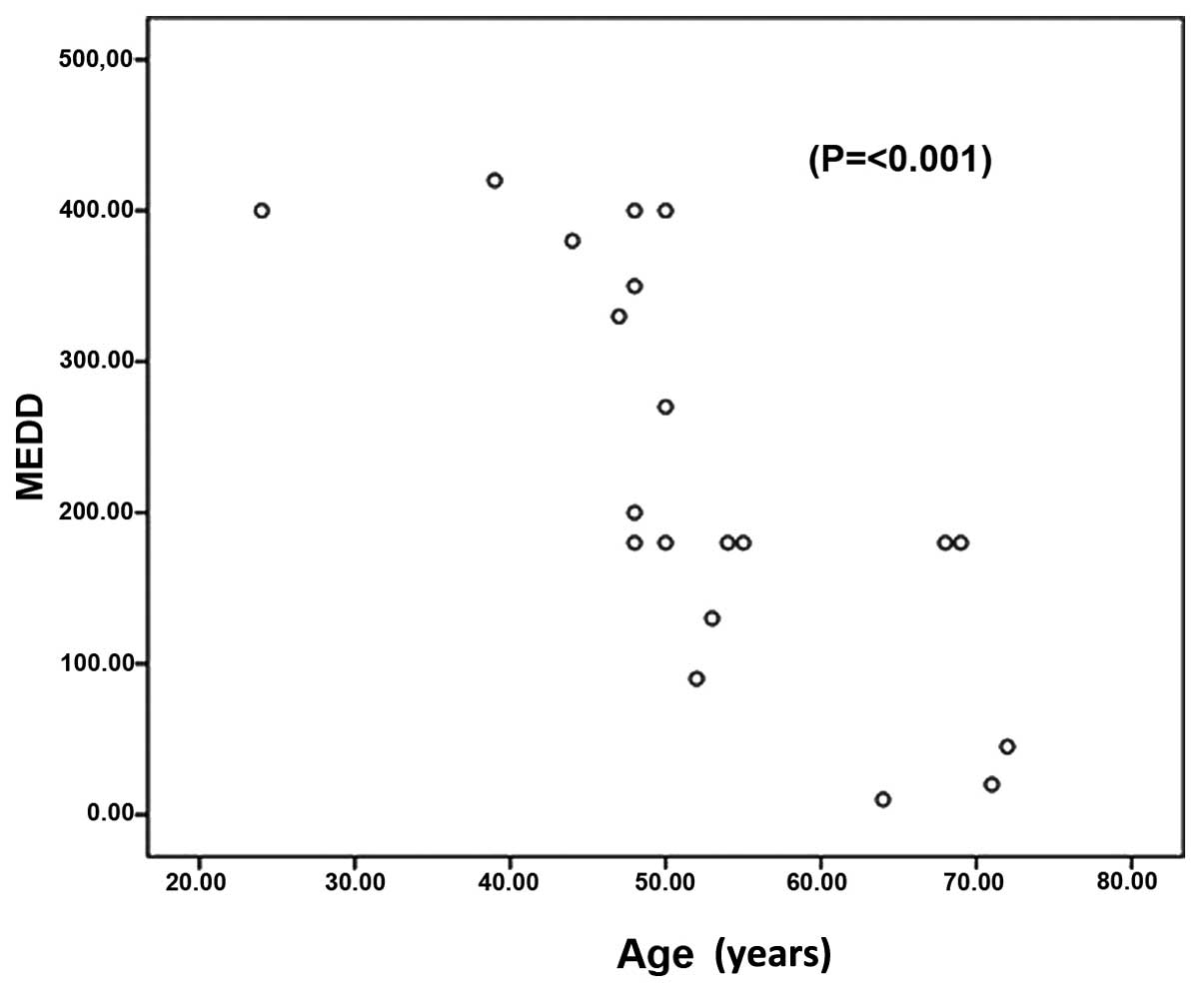
determined to increase as the MEDD increases (P=0.083). Lastly,
MEDD was found to be significantly affected by age (P≤0.001),
indicating that the required dose of opioid analgesic is affected
by age (Fig. 2).
Discussion
Opioids induce a wide spectrum of endocrinopathies,
and hypogonadism is the most well-documented endocrinopathic
adverse effect of opioid usage (1,2).
Although the effects of opioids on LH and sex hormone release have
yet to be fully understood, opioids may alter the sex
hormone-hypothalamic feedback process (3). Opioids may also interfere with the
pituitary release of LH and FSH (3).
Lastly, opioids may have direct negative effects on the testes,
resulting in decreased testosterone secretion and decreased
testicular interstitial fluid (8).
The results of the present study demonstrated that opioid therapy
in patients with cancer may inhibit gonadal function and cause
hyperprolactinemia. It has previously been reported that
testosterone levels decrease as the MEDD increases (2,8), and the
results of the present study are concordant with this. No
statistically significant correlation was identified between opioid
dosage and TSH, GH, FSH or LH levels. However, prolactin hormone
levels increased with MEDD.
Opioid-induced suppression of the HPA axis is not a
common differential diagnosis and may be misdiagnosed in clinical
settings. The exact mechanism underlying the association of opioids
with hypocortisolism is unknown. There are rare case reports of
adrenal insufficiency secondary to chronic opioid usage (10,11).
Weakness and fatigue are symptoms frequently observed in patients
with cancer. These symptoms may be attributed to the underlying
malign disease, but may also be associated with adrenocortical
insufficiency in the case of chronic high-dose opioid usage. The
results of the present study demonstrated markedly low ACTH and
cortisol levels in patients with cancer-associated pain, although
the association between opioid chronic usage and low ACTH and
cortisol levels was not found to be statistically significant.
The results also showed that opioid analgesic
requirement increases with age. Further studies are required in
order to clarify the mechanisms underlying these effects.
The signs and symptoms of hypogonadism range from
loss of libido and depression to fatigue and osteoporosis. These
symptoms can also be seen in patients with chronic cancer but
without any hypogonadism.
In conclusion, it is recommended that patients with
cancer should be screened for sex hormone deficiency prior to the
initiation of opioid treatment, and should be followed-up regularly
for hypogonadism during opioid treatment. In addition, further
studies are required in order to further clarify the association
between hypocortisolism, decreased GH and TSH levels, and opioid
usage.
Acknowledgements
The abstract was presented at the 39th ESMO Congress
Sep 26–30, 2014 in Madrid, Spain and published as abstract no.
1525P in Ann Oncol 25 (Suppl 4): 2014.
References
|
1
|
Dev R, Hui D, Dalal S, Nooruddin ZI,
Yennurajalingam S, Del Fabbro E and Bruera E: Association between
serum cortisol and testestorone levels, opioid therapy and symptom
distress in patients with advanced cancer. J Pain Symptom Manage.
41:788–795. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rajagopal A, Vassilopoulou-Sellin R,
Palmer JL, Kaur G and Bruera E: Symptomatic hypogonadism in male
survivors of cancer with chronic exposure to opioids. Cancer.
100:851–858. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Colameco S and Coren JS: Opioid-induced
endocrinopathy. J Am Osteopath Assoc. 109:20–25. 2009.PubMed/NCBI
|
|
4
|
Abs R, Verhelst J, Maeyaert J, Van Buyten
JP, Opsomer F, Adriaensen H, Verlooy J, Van Havenbergh T, Smet M
and Van Acker K: Endocrine consequences of long-term intratecal
administration of opioids. J Clin Endocrinol Metab. 85:2215–2222.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lee C, Ludwig S and Duerksen DR: Low-serum
cortisol associated with opioid use: Case report and review of the
literature. Endocrinologist. 12:5–8. 2002. View Article : Google Scholar
|
|
6
|
Vuong C, Van Uum SH, O'Dell LE, Lutfy K
and Friedman TC: The effects of opioids and opioid analogs on
animal and human endocrine systems. Endocr Rev. 31:98–132. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ducat E, Ray B, Bart G, Umemura Y, Varon
J, Ho A and Kreek MJ: Mu-opioid receptor A118G polymorphism in
healthy volunteers affects hypothalamic-pituitary-adrenal axis
adrenocorticotropic hormone stress response to metyrapone. Addict
Biol. 18:325–331. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Adams ML, Sewing B, Forman JB, Meyer ER
and Cicero TJ: Opioid-induced suppression of rat testicular
function. J Pharmacol Exp Ther. 266:323–328. 1993.PubMed/NCBI
|
|
9
|
Cepeda MS, Etropolski M, Weinstein R, Fife
D, Boston R and Matcho A: Dose patterns in commercially insured
subjects chronically exposed to opioids: A large cohort study in
the United States. BMC Palliat Care. 9:142010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Oltmanns KM, Fehm HL and Peters A: Chronic
fentanyl application induces adrenocortical insufficiency. J Intern
Med. 257:478–480. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Schimke KE, Greminger P and Brändle M:
Secondary adrenal insufficiency due to opiate therapy - another
differential diagnosis worth consideration. Exp Clin Endocrinol
Diabetes. 117:649–651. 2009. View Article : Google Scholar : PubMed/NCBI
|