Introduction
Primary pulmonary synovial sarcoma is a rare lesion
that occurs in 0.5% cases of lung malignancies (1). It is a highly aggressive malignant
neoplasm that may arise from the lung parenchyma, bronchial tree or
pulmonary arteries (1). It is more
common in males and, unlike other malignancies, it has not been
associated with cigarette smoking (1). The diagnosis of primary pulmonary
synovial sarcoma requires clinical, radiological, pathological and
immunohistochemical investigations to exclude alternative primary
tumors and metastatic sarcoma (2).
Immunohistochemistry and cytogenetic studies have reported an
increasing incidence of primary synovial sarcomas among pulmonary
synovial sarcomas (1–3).
Primary pulmonary synovial sarcoma has no diagnostic
radiological features and the differential diagnosis of this tumor
is very difficult. Chest computed tomography (CT) reveals a
heterogeneously enhancing mass in the lobe or hilum of the lung,
frequently calcified and with pleural invasion (4–6).
However, involvement of the mediastinum, particularly presenting
with a large lump mass in the mediastinum as the sole initial
imaging manifestation, in the course of primary pulmonary synovial
sarcoma is extremely rare, which may contribute to a delayed
diagnosis or misdiagnosis. To the best of our knowledge, there are
no prior reports describing a primary pulmonary synovial sarcoma
presenting with a large lump mass in the mediastinum as the sole
initial imaging manifestation in the English-language literature.
The present study describes a case finally diagnosed as primary
pulmonary synovial sarcoma, which initially manifested as a large
lump mass in the mediastinum.
Case report
The present study was conducted in accordance with
the Declaration of Helsinki and approved by the Ethics Committee of
Taizhou People's Hospital (Jiangsu, China). Written informed
consent was obtained from the patient. A 59-year-old patient was
admitted to the Department of Respiratory Medicine of Taizhou
People's Hospital in March 2014 complaining of a persistent cough
and blood sputum for 2 weeks. The patient had no prior history of
lung disease, but had a 30-year history of tobacco use, smoking one
pack of cigarettes per day for 25 years. Following admission,
physical examinations revealed a body weight of 65 kg, body height
of 173 cm, body temperature of 37°C, pulse of 86 bpm, respiratory
rate of 18 bpm and blood pressure of 110/72 mmHg. The patient had
yellow skin and bloodshot eyes, but no cyanosis of the lips. No
enlargement of superficial lymph nodes of the neck and no
abnormality was detected in the cardiopulmonary physical
examination.
At the initial examination, laboratory results were
as follows: Red blood cells, 3.98×1012/l
(4–5.5×1012/l); hemoglobin, 118 g/l (120–160 g/l); white
blood cells, 4.57×109/l (4–10×109/l);
platelets, 121×109/l (100–300×109/l); and
erythrocyte sedimentation rate, 23 mm/h (0–15 mm/h). Biochemical
examination revealed the following results: Total serum protein,
61.6 g/l (66–87 g/l); albumin, 29.6 g/l (35–54 g/l); globulin, 32
g/l (20–40 g/l); C-reactive protein, 17 mg/l (0–5.0 mg/l); serums
carcinoembryonic antigen, 5.12 ng/ml (0–6.5 ng/ml); neuron-specific
enolase, 9.45 ng/ml (0–20.0 ng/ml); and CYFRA 21-1, 1.21 ng/ml
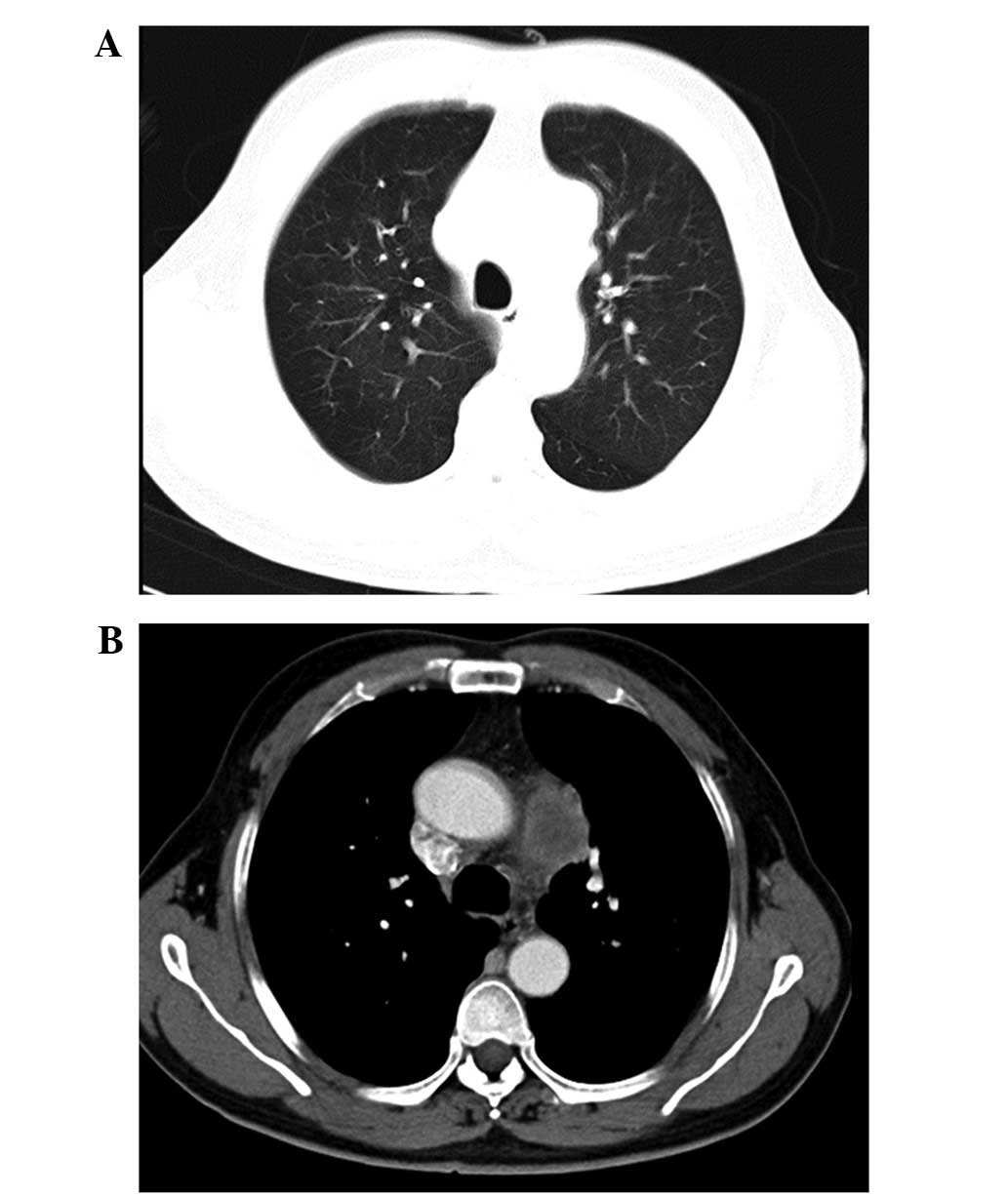
(0.1–3.3 ng/ml). Chest CT revealed a large lump mass in left upper
mediastinum (Fig. 1A and B).
Thoracoscopy was performed and revealed that the left pulmonary
artery was engulfed by the lump mass. As a result, the surgical
resection of the tumor was abandoned. The patient was confirmed
with a diagnosis of primary pulmonary synovial sarcoma following
the histopathological and immunohistochemical analysis of biopsy
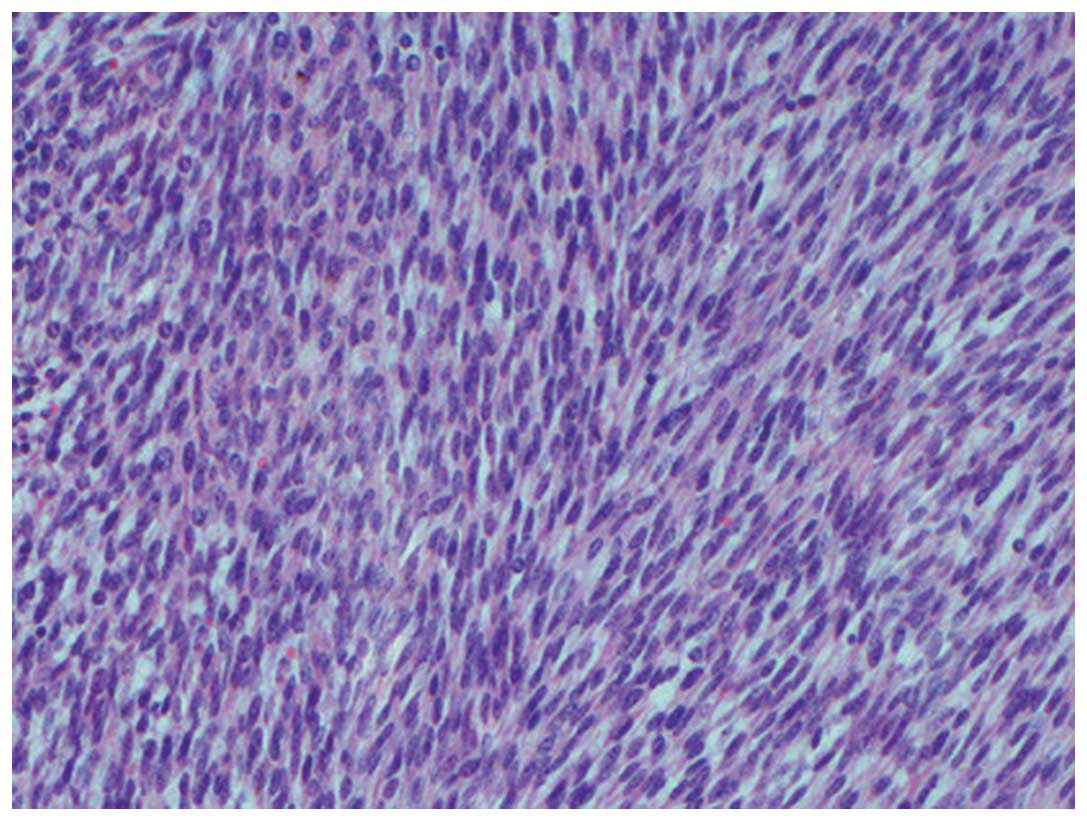
specimens via thoracoscopy. Histologically, the lesion was composed
of bundles of spindle-shaped cells, with areas of necrosis,
sclerosis and hyalinosis (Fig. 2).
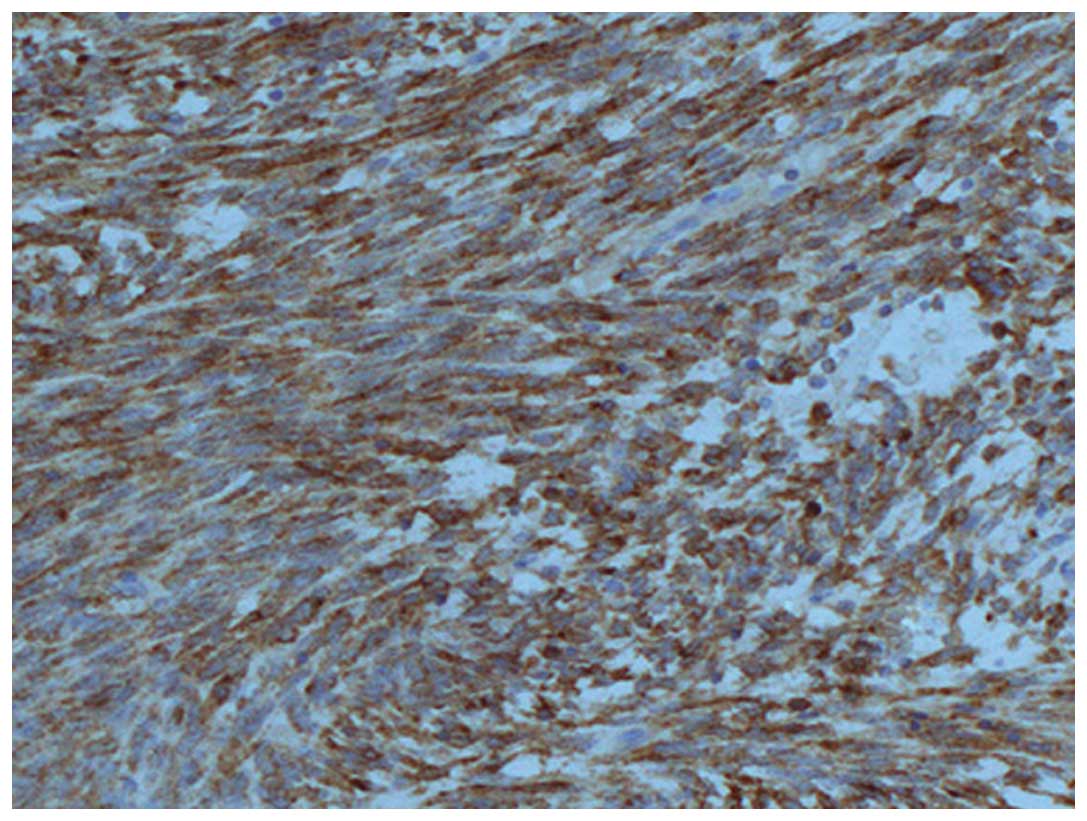
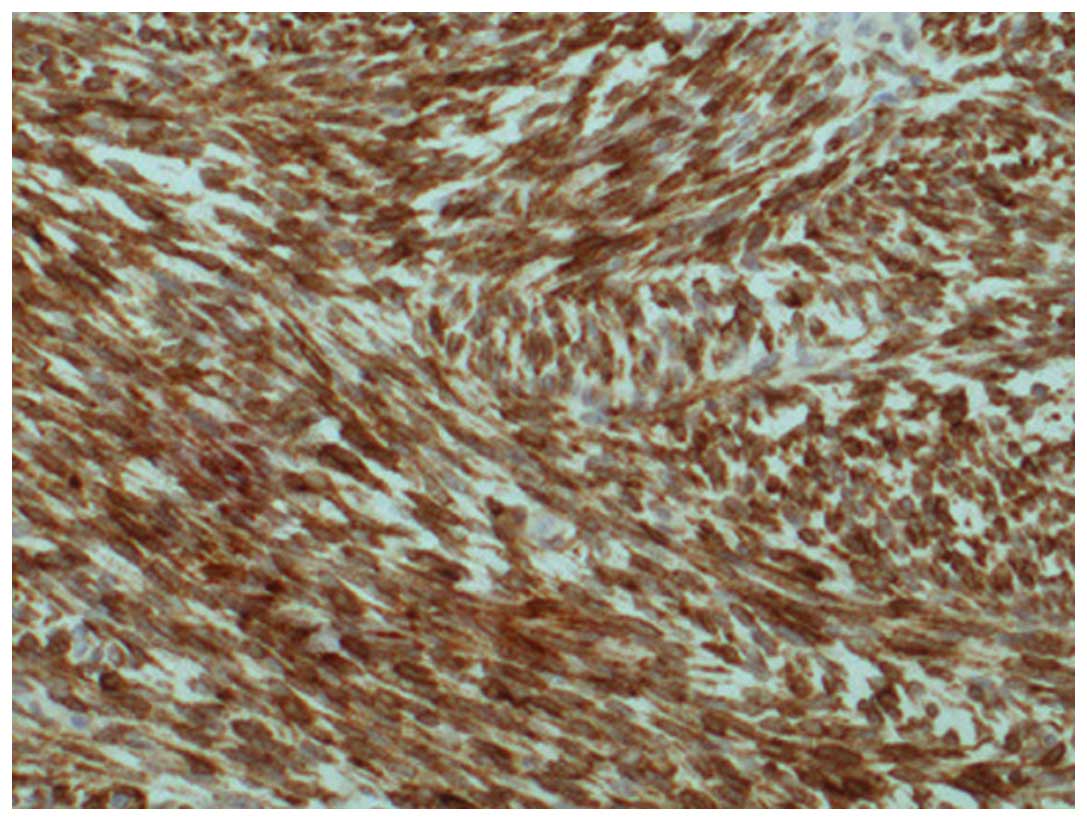
Immunohistochemically, the tumor cells were positive for epithelial
membrane antigen (EMA), CD99, B-cell lymphoma 2 (bcl-2) and
vimentin (Figs. 3 and 4), but negative for S-100, SyN, Myo-D1 and
CD20. Based on all of these findings, primary pulmonary synovial
sarcoma was definitely diagnosed.
Following confirmation, the patient was transferred
to the Department of Oncology for chemotherapy treatments with
ifosfamide (2.5 g/m2 i.v., day 1–3) and doxorubicin (25
mg/m2 i.v., day 1–3), which were planned to be repeated
every 21 days. Unfortunately, no partial regression was achieved
after two rounds of chemotherapy, and the patient was lost to
follow-up 3 months after diagnosis.
Discussion
Primary pulmonary synovial sarcoma is rare,
constituting <0.5% of all pulmonary malignancies (7) and ~10% of all primary pulmonary
sarcomas (8). Primary pulmonary
synovial sarcomas may arise from the parenchyma, tracheobronchial
tree or pulmonary artery, and are designated as mesenchymal tumors
in the World Health Organization classification (9).
Clinical symptoms of primary pulmonary synovial
sarcoma may be associated with the histological type, region, size
and degree of differentiation of the tumor (10). Patients suffering from primary
pulmonary synovial sarcomas may have no overt symptoms during the
initial stages; however, as the disease progresses, they are likely
to present with a cough, chest pain caused by the tumor, hemoptysis
from erosion of the airways and dyspnea caused by obstructive
pneumonia (4).
Radiographic and subsequent CT imaging of the chest
are typically conducted as primary investigative measures in the
diagnosis of primary pulmonary synovial sarcoma. A chest CT scan
showed that the majority of the masses were well-defined and
measured >5 cm, displaying heterogeneous enhancement using
intravenous contrast materials. Tumors of this type are often
calcified and exhibit invasion of the pleura, resulting in pleural
effusion (4,11). To the best of our knowledge,
involvement of the mediastinum, particularly presenting with a
large lump mass in the mediastinum as the sole initial imaging
manifestation, in the course of primary pulmonary synovial sarcoma
is extremely rare, which may have been a factor in the delayed
diagnosis or misdiagnosis. We speculate a number of possible
causes: i) The tumor in the present case may have originated in the
left pulmonary artery and grew to the left upper mediastinum; or
ii) the characteristics of expansive growth, well-defined with
coated or fake capsule formation of the tumor resulted in clear
delineation between the tumor and the lung.
Diagnosis of primary pulmonary synovial sarcoma was
based on pathological and immunohistochemical analyses, as well as
physical and radiological examinations to exclude alternative
primary tumors and metastatic sarcoma. Primary pulmonary synovial
sarcomas are of four subtypes: Monophasic fibrous (spindle),
monophasic epithelial, biphasic and poorly differentiated, among
which the former two are most common (12). Immunohistochemical examination may be
useful in differentiating synovial cell sarcomas from other
sarcomas. In recent studies, synovial cell sarcomas were shown to
be almost uniformly positive for vimentin and bcl-2, as well as
positive for EMA in 55–91% of cases, cytokeratin in 70%, and CD99
in 90% (13,14). In the present case study,
histological results revealed that the neoplastic cells were of
moderate size with obvious nucleoli and thick cell membranes, as
well as with varying arrangements of epithelial cells and spindle
cells. The following immunohistochemical analysis revealed that the
tumor cells were positive for EMA, bcl-2, CD99 and vimentin, but
negative for S-100, SyN, Myo-D1 and CD20. On the basis of these
results, primary pulmonary synovial sarcoma was diagnosed.
Cytogenetic testing may be performed when diagnosis is unclear,
which is a new diagnostic method for synovial sarcoma (15). The t (X;18) (p11.2;q11.2)
translocation, commonly identified in synovial sarcoma, results
from the fusion of the SYT gene on chromosome 18 to either
of two closely related genes, SSX1 and SSX2, on
chromosome X.
To the best of our knowledge, complete surgical
resection is preferred therapy for patients with primary pulmonary
synovial sarcoma. Recent studies reveal that patients able to
undergo complete surgical resection have significantly improved
survival compared with patients with positive surgical margins or
unresectable tumors (16–18). Radiotherapy has no apparent effect on
the control of local disease or overall survival. Chemotherapy
reported in unresectable primary pulmonary synovial cell sarcoma is
very rare and often administered in palliative cases where surgical
resection is not possible (6).
Spillane et al (19) reported
that synovial sarcoma is chemosensitive to ifosfamide and
doxorubicin, with an overall response rate of ~24%. The study
formed the rationale for offering chemotherapy to patients with
pulmonary synovial sarcomas. In response to the left pulmonary
artery was wrapped by the tumor, the patient in the present case
study was referred for palliative chemotherapy using ifosfamide and
doxorubicin. Unfortunately, no partial regression was achieved
after two rounds of chemotherapy and the patient was lost to
follow-up 3 months after diagnosis.
In conclusion, primary pulmonary synovial sarcoma
presenting with a large lump mass in the mediastinum as the sole
initial imaging manifestation is extremely rare, which may have
been a factor in the delayed diagnosis or misdiagnosis. In this
situation, the raised awareness of diagnosis and knowledge
concerning the clinical presentation of primary pulmonary synovial
sarcoma are key factors in ensuring an immediate diagnosis and
adequate intervention.
References
|
1
|
Devleena Bansal V, Chaudhuri T and Roy S:
Primary synovial sarcoma of lung. Lung India. 31:277–279. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kim GH, Kim MY, Koo HJ, Song JS and Choi
CM: Primary Pulmonary Synovial Sarcoma in a Tertiary Referral
Center: Clinical Characteristics, CT, and 18F-FDG PET Findings,
With Pathologic Correlations. Medicine (Baltimore). 94:e13922015.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Teng XD and Kong M: Primary pulmonary soft
tissue sarcoma. Zhonghua Bing Li Xue Za Zhi. 41:204–208. 2012.(In
Chinese). PubMed/NCBI
|
|
4
|
Jiang J, Zhou J and Ding W: Primary
pulmonary synovial sarcoma, a rare primary lung neoplasm: Two case
reports and review of the current literature. Respirology.
13:748–750. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Cabuk D, Ustuner B, Akgul AG, Acikgoz O,
Yaprak B, Uygun B, Topcu S and Muezzinoglu B: Primary synovial
sarcoma of lung. Korean J Thorac Cardiovasc Surg. 47:306–309. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Falkenstern-Ge RF, Kimmich M, Grabner A,
Horn H, Friedel G, Ott G and Kohlhäufl M: Primary pulmonary
synovial sarcoma: A rare primary pulmonary tumor. Lung.
192:211–214. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Dennison S, Weppler E and Giacoppe G:
Primary pulmonary synovial sarcoma: A case report and review of
current diagnostic and therapeutic standards. Oncologist.
9:339–342. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Spraker MB, Bair E, Bair R, Connell PP,
Mahmood U and Koshy M: An analysis of patient characteristics and
clinical outcomes in primary pulmonary sarcoma. J Thorac Oncol.
8:147–151. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Weiss SW: Histological Typing of Soft
Tissue Tumors. Sobin LH: (2nd). Berlin: Springer-Verlag. 7–14.
1994. View Article : Google Scholar
|
|
10
|
Liu K and Li W: Analysis of 19 cases of
primary pulmonary sarcoma. Zhongguo Fei Ai Za Zhi. 15:375–380.
2012.(In Chinese). PubMed/NCBI
|
|
11
|
Cai AQ, Chen JW, Zhou XG and Lin JB: CT
diagnosis of primary sarcoma of lung. Han Shao Ji Bing Za Zhi.
11:10–12. 2004.(In Chinese).
|
|
12
|
Okamoto S, Hisaoka M, Daa T, Hatakeyama K,
Iwamasa T and Hashimoto H: Primary pulmonary synovial sarcoma: A
clinicopathologic, immunohistochemical and molecular study of 11
cases. Hum Pathol. 35:850–856. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hartel PH, Fanburg-Smith JC, Frazier AA,
Galvin JR, Lichy JH, Shilo K and Franks TJ: Primary pulmonary and
mediastinal synovial sarcoma: A clinicopathologic study of 60 cases
and comparison with five prior series. Mod Pathol. 20:760–769.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Olsen SH, Thomas DG and Lucas DR: Cluster
analysis of immunohistochemical profiles in synovial sarcoma,
malignant peripheral nerve sheath tumor and Ewing sarcoma. Mod
Pathol. 19:659–668. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
van de Rijn M, Barr FG, Collins MH, Xiong
QB and Fisher C: Absence of SYT-SSX fusion products in soft tissue
tumors other than synovial sarcoma. Am J Clin Pathol. 112:43–49.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Magné N, Porsin B, Pivot X, Tchiknavorian
X, Marcy PY, Foa C, Otto J, Schneider M and Thyss A: Primary lung
sarcomas: Long survivors obtained with iterative complete surgery.
Lung Cancer. 31:241–245. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Régnard JF, Icard P, Guibert L, de
Montpreville VT, Magdeleinat P and Levasseur P: Prognostic factors
and results after surgical treatment of primary sarcomas of the
lung. Ann Thorac Surg. 68:227–231. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Trassard M, Le Doussal V, Hacène K,
Terrier P, Ranchère D, Guillou L, Fiche M, Collin F, Vilain MO,
Bertrand G, et al: Prognostic factors in localized primary synovial
sarcoma: A multicenter study of 128 adult patients. J Clin Oncol.
19:525–534. 2001.PubMed/NCBI
|
|
19
|
Spillane AJ, A'Hern R, Judson IR, Fisher C
and Thomas JM: Synovial sarcoma: A clinicopathologic, staging and
prognostic assessment. J Clin Oncol. 18:3794–3803. 2000.PubMed/NCBI
|