Introduction
Atherosclerosis (AS) is a common pathological basis
of many cardiovascular and cerebrovascular diseases. It is the most
common disease among cardiovascular diseases that may be life
threatening. The prevailing view is that the occurrence and
development of AS is a chronic inflammatory process (1,2).
Endothelial cells synthesize a variety of adhesion molecules in
response to the injury factors. The mononuclear cells adhere to the
vessel wall, enter through the endothelial cells and differentiate
into macrophages. Subsequently, mediated by scavenger receptor A
(SRA), the macrophages engulf a large amount of lipid deposited in
the intimal, and gradually transform into foam cells (3).
The concentration of inflammatory mediators in the
local environment increase vascular damage, accompanied by the
change of activities of the local coagulation, complement, and
kinin-kallikrein systems (4). The
change of local signal microenvironment leads to smooth muscle
cells and endothelial cell dysplasia into the vessel wall. Part of
smooth muscle cells secret collagen fibers, elastic fibers and
proteoglycans, which embed lipid and cells forming a fibrous plaque
(5). The further involvement of
inflammatory cells and inflammatory factors leads to the fibrous
plaque cap rupturing and shedding, resulting in the exposure of
deep lesions (collagen, tissue necrosis disintegrating substance,
cholesterol and calcium). The exposure leads to the formation of
thrombosis and vascular embolism and triggers serious
cardiovascular and cerebrovascular events (3).
Previous findings have confirmed that macrophages
are important in the atherosclerotic vulnerable plaque formation
process. Ultrasmall superparamagnetic iron oxide (USPIO) can be
engulfed by macrophages and as a result, engulfed USPIO may deposit
within macrophages (6–8). The engulfed USPIO inside macrophages
can be detected using Prussian blue staining. According to this
feature, USPIO-enhanced MRI becomes an effective technique in
detecting AS vulnerable plaque (9).
It has been demonstrated that the expression of cell adhesion
molecule 1 (ICAM-1) and vascular cell adhesion molecule-l (VCAM-1)
in macrophages increase in atherosclerotic rabbits (10). Adhesion molecules are important
inflammatory factors in the plaque formation process. ICAM-1 and
VCAM-1 are cell surface transmembrane glycoproteins that regulate
the adhesions and interactions between cells, as well as between
cells and matrix. They promote the adhesion of leukocytes to
endothelial cells, which is the initiating step during the AS
process (11). Previous experiments
have shown that statins have lipid-lowering, anti-inflammatory, and
plaque stability, albeit the mechanism is not clear. The rabbit was
selected to establish the AS model, given atorvastatin
pharmaceutical intervention, and related indicators were measured
to verify the role of atorvastatin in the vulnerable plaque.
Materials and methods
Experimental animals and groups
In the present study, 30 healthy male New Zealand
(NZ) white rabbits (Experimental Animal Center of Xuzhou Medical
College, Xuzhou, China), weighing 2.5–3.0 kg were used. The rabbits
were kept in single cages, with access to water and feed ad
libitum. The animals were divided into three groups: group A,
high-fat (1% cholesterol, 0.2% bile salt, 10% lard, 88.8% normal
diet, each 120–140 g/day) feeding alone group; group B,
balloon-induced injury plus high cholesterol feeding group; and
group C, atorvastatin group (n=10/group). Approval for the animal
studies was provided by the Xuzhou Medical Ethics Committee,
license number: CMCACUC2009-04–135.
Atherosclerotic vulnerable plaque
model
In total, 30 male NZ white rabbits were fed with a
high-fat diet. The rabbits in groups B and C underwent abdominal
aorta balloon-induced injury after one week. Briefly, the rabbits
were anesthetized through with 30 mg/kg sodium pentobarbital via
injecting the rabbit ear vein. Puncture of the right femoral artery
was performed and a balloon catheter of 3.5-mm diameter and 15 mm
in length was introduced into the aorta approximately 20 cm along
the 0.014 inch guide wire. The balloon was inflated by injecting
distilled water up to 8 atmospheres and was then pulled back to the
common iliac artery. The balloon was repeatedly pulled back 3 times
to injure the abdominal aortic endothelium. The femoral artery was
ligated and intramuscular injection of penicillin was given to
prevent infection. A high-cholesterol diet (1% cholesterol, 0.2%
bile salt, 10% lard, and 88.8% normal diet, each 120–140 g/day) was
provided to experimental animals for 8 weeks.
Wild-type Ad-p53 virus transfection in
local plaque
At the end of week 8, the rabbits underwent Ad-p53
transfection. The animals were anesthetized through the injection
of 30 mg/kg sodium pentobarbital via the rabbit ear vein. An
incision was made to the abdominal cavity to expose the abdominal
aorta to locate the largest patch at the vessel segment between the
right renal artery and common iliac artery; this was the site where
the viral vector were transfected. Following transient closure of
the blood vessel in the two sides, 10 µl of 1.5×1010
pfu/ml Ad5-p53 recombinant vector were injected into the plaque.
After 10 min, the blood supply was restored in the abdominal
artery. A suture mark was added in the ligation site and the
abdominal cavity was closed. Penicillin was intramuscularly
injected to prevent infection.
First MRI examination to detect plaque
formation
At the end of week 8, an MRI (Philips MedicalSystem,
Eindhoven, The Netherlands) examination was conducted on all the
experimental rabbits to monitor whether atherosclerotic plaques
were formed. Various plaque characteristics were observed and
recorded. At the end of week 8, when plaque formation was confirmed
by MRI, the drug intervention (2 mg/kg/day) was given immediately
for 8 weeks. At the end of week 16, based on the methodology
previously described (12),
peritoneal injection of 0.15 mg/kg Chinese Russell's viper venom
(CRVV Guangdong, Research Institute of Snake Venom, Guangdong,
China) was performed twice. After 30 min and 24 h, 0.02 mg/kg
histamine (Dongfeng Biological Technology, Shanghai, China) was
injected via the ear vein.
Second MRI examination to detect
breakage of plaque
Aortic MRI imaging was conducted at time points
prior to medication and 0, 24, 48, 72 and 96 h after the
medication. The signal intensity (SI), signal-to-noise ratio (SNR),
size of lumen area and size of plaque area were determined to
compare difference in plaque characteristics in the three
groups.
Blood biochemical indices and
detection of inflammatory factors
Total cholesterol (TC), triglyceride (TG),
high-density lipoprotein cholesterol (HDL-C) and low-density
lipoprotein cholesterol (LDL-C) levels were measured in all the
rabbits prior to and following the intervention of simvastatin. The
blood was collected in the morning on fasting via the marginal ear
vein. VCAM-1 and ICAM-1 levels were determined using enzyme-linked
immunosorbent assay (ELISA).
Histopathological detection
Morphological characteristics of ruptured and
unruptured plaque were observed using hematoxylin and eosin
(H&E) and Masson's trichrome staining. The deposition of the
USPIO particles within the plaque was observed using Prussian blue
staining.
Electron microscopy measurement
The ultrastructural changes and apoptosis of cells
were observed using transmission electron microscope (TEM).
Statistical analysis
Quantitative data were presented as the mean ± SD,
of multiple sets of variables and compared using one-way ANOVA and
Cochran's Q test pairwise comparisons, P<0.05 was considered
statistically significant differences. Data were analyzed using
SPSS 16.0 software.
Results
Comparison of blood lipid profile
TC, LDH, and triglycerol blood levels were
significantly higher (P<0.05) at the end of week 16 in all three
groups. At the end of week 16, the inter-group comparison showed a
significant reduction in blood TC, LDH, and triglycerol of group C
(P<0.05) in comparison to groups A and B (Table I).
 | Table I.Comparison of blood lipid profile. |
Table I.
Comparison of blood lipid profile.
| Variables | Group A | Group B | Group C |
|---|
| TC (mmol/l) |
|
|
|
| Day
0 |
1.331±0.069 |
1.324±0.054 |
1.293±0.047 |
| End of
W16 |
10.911±0.646a |
11.571±0.683a |
2.388±0.128ab |
| LDH (mmol/l) |
|
|
|
| Day
0 |
0.548±0.042 |
0.548±0.042 |
0.533±0.048 |
| End of
W16 |
7.159±0.188a |
8.286±0.119a |
2.087±0.056b |
| HDL (mmol/l) |
|
|
|
| Day
0 |
1.046±0.062 |
1.128±0.051 |
1.286±0.119 |
| End of
W16 |
0.690±0.045 |
0.708±0.030 |
0.699±0.021 |
| Triglycerol
(mmol/l) |
|
|
|
| Day
0 |
1.079±0.068 |
1.081±0.041 |
1.113±0.047 |
| End of
W16 |
1.24±0.09a |
4.977±0.121a |
2.106±0.073ab |
Comparison of the expression of VCAM-1
and ICAM-1
VCAM-1 and ICAM-1 levels were significantly higher
(P<0.05) at the end of week 16 in groups A and B. Inter-group
comparison at the end of week 16 showed that VCAM-1 and ICAM-1
levels were significantly lower (P<0.05) as compared to groups A
and B (Table II).
| Table II.Comparison of VCAM-1 and ICAM-1. |
Table II.
Comparison of VCAM-1 and ICAM-1.
| Variables | Group A | Group B | Group C |
|---|
| VCAM-1 (pg/ml) |
|
|
|
| Day
0 |
1.100±0.065 |
1.115±0.043 |
1.104±0.040 |
| End of
W16 |
2.018±0.062a |
2.477±0.060a |
1.420±0.046b |
| ICAM-1 (pg/ml) |
|
|
|
| Day
0 |
0.954±0.046 |
0.973±0.035 |
0.979±0.023 |
| End of
W16 |
1.904±0.033a |
2.920±0.041a |
1.263±0.041b |
Comparison of MRI indices
Indices in group B or C were statistically different
from the counterparts in group A regarding EEMA, LA, PA, LAS%, VD,
LD, PT, and EI values (Table
III).
| Table III.Comparison of indices of MRI
(mm2). |
Table III.
Comparison of indices of MRI
(mm2).
| Variables | Group A | Group A | Group A |
|---|
| EEMA
(mm2) |
12.91±1.37 |
21.15±2.69a,b |
17.40±0.58a |
| LA
(mm2) |
8.71±0.61 |
12.49±0.92a,b |
10.9±0.84a |
| LD min (mm) |
1.56±0.17 |
2.78±0.19a,b |
2.7±0.23a |
| VD max (mm) |
1.18±0.08 |
1.56±0.19a,b |
2.36±0.09a |
| VD min (mm) |
1.06±0.11 |
0.74±0.11a,b |
2.12±0.24a |
| PT max (mm) |
0.48±0.08 |
0.76±0.05a,b |
0.30±0.07a |
| PT min (mm) |
0.34±0.05 |
0.32±0.04a,b |
0.20±0.07a |
| LAS (%) |
32.15±5.99 |
40.40±6.4a,b |
37.14±4.50a |
| EI |
0.32±0.08 |
0.55±0.08a,b |
0.35±0.09a |
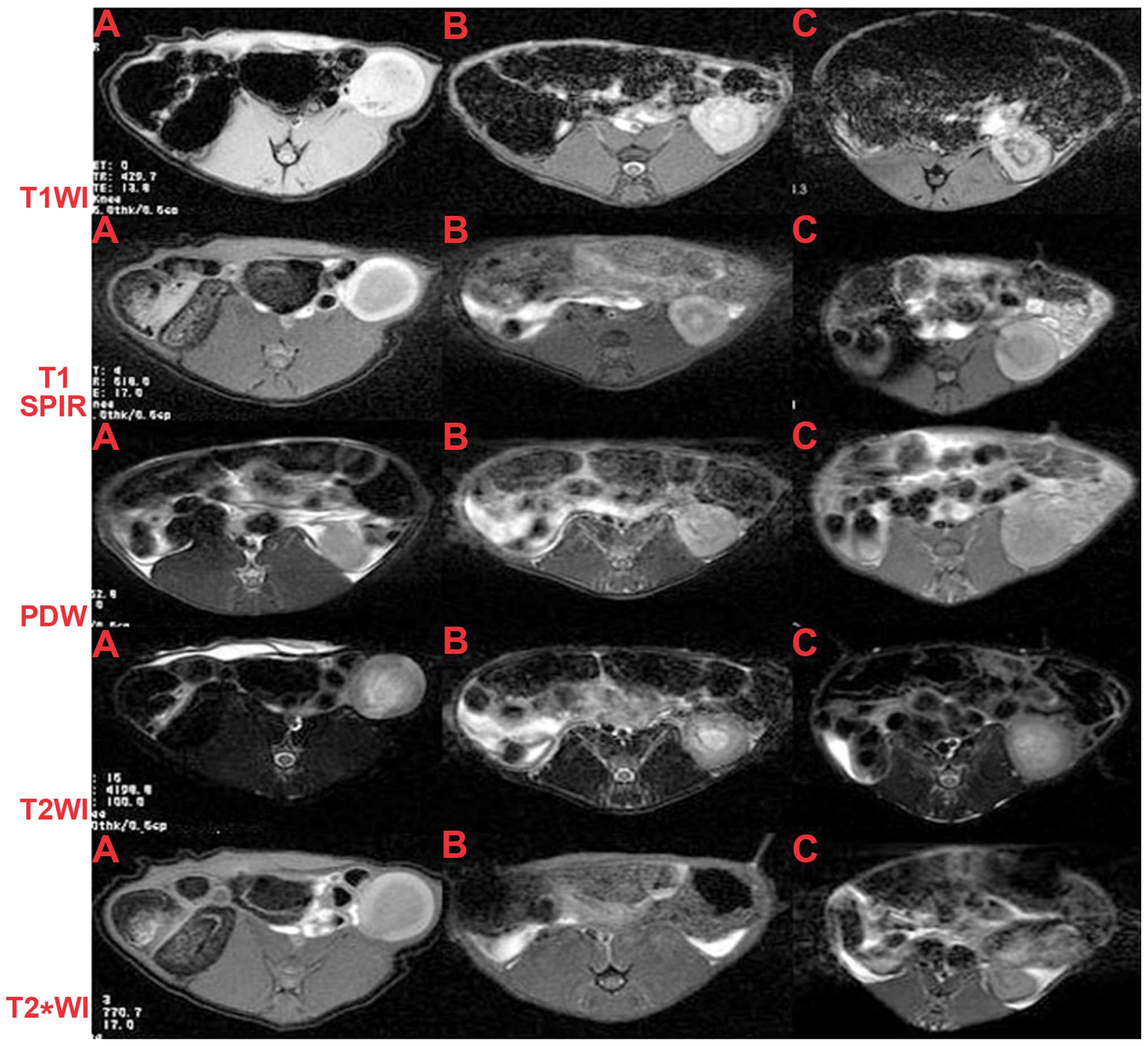
Comparison of MRI imaging among the
different groups
In group A, a narrow lumen ring is evident in the
images as a flat- or crescent-shaped plaque protruding into the
lumen (Fig. 1). The lipid
composition basically can be distinguished in terms of the
prominent plaque. The fibrous caps were clearly evident in some
sequences. Lipid composition showed slightly higher signals in
T1WI, PDWI and T2*WI as compared to the low signal from the entire
plaque in T2WI (Fig. 1). In T2WI,
the lipid core cannot be clearly distinguished and the unenhanced
T1WI fat-suppression cannot inhibit completely the lipid signal.
After injection of USPIO, the high signal in T2*WI was markedly
reduced. Pathological results confirmed iron deposition in the high
signal area. In other sequences, the changes of plaque signals were
not obvious. The sensitivity of USPIO-enhanced sequences did not
significantly increase in distinguishing the fibrous caps. In group
B, abdominal aortic lumen narrow ring or eccentric plaque was
evident in all the scan sequences. The plaque signals were high in
T1WI, PDWI and T2*WI and low in T2WI. In the lipid suppression
sequence T1WI, the decrease of plaque signal was not obvious.
Following the medication trigger, the obvious breakage of plaque
was evident. By 96 h after enhanced USPIO, the plaque signals in
the T2WI and T2*WI were significantly reduced. At 96 h after
injection of contrast, the negative reinforcement reached its peak
(Fig. 1). In group C, the reduction
of plaques after medication intervention and increase of lumen
diameter were observed. Obvious breakage of plaques was not
observed (Fig. 1).
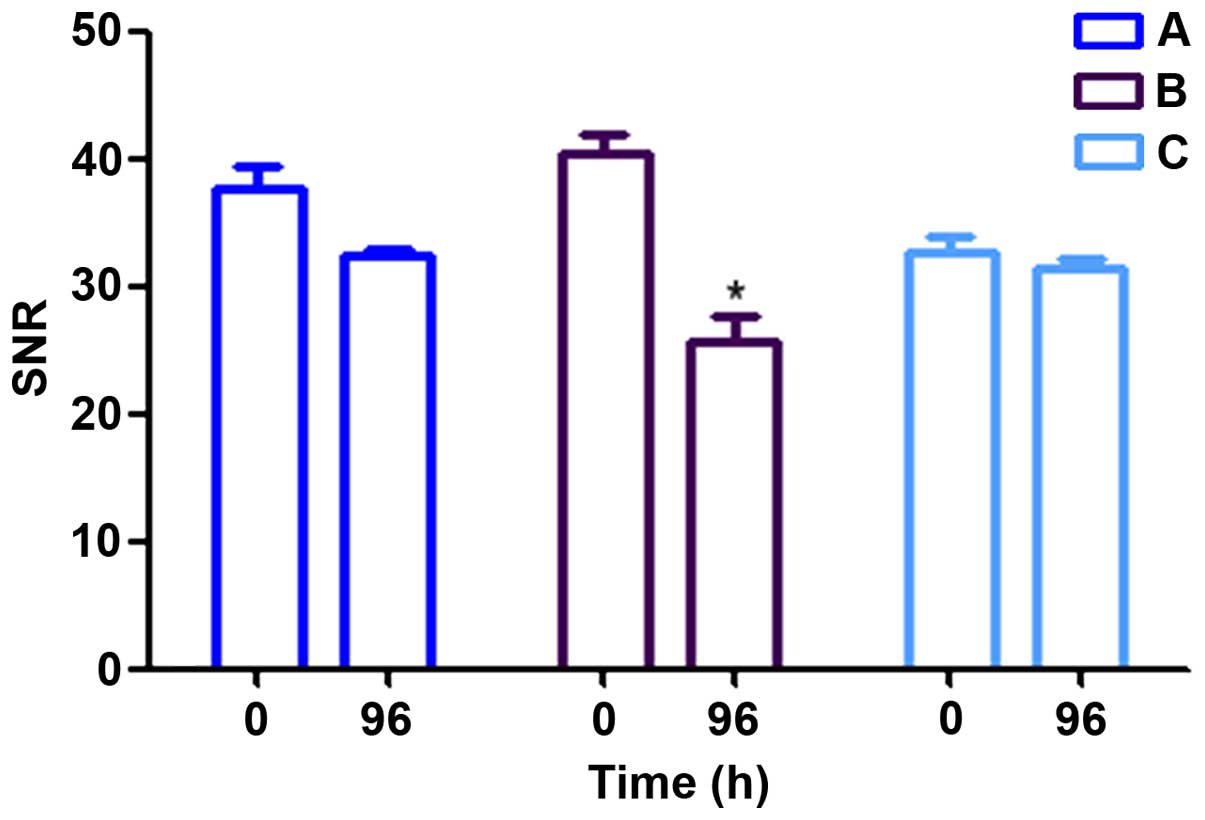
Comparison of SNR
A comparison of the SNR change prior to its
enhancement at 96 h and after enhancement revealed that the
negative enhancement of plaque signals in group B peaked. By
contrast, the changes in groups A and C showed no statistical
difference (P>0.05), indicating that the nature and composition
of plaques did not change significantly (Fig. 2).
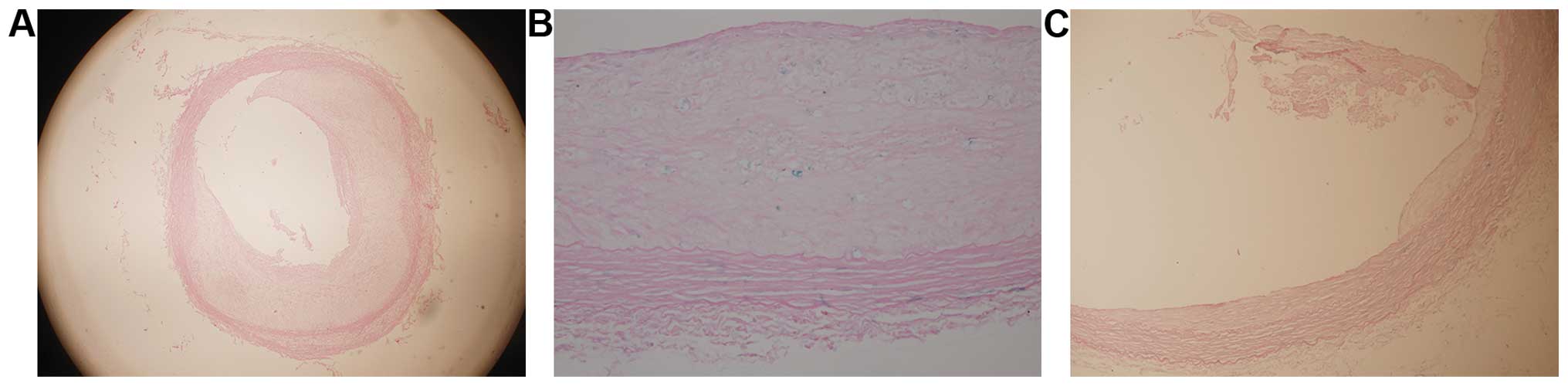
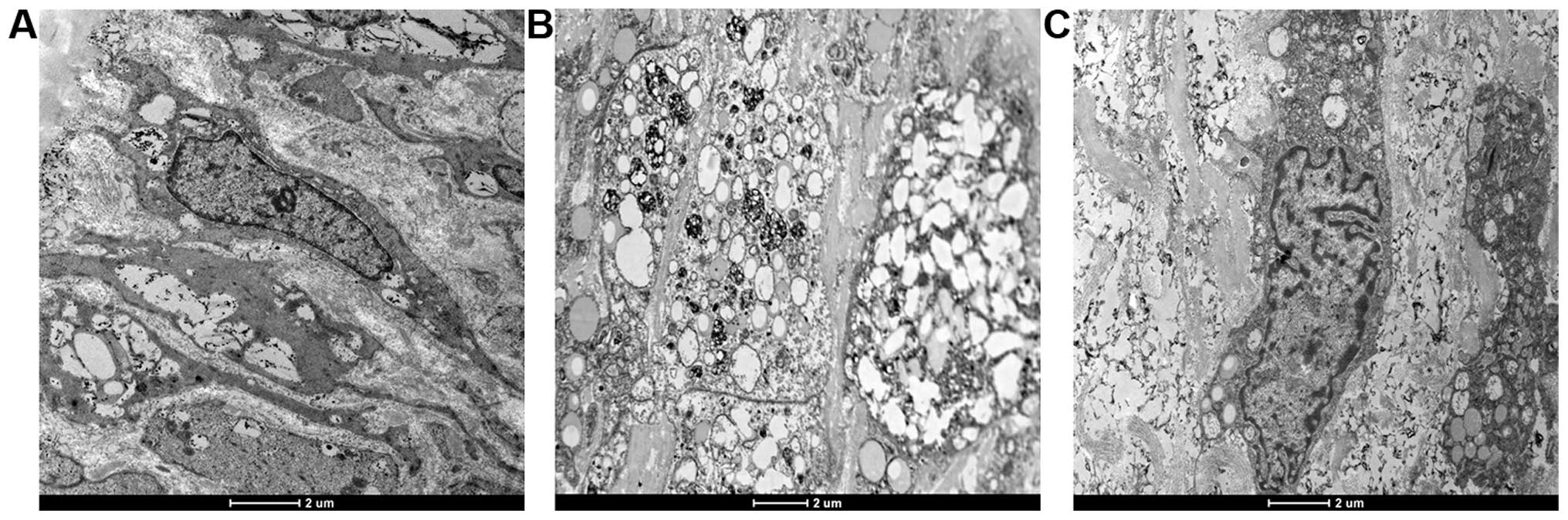
Comparison of microscopic observations
in different groups
Comparisons of foam cells, degree of narrowing and
existence of plaque hemorrhage were evaluated using H&E
staining. We found some wall thickening in group A and obvious
thickening with substantial foam cell formation and large lipid
core plaque hemorrhage in group B. Additionally, the wall was
relatively smooth and obvious foam cell formation or plaque
hemorrhage was not observed (Fig.
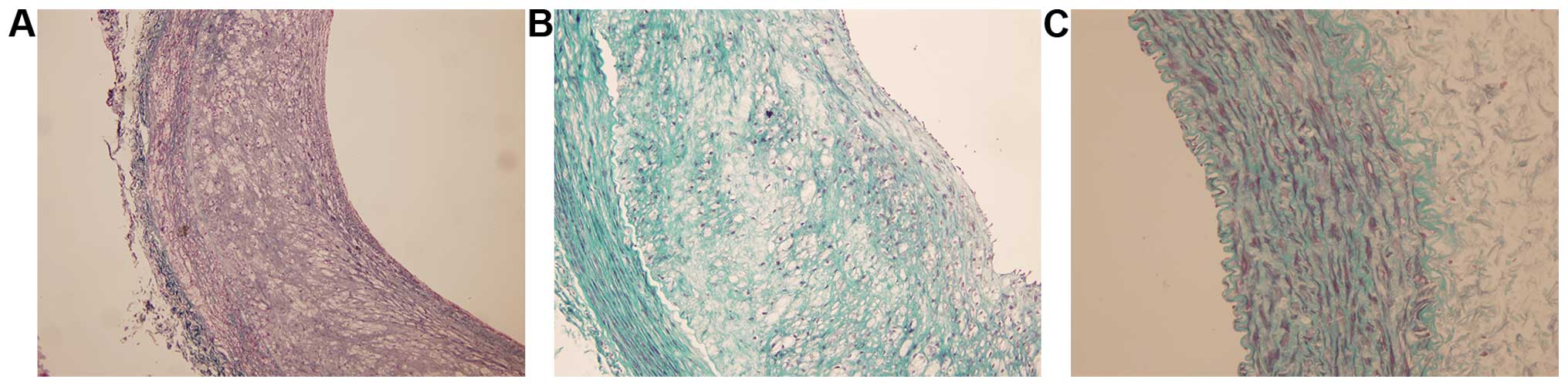
3). Moreover, Masson's staining reflected the collagen fiber
hyperplasia in the vessel wall. In group B, substantial collagen
fiber proliferation was evident (Fig.
4). In addition, Prussian blue staining in group B indicated
the iron deposition inside macrophages and no iron deposition was
evident in the remaining two groups (Fig. 5). In group B visible lysosome
increased, foam cells proliferated, intracellular lipid droplets
were visible, while fewer foam cells were present in group C, no
lysosomal generation, and iron particles were rare (Fig. 6).
Discussion
ACS is one of the common diseases of the
cardiovascular system forming the basis of the pathophysiology of
atherosclerotic plaque, and plaque instability or rupture are
clinically acute syndromes and the main reasons especially for
acute coronary syndrome (13,14). The
instability is caused by multiple factors plaques, including the
size of the plaque itself, and thickness of the fibrous cap,
apoptosis, the release of various cytokines and enzymes (15), and atherosclerotic plaques block
instability and rupture caused by a series of cardiovascular
events.
Although the establishment of atherosclerotic
vulnerable plaque model has been intensively studied, well-rounded
vulnerable plaque models are rare. Some researchers used simple
high-fat diet feeding and as a result most of the established
models are stable plaque models (16,17).
Kurz et al established a model using the Rose Bengal antigen
or Fe3+ (18). However,
these models were not established based on the disease. A
Successfully established animal model of drug-induced plaque
breakage using the CRVV and histamine triggering atherosclerotic
plaque has been reported (19).
In some studies, the authors found that the
regulatory genes of AS plaque apoptosis are mainly c-Myc, Bcl-2 and
p53. Most of p53 genes are mutants, while the expression level of
wild-type p53 gene is low. It is considered that abnormal SMC
proliferation is related to the gene mutation of p53. However, the
roles of wild-type and mutant p53 are different. Wild-type p53 gene
plays a role in promoting apoptosis whereas mutant p53 genes
inhibit apoptosis. The p53 gene directly transfecting the local
plaque and thinning the fibrous cap via the role of pro-apoptosis
on VSMC are good methods to establish the animal model of
vulnerable plaque. The VSMC apoptotic rate increases and smooth
muscle actin-positive cells were significantly reduced after p53
gene transfection, leading to a significantly thinner fibrous cap
of the plaque. As a result, the plaque becomes unstable. Chen et
al firstly established an animal model of vulnerable plaque
using exogenous p53 gene transfecting rabbit AS plaque (19,20). The
success rate was significantly increased following a combination of
the two methods. In this study, we utilized exogenous p53
gene-transfecting rabbit AS plaque in the abdominal aorta and
successfully established a rabbit model of vulnerable plaque.
USPIO is a new type of magnetic MRI contrast agent
that is recognized by the reticuloendothelial system (RES) and
uptaken by macrophage. Due to the long plasma half-life, USPIO can
be widely distributed in the macrophages of RES (21,22). One
of the targeting studies of MRI focused on macrophages which
reflect the instability of the plaques. Among several methods for
the identification, analysis and quantification of the plaque
macrophage density, two important types are: i) passive targeting
USPIO; and ii) active targeting gadolinium-labeled antibody
particles. The active macrophages inside the plaque can
significantly engulf the iron oxide particles, thus, USPIO-labeled
macrophage imaging is often used as a passive target. Nevertheless,
the characteristics that macrophages uptake USPIO has been widely
confirmed, and the exact route how USPIO enter macrophages remain
unclear. When the diameter of iron nanoparticles is less than the
critical value of the magnetic particles (30 nm), it shows
superparamagnetism. When it enters the body and binds to plasma
protein, these iron nanoparticles are recognized by opsonized RES
and engulfed by phagocytes and residue inside the
reticuloendothelial cells. The superparamagnetic effect causes an
uneven local magnetic field in tissues. When the water molecules
diffuse through the heterogeneous magnetic field, water accelerates
the proton loss phase, and shortens the tissue transverse
relaxation time (T2) and longitudinal relaxation time (T1). As a
result, the corresponding T1 and T2 changes can be detected on MR
images. Therefore, USPIO can be used to mark the inflammatory cells
and can be observed on MR in vivo. Due to its
multi-parameter, multi-sequence characteristics, magnetic resonance
can distinguish fat, calcification, fibrous and thrombosis
ingredients with a characteristic signal (23).
Effects of statins, other than on lipid
modification, have been previously reported (24). Results from clinical trials have
shown that statins can significantly reduce cardiovascular-related
morbidity and mortality in patients with and without cardiovascular
diseases (24). Results from
experimental animal models have confirmed that statin therapy can
stabilize atherosclerotic plaques, including reducing extracellular
lipid deposition, reducing the number of macrophages and the amount
of cholesterol inside the intima, increasing collagen and the SMC
area, reducing calcification of the intima and angiogenesis,
reducing the lipid cores of plaques by reducing LDL levels in the
blood, reducing plaque surface tension, strengthening the fibrous
cap, and maximally stabilizing and shrinking plaques (25,26). In
general, statins have strong anti-proliferation and anti-migration
effects. Atorvastatin calcium is a 3-hydroxy-3-methyl-diacyloxy
coenzyme (HMA-CoA) reductase inhibitor, by inhibiting HMA-CoA, the
synthesis rate-limiting enzyme of TC. Atorvastatin can
significantly reduce the blood LDL-C level by inhibiting the
synthesis of TC in hepatocytes and upregulating the density and
activity of LDL-C receptor on the surface of hepatocytes.
In the present study, we found that VCAM-1 is
overexpressed in the AS lesion site. Atorvastatin inhibits VCAM-1
expression and the hyperplasia of the artery intima, leading to the
shrinkage of AS plaques. In conclusion, atorvastatin has a role,
not only in lowering the lipid profile, but in reversing AS.
Inhibiting VCAM-1 expression may be one of the mechanisms in which
atorvastatin inhibits AS. We believe that the effective
anti-inflammatory dose of atorvastatin may be lower than the
effective lipid-lowering doses. The lipid-lowering efficacy is
associated with the dose and duration, whereas the
anti-inflammatory effect is dose-dependent.
Acknowledgements
The present study was funded by the Six Talents
Peak, no. 2014-WSN-044.
References
|
1
|
Virani SS, Polsani VR and Nambi V: Novel
markers of infam-mation in atherosclerosis. Curr Atheroscler Rep.
10:164–170. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kleemann R, Zadelaar S and Kooistra T:
Cytokines and athero-sclerosis: A comprehensive review of studies
in mice. Cardiovasc Res. 79:360–376. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wang HD, Yu SQ, Gao F and Qin ML: The
anti-atherosclerosiseffect of adiponectin. Chongqing Med J.
38:2509–2510. 2009.(In Chinese).
|
|
4
|
Pasceri V, Willerson JT and Yeh ET: Direct
proinflammatory effect of C-reactive protein on human endothelial
cells. Circulation. 102:2165–2168. 2002. View Article : Google Scholar
|
|
5
|
Beck B, Weintraub W and Alexander R:
Elevation of C-reactive protein in ‘active’ coronary artery
disease. AMJ Cardiol. 65:168–172. 1990. View Article : Google Scholar
|
|
6
|
Ross R: Atherosclerosis - an infammatory
disease. N Engl J Med. 340:115–126. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tang T, Howarth SP, Miller SR, Trivedi R,
Graves MJ, King-Im JU, Li ZY, Brown AP, Kirkpatrick PJ, Gaunt ME,
et al: Assessment of infammatory burden contralateral to the
symptomatic carotid stenosis using high-resolution ultrasmall,
superparamagnetic iron oxide-enhanced MRI. Stroke. 37:2266–2270.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Howarth SP, Tang TY, Graves MJ, U-King-Im
JM, Li ZY, Walsh SR, Gaunt ME and Gillard JH: Non-invasive MR
imaging of infammation in a patient with both asymptomatic
carotidatheroma and an abdominal aortic aneurysm: A case report.
Ann Surg Innov Res. 1:42007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Metz S, Beer AJ, Settles M, Pelisek J,
Botnar RM, Rummeny EJ and Heider P: Characterization of carotid
artery plaques with USPIO-enhanced MRI: Assessment of infammation
and vascu-larity as in vivo imaging biomarkers for plaque
vulnerability. Int J Cardiovasc Imaging. 27:901–912. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Truskey GA, Herrmann RA, Kait J and Barber
KM: Focalincreases in vascular cell adhesion molecule-1 and intimal
macrophages at atherosclerosis-susceptible sites in the rabbit
aorta after short-term cholesterol feeding. Arterioscler Thromb
Vasc Biol. 19:393–401. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cybulsky MI, Iiyama K, Li H, Zhu S, Chen
M, Iiyama M, Davis V, Gutierrez-Ramos JC, Connelly PW and Milstone
DS: A major role for VCAM-1, but not ICAM-1, in early
atherosclerosis. J Clin Invest. 107:1255–1262. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kolodgie FD, Gold HK, Burke AP, Fowler DR,
Kruth HS, Weber DK, Farb A, Guerrero LJ, Hayase M, Kutys R, et al:
Intraplaque hemorrhage and progression of coronary atheroma. N Engl
J Med. 349:2316–2325. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Danesh J, Wheeler JG, Hirschfield GM, Eda
S, Eiriksdottir G, Rumley A, Lowe GD, Pepys MB and Gudnason V:
C-reactive protein and other circulating markers of inflammation in
the prediction of coronary heart disease. N Engl J Med.
350:1387–1397. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Curb JD, Abbott RD, Rodriguez BL, Sakkinen
P, Popper JS, Yano K and Tracy RP: C-reation protein and the future
risk of thromboembolic stroke in healthy men. Circulation.
107:2016–2020. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Schupp M, Janke J, Clasen R, Unger T and
Kintscher U: Angiotensin type-1 receptor blockers induce peroxisome
proliferator-activated receptor-gamma activity. Circulation.
109:2054–2057. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Padda RS, Shi Y, Lo CS, Zhang SL and Chan
JS: Angiotensin-(1–7): A novel peptide to treat hypertension and
nephropathy in diabetes? J Diabetes Metab. 6:1–6. 2015.
|
|
17
|
Padda RS, Gkouvatsos K, Guido M, Mui J,
Vali H and Pantopoulos K: A high-fat diet modulates iron metabolism
but does not promote liver fibrosis in hemochromatotic
Hjv−/− mice. Am J Physiol Gastrointest Liver Physiol.
308:G251–G261. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kurz KD, Main BW and Sandusky GE: Rat
model of arterial thrombosis induced by ferric chloride. Thromb
Res. 60:269–280. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Chen WQ, Zhang Y, Zhang M, Ji XP, Yin Y
and Zhu YF: Establishing an animal model of unstable
atherosclerotic plaques. Chin Med J (Engl). 117:1293–1298.
2004.PubMed/NCBI
|
|
20
|
Chen WQ, Zhang L, Liu YF, Chen L, Ji XP,
Zhang M, Zhao YX, Yao GH, Zhang C, Wang XL, et al: Prediction of
atherosclerotic plaque ruptures with high-frequency ultrasound
imaging and serum inflammatory markers. Am J Physiol Heart Circ
Physiol. 293:H2836–H2844. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Cormode DP, Skajaa T, Fayad ZA and Mulder
WJ: Nanotechnology in medical imaging: Probe design and
applications. Arterioscler Thromb Vasc Biol. 29:992–1000. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Cormode DP, Briley-Saebo KC, Mulder WJ,
Aguinaldo JG, Barazza A, Ma Y, Fisher EA and Fayad ZA: An
ApoA-Imimetic peptide high-density-lipoprotein-based MRI
contrastagent for atherosclerotic plaque composition detection.
Small. 4:1437–1444. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Clarke SE, Beletsky V, Hammond RR, Hegele
RA and Rutt BK: Validation of automatically classified magnetic
resonance images for carotid plaque compositional analysis. Stroke.
37:93–97. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Drakopoulou M, Toutouzas K, Michelongona
A, Tousoulis D and Stefanadis C: Vulnerable plaque and
inflammation: Potential clinical strategies. Curr Pharm Des.
17:4190–4209. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Li D, Chen H, Romeo F, Sawamura T, Saldeen
T and Mehta JL: Statins modulate oxidized low-density
lipoprotein-mediated adhesion molecule expression in human coronary
artery endothelial cells: Role of LOX-1. J Pharmacol Exp Ther.
302:601–605. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Li DY, Chen HJ and Mehta JL: Statins
inhibit oxidized-LDL-medated LOX-1 expression, uptake of
oxidized-LDL and reduction in PKB phosphorylation. Cardiovasc Res.
52:130–135. 2001. View Article : Google Scholar : PubMed/NCBI
|