Introduction
Schizophrenia is a chronic disabling mental illness
and has been listed as a major public health issue comparable to
that of the HIV epidemic (1). The
incidence of schizophrenia is ~1% worldwide (2). Its cause, however, remains unclear.
There have been advances in the treatment options to control
symptoms but the prognosis for the majority of patients remains
poor with the majority of patients staying incapacitated for life
(3). New evidence seems to indicate
that white matter abnormalities may be an important
pathophysiological finding in schizophrenia (4); however, the results are inconsistent.
Previous findings have shown that the seriousness of negative
symptoms of schizophrenia may be associated with more intense white
matter abnormalities (5), although
other authors have found opposing results (6) complicating the analysis. The focus thus
far has been on initial positive symptoms, therapeutic effects in
patients with negative symptoms, social function and the extent of
damage and prognosis, where there is a tendency to identify brain
cell loss and degeneration (7).
Diffusion-tensor tractography (DTT) is a new
magnetic resonance imaging (MRI) technology characterized by being
non-invasive, not requiring exogenous contrast agents (8). It measures dispersion characteristics
throughout nervous tissues, and is the only method providing
high-quality biological tissue imaging to obtain clinical
information, physical properties, microstructure and structural
up-to-date data. Diffusion-tensor imaging (DTI) can identify
abnormalities in the brain white matter microstructure, and is
widely used in studies of brain connection structures in
schizophrenia (9). Compared with
single techniques, the combined applications of the region of
interest (ROI), such as brain analysis based on voxel (VBA) and
fiber tracking (FT) in DTI, as well as data statistical analysis
methods have a higher diagnostic accuracy, and can produce real and
reliable results (10). Different
MRI analysis methods and FT have been combined and applied to
children with retinal congenital malformations, congenital brain
malformation, amyotrophic lateral sclerosis, computing capacity in
developmental disorders as well as to healthy individuals,
achieving promising results (11).
However, to the best of our knowledge, this is the first study to
be applied to schizophrenic patients.
A previous meta-analysis concluded that the white
matter abnormalities of schizophrenia are mainly located on the
left prefrontal deep and deep white matter in the left temporal
lobe (12). However, findings of
other studies have shown that schizophrenia with typical first
negative symptoms is correlated with complete damage in the
inferior frontal gyrus white matter (13). The present study used VBA and FT on
structural integrity of white matter in schizophrenic patients with
typical first negative symptoms to obtain more accurate
results.
Patients and methods
Patient information
Patients diagnosed as schizophrenic at the Tongde
Hospital of Zhejiang Province (Zhejiang, China) between June 2014
and December 2015 were continuously enrolled in the study. The
diagnostic criteria conformed to those of the American Diagnostic
and Statistical Manual of Mental Disorders, 4th edition (14), and two psychiatrists diagnosed each
patient independently. Inclusion criteria for the study were: i)
Negative scores in positive and negative symptom scale (PANSS) of
≥40 as well as positive scores of ≤20, ii) patients aged 16–60
years, iii) right-handedness and taking no psychotropic substances,
and iv) guardians signed the informed consent. Exclusion criteria
for the study were: i) MRI scan contraindications, ii) presence of
severe organic disease, iii) history of psychoactive substance
abuse, iv) history of traumatic brain injury or electric shock, v)
pregnant and lactating women, and vi) symptoms of other psychiatric
diseases confounding the diagnoses.
A total of 30 schizophrenic patients with typical
first negative symptoms were selected for the observation group.
Thirty right-handed healthy individuals served as the control
group. The observation group included 12 men and 14 women, aged
23–58 years, average age of 39.7±11.6 years, with the length of
education time from 11 to 18 years, and an average of 13.5±4.4
years, and disease history of 1–6 months. The control group
included 13 men and 17 women, aged 21–56 years, average of
36.8±12.5 years, with the length of education time from 12 to 19
years, and an average of 13.8±4.3 years. Comparisons of gender, age
and education time differences between the two groups yielded no
statistically significant results (P>0.05). The ethics committee
of the Tongde Hospital of Zhejiang Province approved this
study.
Inspecting methods
A 3.0 T GE Signa TwinSpeed MRI machine (GE
Healthcare, Piscataway, NJ, USA) was used to scan a patients
education time of 12–19 years (with an average of 13 years). The
patient was required to remain in a supine position wearing
earplugs to reduce the noise from the machine (GEHealthcare,
Piscataway, NJ, USA). The head was immobilized using foams as per
the manufacturer's instructions.
The MRI data collection involved two separate steps:
i) The image relevant to the clinical diagnosis was collected: A
coronary spin echo sequence was used to obtain the T2-weighted and
proton density-weighted images while the neuroimaging
diagnosticians eliminated irrelevant data. ii) DTI data collection
involved using the spin echo sequence to scan the plane parallel to
the anterior and posterior joint line to obtain a
diffusion-weighted imaging.
DTI data pre-treatment involved conversion of the
original DICOM format images to analyze the format by DTI Studio
(Pittsburgh, PA, USA). The b0 and fractional anisotropy (FA)
parameters were also obtained. T-weighted images were normalized to
the Montreal Neurological Institute (MNI) anatomical coordinates
using the SPM5 (statistical parametric mapping) software
implemented in the MATLAB 7.1 platform (MathWorks, Inc., Natick,
MA, USA). Subsequently, the package was used to distribute each
subject's b0 image to the T. A standard templte was constructed by
MNI, and transformation parameters were applied to the FA images
corresponding to each subject, thus standardizing the space of each
subject's FA image. The 12-mm full width at the half maximum of
Gaussian kernel was used to spatially smoothen each FA image after
the standardization to increase the ratio of signal to noise, and
have the data distribution align with the Gaussian
distribution.
Indicators
The PANSS and Global Assessment Scale (GAS) were
used to assess the clinical symptoms and determine the severity of
the disease in each patient. At the same time, MRI and FA images
were used to evaluate white matter functional connections between
brain regions to identify any abnormalities, and determine whether
there were correlations between the signs and clinical symptom
types. PANSS included 7 positive scales (scores ranging from 7 to
49), 7 negative scales (scores ranging from 7 to 49), and 16
general psychopathology scales (scores ranging from 16 to 112). GAS
scores ranged from 1 to 100, and lower scores indicated severity of
the disease.
Statistical analysis
SPSS 19.0 software (SPSS, Inc., Chicago, IL, USA)
was used for the statistical analysis of the data obtained.
Quantitative data were presented as mean ± standard deviation, and
the independent sample t-test was applied for comparison between
groups. Qualitative data were expressed as cases and percentages,
and the χ2 test was used for comparisons of groups. The
Pearson correlation analysis was used to determine whether the data
conformed to normal distribution. P<0.05 was considered to
indicate a statistically significant difference.
Results
Routine MRI findings
MRI images (Fig. 1)
show no significant difference between the observation and control
groups.
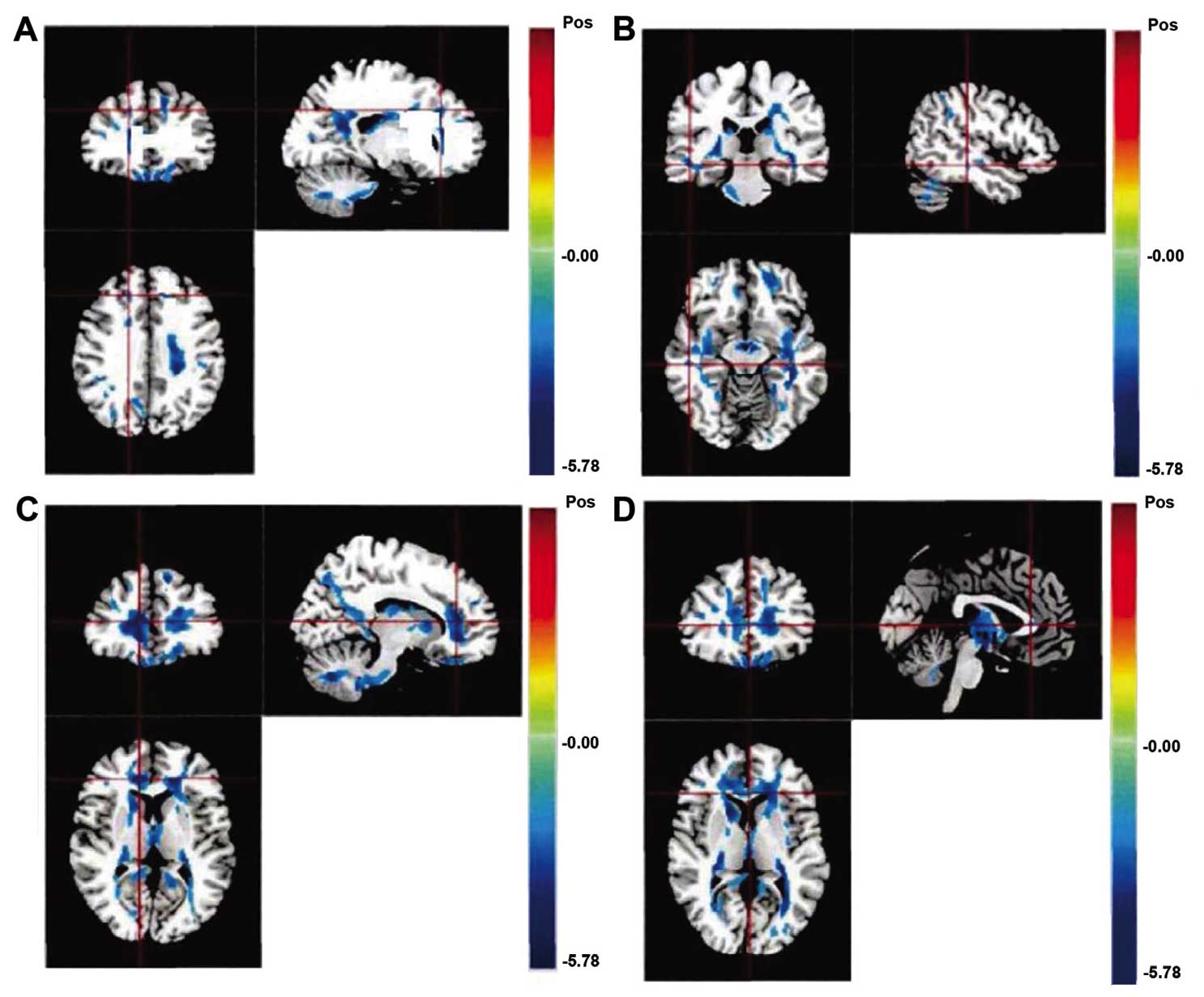
Comparison of FA values in different
brain white matter regions on DTT
Compared with the control group, the FA values in
the observation group shown by DTT were significantly lower in the
left deep prefrontal cortex, the right deep temporal lobe, the
white matter of the inferior frontal gyrus and part of the corpus
callosum (P<0.05; Fig. 2 and
Table I).
 | Table I.Comparison of FA values in different
brain white matter sites on DTT. |
Table I.
Comparison of FA values in different
brain white matter sites on DTT.
|
|
| MNI coordinate |
|
|
|---|
|
|
|
|
|
|
|---|
| Reduction area | Hemisphere | X | Y | Z | Biggest difference in
FA reduction value (t) | P-value |
|---|
| Deep prefrontal
cortex | Left | 13 | 29 | 33 | −4.632 | 0.036 |
|
| Right | −16 | 27 | 30 | 0.329 | 0.953 |
| Deep temporal
lobe | Left | −55 | −7 | −3 | 0.525 | 0.427 |
|
| Right | −46 | −5 | −2 | −4.957 | 0.034 |
| Inferior gyrus
frontalis |
| 10 | 35 | 8 | −5.302 | 0.031 |
| Part of corpus
callosum |
| −2 | 26 | 4 | −5.618 | 0.028 |
Evaluation of PANSS and GAS
The average positive scale score of PANSS in the
observation group was 7.7±1.5, while the average negative scale
score was 46.6±5.9; with the general psychopathology scale average
score being 65.4±10.3. The GAS average score was 53.8±19.2.
According to the results of the Pearson correlation analysis, the
FA values of the deep left prefrontal cortex, the deep right
temporal lobe, the white matter of the inferior frontal gyrus and
part of the corpus callosum had a negative correlation with the
negative symptoms scales (r=0.432, P=0.041; r=0.475, P=0.039;
r=0.512, P=0.037; r=0.533, P=0.035), and a positive correlation
with GAS (r=0.468, P=0.037; r=0.477, P=0.035; r=0.496, P=0.033;
r=0.503, P=0.031).
Discussion
Positive and negative symptoms are independent of
each other (15). A negative symptom
is a reduction or loss of the normal function, consisting of a
defective function, such as poor thought, bleak emotion, depression
and passive social withdrawal. Negative symptoms can become stable
over time and are associated with poor cognitive development, poor
premorbid state, drug resistance and poor prognosis in the chronic
phases (16). A type of
schizophrenia with predominantly negative symptoms is classified as
a special group of the disease. The analysis of the type of brain
connections in cases presenting negative symptoms can reduce the
heterogeneity effect of the sample on the study results, and can be
useful in elucidating clearly the function of the abnormal brain
connections in the pathogenesis of schizophrenia (16). Assuming that FA can reflect the nerve
fiber connectivity of the white matter in the brain, the reduction
of FA represents damage of regional cerebral white matter integrity
and the reduction of nerve fiber connectivity. Previous findings
have shown that the patients with schizophrenia mainly have
structural abnormalities of the middle frontal lobe (complex of
hippocampus-amygdala and entorhinal cortex), the superior frontal
gyrus, the hippocampal sulcus, the corpus callosum, the frontal
lobe and the cingulate gyrus (17).
DTI can demonstrate the shape of white matter
tracts, allowing for observation of the structural characteristic
of the brain's white matter, and revealing microchanges in the
brain white matter nerve fiber tracts of schizophrenics, providing
evidence for a possible neuropathological basis. FA is an important
expression parameter of DTI, as it refers to the proportion of
anisotropic water molecules in the whole diffusion tensor, and is
able to reflect the diffusion anisotropy of water molecules and
reveal the ordering of the tissue microstructures (18). Its size is correlated with the
integrity of the myelin sheath, fiber compactness, and parallelism.
Compared with relative anisotropic values and volume ratio values,
FA values are characterized by less variability and higher imaging
signal to noise ratio (19). DTT is
the only non-invasive imaging method to display brain white matter
fiber tracts on the living body; however, it lacks a golden
standard to test its reliability. Tractography is divided into two
methods: One involves line propagation techniques, and the other
energy minimization techniques. The present study utilized the
former technique, where seed and tracking conditions for the
termination of the fiber bundle were established, and computers
automatically displayed marked 3D fiber bundles, as previously
described by Chung et al (20). The reliability of DTT results are
influenced by image acquisition quality, applied algorithms,
control parameters, ROI location and proficiency of relevant
anatomical knowledge by the operator (21).
Among the brain structures identified as defective
in the study, the corpus callosum is the largest commissural fiber
that bears the function of information transfer and integration
between the two cerebral hemispheres, including organizing hand
movement and unifying emotion. Furthermore, it is associated with
memory retrieval function, attention and wake-up states, and speech
and hearing functions. It is an integral part of the active state
of a person (22). It is generally
considered that the left hemisphere of the brain is responsible for
abstract thinking while the right one is responsible for imagery
thinking (23). However, only by
integrating abstract and imagery thinking constantly by means of
connections can a person maintain a normal mode of thinking. When
this connection is insufficient, abstract thinking and imagery
thinking become fragmented, and thus abnormal thinking may occur
(24).
In conclusion, the reduction of the FA values in the
left deep prefrontal cortex, right deep temporal lobe, white matter
of the inferior frontal gyrus and part of the corpus callosum may
be associated with the pathogenesis of schizophrenia with typical
first negative symptoms. Thus, the application of MRI DTI-FT is
potentially valuable in improving diagnostic accuracy.
Acknowledgements
This study was supported by the Hospital-level
issues, Zhejiang Tongde Hospital (Hangzhou, China), item no.
2012018.
References
|
1
|
No authors listed: Where next with
psychiatric illness? Nature. 336:95–96. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Insel TR: Rethinking schizophrenia.
Nature. 468:187–193. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hegarty JD, Baldessarini RJ, Tohen M,
Waternaux C and Oepen G: One hundred years of schizophrenia: A
meta-analysis of the outcome literature. Am J Psychiatry.
151:1409–1416. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
White T, Magnotta VA, Bockholt HJ,
Williams S, Wallace S, Ehrlich S, Mueller BA, Ho BC, Jung RE, Clark
VP, et al: Global white matter abnormalities in schizophrenia: A
multisite diffusion tensor imaging study. Schizophr Bull.
37:222–232. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Miyata J, Sasamoto A, Koelkebeck K, Hirao
K, Ueda K, Kawada R, Fujimoto S, Tanaka Y, Kubota M, Fukuyama H, et
al: Abnormal asymmetry of white matter integrity in schizophrenia
revealed by voxelwise diffusion tensor imaging. Hum Brain Mapp.
33:1741–1749. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Skelly LR, Calhoun V, Meda SA, Kim J,
Mathalon DH and Pearlson GD: Diffusion tensor imaging in
schizophrenia: Relationship to symptoms. Schizophr Res. 98:157–162.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ayesa-Arriola R, Rodríguez-Sánchez JM,
Suero ES, Reeves LE, Tabarés-Seisdedos R and Crespo-Facorro B:
Diagnosis and neurocognitive profiles in first-episode
non-affective psychosis patients. Eur Arch Psychiatry Clin
Neurosci. 1:123–125. 2016.
|
|
8
|
Zhang XY, Fan FM, Chen DC, Tan YL, Tan SP,
Hu K, Salas R, Kosten TR, Zunta-Soares G and Soares JC: Extensive
white matter abnormalities and clinical symptoms in drug-naive
patients with first-episode schizophrenia: a voxel-based diffusion
tensor imaging study. J Clin Psychiatry. 77:205–211. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mamata H, Mamata Y, Westin CF, Shenton ME,
Kikinis R, Jolesz FA and Maier SE: High-resolution line scan
diffusion tensor MR imaging of white matter fiber tract anatomy.
AJNR Am J Neuroradiol. 23:67–75. 2002.PubMed/NCBI
|
|
10
|
Pettersson-Yeo W, Allen P, Benetti S,
McGuire P and Mechelli A: Dysconnectivity in schizophrenia: Where
are we now? Neurosci Biobehav Rev. 35:1110–1124. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Salmela MB, Cauley KA, Nickerson JP, Koski
CJ and Filippi CG: Magnetic resonance diffusion tensor imaging
(MRDTI) and tractography in children with septo-optic dysplasia.
Pediatr Radiol. 40:708–713. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ellison-Wright I and Bullmore E:
Meta-analysis of diffusion tensor imaging studies in schizophrenia.
Schizophr Res. 108:3–10. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wolkin A, Choi SJ, Szilagyi S, Sanfilipo
M, Rotrosen JP and Lim KO: Inferior frontal white matter anisotropy
and negative symptoms of schizophrenia: A diffusion tensor imaging
study. Am J Psychiatry. 160:572–574. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Rabe-Jablonska J: [Affective disorders in
the fourth edition of the classification of mental disorders
prepared by the American Psychiatric Association - diagnostic and
statistical manual of mental disorders]. Psychiatr Pol. 27:269–279.
1993.PubMed/NCBI
|
|
15
|
Strauss GP, Vertinski M, Vogel SJ,
Ringdahl EN and Allen DN: Negative symptoms in bipolar disorder and
schizophrenia: A psychometric evaluation of the brief negative
symptom scale across diagnostic categories. Schizophr Res.
170:285–289. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Siegrist K, Millier A, Amri I, Aballéa S
and Toumi M: Association between social contact frequency and
negative symptoms, psychosocial functioning and quality of life in
patients with schizophrenia. Psychiatry Res. 230:860–866. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wu CH, Hwang TJ, Chen YJ, Hsu YC, Lo YC,
Liu CM, Hwu HG, Liu CC, Hsieh MH, Chien YL, et al: Primary and
secondary alterations of white matter connectivity in
schizophrenia: A study on first-episode and chronic patients using
whole-brain tractography-based analysis. Schizophr Res. 169:54–61.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Meoded A, Faria AV, Hartman AL, Jallo GI,
Mori S, Johnston MV, Huisman TA and Poretti A: Cerebral
Reorganization after Hemispherectomy: A DTI Study. AJNR Am J
Neuroradiol. 14:12–14. 2016.
|
|
19
|
Lei W, Li N, Deng W, Li M, Huang C, Ma X,
Wang Q, Guo W, Li Y, Jiang L, et al: White matter alterations in
first episode treatment-naïve patients with deficit schizophrenia:
A combined VBM and DTI study. Sci Rep. 5:129942015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Chung MK, Adluru N, Lee JE, Lazar M,
Lainhart JE and Alexander AL: Cosine series representation of 3D
curves and its application to white matter fiber bundles in
diffusion tensor imaging. Stat Interface. 3:69–80. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Chung MK, Adluru N, Lee JE, Lazar M,
Lainhart JE and Alexander AL: Efficient parametric encoding scheme
for white matter fiber bundles. Conf Proc IEEE Eng Med Biol Soc.
2009:6644–6647. 2009.PubMed/NCBI
|
|
22
|
Del Re EC, Konishi J, Bouix S, Blokland
GA, Mesholam-Gately RI, Goldstein J, Kubicki M, Wojcik J, Pasternak
O, Seidman LJ, et al: Enlarged lateral ventricles inversely
correlate with reduced corpus callosum central volume in first
episode schizophrenia: Association with functional measures. Brain
Imaging Behav. 17:156–158. 2015.
|
|
23
|
Whitehouse PJ: Imagery and verbal encoding
in left and right hemisphere damaged patients. Brain Lang.
14:315–332. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Rigucci S, Santi G, Corigliano V, Imola A,
Rossi-Espagnet C, Mancinelli I, De Pisa E, Manfredi G, Bozzao A,
Carducci F, et al: White matter microstructure in ultra-high risk
and first episode schizophrenia: A prospective study. Psychiatry
Res. 247:42–48. 2016. View Article : Google Scholar : PubMed/NCBI
|