Introduction
Multiple simultaneous intracerebral hemorrhages
(MSIH) is rare phenomenon, accounting for ~3% of all intracranial
hemorrhage events (1). MSIH remains
intriguing regarding the causes and MMD can be caused by a variety
of factors, including hypertension, cerebral vasculitis,
sympathetic nerve stimulants, drugs that affect blood coagulation,
brain tumors, cerebral amyloidosis, venous sinus thrombosis and
coagulation disorders, in addition to other unexplained factors
(2,3). The treatment for MSIH mainly consists
of releasing the intracranial pressure caused by the hematoma,
identifying the cause of the original hemorrhage and then providing
surgical treatment (4). Although
there are numerous studies describing MSIH in the literature, MSIH
of Moyamoya disease (MMD) is rare. Kikuta et al (5) in 2008 reported a series of multiple
intracerebral hemorrhages of MMD, but these hemorrhages were
limited to multiple trace bleeding. However, to the best of our
knowledge, no case of severe MSIH caused by MMD has been reported
to date. MMD is an uncommon disease characterized by progressive
occlusion of the terminal portion of the internal carotid artery
and its main branches within the circle of Willis. This occlusion
results in the formation of a fine vascular network at the base of
the brain. These MMD vessles are fragile and easy to rupture
(6); therefore, MSIH in MMD is
possible. Intracranial hemorrhage in MMD is not easy to treat
(7), so MSIH would be more difficult
to treat.
The present study reports a rare case of severe MSIH
caused by MMD, which was treated with hematoma evacuation and
decompressive craniectomy, resulting in good recovery. In addition
to the case report, the mechanism of MMD-induced MSIH is also
discussed.
Case report
Written informed consent was obtained from the
patient. A 40-year-old female patient with no history of
hypertension and diabetes mellitus was admitted the First Hospital
of Jilin University (Changchun, China) in June 2015 due to
presentation of sudden severe headache and vomiting followed by
gradual coma for 2 h. Physical examinations revealed stable vital
signs with a blood pressure of 140/90 mmHg, and the neurological
examination showed minor coma (Glasgow Coma Scale score, 11)
(8), right hemiplegia, degree 3
muscle strength, positive Babinski sign, and stiffness in the neck
with Kernig's sign (9). Laboratory
tests indicated normal blood coagulation and platelet counts.
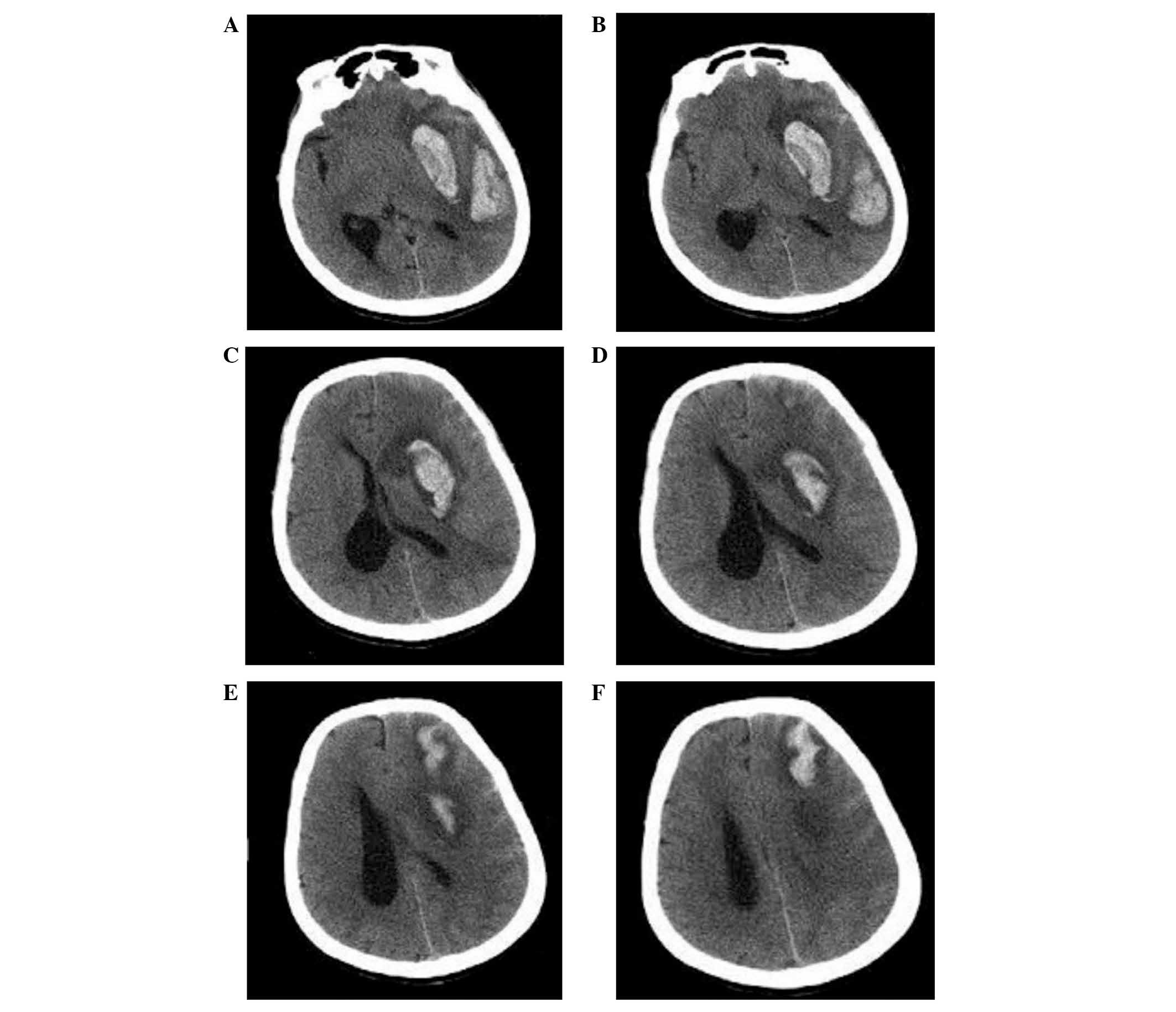
Cranial computed tomography (CT) revealed multiple irregular high
density zones in the left basal ganglia, posterior temporal lobe
and frontal lobe, with mild peripheral edema. The left ventricle
showed deformation under compression, with the midline shifted to
the right (Fig. 1). Cranial CT
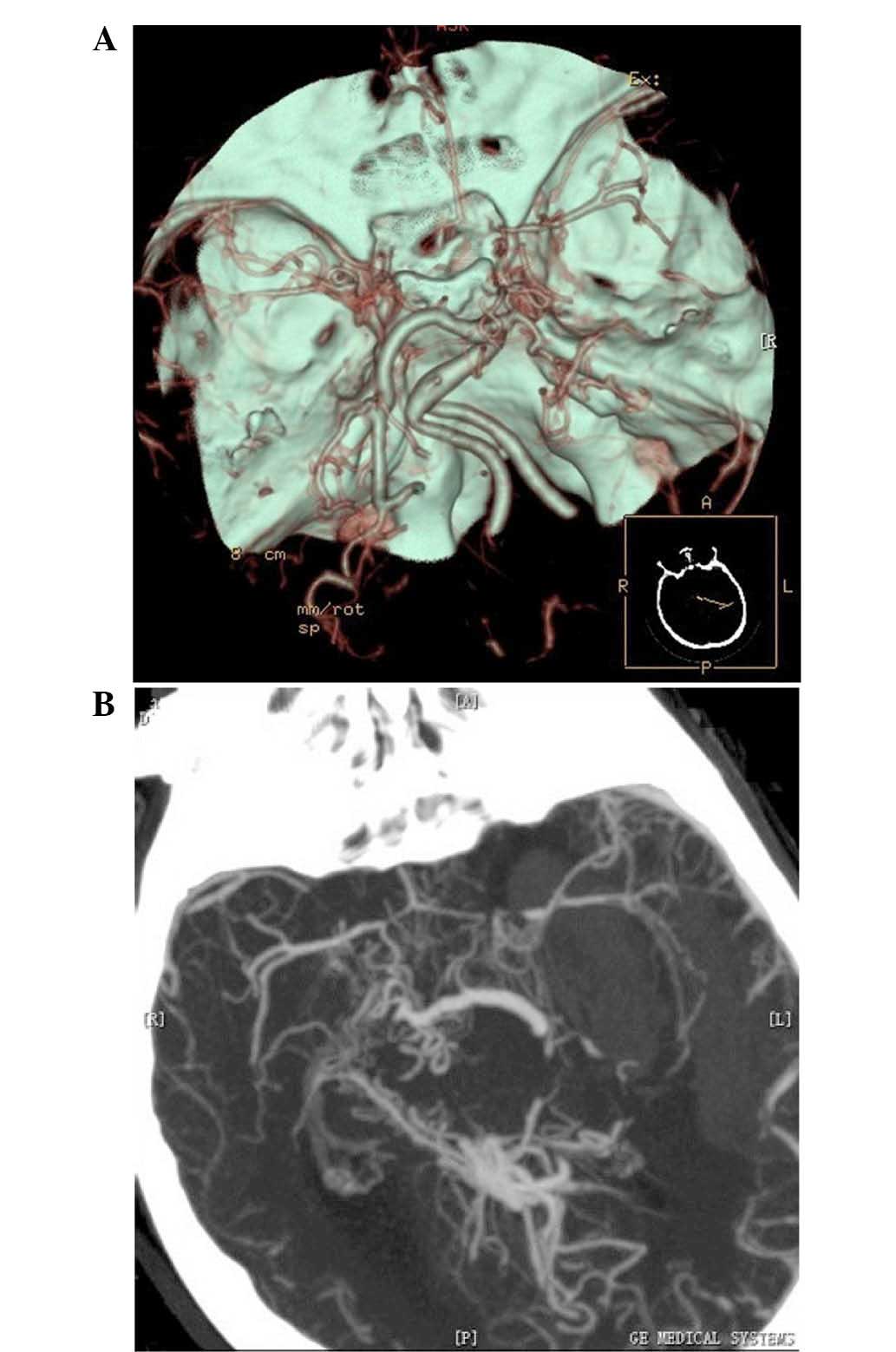
angiography (CTA) subsequent to admission demonstrated that the
normal vascular morphology in the area of the bilateral middle
cerebral artery was disrupted, with visible hematomas in the
maximum intensity projection axis (Fig.
2). Based on the symptoms and the radiographic examination
findings, a clear diagnosis of MMD and intracerebral MSIH was
established.
An emergency hematoma evacuation and decompressive
craniectomy was scheduled. To further clarify the circumstances of
the intracranial arteries, preoperative digital subtraction
angiography (DSA) was performed under general anesthesia in the
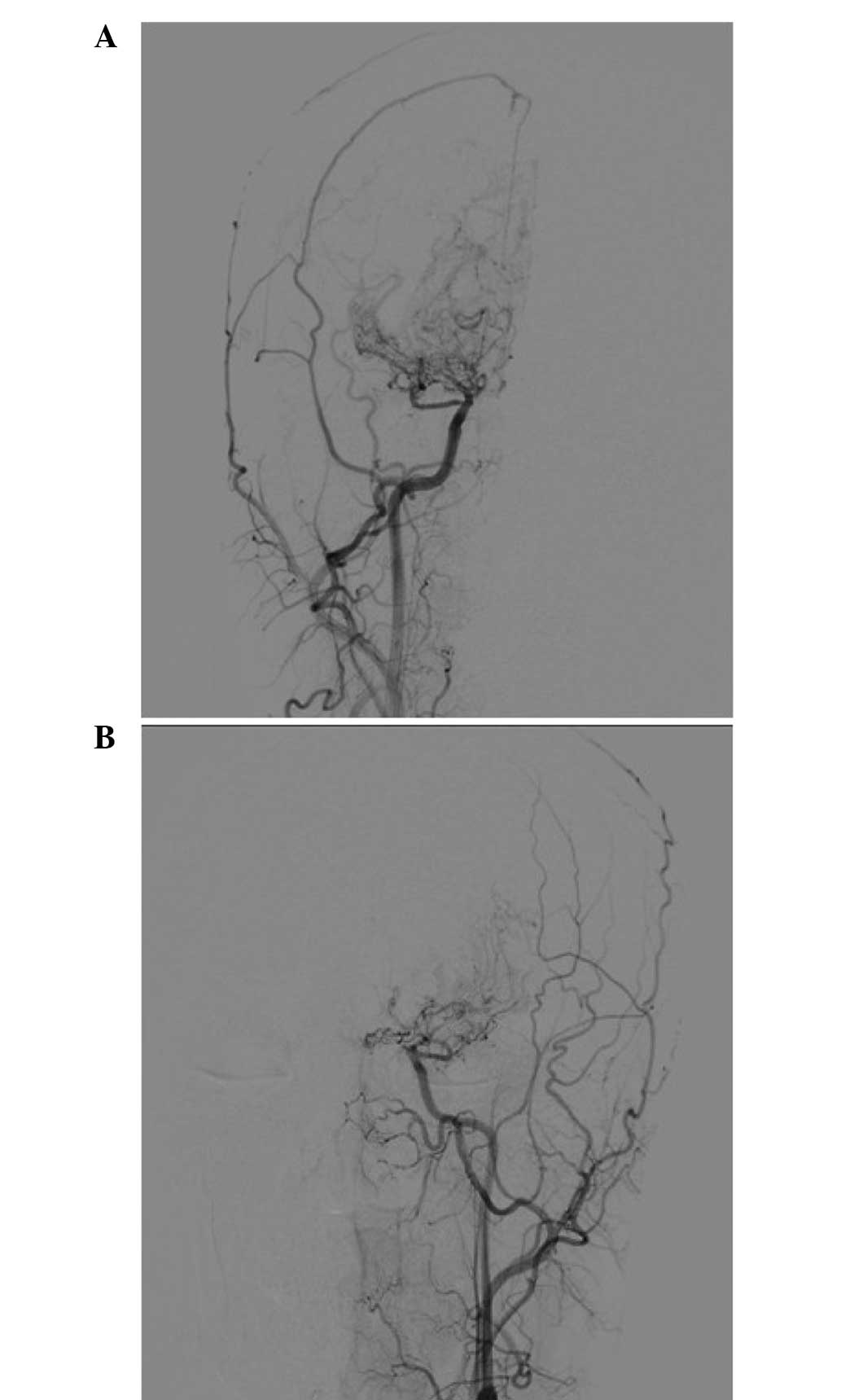
catheterization room. The DSA results showed occlusions at the ends
of the bilateral carotid arteries, which were replaced with
‘smoke-like’ blood vessels (Fig. 3).
With the exception of these smoke-like blood vessels, no aneurysms
or vascular malformations were observed in the areas of the left
middle cerebral artery or anterior artery areas (Fig. 3). Hematoma evacuation and
decompressive craniectomy were performed under general anesthesia
in order to remove the majority of the hematoma in the left basal
ganglia and posterior temporal lobe; however, the hemorrhage in the
left frontal lobe was not treated as it was risky and unnecessary.
Following hematoma evacuation, the temporal muscle was attached to
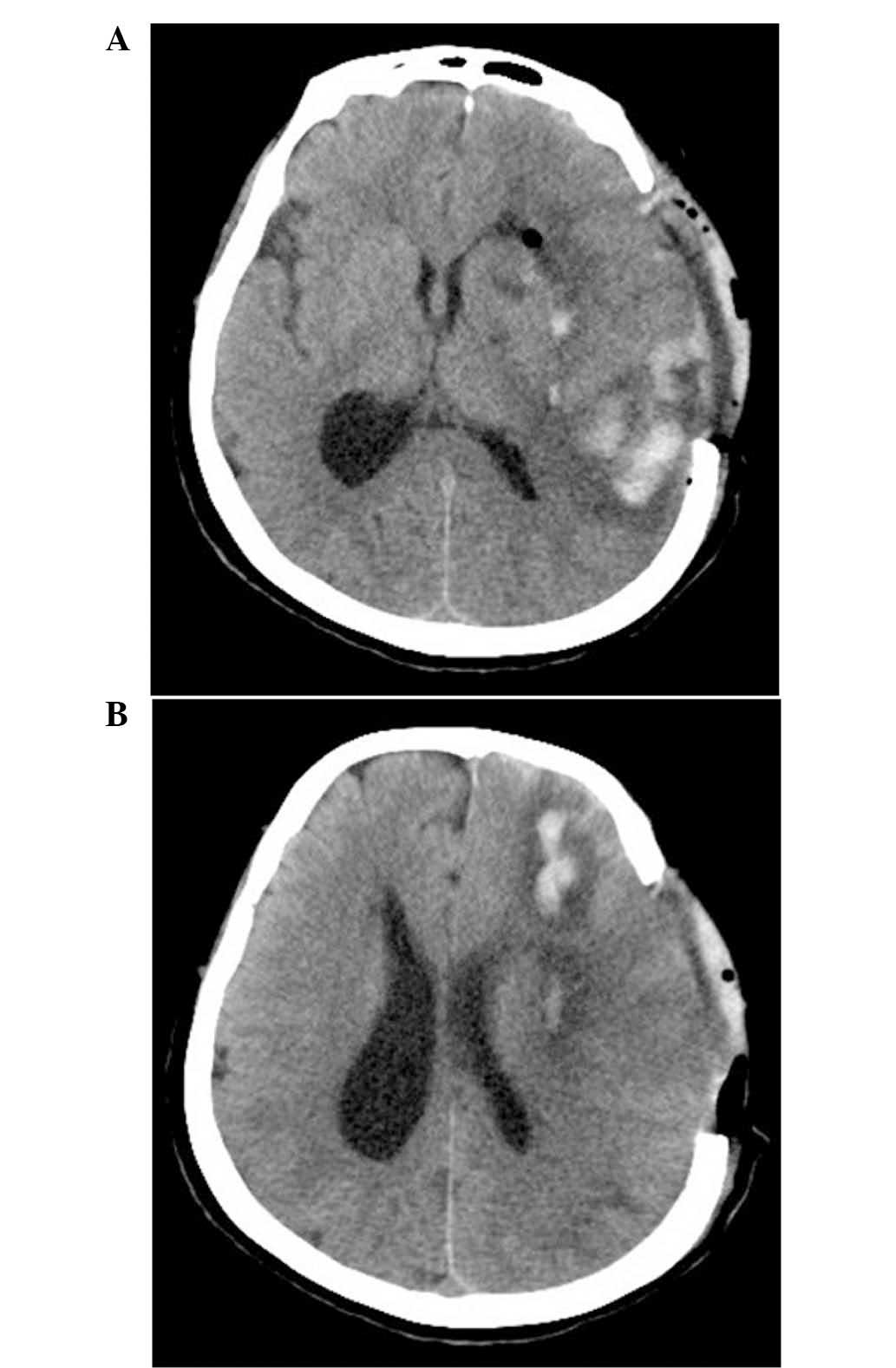
the brain surface for fusion. A postoperative CT scan revealed that
the majority of the intracranial hematoma was removed and that the
ventricular size had returned to normal, with the midline in the
center (Fig. 4). Postoperative
nutritional support, including Nutrison Fibre (80 ml/h
intranasally; Nutrica Pharmaceutical Co., Ltd., Wuxi, China) and
trimebutine maleate (400 mg once every three days; Tanabe
Pharmaceutical Co., Ltd., Tianjin, China), and symptomatic
treatment were provided for 1 week, and the patient gradually
regained consciousness, with motor aphasia, low pressure in the
left decompression window, right hemiplegia and degree 3 muscle
strength. Over the 3-month follow-up period the patient was
aphasic, with degree 4 muscle strength in her right limb, and
essentially self-sufficient in her daily life. In June 2016, the
patient's symptoms persisted but no hemorrhage had reoccurred, and
the patient's quality of life was good.
Discussion
Intracerebral hematoma commonly occurs at a single
site, although multiple hemorrhages at different sites with long
intervals may also occur. By contrast, the incidence of MSIH is
very rare. In 2010, Stemer et al (10) conducted a study including 522 cases
of spontaneous intracerebral hemorrhage, of which 29 were MSIH
patients, yielding an incidence rate for MSIH of 5.6%. MSIH is
defined, based on imaging examination, as multiple hemorrhages or
hemorrhages at different sites occurring within 24 h, including
secondary hemorrhages with clear causes and an unexplained primary
hemorrhage (10). The incidence of
simple primary MSIH was estimated to be between 0.75 and 3.0%,
which is lower compared with the overall incidence of MSIH
(10). However, the study by Stemer
and colleagues did not include MMD cases, possibly due to the
majority of MMD-induced MSIH cases not being clearly identified and
classified as primary MSIH. Indeed, only a limited number of
MMD-induced multiple intracerebral hemorrhage cases were available
in the literature. In 2014, Laiwattana et al (3) reviewed the MSIH literature published
during the 60-year period between 1953 and 2013, and their results
were consistent with the MSIH incidence rate reported by Stemer
et al (10). In addition, the
authors reviewed the literature in order to analyze the causes of
secondary MSIH, although MMD was not considered as a cause of
secondary MSIH in their review (3).
In the present study, a case of MSIH caused by MMD was described,
aiming to bring clinical attention to the fact that MMD can lead to
MSIH, thereby enriching the available clinical data of MSIH.
In addition to unexplained primary factors, numerous
secondary factors can cause MSIH, including arterial diseases,
venous drainage obstruction, parenchymal diseases (such as brain
tumors and cavernous hemangioma), drug use and hematologic diseases
(4,11,12).
However, the most common causes are arterial diseases, such as
hypertension, atherosclerosis, vasculitis and cerebral amyloidosis.
In 2005, Yen et al (13)
reported 1,306 cases of hypertensive intracerebral hemorrhage,
including 10 cases of MSIH, with an incidence rate of ~0.8%. MSIH
caused by hypertension or by vasculitis has been reported in
several other studies. For instance, in the study by McCormick and
Rosenfield (2) published in 1973, 2
cases of MSIH were clearly caused by vasculitis among 144 cases of
cerebral hemorrhage (2). In
addition, cerebral amyloidosis may cause MSIH; for example, in
1984, Gilles et al (14)
reported 11 cases of MSIH that were directly caused by cerebral
amyloidosis. MSIH caused by arterial disease most likely occurs due
to multiple ruptures in the diseased vessels, induced by
hypertension from the original arterial disease. Alternatively,
ruptures and hemorrhages in a diseased cerebral vessel may lead to
a transient increase in blood pressure, thereby inducing
hemorrhages at other sites in the brain, resulting in MSIH
(15,16).
MMD is an arterial brain disease that is
characterized by occlusions at the end of the intracranial and
carotid arteries. Normal blood vessels disappear and are replaced
by ‘smoke-like’ blood vessel hyperplasia, mainly from expanded and
distorted lenticulostriate and thalamoperforate arteries (17). In these abnormal small arteries,
internal elastic layer fracture, medial fibrosis and local
expansion to form small aneurysms may occur (18,19).
Theoretically, these small diseased arteries are able to cause MSIH
through hypertension, or through hemorrhage at one site that can
lead to a transient increase in blood pressure and induce
hemorrhages at other sites. However, MSIH caused by MMD has been
rarely reported, and the few published studies were limited to
multiple trace bleeding (20). For
instance, the study of Kikuta et al (5) in 2008 investigated 50 cases of MMD
using 3T magnetic resonance imaging (MRI), and identified 11 cases
of multiple trace bleeding, which were caused due to small diseased
arteries. This situation is also a risk factor for future severe
cerebral hemorrhage. By contrast, MMD-induced MSIH has not been
previously described, and was first reported in the present study.
The cranial CT performed in the present study demonstrated no
intracranial malacia, which may occasionally form subsequent to
hemorrhage. One of the pathological changes caused by MMD is that
certain small arteries become fragible, which manifests as internal
elastic layer fracture and medial fibrosis. The rupturing and
hemorrhaging of a diseased cerebral vessel may lead to a secondary
transient increase in blood pressure, thereby inducing hemorrhages
at other sites in the brain and resulting in MSIH.
Following MSIH, the underlying cause must be
identified in order to develop an effective treatment plan. The
causes of MSIH include arterial diseases, clogging of venous
drainage, parenchymal diseases, drug use and hematologic diseases
(3). Therefore, specific
examinations can be performed, including the following: CTA, MRA or
DSA to examine the arteries; CTV, MRV, or DSA to examine the
intracranial veins; CT and MRI for brain parenchymal lesions; and
routine blood tests for determination of platelet count, platelet
function, coagulation function and blood cell sedimentation rate,
in order to identify hematologic diseases (4). In addition, the medical history of the
patient, including hypertension, diabetes and drug use involving
sympathetic stimulants and anticoagulants, is also important.
However, MMD diagnoses are primarily dependent on imaging studies.
For patients with acute cerebral hemorrhage, CTA is a rapid and
effective method to correctly diagnose MMD (21,22),
although examination by DSA may provide more accurate results. The
case reported in the present study was accurately diagnosed as MMD
and MSIH by CTA following the onset, while laboratory tests ruled
out hematologic diseases.
The treatment of MSIH depends on the volume and
location of the hematoma. However, treatment differs from that for
single intracranial hemorrhage, primarily because multiple
hemorrhages can be scattered, and not all multiple hemorrhages can
be removed at the same time. For instance, in the current study,
only the hematomas in the left basal ganglia and the posterior
temporal lobe were removed, while the hemorrhage in the frontal
lobe was not treated as it was risky and unnecessary, although
simultaneous decompressive craniectomy was performed. The efficacy
of MSIH treatment was not better over that for a single hemorrhage
(23). The study by Laiwattana et
al (3) reported that the
prognosis for MSIH was poor, particularly for cases involving the
bilateral thalamus. The case reported in the current study involved
only the hemisphere on the left side of the meninges. Compared with
MSIH cases involving both hemispheres, the efficacy following
active treatment was relatively satisfactory in the current
case.
Therefore, considering the present report of
MMD-induced MSIH, we suggest that the possibility of MMD should be
considered when an MSIH case is identified. In clinical practice,
MMD can be accurately diagnosed using CTA and may lead to
pathological changes in small arteries, causing them to become
fragible. Rupture and hemorrhage occurring at one site may induce a
transient increase in blood pressure, causing the rupture of small
arteries at other sites, and thus leading to MSIH. Subsequent to
ruling out disorders of the blood and blood coagulation, hematoma
evacuation and decompression should be performed in selective
cases, which can lead to good prognosis.
In conclusion, MSIH caused by MMD is extremely rare;
microbleedings are typical of MSIH, and severe MSIH rarely occurs.
The cause of severe MSIH may be a result of transient hypertension
following a hemorrhage, and the hypertension can result in
simultaneous hemorrhages in other locations. In the present study,
the treatment of MSIH was difficult, primarily because hemotomas
were scattered and damaged numerous functional regions of the
brain. Timely decompressive surgery and hemotoma removal is vital
in the treatment of MSIH.
References
|
1
|
Hayashi K, Morofuji Y, Horie N and Izumo
T: A case of neurofibromatosis type 1 complicated with repeated
intracerebral hemorrhage due to quasi-moyamoya disease. J Stroke
Cerebrovasc Dis. 24:e109–e113. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
McCormick WF and Rosenfield DB: Massive
brain hemorrhage: A review of 144 cases and an examination of their
causes. Stroke. 4:946–954. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Laiwattana D, Sangsawang B and Sangsawang
N: Primary multiple simultaneous intracerebral hemorrhages between
1950 and 2013: Analysis of data on age, sex and outcome.
Cerebrovasc Dis Extra. 4:102–114. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Finelli PF: A diagnostic approach to
multiple simultaneous intracerebral hemorrhages. Neurocrit Care.
4:267–271. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kikuta K, Takagi Y, Nozaki K, Sawamoto N,
Fukuyama H and Hashimoto N: The presence of multiple microbleeds as
a predictor of subsequent cerebral hemorrhage in patients with
moyamoya disease. Neurosurgery. 62:104–111; discussion 111–122.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kim T, Oh CW, Bang JS, Kim JE and Cho WS:
Moyamoya disease: Treatment and outcomes. J Stroke. 18:21–30. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kim JS: Moyamoya disease: Epidemiology,
clinical features, and aiagnosis. J Stroke. 18:2–11. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Balestreri M, Czosnyka M, Chatfield DA,
Steiner LA, Schmidt EA, Smielewski P, Matta B and Pickard JD:
Predictive value of Glasgow Coma Scale after brain trauma: Change
in trend over the past ten years. J Neurol Neurosurg Psychiatry.
75:161–162. 2004.PubMed/NCBI
|
|
9
|
Seeder L: Muscle strength grading. Ann
Emerg Med. 12:4071983. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Stemer A, Ouyang B, Lee VH and Prabhakaran
S: Prevalence and risk factors for multiple simultaneous
intracerebral hemorrhages. Cerebrovasc Dis. 30:302–307. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Chanda A and Nanda A: Multiple cavernomas
of brain presenting with simultaneous hemorrhage in two lesions: A
case report. Surg Neurol. 57:340–344; discussion 334–335. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kidd D, Plant GT, Scaravilli F, McCartney
AC, Stanford M and Graham EM: Metastatic choriocarcinoma presenting
as multiple intracerebral haemorrhages: The role of imaging in the
elucidation of the pathology. J Neurol Neurosurg Psychiatry.
65:939–941. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yen CP, Lin CL, Kwan AL, Lieu AS, Hwang
SL, Lin CN and Howng SL: Simultaneous multiple hypertensive
intracerebral haemorrhages. Acta Neurochir (Wien). 147:393–399;
discussion 399. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Gilles C, Brucher JM, Khoubesserian P and
Vanderhaeghen JJ: Cerebral amyloid angiopathy as a cause of
multiple intracerebral hemorrhages. Neurology. 34:730–735. 1984.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Mauriño J, Saposnik G, Lepera S, Rey RC
and Sica RE: Multiple simultaneous intracerebral hemorrhages:
Clinical features and outcome. Arch Neurol. 58:629–632. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Komiyama M, Yasui T, Tamura K, Nagata Y,
Fu Y and Yagura H: Simultaneous bleeding from multiple
lenticulostriate arteries in hypertensive intracerebral
haemorrhage. Neuroradiology. 37:129–130. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Piao J, Wu W, Yang Z and Yu J: Research
progress of moyamoya disease in children. Int J Med Sci.
12:566–575. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hosoda Y, Ikeda E and Hirose S:
Histopathological studies on spontaneous occlusion of the circle of
Willis (cerebrovascular moyamoya disease). Clin Neurol Neurosurg.
99(Suppl 2): S203–S208. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Zhang L, Xu K, Zhang Y, Wang X and Yu J:
Treatment strategies for aneurysms associated with moyamoya
disease. Int J Med Sci. 12:234–242. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ryan RW, Chowdhary A and Britz GW:
Hemorrhage and risk of further hemorrhagic strokes following
cerebral revascularization in Moyamoya disease: A review of the
literature. Surg Neurol Int. 3:722012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Sugino T, Mikami T, Ohtaki S, Hirano T,
Iihoshi S, Houkin K and Mikuni N: Assessment of moyamoya disease
using multidetector row computed tomography. J Stroke Cerebrovasc
Dis. 22:644–649. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zhang J, Wang J, Geng D, Li Y, Song D and
Gu Y: Whole-brain CT perfusion and CT angiography assessment of
Moyamoya disease before and after surgical revascularization:
Preliminary study with 256-slice CT. PLoS One. 8:e575952013.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Chen Y, Henon H, Bombois S, Pasquier F and
Cordonnier C: Multiple simultaneous spontaneous intracerebral
hemorrhages: A rare entity. Cerebrovasc Dis. 41:74–9. 2016.
View Article : Google Scholar : PubMed/NCBI
|