Introduction
Kawasaki disease (KD), also known as
skin-mucosal-associated lymphoid syndrome (a vasculitis syndrome),
is a rare childhood illness that affects the blood vessels
(1). The disease is most common in
children and can be extremely harmful to infants. Damage may occur
to coronary arteries and to the heart muscle itself (1). Affected children may suffer from
systemic small and middle-sized vascular inflammation which can be
transformed into coronary artery sustainable expansion (2), coronary artery aneurysm and even
death.
The causative factors of Kawasaki disease are
unknown and the disease does not appear to be hereditary or
contagious. Identifying treatment for Kawasaki disease has become
the focus of investigations worldwide (3). Results obtained from prior studies
(4) showed that intravenous
immunoglobulin (IVIG) therapy is effective with regard to the
adverse effects of Kawasaki disease, however the underlying
mechanism remains to be determined. Suzuki et al (5) showed that serum 25-hydroxyvitamin
D3 [25-(OH)D3] in blood ameliorates the
immune system and prevents coronary artery abnormalities. Results
from another related study (6)
suggested that interleukin-6 (IL-6) was correlated with
immunoreaction and had multiple effects such as stimulating and
activating the proliferation of B cell, promoting antibody
secretion, stimulating the proliferation of T cells and CTL
activation (7). IL-6 affects the
expression of acute phase protein in hepatic cells, which are
involved in inflammatory reactions and accelerating cell
development (8).
In the present study, we investigated the
significance of serum 25-(OH)D3 and IL-6 levels prior to
and after immunoglobulin treatment in children suffering from
Kawasaki disease. We aimed to provide some theoretical and
practical references for the successful treatment of Kawasaki
disease in children.
Materials and methods
General materials
From February, 2013 to February, 2015, 45 patients
with Kawasaki disease, including 24 men and 21 women with an
average age of 3.2±3 years, were enrolled in the present study, and
constituted the observation group. The normal control group
comprised 43 healthy volunteers during the same period. The normal
control group comprised 22 men and 21 women with an average age of
2.9±2.7 years. The feverish control group comprised 46 patients (22
men and 24 women), with an average age of 3.1±2.9 years, and had
respiratory infection and fever.
The aims of the study were established in accordance
with relevant diagnostic criteria of Kawasaki disease presented by
Japan KD Research Committee. The present study was approved by the
ethics committee of Xuzhou Children's Hospital. Written informed
consent was obtained from the patients and/or guardians.
Methods
Venous blood (4 ml) was collected from each case
prior to treatment. Samples were centrifuged at 2,000 × g for 5 min
at 4°C and the upper layer of the serum was collected and
transferred into a cryogenic tube (Suzhou Alpha Biotech Co., Ltd,
Suzhou, China) and kept at −80°C (1)
and the content of 25-(OH)D3 and IL-6 were verified.
Antibodies used in this study were purchased from Roche Diagnostics
(Basel, Switzerland), and RNA extraction kits were purchased from
Takara Bio (Dalian, China). Patients were then treated with IVIG
therapy (2 g/kg intravenous drip and oral aspirins, 2–5 days after
the fever subsided). The serum was kept and the content of
25-(OH)D3 and IL-6 was detected.
RT-polymerase chain reaction
(PCR)
RNA extraction
Cryophylactic tissue samples (0.1 g) were extracted
from the liquid nitrogen and melted on ice. Subsequently, 0.45 ml
of RNA Plus was added and the tissues were ground in a precooled
mortar and transferred into a 1.5-ml Eppendorf tube (Hamburg,
Germany). After adding 0.45 ml of RNA Plus in the mortar, the
samples were washed in centrifuge tube and 200 µl chloroform was
then added. The samples were vigorously agitated using a vortex for
15 sec and kept on ice for 15 min. The samples were centrifuged at
8,000 × g for 15 min at 4°C and the upper layer of the serum was
collected in an Eppendorf tube (RNase-treated). Isopropanol
(equivalent) was added to the tube and after mixing it was left on
for 10 min. The samples were centrifuged again at 8,000 × g for 10
min at 4°C and the upper layer of the serum was removed. Then, 750
µl of ethyl alcohol (75%) was added and mixed gently followed by
further centrifugation at 8,000 × g at 4°C for 10 min. The upper
layer of the serum was discarded and residual ethyl alcohol was
removed. The quality of extracted RNA was verified and RNA was
stored to be used in reverse transcription.
Fluorescent quantitative PCR
Fluorescent quantitative PCR kits were carried out
as per the manufacturer's instructions (Takara), with slight
modification (Table I).
 | Table I.Fluorescent quantitative PCR
primers. |
Table I.
Fluorescent quantitative PCR
primers.
| Gene | Primer sequences
(5′-3′) | Fragment length
(bp) |
|---|
|
25-(OH)D3 | F:
CGATCTGCATGACTTCTTCCA | 164 |
|
| R:
GCTAGTACGATCATCATCTAC |
|
| IL-6 | F:
CGTAACGTTAGCGGCAGCTA | 138 |
|
| R:
CGTAGTCCAGGTACTAGCAG |
|
| GAPDH | F:
GAAGGTGAAGGTCGGAGTC | 226 |
|
| R:
GAAGATGGTGATGGGATTTC |
|
Enzyme-linked immunosorbent assay (ELISA)
The standard protocol for the ELISA kit was carried
out, with some improvements (9).
25-(OH)D3 and IL-6 were diluted at a ratio of 1:40 using
the assay buffer and designed the standard curve. Samples were
diluted (1:100) and 80 µl of test solution and 60 µl of detection
solution were added into each well (96-wells). After 1 h incubation
at 25°C, TMB chromogenic substrate was added. The light absorption
value was measured at 495 nm using a microplate reader (Bio-Tek
Instruments Inc., Winooski, VT, USA) and the concentration of
25-(OH)D3 and IL-6 was calculated using the standard
curve.
Western blotting
An animal cell protein extraction kit was used to
extract the total protein [standard protocol carried out with some
improvement (10)].
Statistical analysis
We used SPSS 20.2 software (Chicago, IL, USA) for
statistical analyses. Measurement data were presented as mean ± SD,
and countable data were expressed by the number of cases or the
percentage. Intergroup comparison was carried out using the
χ2 test. P<0.05 indicated the difference was
statistically significant.
Results
25-(OH)D3 and IL-6 levels
in the serum prior to treatment
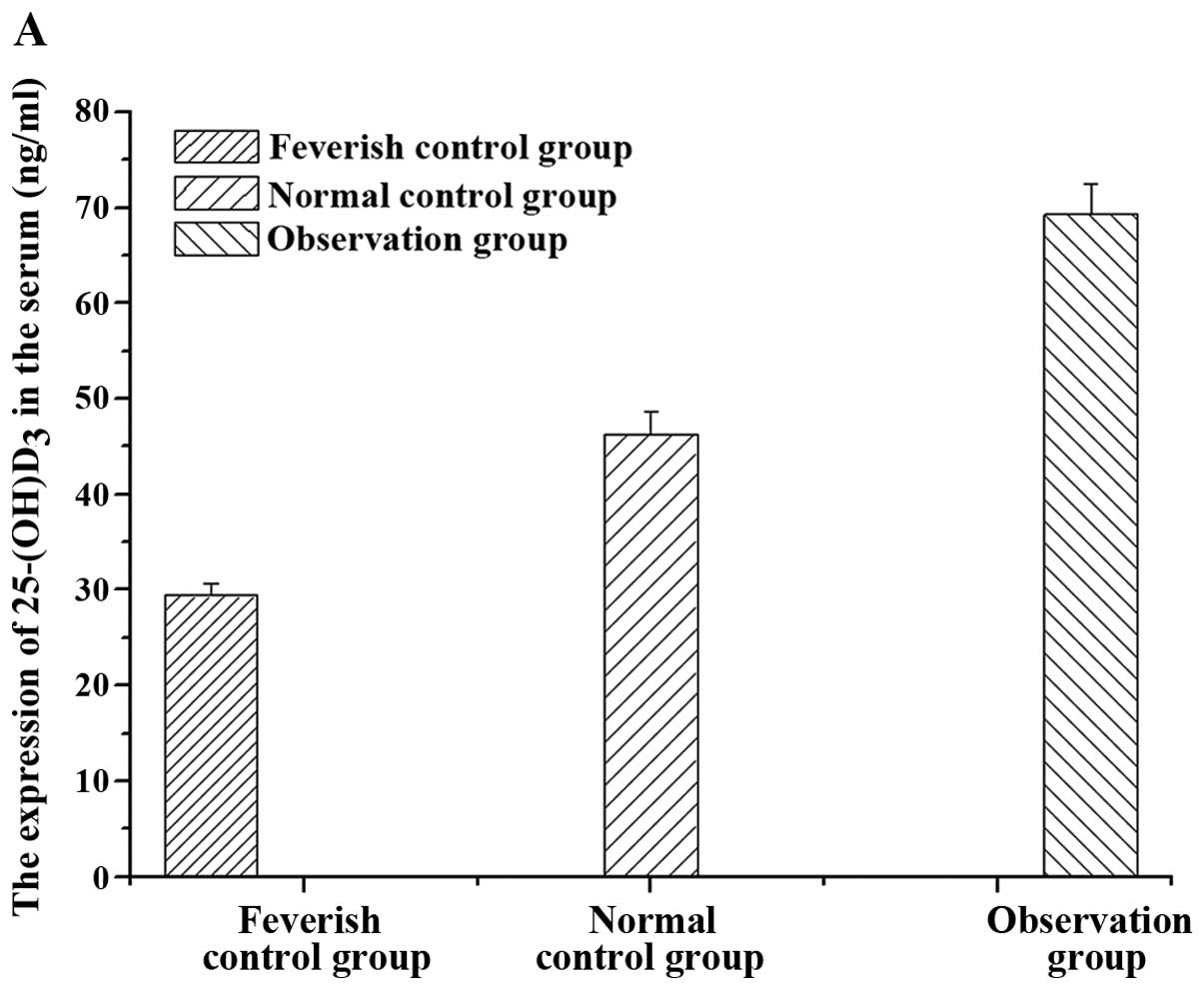
We detected the 25-(OH)D3 and IL-6 levels
in the serum samples collected from the three groups prior to
treatment with immunoglobulin (Fig.
1). The results showed that the content of serum
25-(OH)D3 in the feverish control group was lower than
that of the normal control group. By contrast, the level of serum
25-(OH)D3 in the observation group was higher than that
of the normal control group. The differences were statistically
significant (P<0.05). The level of serum 25-(OH)D3 in
the feverish control group was lower than that of serum IL-6 in the
normal children, but there were no statistically significant
differences (P>0.05). The level of serum 25-(OH)D3 in
the observation group was higher than the content of serum IL-6 in
the normal children, and the difference was statistically
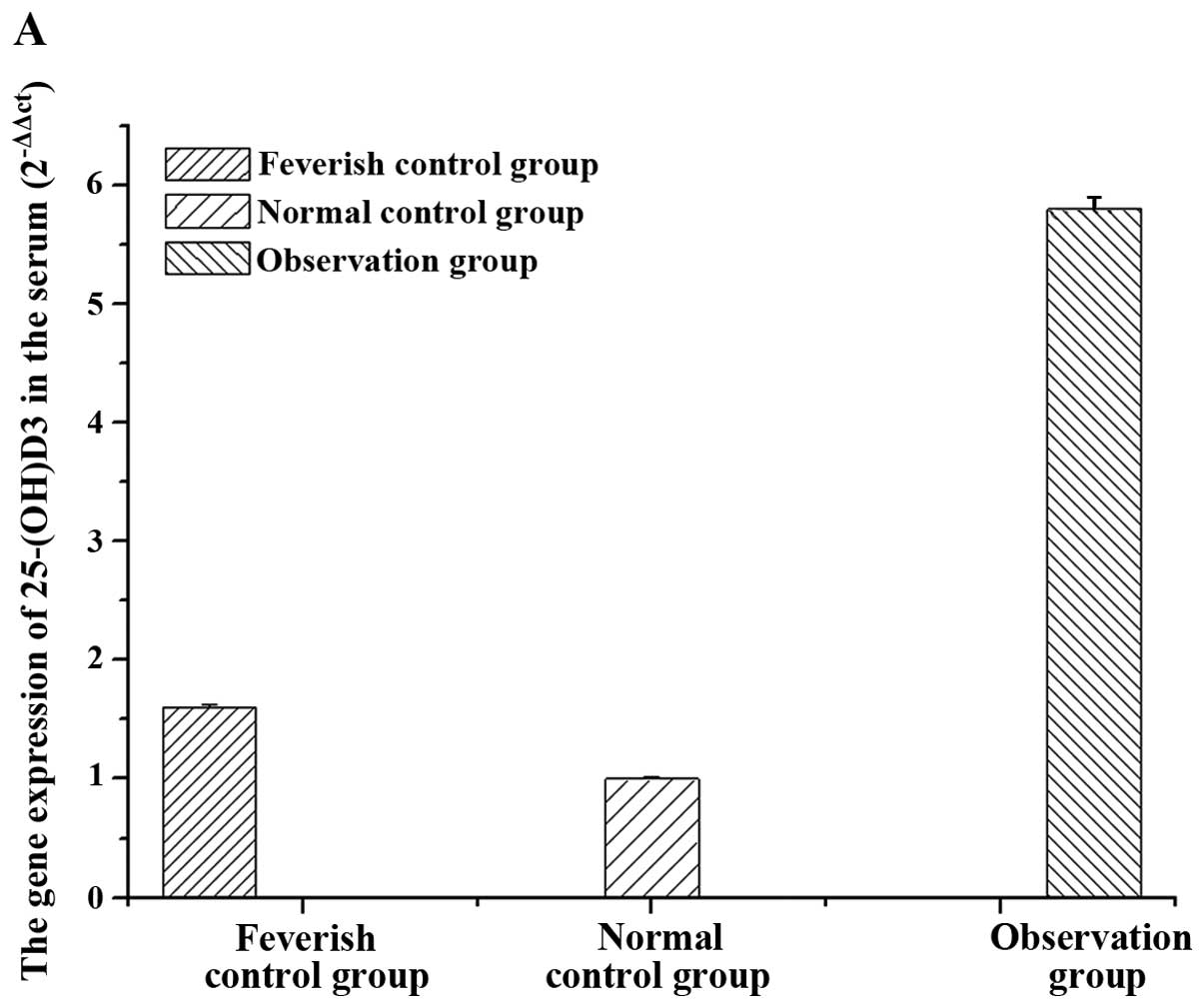
significant (P<0.05). The 25-(OH)D3 and IL-6 gene
expression levels in the three groups prior to treatment with
immunoglobulin showed the same pattern observed in the protein
expression (Fig. 2).
25-(OH)D3 and IL-6 gene
expression levels after immunoglobulin treatment
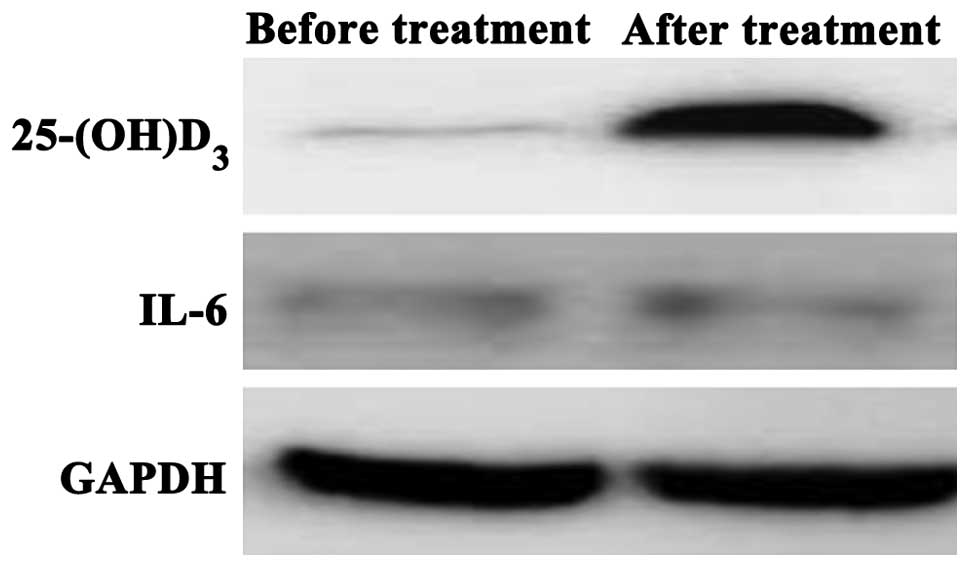
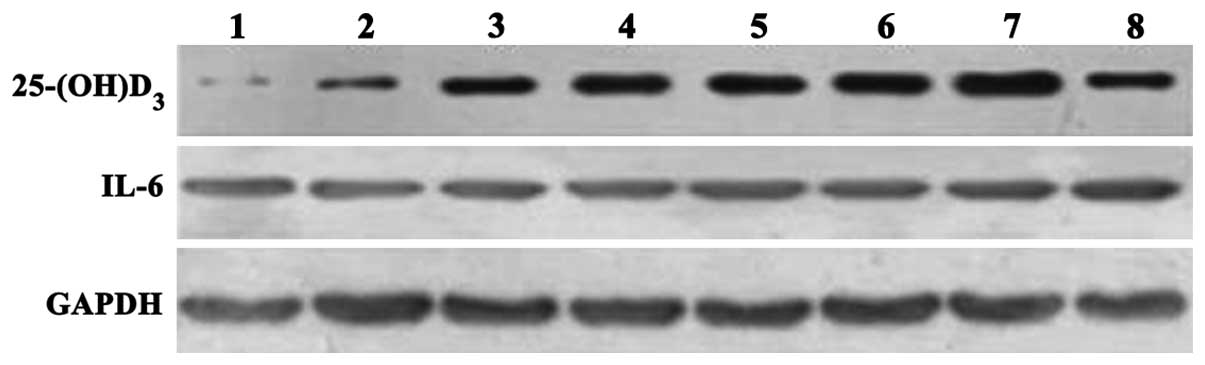
We measured 25-(OH)D3 and IL-6 gene
expression levels in the three groups after immunoglobulin
treatment (Table II) and observed a
significant increase in serum 25-(OH)D3 levels compared
with the levels prior to treatment and the differences were
statistically significant (P<0.05). In the observation group,
after immunoglobulin treatment, the IL-6 level in serum was lower
compared with the level before treatment, albeit the difference was
not statistically significant (P>0.05). The IL-6 level in the
observation group after immunoglobulin treatment had no significant
difference compared to that in the normal control and feverish
control groups (P>0.05). The 25-(OH)D3 and IL-6
expression levels were measured using western blotting (Fig. 3). The results were comparable to
those obtained from ELISA and RT-PCR.
| Table II.Protein expression of
25-(OH)D3 and IL-6 in the serum of the patients in the
observation group before treatment. |
Table II.
Protein expression of
25-(OH)D3 and IL-6 in the serum of the patients in the
observation group before treatment.
| Gene | Before treatment | After treatment | t | P-value |
|---|
|
25-(OH)D3 | 64.3±28.4 | 86.3±14.2 | 2.74 | 0.012 |
| IL-6 | 462.2±198.3 | 443.2±110.4 | 1.03 | 0.409 |
Correlation between
25-(OH)D3 and IL-6 expression in the observation group
prior to and after treatment
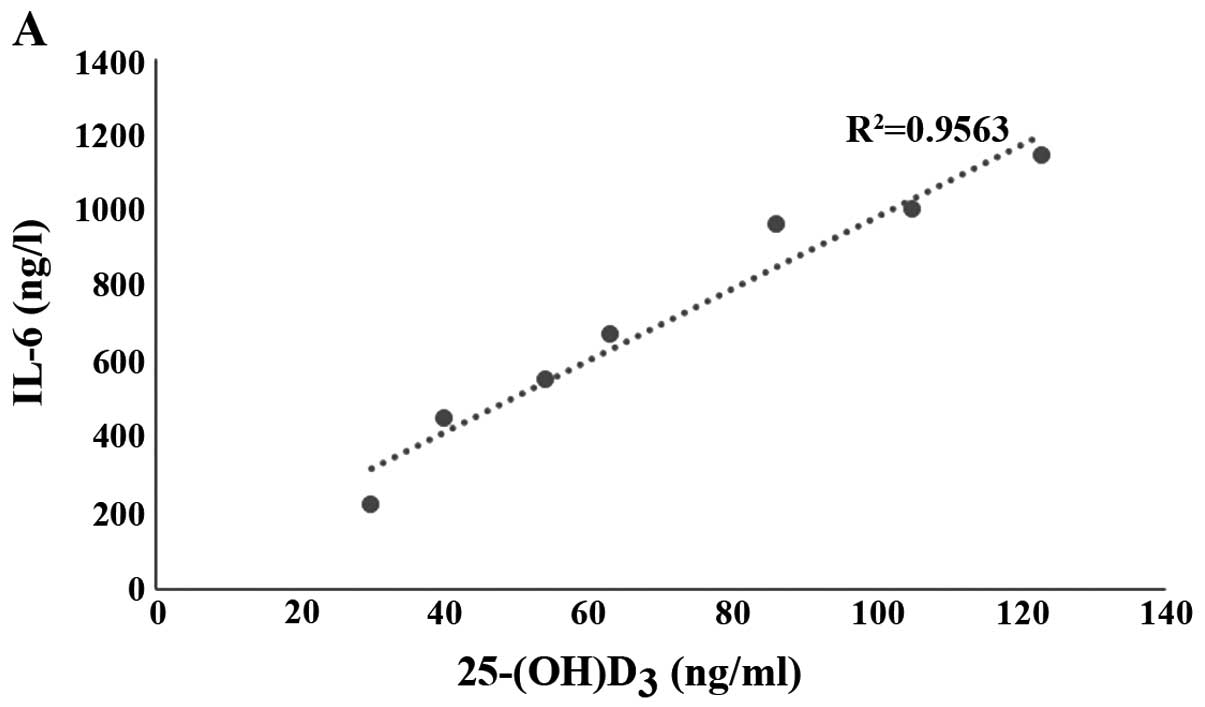
Before treatment, levels of 25-(OH)D3 and
IL-6 in the observation group were positively correlated
(R2=0.9563) (Fig. 4A).
However, no significant correlation was established for levels
after treatment of 25-(OH)D3 and IL-6 (Fig. 4B).
Correlation between
25-(OH)D3 and IL-6 and the disease course in the
observation group
Our results showed that the pathogenic condition of
patients in the observation group was aggravated with time and the
level of 25-(OH)D3, and also increased with time whereas
the content of IL-6 protein remained unchanged in the course of the
disease (Fig. 5).
Discussion
Kawasaki disease is a serious threat to infant
health and growth (11). Related
data (12) have shown that despite
advances in studies and treatment of Kawasaki disease, the exact
pathogenesis of this disease remains to be determined and there is
therefore no effective treatment method that can be utilized
(13). It has been shown that T
cells in patients with Kawasaki disease are abnormally active
(14). Additionally, it has been
established that T cells, to a large extent, can enhance the
immunity and improve the organism's resistance against various
illnesses (15). The results
obtained from related studies have shown that the overactive T cell
can interact with mononuclear cells and stimulate the
overexpression of different cytokines and inflammatory substances
that can damage the blood vessels (16,17). To
shed some light on the subject of the pathogenesis of Kawasaki
disease's, it is extremely important to investigate any possible
connection between this disease and the level of cytokines.
Vitamin D is an important signal molecule in human
body that is involved in the regulation of cellular signal
substances such as calcium and phosphorus, cytomembrane elements,
and immunoreaction such as inhibiting the abnormal proliferation of
body T/B lymphocyte (18). Kudo
et al (4) demonstrated that
in coronary endothelial cells, 25-(OH)D3 inhibited the
release of IL-8 and the expression of cell adhesion molecule-1
induced by TNF-α. However, it could not affect the level of IL-6.
It has been shown that a specific amount of 25-(OH)D3 is
needed for regulating KD coronary artery inflammation (19).
By measuring the 25-(OH)D3 and IL-6 mRNA
and protein in different groups prior to treatment, we showed that
serum 25-(OH)D3 and IL-6 levels in the feverish control
group were significantly lower than those in the normal control
group. The level of 25-(OH)D3 in the serum of children
in the observation group was significantly higher than the level
observed in the normal control group. The level of
25-(OH)D3 in the feverish control group was lower than
the level of IL-6 in the normal children, but the difference was
not statistically significant (P>0.05) while the content of
25-(OH)D3 in the observation group was significantly
higher than the content of serum IL-6 in the normal children. The
results also revealed that before treatment 25-(OH)D3
and IL-6 levels were positively correlated (R2=0.9563).
The same comparison did not reveal any significant correlation
between 25-(OH)D3 and IL-6 levels after treatment. By
measuring 25-(OH)D3 in the serum of children patients
with Kawasaki disease in different courses of disease, we showed
that the pathogenic condition aggravated with time and the level of
25-(OH)D3 was also increased significantly. This finding
suggested that 25-(OH)D3 is involved in the occurrence
of Kawasaki disease in children and may be involved in the
aggravation of the disease to some extent.
References
|
1
|
Hewison M: Vitamin D and the
intracrinology of innate immunity. Mol Cell Endocrinol.
321:103–111. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
White JH: Vitamin D as an inducer of
cathelicidin antimicrobial peptide expression: past, present and
future. J Steroid Biochem Mol Biol. 121:234–238. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Huang G: Epidemiology of Kawasaki disease.
Chinese Journal of Practical Pediatrics. 21:721–723. 2006.
|
|
4
|
Kudo K, Hasegawa S, Suzuki Y, Hirano R,
Wakiguchi H, Kittaka S and Ichiyama T: 1α,25-Dihydroxyvitamin D(3)
inhibits vascular cellular adhesion molecule-1 expression and
interleukin-8 production in human coronary arterial endothelial
cells. J Steroid Biochem Mol Biol. 132:290–294. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Suzuki Y, Ichiyama T, Ohsaki A, Hasegawa
S, Shiraishi M and Furukawa S: Anti-inflammatory effect of
1alpha,25-dihydroxyvitamin D(3) in human coronary arterial
endothelial cells: implication for the treatment of Kawasaki
disease. J Steroid Biochem Mol Biol. 113:134–138. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Schwalfenberg GK: A review of the critical
role of vitamin D in the functioning of the immune system and the
clinical implications of vitamin D deficiency. Mol Nutr Food Res.
55:96–108. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Jackson DJ and Johnston SL: The role of
viruses in acute exacerbations of asthma. J Allergy Clin Immunol.
125:1178–1187. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zhang Z, Xing X, Hensley G, Chang LW, Liao
W, Abu-Amer Y and Sandell LJ: Resistin induces expression of
proinflammatory cytokines and chemokines in human articular
chondrocytes via transcription and messenger RNA stabilization.
Arthritis Rheum. 62:1993–2003. 2010.PubMed/NCBI
|
|
9
|
Donovan C, Tan X, Bourke JE and Rehan VK:
PPARγ ligands regulate noncontractile and contractile functions of
airway smooth muscle: implications for asthma therapy. PPAR Res.
2012:8091642012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Keet CA, McCormack MC, Peng RD and Matsui
EC: Age- and atopy-dependent effects of vitamin D on wheeze and
asthma. J Allergy Clin Immunol. 128:414–416.e5. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Huang Z and Wu ZG: Research status of
pathogenesis of Kawasaki's disease. Journal of Guangdong Medical
College. 28:57–61. 2010.(In Chinese).
|
|
12
|
Jartti T, Ruuskanen O, Mansbach JM,
Vuorinen T and Camargo CA Jr: Low serum 25-hydroxyvitamin D levels
are associated with increased risk of viral coinfections in
wheezing children. J Allergy Clin Immunol. 126:1074–1076,
1076.e1-1076.e4. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Holick MF, Binkley NC, Bischoff-Ferrari
HA, Gordon CM, Hanley DA, Heaney RP, Murad MH and Weaver CM:
Endocrine Society: Evaluation, treatment, and prevention of vitamin
D deficiency: an Endocrine Society clinical practice guideline. J
Clin Endocrinol Metab. 96:1911–1930. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Searing DA and Leung DYM: Vitamin D in
atopic dermatitis, asthma and allergic diseases. Immunol Allergy
Clin North Am. 30:397–409. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
White JH: Vitamin D metabolism and
signaling in the immune system. Rev Endocr Metab Disord. 13:21–29.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Gorman S, Tan DHW, Lambert MJM, Scott NM,
Judge MA and Hart PH: Vitamin D(3) deficiency enhances
allergen-induced lymphocyte responses in a mouse model of allergic
airway disease. Pediatr Allergy Immunol. 23:83–87. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Liu R, Gao F, Huo J and Yi Q: Study on the
relationship between mean platelet volume and platelet distribution
width with coronary artery lesion in children with Kawasaki
disease. Platelets. 23:11–16. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Rothers J, Wright AL, Stern DA, Halonen M
and Camargo CA Jr: Cord blood 25-hydroxyvitamin D levels are
associated with aeroallergen sensitization in children from Tucson,
Arizona. J Allergy Clin Immunol. 128:1093–9.e1, 5. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kim SK, Choe JY, Park SH, Lee SW, Lee GH
and Chung WT: Increased insulin resistance and serum resistin in
Korean patients with Behçet's disease. Arch Med Res. 41:269–274.
2010. View Article : Google Scholar : PubMed/NCBI
|