Introduction
Parenteral nutrition (PN) and enteral nutrition (EN)
are two important supportive therapies for clinical surgical
treatment. Early EN (EEN) should be preferred to total PN (TPN)
whenever possible or at any point that the patient has a
functioning gut (1–4).
Numerous studies showed that EEN had a positive
influence on improving intestinal function and reducing the
incidence of postoperative complications, especially for severe
illness (5–7). Additionally, EEN has been demonstrated
to be more physiological, to prevent morphologic and functional
trauma-related alterations of the gut, to modulate the immune and
inflammatory responses to injury, and to be more cost-efficient
than TPN (8–12). However, the feasibility and efficacy
of EEN in patients with digestive tract surgery has remained
inconclusive.
Randomized controlled trials (RCTs) (13) suggested that the early resumption of
oral intake does not decrease the duration of postoperative ileus
or lead to a significantly increased rate of nasogastric tube
reinsertion. Eckerwall et al found that the overall early
complication rate was higher in EN than TPN in patients with
predicted severe acute pancreatitis (14).
The present meta-analysis was performed to
investigate RCTs in patients with and without EEN after digestive
tract surgery to provide concrete clinical evidence for the
feasibility and efficacy of EEN.
Materials and methods
Study selection
The databases PubMed (http://www.pubmed.com), EMBASE (http://www.embase.com), Web of Science (http://apps.webofknowledge.com), The Cochrane
Library (http://www.thecochranelibrary.com), China National
Knowledge Infrastructure (CNKI; http://www.cnki.net/) and VIP (http://www.cqvip.com/) were systematically searched
for RCTs concerning the effect of EEN (using the key terms: ‘early
feeding’, ‘early postoperative feeding’, ‘early postoperative
enteral nutrition’, ‘early postoperation oral feeding’, ‘immediate
enteral nutrition’, ‘immediate postoperative feeding’ and their
variants) in patients with digestive tract surgery (using the key
terms ‘operation’, ‘gastrointestinal surgery’, ‘upper digestive
tract’, ‘alimentary tract’, ‘gut’, ‘colorectal’, ‘colon’, ‘rectum’,
‘stomach’, ‘pancreas’, ‘duodenum’, ‘gastric’, ‘intestinal’,
‘gastrectomy’, and ‘enterectomy’ and their variants). When multiple
articles for a similar study were found, we considered only the
most complete and recently published ones and supplemented the
present meta-analysis, if necessary, with data from the most
complete or updated publication. References from the extracted
articles and reviews were also consulted to complete the data
bank.
Studies were included for the present meta-analysis
if they complied with the following inclusion criteria: i) RCTs
with parallel controlled design; ii) patients underwent digestive
tract surgery for reasons other than renal, cardiac or hepatic
failure; iii) EEN was provided within one postoperative day in the
treatment group; iv) biochemical indices (serum total protein,
serum albumin and serum prealbumin), length of first bowel action,
infectious and non-infectious complications and length of hospital
stay; and v) supplementary data relevant to this meta-analysis were
available. Studies were excluded from the present meta-analysis due
to: i) patients not being randomized; ii) inadequate statistical
analysis; and iii) use of animal trials, less relevant, review
articles and case reports.
Data extraction
From each study, we extracted information regarding
first author, year of publication, country of origin, sample size,
age, gender, type of diseases or surgeries, average study follow-up
time, type of intervention, duration of intervention, disease
outcome, method of outcome ascertainment, unit of measurement and
corresponding 95% confidence intervals (CIs), standard error (SEs),
or exact P-values from text, and Tables and Figs. Since the
differences in the study populations and study design of the
included studies potentially cause variations in the results, a
study-quality score was calculated using methodological quality
assessment (15) for each of the
included traits ranging from 0 to 5. Based on this, the studies
were categorized into high quality score (3–5 points), low quality
score (1–2 points) and no RCTs (0 point).
Data analysis
The data pooling was performed following classical
meta-analysis method using the Review Manager (RevMan) (Computer
Program). (Version 5.2. Copenhagen: The Nordic Cochrane Centre, The
Cochrane Collaboration 2014; http://ims.cochrane.org/revman/). P<0.05 was
considered statistically significant. The missing standard
deviation (SD) value for one trial was imputed from SD values of
the remaining trials using the same measure (16). For estimation of the analysis
indexes, relative risk (RR) was used as the effect size of the
categorical variable, while the weighted mean difference (MD) was
used as the effect size of the continuous variable. The 95% CI was
calculated for each investigation and for each outcome variable.
The statistical heterogeneity test was performed using the
I2 statistic (α=0.05), which assessed the
appropriateness of pooling the individual study results prior to
calculating the standardized mean effect for all the trials. The
I2 value provided an estimate of the amount of variance
across studies because of heterogeneity rather than chance
(17). The I2 values 25,
50 and 75% corresponded to low, moderate and high levels of
heterogeneity, respectively. If P≥0.05, the heterogeneity was not
substantial and low between the trials. Thus, fixed-effects models
were used with the Mantel-Haenszel (M-H) method weighting for
combined statistics. If P<0.05, the heterogeneity was considered
substantial and high between the trials. Consequently, combined
results were conducted using the random-effects models, which were
inverse variance weighting or the DerSimonian-Laird method based on
the fixed-effects models. A priori potential sources of
heterogeneity were a concern for publication bias. The possible
publication bias was investigated by drawing a funnel plot to
search for funnel plot asymmetry and meta-regression based on study
size (18).
Results
Characteristics of the studies
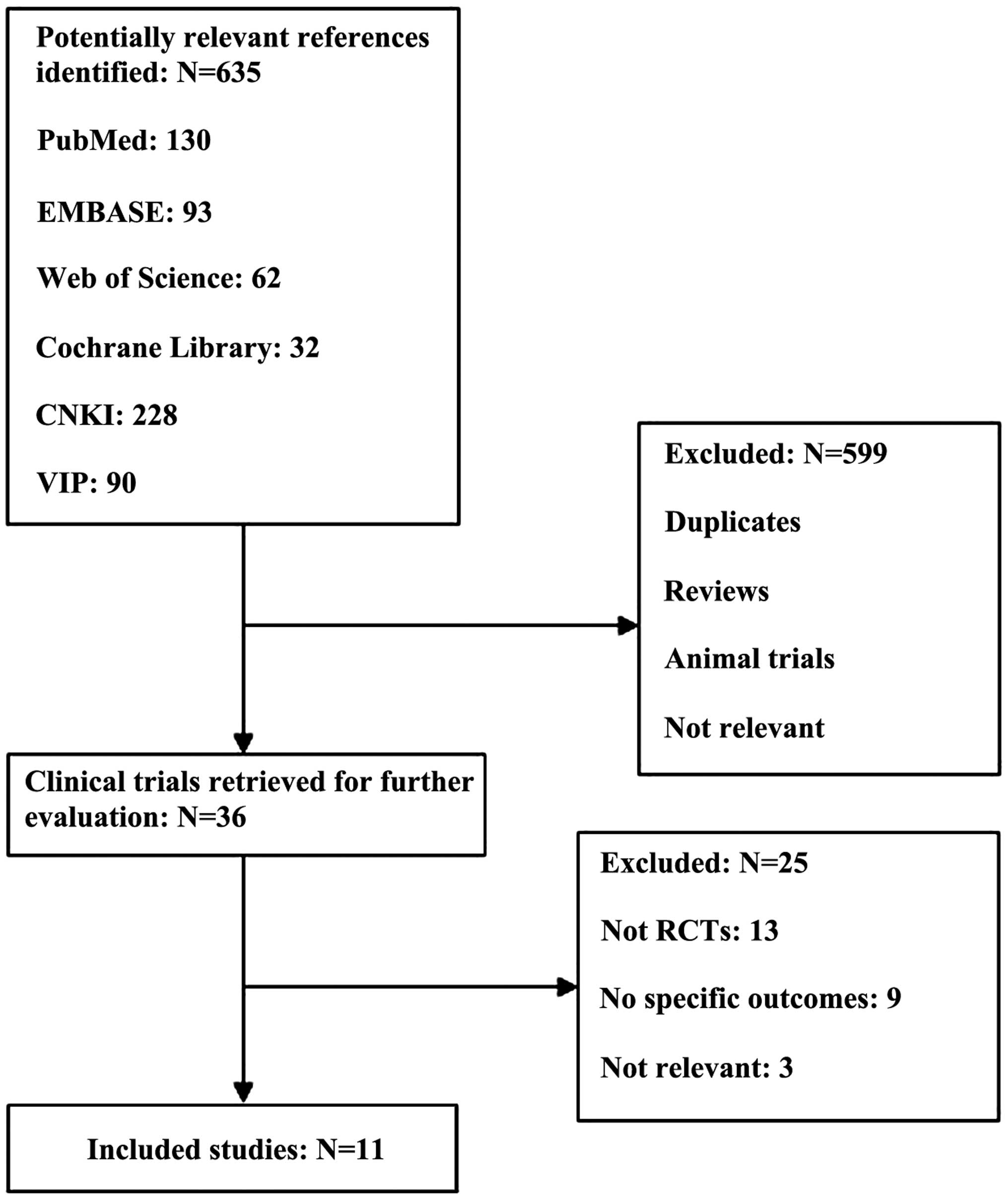
The initial search yielded 635 potentially relevant
results and from these only 11 (19,29) RCTs
complied with the inclusion criteria and were subsequently included
in the present meta-analysis (Fig.
1). A total of 1,095 samples were considered from these 11 RCTs
and the sample size varied between studies ranging from 28 to 317.
Only the subjects who received EEN within one postoperative day
constituted the treatment group for this meta-analysis. The
information extracted from these RCTs is presented in Table I. The 11 RCTs were published during
the period between October, 1966 to December, 2014.
 | Table I.Characteristics of the trials
included in the present meta-analysis in chronological order by
year of publication. |
Table I.
Characteristics of the trials
included in the present meta-analysis in chronological order by
year of publication.
| Author (year) | Country | Type of diseases or
surgeries | Age, year
(treatment/control) | Gender (M/F) | No. of subjects
(treatment/control) | Intervention
(treatment/control) | Duration, day | Design | Study-quality
score | (Refs.) |
|---|
| Schroeder et
al (1991) | New Zealand | Bowel
resection | 51±18/53±22 | 17/15 | 32 (16/16) | POD 1 EN | Routine
postoperative feeding | 14 | DB, C, R | 5 | (19) |
| Reissman et
al (1995) | USA | Elective colorectal
surgery | 16–90 | 77/84 | 161 (80/81) | POD 1 EN | Regular
feeding | – | PC, R | 3 | (20) |
| Ortiz et al
(1996) | Spain | Elective colorectal
and rectal surgery | 22–90 | – | 190 (91/91) | POD1 EN | Routine
postoperative feeding | 10 | PC, R | 3 | (21) |
| Braga et al
(1996) | Italy | Gastric or
pancreatic cancer | 59±9/61±7 | – | 40 (20/20) | POD 1 EN | TPN | 7 | PC, R | 3 | (22) |
| Singh et al
(1998) | India | Non-traumatic
intestinal perforation and peritonitis |
38.9±2.1/40.8±2.3 | – | 43 (21/22) | POD 0.5 EN | TPN | 7 | PC, R | 3 | (23) |
| Watters et
al (1997) | Canada | Esophagectomy or
pancreatoduodenectomy | 64±11/61±12 | 22/6 | 28 (13/15) | POD 1 EN | Unfed | 6 | PC, R | 3 | (24) |
| Stewart et
al (1998) | Australia | Elective
intraperitoneal colorectal resections | 17–89 | 43/37 | 80 (40/40) | POD 1 EN | POD1-2 EN | 10 | PC, R | 3 | (25) |
| Hu et al
(1999) | China | Gastrointestinal
surgery | 38±10.2/45±9.8 | 30/8 | 38 (18/20) | POD 1 EN | PN | 5 | PC, R | 3 | (26) |
| Bozzetti et
al (2001) | Italy | Gastrointestinal
cancer |
64.8±10.8/64.1±9.8 | 185/132 | 317 (159/158) | POD 1 EN | PN | 7 | PC, R | 3 | (27) |
| Farreras et
al (2005) | Spain | Gastric cancer |
66.7±8.3/69.2±13.8 | 32/28 | 60 (30/30) | POD 1 EN | Routine
postoperative feeding | 7 | DB, C, R | 5 | (28) |
| Wu et al
(2006) | China | Esophageal
carcinoma | 33–79 | 78/28 | 106 (53/53) | POD 1 EN | PN | 7 | PC, R | 3 | (29) |
Relevant biochemical indices
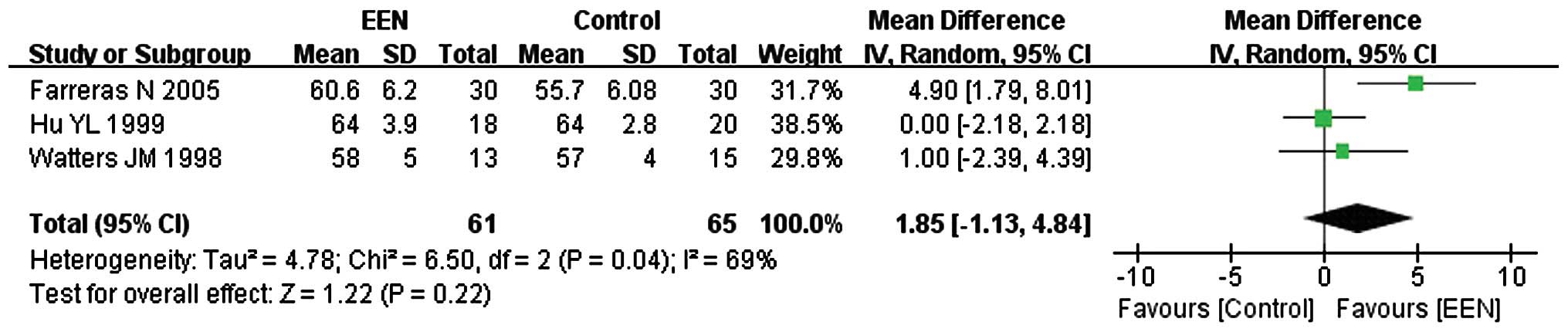
Serum total protein
In total, 126 participants from 3 (24,26,28) of
the 11 studies were enrolled to evaluate the change of serum total
protein (g/l). Since the heterogeneity of serum between the studies
was significant (I2=69%; P<0.05; χ2=6.50)
the random-effects model was used. From the analysis, we found
statistically insignificant difference between the EEN and control
group (MD=1.85, 95% CI: −1.13, 4.84; P>0.05) (Fig. 2).
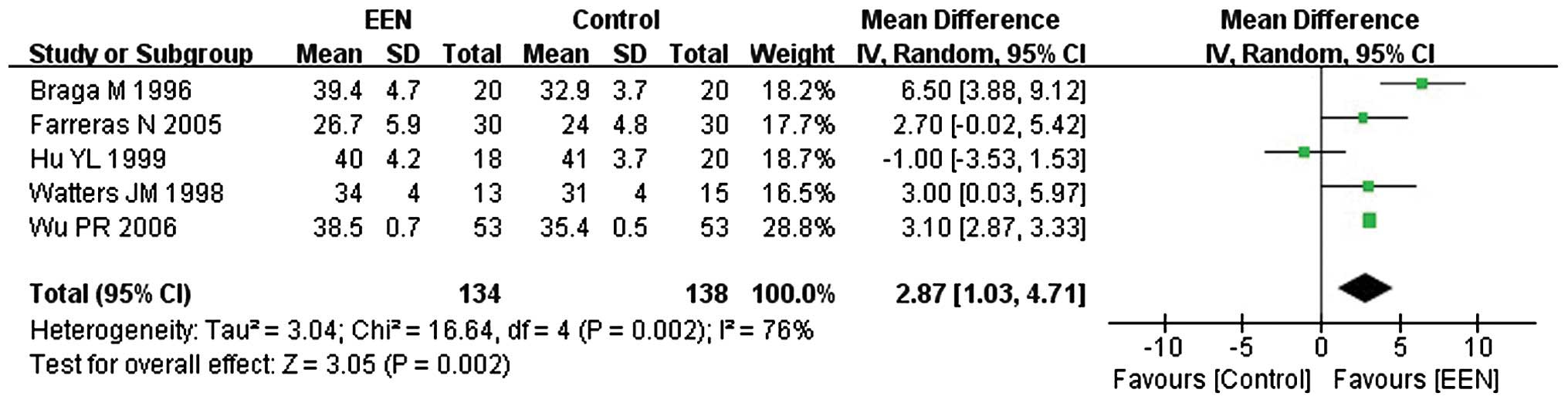
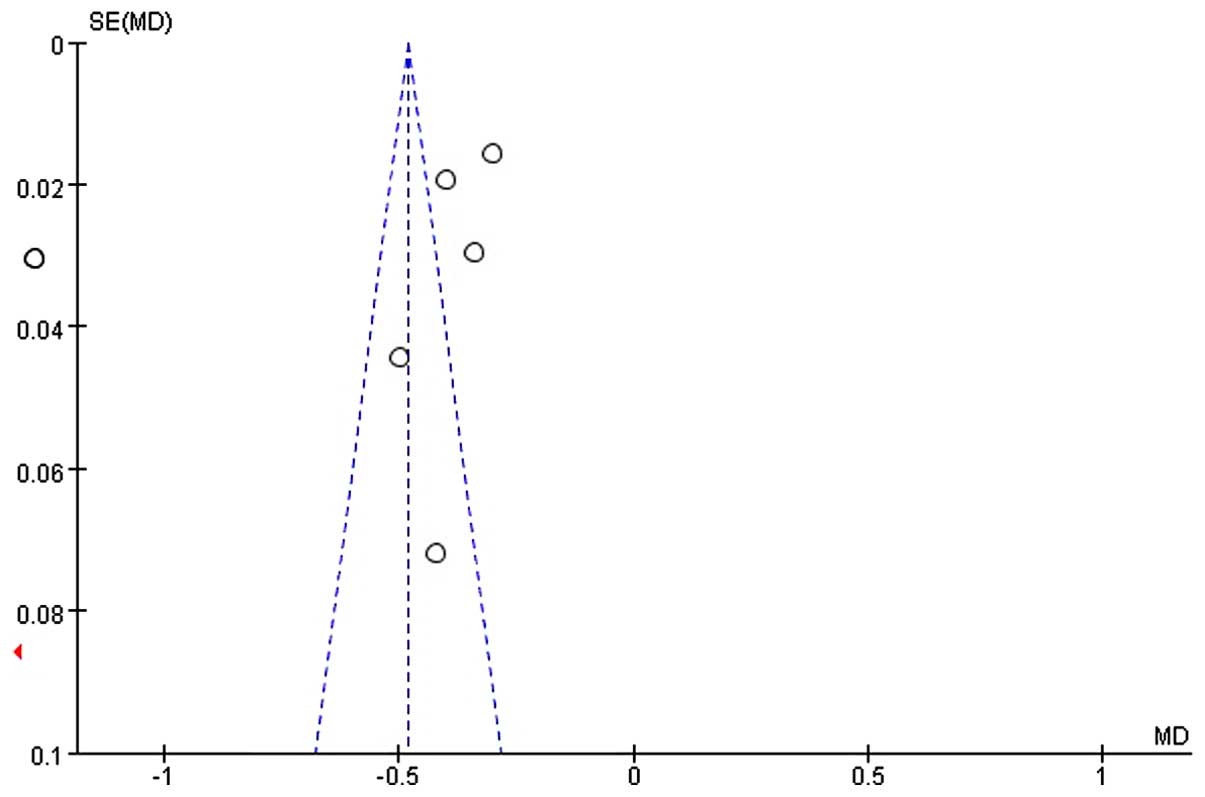
Serum albumin
Approximately 272 participants from 5 of the 11
studies (22,24,26,28,29) were
enrolled to evaluate the serum albumin (g/l). Since, the
heterogeneity of serum albumin between the studies was significant
(I2=76%; P<0.05; χ2=16.64) we applied the
random-effects model. We found a statistically significant
difference between the EEN and control groups (MD=2.87, 95% CI:
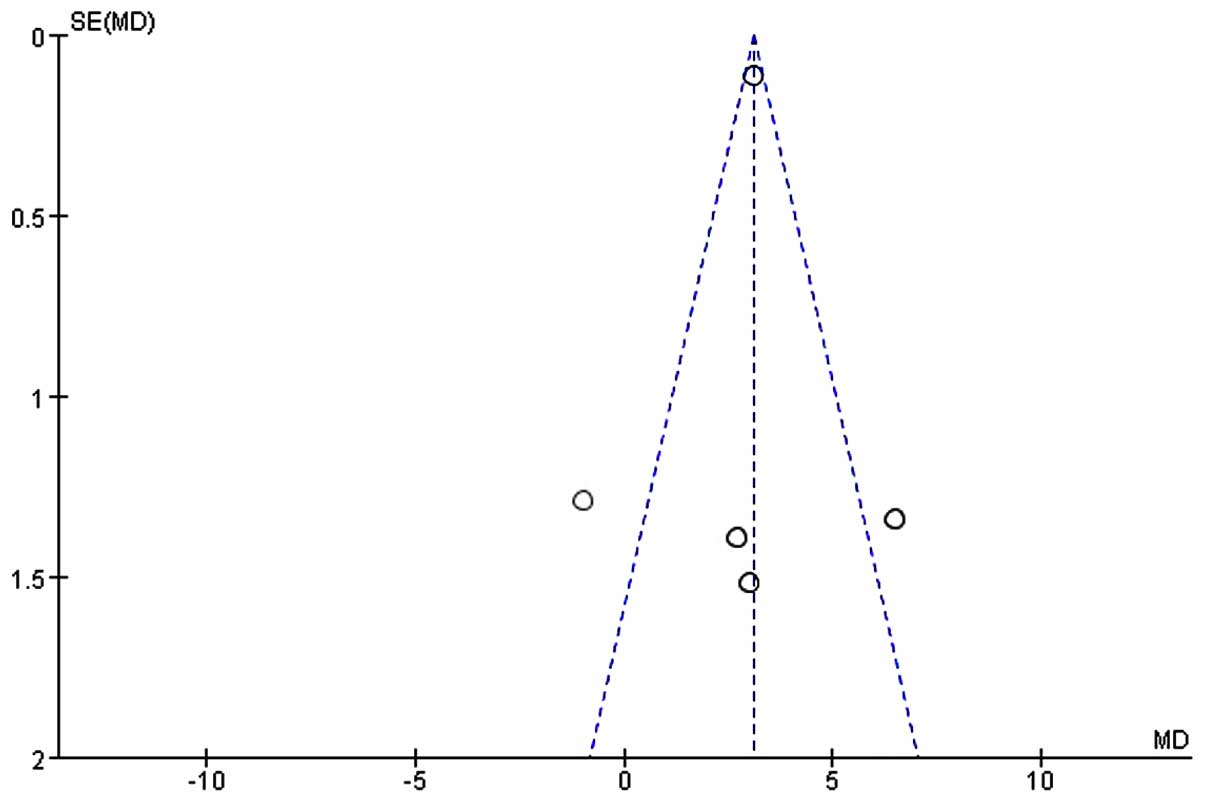
1.03, 4.71; P<0.05) (Fig. 3). The
symmetry funnel plot suggested scarcely any publication bias
existed between studies mentioning change of serum albumin
(Fig. 4).
Serum prealbumin
Of the 11 studies, only 2 (22,28)
studies with a sample size of 100 subjects focused on serum
prealbumin (g/l). The fixed-effects model was used for the
heterogeneity to be considered acceptable (I2= 8%;
P>0.05; χ2=1.09). Our analysis revealed that
providing EEN was more effective in increasing the serum prealbumin
(MD=0.04, 95% CI: 0.02, 0.05; P<0.05) than the control (Fig. 5).
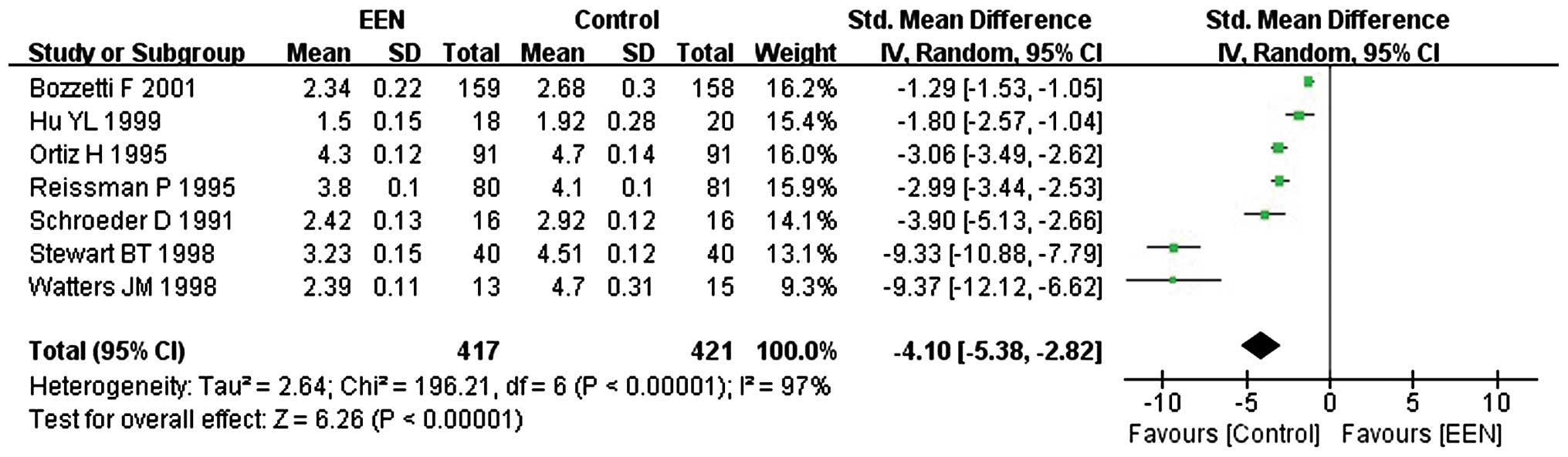
Length of first bowel action
Information was obtained on the length of first
bowel action in 838 patients from 7 studies (19–21,24–27).
Since the heterogeneity was significant (I2= 97%;
P<0.05; χ2=196.21) (Fig.
7) and the asymmetry funnel plot suggested possible publication
bias existed between these (Fig. 6),
we applied the random-effects model to analyze the data. Our
analysis revealed that the patients in the EEN group had a shorter
length of first bowel action than the control group (MD=−4.10, 95%
CI: −5.38, −2.82; P<0.05) (Fig.
7).
Complications
In 8 studies (19–21,23,25,27–29)
analysed, it was found that EEN had an impact on postoperative
complications (infectious and non-infectious complications)
(Table II) in 981 patients with
digestive tract surgery.
| Table II.Classification of complications in
the included trials. |
Table II.
Classification of complications in
the included trials.
| Sl., no. | Infectious
complications | Non-infectious
complications |
|---|
| 1 | Bacteraemia | Anastomotic
leak |
| 2 | Intra-abdominal
abscess | Gastrointestinal
bleeding |
| 3 | Pelvic abscess | Hemoperitoneum |
| 4 | Pneumonia | Hepatic
dysfunction |
| 5 | Sepsis | Ileus/intestinal
obstruction |
| 6 | Septic shock | Myocardial
infarction |
| 7 | Septic
coagulopathy | Pancreatic
fistula |
| 8 | Urinary tract
infections | Pancreatitis |
| 9 | Wound
infections | Pericarditis |
| 10 |
| Pleural
effusion |
| 11 |
| Suture failure |
| 12 |
| Renal failure |
| 13 |
| Respiratory
failure |
| 14 |
| Venous
thrombosis |
| 15 |
| Wound
dehiscence |
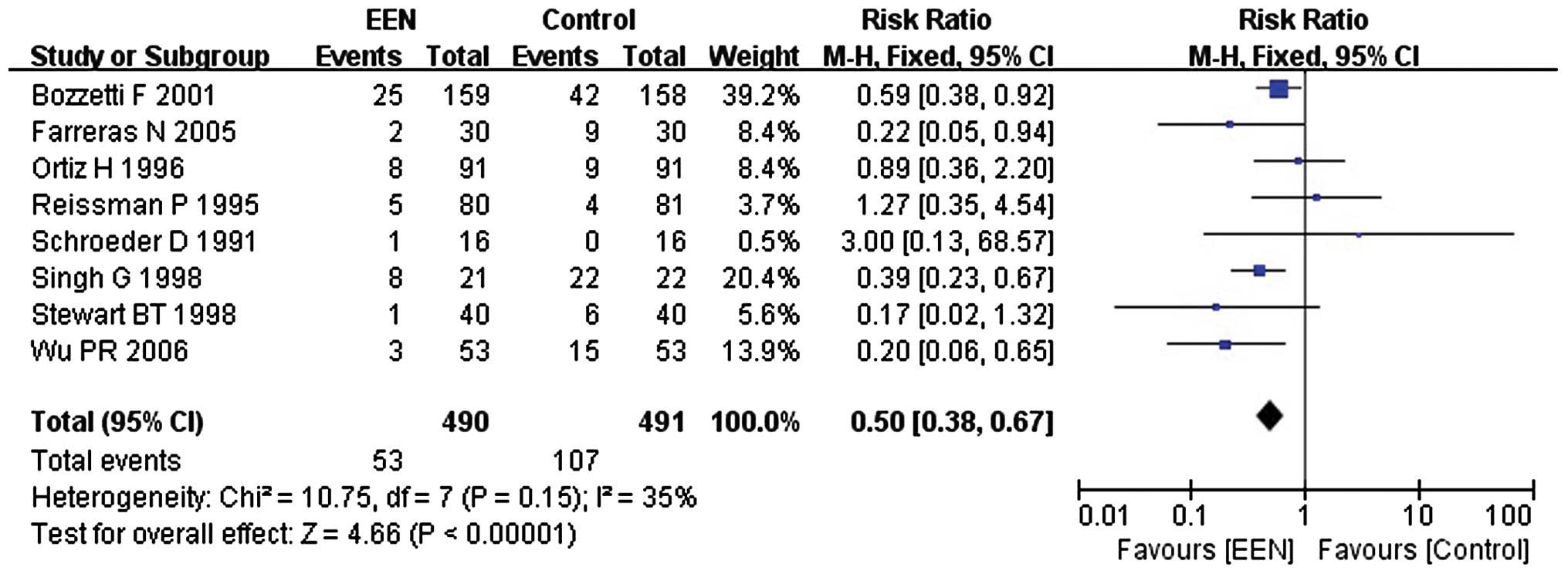
Infectious complications
Our analysis using the fixed-effect model for
infectious complications (I2=35%; P>0.05;
χ2=10.75) suggested that, EEN was more effective in
decreasing the incidence of infectious complications in comparison
with control (RR=0.50, 95% CI: 0.38, 0.67; P<0.01) (Fig. 8).
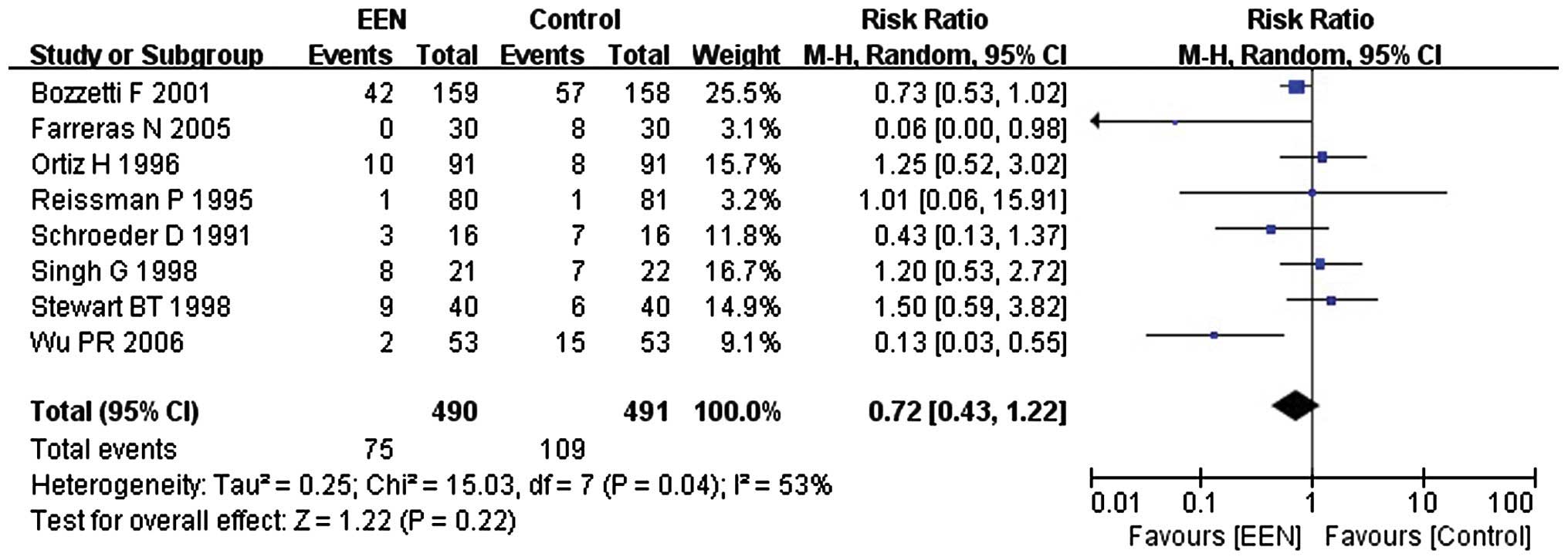
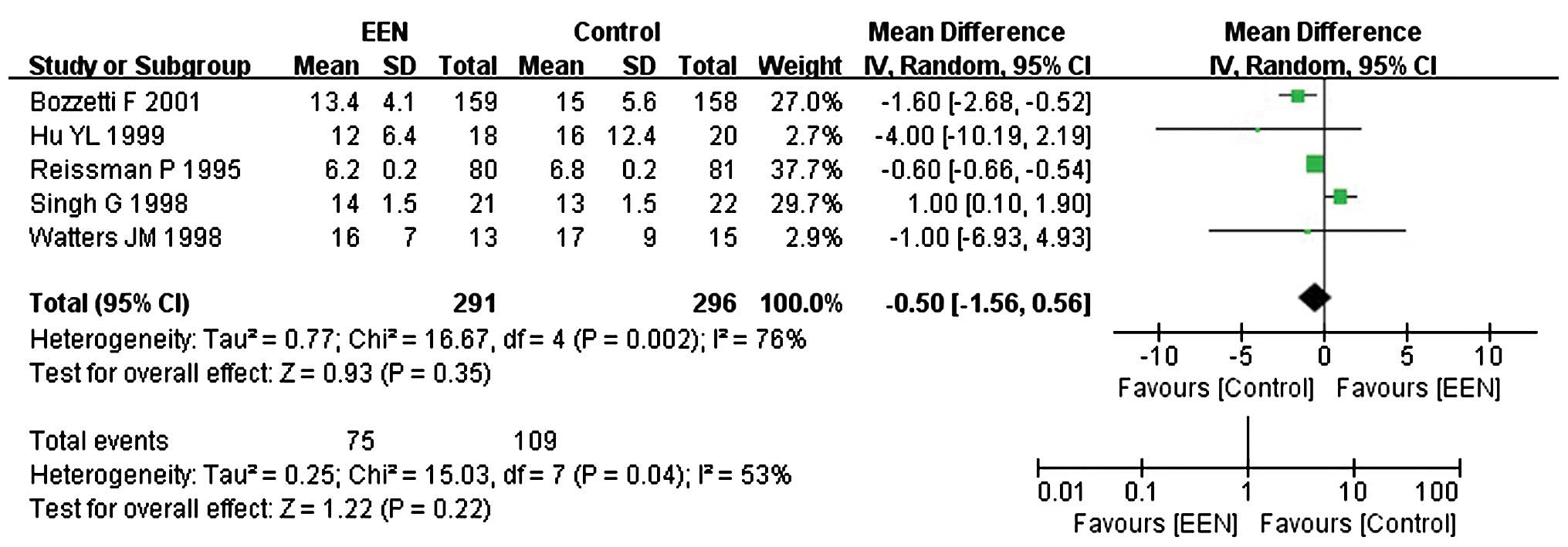
Non-infectious complications
Our analysis revealed that the heterogeneity of
non-infectious complications between the studies was significant
(I2=53%; P<0.05; χ2=15.03). Thus, we
performed a subgroup analysis and the subgroups were divided
dependent on whether the EN or PN were added to the control group.
I2 between the subgroups was 0% (P=0.60;
Chi2=0.28). Consequently, the fixed-effects model was
used. The results suggested that patients in the EEN group had a
lower incidence of non-infectious complication (RR=0.72, 95% CI:
0.43, 1.22; P<0.05) than the control (Fig. 9).
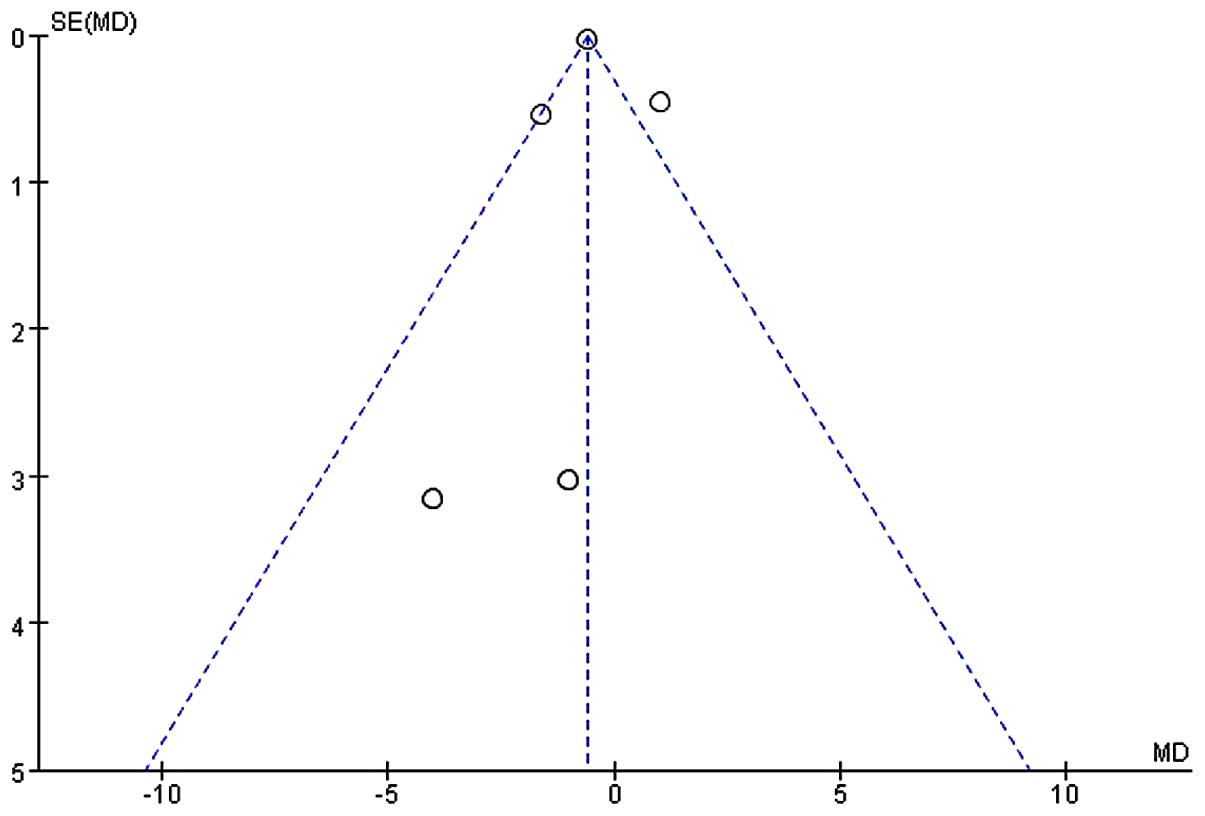
Length of hospital stay
Five studies (20,23,24,26,27)
comprising 587 subjects mentioned the length of hospital stay
(day). I2 between the studies was 76% (P<0.05;
χ2=16.67) and thus a random-effects model was used. Our
analysis revealed no significant difference with respect to
shortening the length of hospital stay between the EEN and control
groupa (MD=−0.50, 95% CI: −1.56, 0.56; P>0.05) (Fig. 10). Furthermore, the asymmetry funnel
plot suggested a possible publication bias existed between the
studies in which patients mentioned the change of length of
hospital stay (Fig. 11).
Discussion
Nutritional support is a vital part of the therapy
of most surgical patients. Early initiation, particularly via the
enteral route has a significant effect on postoperative recovery in
a wide variety of patients (30).
However, the physiological mechanisms underlying the beneficial
effect of EEN have yet to be fully elucidated. Factors that may
play a role include preservation of gut mass, prevention of
increased gut permeability to bacteria and other toxins, and
maintenance of the gut-associated lymphoid tissue (31). Classically, the term ‘early’ was
defined as EN administration within postoperative day 3 (32); however, ‘early’ has been more
recently redefined as EN administration within 24–48 h after
admission or surgery (33). It
appears that administration of nutrition within 24 h of major
surgery, injury, or burn is ideal, but within 48 h is acceptable.
However, hemodynamic stability is a prerequisite to the initiation
of enteral feeding (34). RCTs
included in the present meta-analysis administered EN support to
patients within 12 or 24 h after digestive tract surgery.
Surgical patients usually present an intense
metabolic state due to neuroendocrine stress, which may exacerbate
protein catabolism developing negative nitrogen balance (35). Serum protein is an important
indicator of the body's nutritional status. Serum albumin is the
most abundant protein in blood plasma with a serum half-life of
approximately 20 days, serving as a potential marker for
nutritional status (36). The serum
half-life of prealbumin is approximately 1.9 days, constituting it
a sensitive marker of nutritional evaluation for a short period of
time (37). In the present
meta-analysis, although the administration of EEN had no
significant effect on serum total protein, it significantly
increased the levels of serum albumin and prealbumin, suggesting
use of EEN benefited protein synthesis and wound healing, thereby
improving the nutritional status of patients.
Previous findings have shown that PN induced an
atrophy of the small intestinal mucosa due to a strong reduction in
villi height and the crypt length, resulting in intestinal barrier
dysfunction (38,39). Therefore, PN often induced
enterogenic infection in patients with digestive tract surgery. EN
support had fewer infectious complications than others by
comparison. The rationale of nil by mouth and gastric decompression
aims to prevent postoperative nausea and vomiting and protect
anastomosis, thus allowing wound healing to occur prior to the body
experiencing stress from food (40).
Our meta-analysis revealed that EEN for patients with digestive
tract surgery decreased the incidence of postoperative infectious
and non-infectious complications effectively, suggesting EEN is
important in protecting the intestinal barrier, improving immune
function and reducing the incidence of postoperative infections. In
addition, EEN administration for patients with digestive tract
surgery resulted in shorter length of first bowel action after
surgery. Thus, EEN may stimulate the growth of intestinal
epithelial cells, regulate the neuroendocrine system and induce gut
hormone secretion, and subsequently increased blood flow to vital
organs of the digestive system for functional recovery (41–43).
Furthermore, fiber in the EN may have also contributed to the
gastrointestinal recovery after surgery (44). As for the length of hospital stay,
the analysis showed no significant difference between the EEN and
control groups.
The present meta-analysis has some limitations.
First, the 11 included trials mentioned randomization and parallel
control, but did not mention whether the studies were blinded,
which affects the quality scores of the included trials. Second,
the quality score of Bozzetti et al (27) was 3, but the number of enrolled
subjects was large, which leads to uncertainty in biases to the
final result of the present meta-analysis. Third, the variety of
intervention in the control group and duration of nutrition support
between the included trials may also affect the final results.
In conclusion, the results show that EEN for
patients with digestive tract surgery improves the nutritional
status, promotes the functional recovery of digestive system and
reduces the risk of postoperative complications.
Acknowledgements
The present study was supported by the ‘Twelfth
Five-Year’ National Key Technology R&D Program of China (grant
no. 2012BAI35B03).
References
|
1
|
Klein S, Kinney J, Jeejeebhoy K, Alpers D,
Hellerstein M, Murray M and Twomey P: Nutrition support in clinical
practice: Review of published data and recommendations for future
research directions. National Institutes of Health, American
Society for Parenteral and Enteral Nutrition, and American Society
for Clinical Nutrition. JPEN J Parenter Enteral Nutr. 21:133–156.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
American Gastroenterological Association
Medical Position Statement, . Guidelines for the use of enteral
nutrition. Gastroenterology. 108:1280–1281. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chambrier C and Sztark F: Société
Francophone de nutrition clinique et métabolisme (SFNEP); Société
française d'anesthésie et réanimation (SFAR): French clinical
guidelines on perioperative nutrition. Update of the 1994 consensus
conference on perioperative artificial nutrition for elective
surgery in adults. J Visc Surg. 149:e325–e336. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Pironi L, Candusso M, Biondo A, Bosco A,
Castaldi P, Contaldo F, Finocchiaro E, Giannoni A, Mazzuoli S,
Orlandoni P, et al: Italian Society for Parenteral and Enteral
Nutrition Executive Committee: Prevalence of home artificial
nutrition in Italy in 2005: A survey by the Italian Society for
Parenteral and Enteral Nutrition (SINPE). Clin Nutr. 26:123–132.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kaur N, Gupta MK and Minocha VR: Early
enteral feeding by nasoenteric tubes in patients with perforation
peritonitis. World J Surg. 29:1023–1027; discussion 1027-1028.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Grizas S, Gulbinas A, Barauskas G and
Pundzius J: A comparison of the effectiveness of the early enteral
and natural nutrition after pancreatoduodenectomy. Medicina
(Kaunas). 44:678–686. 2008.PubMed/NCBI
|
|
7
|
Zhang K, Sun WB, Wang HF, Li ZW, Zhang XD,
Wang HB and Ji X: Early enteral and parenteral nutritional support
in patients with cirrhotic portal hypertension after pericardial
devascularization. Hepatobiliary Pancreat Dis Int. 4:55–59.
2005.PubMed/NCBI
|
|
8
|
Gianotti L, Alexander JW, Nelson JL,
Fukushima R, Pyles T and Chalk CL: Role of early enteral feeding
and acute starvation on postburn bacterial translocation and host
defense: Prospective, randomized trials. Crit Care Med. 22:265–272.
1994. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Johnson CD and Kudsk KA: Nutrition and
intestinal mucosal immunity. Clin Nutr. 18:337–344. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Braga M, Gianotti L, Gentilini O, Parisi
V, Salis C and Di Carlo V: Early postoperative enteral nutrition
improves gut oxygenation and reduces costs compared with total
parenteral nutrition. Crit Care Med. 29:242–248. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
CunninghamRundles S and Lin DH: Nutrition
and the immune system of the gut. Nutrition. 14:573–579. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lin MT, Saito H, Fukushima R, Inaba T,
Fukatsu K, Inoue T, Furukawa S, Han I and Muto T: Route of
nutritional supply influences local, systemic, and remote organ
responses to intraperitoneal bacterial challenge. Ann Surg.
223:84–93. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
HanGeurts IJ, Hop WC, Kok NF, Lim A,
Brouwer KJ and Jeekel J: Randomized clinical trial of the impact of
early enteral feeding on postoperative ileus and recovery. Br J
Surg. 94:555–561. 2007. View
Article : Google Scholar : PubMed/NCBI
|
|
14
|
Eckerwall GE, Axelsson JB and Andersson
RG: Early nasogastric feeding in predicted severe acute
pancreatitis: A clinical, randomized study. Ann Surg. 244:959–965;
discussion 965-967. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Jadad AR, Moore RA, Carroll D, Jenkinson
C, Reynolds DJM, Gavaghan DJ and McQuay HJ: Assessing the quality
of reports of randomized clinical trials: Is blinding necessary?
Control Clin Trials. 17:1–12. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Furukawa TA, Barbui C, Cipriani A,
Brambilla P and Watanabe N: Imputing missing standard deviations in
meta-analyses can provide accurate results. J Clin Epidemiol.
59:7–10. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sofi F, Abbate R, Gensini GF and Casini A:
Accruing evidence on benefits of adherence to the Mediterranean
diet on health: An updated systematic review and meta-analysis. Am
J Clin Nutr. 92:1189–1196. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sterne JAC, Egger M and Smith GD:
Systematic reviews in health care: Investigating and dealing with
publication and other biases in meta-analysis. BMJ. 323:101–105.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Schroeder D, Gillanders L, Mahr K and Hill
GL: Effects of immediate postoperative enteral nutrition on body
composition, muscle function, and wound healing. JPEN J Parenter
Enteral Nutr. 15:376–383. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Reissman P, Teoh TA, Cohen SM, Weiss EG,
Nogueras JJ and Wexner SD: Is early oral feeding safe after
elective colorectal surgery? A prospective randomized trial. Ann
Surg. 222:73–77. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ortiz H, Armendariz P and Yarnoz C: Early
postoperative feeding after elective colorectal surgery is not a
benefit unique to laparoscopy-assisted procedures. Int J Colorectal
Dis. 11:246–249. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Braga M, Vignali A, Gianotti L, Cestari A,
Profili M and Carlo VD: Immune and nutritional effects of early
enteral nutrition after major abdominal operations. Eur J Surg.
162:105–112. 1996.PubMed/NCBI
|
|
23
|
Singh G, Ram RP and Khanna SK: Early
postoperative enteral feeding in patients with nontraumatic
intestinal perforation and peritonitis. J Am Coll Surg.
187:142–146. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Watters JM, Kirkpatrick SM, Norris SB,
Shamji FM and Wells GA: Immediate postoperative enteral feeding
results in impaired respiratory mechanics and decreased mobility.
Ann Surg. 226:369–377. discussion 377-380, . 1997. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Stewart BT, Woods RJ, Collopy BT, Fink RJ,
Mackay JR and Keck JO: Early feeding after elective open colorectal
resections: A prospective randomized trial. Aust N Z J Surg.
68:125–128. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Hu YL, Xiao XM, Yang CY and Xia HS: Early
enteral nutrition after gastrointestinal surgery clinical research.
J Clin Surg. 7:14–16. 1999.
|
|
27
|
Bozzetti F, Braga M, Gianotti L, Gavazzi C
and Mariani L: Postoperative enteral versus parenteral nutrition in
malnourished patients with gastrointestinal cancer: A randomised
multicentre trial. Lancet. 358:1487–1492. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Farreras N, Artigas V, Cardona D, Rius X,
Trias M and González JA: Effect of early postoperative enteral
immunonutrition on wound healing in patients undergoing surgery for
gastric cancer. Clin Nutr. 24:55–65. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Wu PR, Xu L and Zhang ZM: Comparative
study of postoperative early enteral nutrition and parenteral
nutrition in esophageal carcinoma. Zhonghua Wei Chang Wai Ke Za
Zhi. 9:320–322. 2006.(In Chinese). PubMed/NCBI
|
|
30
|
Minard G and Kudsk KA: Is early feeding
beneficial? How early is early? New Horiz. 2:156–163.
1994.PubMed/NCBI
|
|
31
|
Kobayashi K, Koyama Y, Kosugi S, Ishikawa
T, Sakamoto K, Ichikawa H and Wakai T: Is early enteral nutrition
better for postoperative course in esophageal cancer patients?
Nutrients. 5:3461–3469. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Garrel DR, Davignon I and Lopez D: Length
of care in patients with severe burns with or without early enteral
nutritional support. A retrospective study. J Burn Care Rehabil.
12:85–90. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Doig GS, Heighes PT, Simpson F, Sweetman
EA and Davies AR: Early enteral nutrition, provided within 24 h of
injury or intensive care unit admission, significantly reduces
mortality in critically ill patients: A meta-analysis of randomised
controlled trials. Intensive Care Med. 35:2018–2027. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Serón-Arbeloa C, Puzo-Foncillas J,
Garcés-Gimenez T, Escós-Orta J, Labarta-Monzón L and Lander-Azcona
A: A retrospective study about the influence of early nutritional
support on mortality and nosocomial infection in the critical care
setting. Clin Nutr. 30:346–350. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Japur CC, Monteiro JP, Marchini JS, Garcia
RW and Basile-Filho A: Can an adequate energy intake be able to
reverse the negative nitrogen balance in mechanically ventilated
critically ill patients? J Crit Care. 25:445–450. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Roberts I, Blackhall K, Alderson P, Bunn F
and Schierhout G: Human albumin solution for resuscitation and
volume expansion in critically ill patients. Cochrane Database Syst
Rev. 9:CD0012082011.
|
|
37
|
Bae HJ, Lee HJ, Han DS, Suh YS, Lee YH,
Lee HS, Cho JJ, Kong SH and Yang HK: Prealbumin levels as a useful
marker for predicting infectious complications after gastric
surgery. J Gastrointest Surg. 15:2136–2144. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Groos S, Hunefeld G and Luciano L:
Parenteral versus enteral nutrition: Morphological changes in human
adult intestinal mucosa. J Submicrosc Cytol Pathol. 28:61–74.
1996.PubMed/NCBI
|
|
39
|
Duran B: The effects of long-term total
parenteral nutrition on gut mucosal immunity in children with short
bowel syndrome: a systematic review. BMC Nurs. 4:22005. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Silk DB and Gow NM: Postoperative
starvation after gastrointestinal surgery. Early feeding is
beneficial. BMJ. 323:761–762. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Cummings DE and Overduin J:
Gastrointestinal regulation of food intake. J Clin Invest.
117:13–23. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Chapman MJ, Nguyen NQ and Deane AM:
Gastrointestinal dysmotility: Evidence and clinical management.
Curr Opin Clin Nutr Metab Care. 16:209–216. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Go VL, Srihari P and Kamerman Burns LA:
Nutrition and gastroenteropancreatic neuroendocrine tumors.
Endocrinol Metab Clin North Am. 39:827–837. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
VanOoteghem G, ElMourad M, Slimani A,
Margos W, El Nawar A, Patris A, Gallez JF, Kirsch J, Hauters P,
Vallot F, et al: Is early enteral nutrition dangerous in acute non
surgical complicated diverticulitis? About 25 patients fed with
oral fiber free energetic liquid diet. Acta Gastroenterol Belg.
76:235–240. 2013.PubMed/NCBI
|