Introduction
Following total thyroidectomy, patients with
differentiated thyroid cancer (DTC) who are to receive
radioiodine-131 (I-131) therapy should be in a state of overt
hypothyroidism in order to achieve optimal therapeutic outcomes
(1). Such patients have low levels
of thyroid hormones and an increased level of thyroid-stimulating
hormone (TSH). Under these circumstances, the concentrations of
serum lipids are always elevated. Thyroid hormone is known to have
significant effects on lipid metabolism (2–4).
Although numerous studies have been conducted to assess the
association between thyroid dysfunction and hyperlipidemia
(4–9), to the best of our knowledge, this
association in DTC patients has never been investigated before. In
addition, previous studies have revealed that age and gender could
influence this association; however, the observations were not
consistent (9–12). The present study aimed to investigate
the correlation between thyroid function and lipid metabolic
profile in patients with DTC, with an focus on differences
resulting from different genders.
Materials and methods
Study population
The subjects studied were selected from the
hospitalized DTC patient data archive in the Department of Nuclear
Medicine of Tianjin Medical University General Hospital between
January 2010 and January 2014. The entry criteria were as follows:
DTC patients who had previously undergone total or near-total
thyroidectomy and were ready for I-131 therapy. The exclusion
criteria were as follows: Patients with coronary heart, chronic
liver and chronic renal diseases, uncontrolled diabetes mellitus
and those who had taken lipid-lowering drugs or other treatments
that potentially influenced the lipid profile. Information on the
medication and a history of previous diseases for each patient was
obtained in detail. In total, 352 DTC patients (89 males and 263
females) were included with adequate information for the analysis.
The gender– and age-matched healthy control participants (n=352)
were selected from the data archive in the Department of Health
Management in the General Hospital of Tianjin Medical University.
The control participants, who came to receive an annual health
checkup, had a normal thyroid profile and no history of any known
diseases.
Blood samples were obtained following overnight
fasting for the measurements of serum free triiodothyronine
(FT3), free thyroxine (FT4) and TSH using a
fully automated ADVIA Centaur analyzer (Siemens Healthcare
Diagnostics, Erlangen, Germany) by chemiluminescence. Total
cholesterol (TC), triglycerides (TG), low-density lipoprotein
cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C),
uric acid (UA) and fasting glucose (FG) levels were enzymatically
determined using an auto-analyzer (Hitachi Model 7170 analyzer;
Hitachi, Ltd., Tokyo, Japan). The weight and height were measured
in kilograms and centimeters, respectively. Furthermore, the body
mass index (BMI) was calculated as the weight divided by the height
squared.
For DTC patients, after I-131 therapy, thyroxine
replacement therapy was initiated. Levothyroxine sodium tablets
(Euthyrox; Merck KGaA, Darmstadt, Germany) was administered to all
DTC patients, with an individualized dose administered to anyone
for maintaining a suppressed TSH level. One month later,
re-assessments on the thyroid hormone levels and serum lipid levels
were performed. For this purpose, 157 DTC patients (36 males and
121 females) had adequate information for analysis.
The present study was ethically approved by the
Institutional Review Board of Tianjin Medical University General
Hospital, and the clinical investigation was conducted according to
the principles expressed in the Declaration of Helsinki. In
addition, informed consent was obtained from each of the
participants.
Diagnostic criteria and grouping
The diagnostic criteria for dyslipidemia were in
accordance with the National Cholesterol Education Program Adult
Treatment Panel III criteria as follows: TC ≥5.18 mmol/l, TG ≥1.70
mmol/l, LDL-C ≥3.37 mmol/l and HDL-C <1.04 mmol/l (13). All of the subjects were divided into
subgroups according to the serum TSH levels, namely: Subgroup 1,
subjects with a normal TSH level (<5 µIU/ml); subgroup 2,
subjects with a TSH level between 5 and 30 µIU/ml; and subgroup 3,
subjects with a TSH level >30 µIU/ml. Age groups included: Age
group 1, <30 years; group 2, 30–39 years; group 3, 40–49 years;
group 4, 50–59 years; and group 5, ≥60 years.
Statistical analysis
Data were presented as mean ± standard deviation.
Statistical analysis was performed with SPSS 19.0 (IBM SPSS,
Armonk, NY, USA), and the independent sample t-test was used to
compare parameter concentrations between the DTC and control group,
as well as prior to and following treatment with thyroxine. Pearson
bivariate correlations were calculated for TC, TG, LDL-C and HDL-C
with FT3, FT4 and TSH in different genders,
respectively. Furthermore, the odds ratio (OR) for hyperlipidemia
with 95% confidence intervals was calculated by binary logistic
regression models. P<0.05 was used to indicate a statistically
significant difference.
Results
Patient characteristics
The values of various parameters for subjects in the
DTC and control groups prior to I-131 therapy are reported in
Table I. There was no difference in
age between the two groups. Furthermore, the subjects in the DTC
group demonstrated significantly higher TSH levels and lower
thyroid hormone levels compared with those in the control group.
BMI, as well as serum TC, TG and LDL-C levels, were also
significantly higher in the DTC group than in the control
group.
 | Table I.Parameters of patients in the DTC and
control groups prior to I-131 therapy. |
Table I.
Parameters of patients in the DTC and
control groups prior to I-131 therapy.
| Parameters | DTC group
(n=352) | Control group
(n=352) |
|---|
| Male | 89 | 89 |
| Female | 263 | 263 |
| Age (years) | 48.73±12.81 | 48.75±12.78 |
| BMI
(kg/m2) |
25.92±3.49a | 25.16±3.93 |
| FT3
(pmol/l) |
2.08±0.71a | 5.07±0.49 |
| FT4
(pmol/l) |
5.62±2.06a | 15.93±2.12 |
| TSH (µIU/ml) |
84.26±45.33a | 2.53±1.40 |
| TC (mmol/l) |
6.63±1.39a | 5.04±0.97 |
| TG (mmol/l) |
2.25±1.82a | 1.46±0.92 |
| LDL-C (mmol/l) |
4.16±1.15a | 2.85±0.84 |
| HDL-C (mmol/l) | 1.59±0.44 | 1.56±0.40 |
| UA (µIU/ml) | 304.10±91.21 | 289.65±87.38 |
| FG (mmol/l) |
5.48±1.14a | 5.23±0.85 |
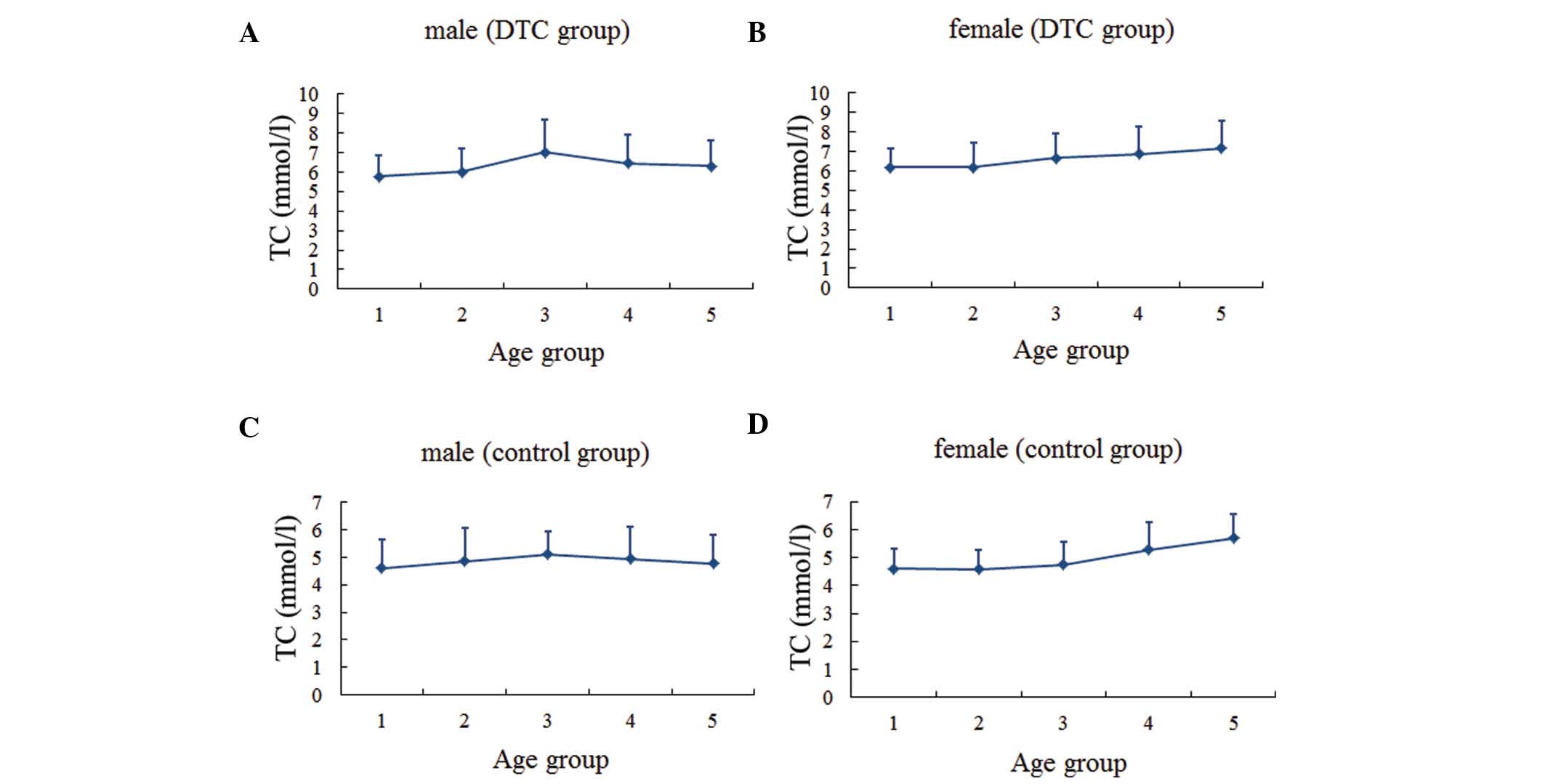
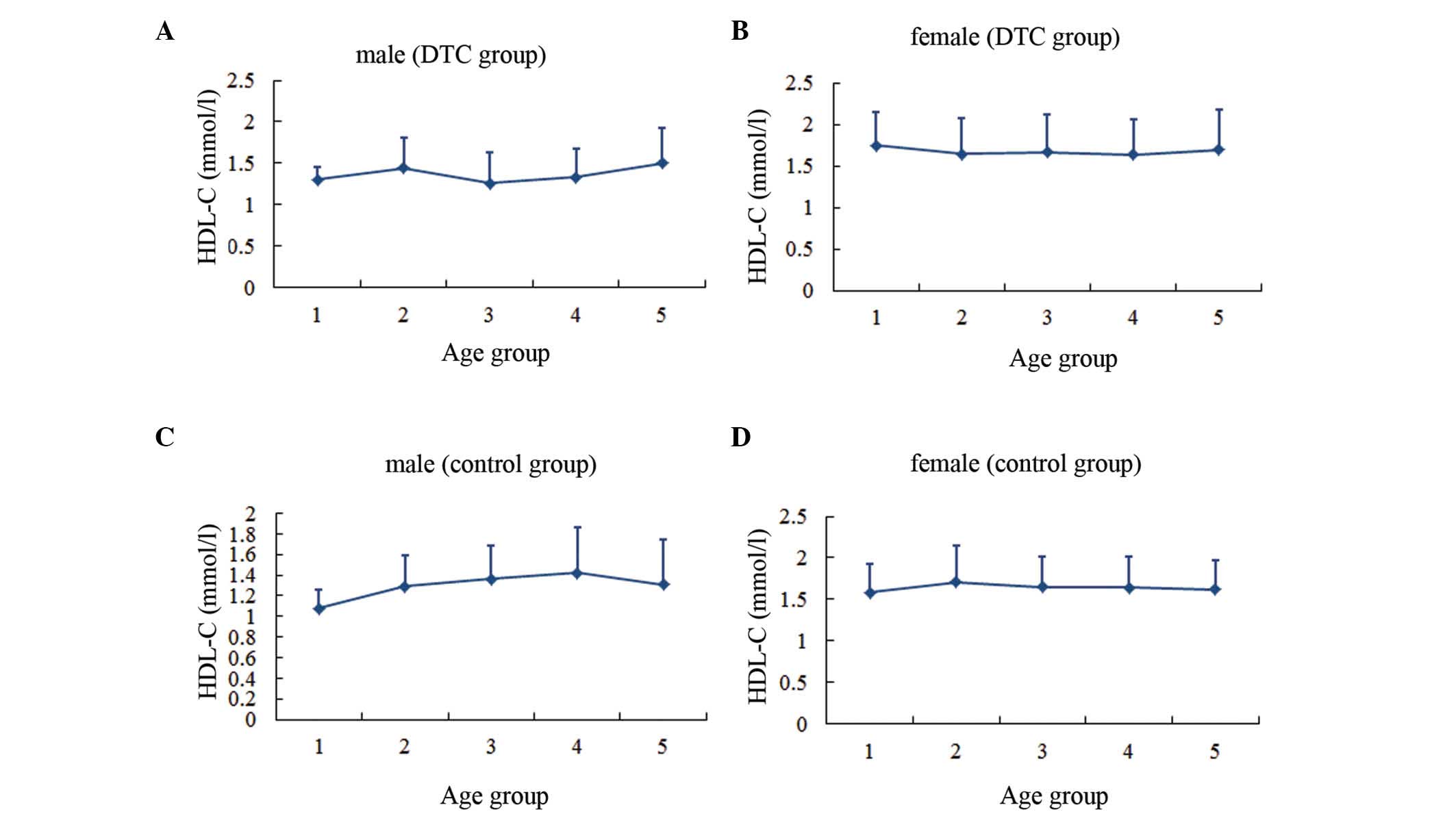
Serum lipid profiles
The serum lipid profiles for patients according to
gender and age group are presented (Figs. 1–4).
In males, the levels of TC and LDL-C in the two groups, as well as
the TG levels in the DTC group, reached the highest level for
individuals between the ages of 40 and 50 years, then gradually
decreased with age. By contrast, TG levels in the control group
were highest between the ages of 30 and 40 years, decreased over
the next two decades, and then increased with age. In females, the
TC and LDL-C levels increased gradually with age in both groups,
while the TG level tended to increase with age until the 50–60-year
age range in the DTC group.
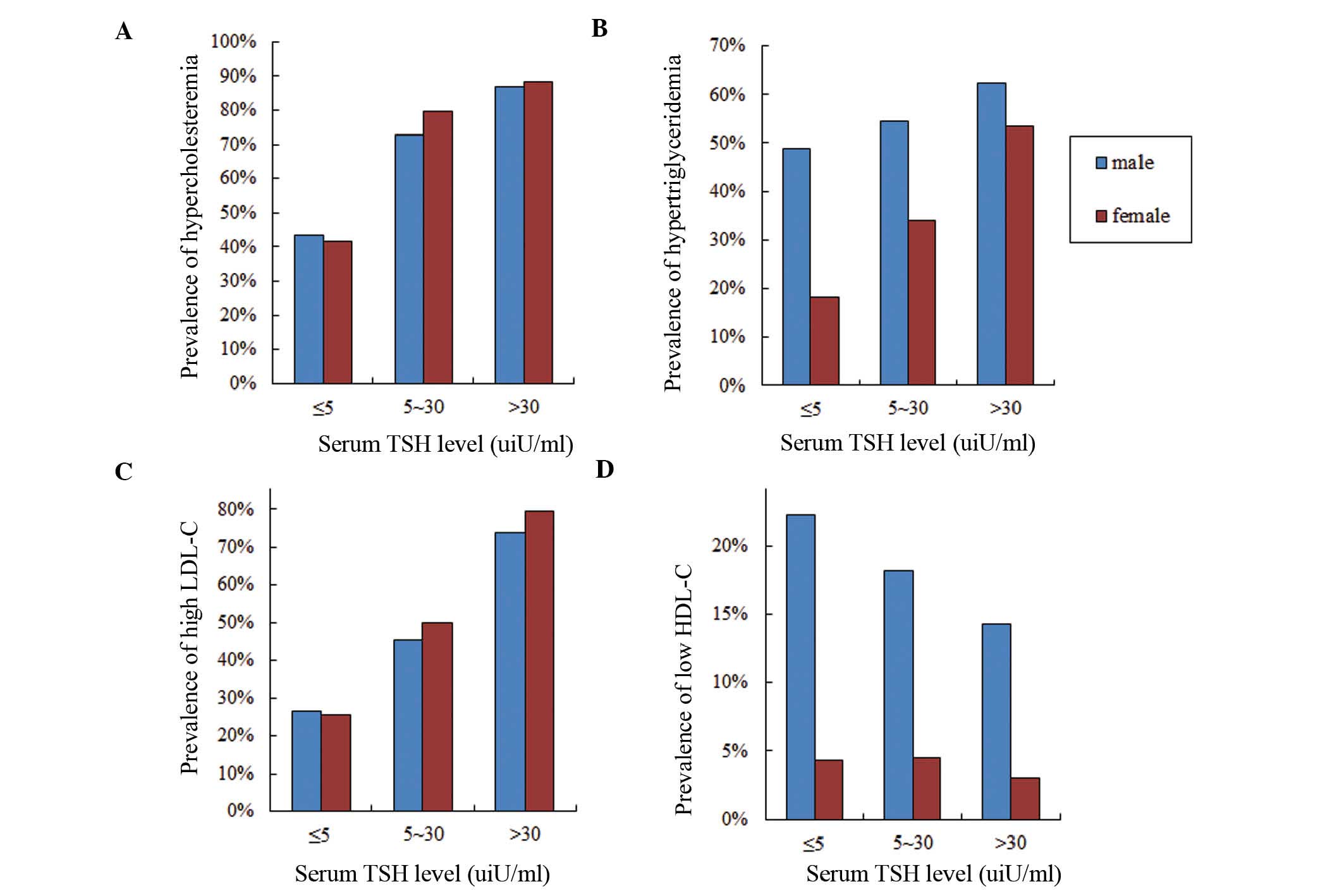
Dyslipidemia
Dyslipidemia prevalence was investigated in
different TSH subgroups in both genders (Fig. 5). Prevalences of hypercholesteremia
and high LDL-C in females were slightly higher compared with those
in males (TC, 65.02 vs. 64.05%; LDL-C, 50.95 vs. 48.32%). As the
serum TSH level increased, the prevalences of hypercholesteremia
and high LDL-C increased. In subgroup 1, the prevalences of
hypercholesteremia and high LDL-C in males (43.33 and 26.67%,
respectively) were slightly higher than those in females (41.73 and
25.59%, respectively). Furthermore, the prevalences of
hypercholesteremia and high LDL-C in females increased more than
those of males as the TSH level increased. By contrast, the
prevalences of hypertriglyceridemia and low HDL-C were
significantly higher in males compared with females (TG, 55.06 vs.
34.79%; HDL-C, 18.54 vs. 3.80%). The incidence of
hypertriglyceridemia rose as the serum TSH level increased,
however, the incidence of HDL-C was reduced.
Changes in parameters after thyroxine
treatment
Parameters prior to and 1 month following thyroxine
treatment are shown in Table II.
Significant changes could be observed in thyroid hormones and serum
lipid concentrations in all DTC patients. Following treatment, the
mean levels of serum TC, TG and LDL-C decreased by 1.77, 0.62 and
1.31 mmol/l respectively. Furthermore, the difference in HDL-C
levels between prior to and following treatment was not
significant.
| Table II.Parameters before and after 1 month
of thyroxine treatment. |
Table II.
Parameters before and after 1 month
of thyroxine treatment.
| Parameters | Before treatment
(n=157) | 1 Month after
treatment (n=157) |
|---|
| Male | 36 | 36 |
| Female | 121 | 121 |
| FT3
(pmol/l) |
2.01±0.73a | 5.19±0.92 |
| FT4
(pmol/l) |
5.38±2.33a | 19.44±4.30 |
| TSH (uIU/ml) |
86.65±43.50a | 7.27±14.61 |
| TC (mmol/l) |
6.96±1.29a | 5.19±1.10 |
| TG (mmol/l) |
2.25±1.40a | 1.63±1.05 |
| LDL-C (mmol/l) |
4.40±1.11a | 3.09±0.98 |
| HDL-C (mmol/l) | 2.69±12.80 | 1.40±0.52 |
Correlation analysis
Pearson bivariate correlation was performed in order
to assess the association between thyroid hormones and lipids
(Table III). This correlation
analysis was performed in all the subjects, including all DTC
patients and the normal controls. In both genders, a significant
negative correlation was observed between free thyroid hormones and
TC, TG or LDL-C levels. By contrast, there were significant
positive correlations between TSH and TC, TG or LDL-C levels. In
addition, a significant negative correlation between FT3
and HDL-C, and a significant positive correlation between TSH and
HDL-C were identified in females, which were not observed in
males.
| Table III.Pearson bivariate correlations (r)
between thyroid function and serum lipids. |
Table III.
Pearson bivariate correlations (r)
between thyroid function and serum lipids.
| Gender | TC | TG | LDL-C | HDL-C |
|---|
| Male (n=178) |
|
FT3 | −0.55a | −0.18a | −0.57a | −0.09 |
|
FT4 | −0.51a | −0.17a | −0.54a | −0.05 |
|
TSH | 0.50a | 0.28a | 0.52a | 0.01 |
| Female (n=526) |
|
FT3 | −0.62a | −0.33a | −0.59a | −0.10b |
|
FT4 | −0.58a | −0.32a | −0.55a | −0.06 |
|
TSH | 0.55a | 0.29a | 0.52a | 0.10b |
Dyslipidemia risk analysis
Finally, the risks of developing dyslipidemia in
different subgroups were investigated using binary logistic
regression (Table IV). This
analysis was performed in all DTC patients and the normal controls,
and TSH was designated as a categorical variable. Age, BMI, UA and
FG were taken as covariates. Significant differences were
demonstrated when subgroup data were compared in different genders.
By taking subgroup 1 as a reference, subjects of the other two
subgroups had a higher risk of developing dyslipidemia. The ORs of
high TC, TG and LDL-C increased progressively in both genders with
the increasing TSH values. For example, the ORs of developing high
TC in subgroup 2 were 3.30 in males and 4.60 in females. However,
in subgroup 3, the ORs were 9.40 in males and 13.12 in females. The
magnitude of gender differences was also examined. Firstly, the ORs
of dyslipidemia were higher in females compared with males.
Secondly, for males, only the ORs of developing high TC and LDL-C
had a statistical significance. However for females, the OR of
developing hypertriglyceridemia was also significant.
| Table IV.Likelihood of developing dyslipidemia
in different genders by the logistic regression model. |
Table IV.
Likelihood of developing dyslipidemia
in different genders by the logistic regression model.
| Gender | TC ≥5.18 mmol/l OR
(95% CI) | TG ≥1.7 mmol/l OR
(95% CI) | LDL-C ≥3.37 mmol/l
OR (95% CI) | HDL-C <1.04
mmol/l OR (95% CI) |
|---|
| Male (n=178) |
|
|
|
|
| TSH
subgroup 2 | 3.30
(0.78–13.92) | 1.35
(0.34–5.30) | 2.63
(0.67–10.29) | 0.72
(0.13–3.91) |
| TSH
subgroup 3 | 9.40a (4.17–21.15) | 1.83
(0.92–3.63) | 9.60a (4.53–20.35) | 0.50
(0.21–1.19) |
| Female (n=526) |
|
|
|
|
| TSH
subgroup 2 | 4.60a (2.05–10.30) | 1.85
(0.88–3.88) | 2.52a (1.27–4.97) | 1.08
(0.23–5.13) |
| TSH
subgroup 3 | 13.12a (7.74–22.25) | 5.50a (3.50–8.65) | 12.98a (8.11–20.78) | 0.68
(0.25–1.83) |
Discussion
It is well known that thyroid hormones affect lipid
metabolism. However, almost all the populations studied thus far
were suffering from benign thyroid diseases, including subclinical
hypothyroidism, and overt hypothyroid or hyperthyroid (4). The population in the present study
comprised DTC patients following partial or total thyroidectomy.
These DTC patients, who were ready to receive I-131 therapy were
put into a state of severe hypothyroidism from euthyroidism in a
short period of time. The aim of the present study was to estimate
the association between thyroid hormones and serum lipids in the
population studied, and to investigate whether the risk of
hyperlipidemia differed between genders.
Thyroid hormones and TSH have different effects on
lipid metabolism. Thyroid hormones affect serum lipid levels by
increasing the elimination of neutral sterols and bile acids
(2), and by reducing the absorption
of cholesterol in the intestines (14). Two animal studies have revealed that
thyroid hormones can stimulate the hepatic LDL-C receptor and
increase the removal of LDL-C from the circulation (2,3). Boone
et al (2) revealed that
thyroid hormones enhanced the cholesterol-accepting capacity of
serum via the ABCA1 transporter. Furthermore, Ness et al
(3) demonstrated that the
hypocholesterolemic effect of thyroid hormone resulted from the
expression of the hepatic cholesterol 7 α hydroxylase gene. Tan
et al (15) suggested that
thyroid hormones could increase the activity of hepatic lipase and
thereby reduce serum TC levels. However, TSH has an opposite effect
on the metabolism of lipids. In addition to thyroid cells, TSH
receptors are also expressed in many extrathyroidal tissues,
including the liver (16,17). TSH binds to the TSH receptor on
hepatocytes and stimulates the cyclic adenosine
monophosphate/protein kinase A/cyclic adenosine
monophosphate-responsive element binding protein signaling system.
In this way, TSH upregulates the expression of
3-hydroxy-3-methyl-glutaryl coenzyme A reductase, a rate-limiting
enzyme in cholesterol synthesis, which can modulate lipoprotein
metabolism and facilitate cholesterol uptake by the liver (7,16,17). Two
cross-sectional studies discovered that TSH levels were associated
with serum lipid profiles independent of thyroid hormones (7,17).
Furthermore, Wang et al (7)
observed that TSH levels induced a significant direct effect on TC
levels. Xu et al (17)
quantitatively demonstrated that each 1 µIU/ml increase in the TSH
level tended to elevate the TC level by 0.016 mmol/l.
In the current study, DTC patients who required
I-131 therapy following partial or total thyroidectomy did not take
thyroxine medication. During this phase, some acute changes
occurred in the serum parameters, including dyslipidemia (18). The present study revealed significant
negative correlations between free thyroid hormones and serum TC,
TG or LDL-C levels, as well as significant positive correlations
between TSH and serum TC, TG or LDL-C levels. Furthermore, the risk
of developing dyslipidemia due to high TSH level was identified as
gender-related. Moreover, the ORs for dyslipidemia were
significantly higher in females than in males. Therefore, the
results of the present study indicate that sex hormones may be an
important contributor to this phenomenon. Tognini et al
(9) also found that gender
substantially influenced the association between thyroid status and
serum lipid levels, and their results were in agreement with those
of the present study.
With regard to the mechanism of different sex
hormones' effects on lipid metabolism, testosterone and estradiol
have different roles, which can be summarized as described below.
First, lipoprotein lipase (LPL) and hepatic lipase (HL) are the
major lipolytic enzymes of the lipoprotein metabolism. These
enzymes remove TG from the bloodstream and decrease the serum
chylomicron levels. Androgens stimulate HL activity, however,
estrogens inhibit the HL and LPL activities (19). Secondly, testosterone increases
lipolysis by stimulating β-adrenergic activity (20). Thirdly, testosterone upregulates
genes responsible for HDL-C catabolism, and increases the activity
of both hepatic lipase and scavenger receptor BI (SR-BI).
Furthermore, SR-BI increases the uptake of lipids into hepatocytes
and enhances cholesterol efflux from peripheral cells (21,22).
Finally, estrogen is capable of increasing cholesterol and LDL-C
levels, and these metabolic effects appear to be mediated by
estrogen receptor α (23).
Clinically, low levels of testosterone and high
levels of estrogen are associated with unfavorable lipid levels
(22,24). Haffner et al (25) demonstrated that serum testosterone
was inversely correlated with TC, TG and LDL-C, yet positively
correlated with HDL-C. Several meta-analyses with the topic of the
changes in lipoprotein profiles resulting from exogenous
testosterone administration have been conducted (26–28). For
instance, Whitsel et al (26)
performed such a meta-analysis by analyzing 19 studies, and
demonstrated that the intramuscular administration of testosterone
esters to hypogonadal males was associated with a dosage-dependent
reduction of TC and LDL-C levels. By contrast, considering
estrogen, Wranicz et al (29)
revealed a significantly positive correlation between estradiol
levels and serum TC, TG and LDL-C levels. Ott et al
(30) performed a study to explore
the change of serum lipid levels of transsexuals after cross-gender
therapy, and significant increases of TC, TG and HDL-C were
identified in male to female transsexuals. Another study
demonstrated that the estradiol concentration in males had a
significant negative correlation with HDL-C concentration and a
significant positive correlation with the TG level (31).
In conclusion, the present study had both strengths
and weaknesses. The uniqueness of the study was that it focused
attention on the correlation between TSH and serum lipid profiles
in terms of different genders in DTC patients. However, due to the
prevalence of DTC in females being higher than that in males, the
number of males in the present study was relatively small. Another
potential limitation of the present study was the lack of
information on lifestyle choices of the patients, such as smoking
or eating habits. This may affect the accuracy of the results.
However, the careful exclusion of patients receiving lipid-lowering
drugs and other treatments that have the potential to influence the
lipid profile improved the statistical power. Finally, since
hyperlipemia is known as a risk factor for cardiovascular diseases,
whether a short-term increase of serum lipids during the thyroid
hormone withdrawal period will increase the risk of cardiovascular
diseases requires further investigation.
In summary, the present study systematically
analyzed the association between the serum TSH profile and serum
lipid levels in DTC patients, and the influence of different
genders on this correlation. Furthermore, DTC patients after
thyroidectomy were demonstrated to be in a severe state of
hypothyroidism, which increased the risk of dyslipidemia. In
addition, female patients were shown to have a higher risk of
dyslipidemia compared with males.
Acknowledgements
This study was supported by the National Key
Clinical Specialty Project (awarded to the Departments of Nuclear
Medicine and Radiology). This study was supported by Tianjin
Medical University General Hospital New Century Excellent Talent
Program; Young and Middle-aged Innovative Talent Training Program
from Tianjin Education Committee; and Talent Fostering Program (the
131 Project) from Tianjin Education Committee, Tianjin Human
Resources and Social Security Bureau (awarded to Zhaowei Meng).
This study was also supported by China National Natural Science
Foundation (grant no. 81571709) and the Key Project of Tianjin
Science and Technology Committee Foundation (grant no.
16JCZDJC34300; awarded to Zhaowei Meng).
Glossary
Abbreviations
Abbreviations:
|
TSH
|
thyroid-stimulating hormone
|
|
DTC
|
differentiated thyroid cancer
|
|
TC
|
total cholesterol
|
|
TG
|
triglycerides
|
|
HDL-C
|
high-density lipoprotein
cholesterol
|
|
LDL-C
|
low-density lipoprotein
cholesterol
|
|
FT3
|
free triiodothyronine
|
|
FT4
|
free thyroxine
|
|
UA
|
uric acid
|
|
FG
|
fasting glucose
|
|
BMI
|
body mass index
|
|
OR
|
odds ratio
|
|
LPL
|
lipoprotein lipase
|
|
HL
|
hepatic lipase
|
|
SR-BI
|
scavenger receptor BI
|
References
|
1
|
American Thyroid Association (ATA)
Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid
Cancer; Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel
SJ, Mazzaferri EL, McIver B, Pacini F, Schlumberger M, et al:
Revised American Thyroid Association management guidelines for
patients with thyroid nodules and differentiated thyroid cancer.
Thyroid. 19:1167–1214. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Boone LR, Lagor WR, Mde L Moya, Niesen MI,
Rothblat GH and Ness GC: Thyroid hormone enhances the ability of
serum to accept cellular cholesterol via the ABCA1 transporter.
Atherosclerosis. 218:77–82. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ness GC, Pendleton LC, Li YC and Chiang
JY: Effect of thyroid hormone on hepatic cholesterol 7 alpha
hydroxylase, LDL receptor, HMG-CoA reductase, farnesyl
pyrophosphate synthetase and apolipoprotein A-I mRNA levels in
hypophysectomized rats. Biochem Biophys Res Commun. 172:1150–1156.
1990. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Walsh JP, Bremner AP, Bulsara MK, O'leary
P, Leedman PJ, Feddema P and Michelangeli V: Thyroid dysfunction
and serum lipids: A community-based study. Clin Endocrinol (Oxf).
63:670–675. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bauer DC, Ettinger B and Browner WS:
Thyroid functions and serum lipids in older women: A
population-based study. Am J Med. 104:546–551. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Chubb SA, Davis WA and Davis TM:
Interactions among thyroid function, insulin sensitivity and serum
lipid concentrations: The Fremantle diabetes study. J Clin
Endocrinol Metab. 90:5317–5320. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wang F, Tan Y, Wang C, Zhang X, Zhao Y,
Song X, Zhang B, Guan Q, Xu J, Zhang J, et al: Thyroid-stimulating
hormone levels within the reference range are associated with serum
lipid profiles independent of thyroid hormones. J Clin Endocrinol
Metab. 97:2724–2731. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Meier C, Staub JJ, Roth CB, Guglielmetti
M, Kunz M, Miserez AR, Drewe J, Huber P, Herzog R and Müller B:
TSH-controlled L-thyroxine therapy reduces cholesterol levels and
clinical symptoms in subclinical hypothyroidism: A double blind,
placebo-controlled trial (Basel Thyroid Study). J Clin Endocrinol
Metab. 86:4860–4866. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Tognini S, Polini A, Pasqualetti G, Ursino
S, Caraccio N, Ferdeghini M and Monzani F: Age and gender
substantially influence the relationship between thyroid status and
the lipoprotein profile: Results from a large cross-sectional
study. Thyroid. 22:1096–1103. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bindels AJ, Westendorp RG, Frölich M,
Seidell JC, Blokstra A and Smelt AH: The prevalence of subclinical
hypothyroidism at different total plasma cholesterol levels in
middle aged men and women: A need for case-finding? Clin Endocrinol
(Oxf). 50:217–220. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Iqbal A, Jorde R and Figenschau Y: Serum
lipid levels in relation to serum thyroid-stimulating hormone and
the effect of thyroxine treatment on serum lipid levels in subjects
with subclinical hypothyroidism: The Tromsø study. J Intern Med.
260:53–61. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Boekholdt SM, Titan SM, Wiersinga WM,
Chatterjee K, Basart DC, Luben R, Wareham NJ and Khaw KT: Initial
thyroid status and cardiovascular risk factors: The EPIC-Norfolk
prospective population study. Clin Endocrinol (Oxf). 72:404–410.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
National Cholesterol Education Program
(NCEP) Expert Panel on Detection, Evaluation, and Treatment of High
Blood Cholesterol in Adults (Adult Treatment Panel III), . Third
Report of the National Cholesterol Education Program (NCEP) Expert
Panel on Detection, Evaluation and Treatment of High Blood
Cholesterol in Adults (Adult Treatment Panel III) final report.
Circulation. 106:3143–3421. 2002.PubMed/NCBI
|
|
14
|
Gälman C, Bonde Y, Matasconi M, Angelin B
and Rudling M: Dramatically increased intestinal absorption of
cholesterol following hypophysectomy is normalized by thyroid
hormone. Gastroenterology. 134:1127–1136. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Tan KC, Shiu SW and Kung AW: Plasma
cholesteryl ester transfer protein activity in hyper- and
hypothyroidism. J Clin Endocrinol Metab. 83:140–143. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Tian L, Song Y, Xing M, Zhang W, Ning G,
Li X, Yu C, Qin C, Liu J, Tian X, et al: A novel role for
thyroid-stimulating hormone: Up-regulation of hepatic
3-hydroxy-3-methyl-glutarylcoenzyme A reductase expression through
the cyclic adenosine monophosphate/protein kinase A/cyclic
adenosine monophosphate-responsive element binding protein pathway.
Hepatology. 52:1401–1409. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Xu C, Yang X, Liu W, Yuan H, Yu C, Gao L
and Zhao J: Thyroid stimulating hormone, independent of thyroid
hormone, can elevate the serum total cholesterol level in patients
with coronary heart disease: A cross-sectional design. Nutr Metab
(Lond). 9:442012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Regalbuto C, Alagona C, Maiorana R, Di
Paola R, Cianci M, Alagona G, Sapienza S, Vigneri R and Pezzino V:
Acute changes in clinical parameters and thyroid function
peripheral markers following L-T4 withdrawal in patients totally
thyroidectomized for thyroid cancer. J Endocrinol Invest. 29:32–40.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Agledahl I, Skjaerpe PA, Hansen JB and
Svartberg J: Low serum testosterone in men is inversely associated
with non-fasting serum triglycerides: The Tromsø study. Nutr Metab
Cardiovasc Dis. 18:256–262. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Haffner SM and Valdez RA: Endogenous sex
hormones: Impact on lipids, lipoproteins and insulin. Am J Med.
98:40S–47S. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Langer C, Gansz B, Goepfert C, Engel T,
Uehara Y, von Dehn G, Jansen H, Assmann G and von Eckardstein A:
Testosterone up-regulates scavenger receptor BI and stimulates
cholesterol efflux from macrophages. Biochem Biophys Res Commun.
296:1051–1057. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Monroe AK and Dobs AS: The effect of
androgens on lipids. Curr Opin Endocrinol Diabetes Obes.
20:132–139. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Pellegrini M, Pallottini V, Marin R and
Marino M: Role of the sex hormone estrogen in the prevention of
lipid disorder. Curr Med Chem. 21:2734–2742. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Mäkinen JI, Perheentupa A, Irjala K,
Pöllänen P, Mäkinen J, Huhtaniemi I and Raitakari OT: Endogenous
testosterone and serum lipids in middle-aged men. Atherosclerosis.
197:688–693. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Haffner SM, Mykkänen L, Valdez RA and Katz
MS: Relationship of sex hormones to lipids and lipoproteins in
nondiabetic men. J Clin Endocrinol Metab. 77:1610–1615. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Whitsel EA, Boyko EJ, Matsumoto AM,
Anawalt BD and Siscovick DS: Intramuscular testosterone esters and
plasma lipids in hypogonadal men: A meta-analysis. Am J Med.
111:261–269. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Calof OM, Singh AB, Lee ML, Kenny AM,
Urban RJ, Tenover JL and Bhasin S: Adverse events associated with
testosterone replacement in middle-aged and older men: A
meta-analysis of randomized, placebo-controlled trials. J Gerontol
A Biol Sci Med Sci. 60:1451–1457. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Isidori AM, Giannetta E, Greco EA,
Gianfrilli D, Bonifacio V, Isidori A, Lenzi A and Fabbri A: Effects
of testosterone on body composition, bone metabolism and serum
lipid profile in middle-aged men: A meta-analysis. Clin Endocrinol
(Oxf). 63:280–293. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Wranicz JK, Cygankiewicz I, Rosiak M, Kula
P, Kula K and Zareba W: The relationship between sex hormones and
lipid profile in men with coronary artery disease. Int J Cardiol.
101:105–110. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Ott J, Aust S, Promberger R, Huber JC and
Kaufmann U: Cross-sex hormone therapy alters the serum lipid
profile: A retrospective cohort study in 169 transsexuals. J Sex
Med. 8:2361–2369. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Yasui T, Uemura H, Irahara M, Arai M,
Kojimahara N, Okabe R, Ishii Y, Tashiro S and Sato H: Associations
of endogenous sex hormones and sex hormone-binding globulin with
lipid profiles in aged Japanese men and women. Clin Chim Acta.
398:43–47. 2008. View Article : Google Scholar : PubMed/NCBI
|