Introduction
Multiple myeloma is the second most common
hematological malignancy, with an incidence of 3.29–4.82 cases per
100,000 individuals a year globally, an incidence that is
increasing due to population ageing (1). The proteasome inhibitor bortezomib was,
at first use, applied to a relapsed or refractory multiple myeloma
(MM) at a 1.3 mg/m2 dose, twice per week (2). It then demonstrated its efficacy via
>10 years of clinical use (2,3).
Bortezomib acts upon multiple myeloma by affecting signaling
cascades, leading to a toxic buildup of misfolded proteins
(4,5). However, the precise mechanism
underlying the action of this agent has yet to be fully elucidated.
Intravenous injection was previously the standard way of
administering bortezomib (2), but
subcutaneous administration is increasingly common in the treatment
of MM due to the comparative efficacy and improved safety profile
of this method of administration, particularly with regard to the
lower incidence and severity of peripheral neuropathy (PN). PN
primarily affects the sensory nerves, causing symptoms such as a
burning sensation, loss of response to external stimuli,
paresthesia, discomfort or neuralgia, interfering with patient
quality-of-life (6). Use of a single
agent, bortezomib, prolonged the median time of progression of MM
from 3 to 9 months (3,7). Furthermore, it has been revealed that
bortezomib-based combination chemotherapy has an improved efficacy
from that of bortezomib alone (2).
However, the resultant PN following combination therapy, which
includes agents such as thalidomide, is of key importance to
address (8). Thalidomide is popular
in MM treatment due to its low cost and efficacy profile; this drug
suppresses vascular regeneration, improves immune regulation and
interferes with the protective bone marrow microenvironment
surrounding myeloma cells, promoting apoptosis of tumor cells. PN
resulting from thalidomide treatment is common (8,9).
Bortezomib-thalidomide-dexamethasone (VTD) is one of the most
common chemotherapy regimens; however, the systemic safety profile,
particularly regarding the inevitable PN, requires additional
attention. In the present study, the incidence of PN following
treatment with subcutaneous bortezomib and its efficacy when
combined with thalidomide was retrospectively analyzed.
Patients and methods
Patients and methods
The present study was approved by the Ethics
Committee of the Affiliated Hospital of Nantong University,
Nantong, China, and written informed consent was obtained from the
patient or patients' families. The clinical data of 81 patients (37
subcutaneously administered and 44 intravenously administered
treatment) of newly diagnosed (n=77) or refractory (n=4) MM
following 1–3 prior therapies were comprehensively analyzed. These
patients were all admitted to the Affiliated Hospital of Nantong
University, Nantong, China between September 2011 and February
2014. All patients received a 21-day cycle of 1.3 mg/m2
bortezomib (Takeda Oncology, Cambridge, MA, USA) on days 1, 4, 8
and 11 by subcutaneous injection (scBor) or intravenous infusion
(ivBor), 75–125 mg thalidomide (Changzhou Pharmaceutical Factory,
Jiangsu, China) daily and 20 mg dexamethasone (Wuhan Yuancheng
Pharmaceutical Co., Ltd., Hubei, China) on days 1, 2, 4, 5, 8, 9,
11 and 12. Neuroprotective therapy, including fursultimine or
mecobalamine was administered upon the development of PN. The
patients were administered the recommended scBor concentration
(3) of 2.5 mg/ml (1.75 mg bortezomib
reconstituted with 0.7 ml normal 0.9% saline) or 1.0 mg/ml ivBor.
The subcutaneous injection sites were the thighs and the abdomen,
regularly switching side of injection to prevent injection site
reaction (ISR). All patients provided written informed consent.
Baseline demographics, disease characteristics and chemotherapy
regimens were comparable between the two treatment groups (Table I; P>0.05 for all baseline
demographics).
 | Table I.Patient demographics and number of
cases demonstrating specific characteristics. |
Table I.
Patient demographics and number of
cases demonstrating specific characteristics.
| Characteristic | Subcutaneous
bortezomib (n=37 patients) | Intravenous
bortezomib (n=44 patients) |
|---|
| Age, years
(range) | 63 (43–85) | 64 (36–83) |
| Age ≥65
years | 15 (40.5%) | 18 (40.9%) |
| Male patients | 28 (75.7%) | 31 (70.5%) |
| Newly diagnosed
patients | 35 (94.6%) | 38 (86.4%) |
| Myeloma type |
|
|
| IgG | 15 (40.5%) | 17 (38.6%) |
| IgA | 11 (29.7%) | 13 (29.5%) |
| IgD | 0 (0.0%) | 2 (4.5%) |
| IgM | 2 (5.4%) | 2 (4.5%) |
| Light
chain | Lam5 (13.5%), kap4
(10.8%) | Lam6 (13.6%), kap4
(9.1%) |
| ISS stage |
| I–II | 15 (40.5%) | 17 (38.6%) |
| III | 22 (59.5%) | 27 (61.4%) |
| No. patients with
lytic bone lesions | 24 (64.9%) | 29 (65.9%) |
| Serum albumin, g/l
(range) | 34.3 (20–40) | 32.5 (21–38) |
| Plasma β2
microglobulin, mg/l (range) | 4.58 (2.9–23) | 5.77 (1.8–26.5) |
| No. patients using
cyclophosphamide | 13 (35.1%) | 15 (34.1%) |
| Renal
insufficiency | 6 (16.2%) | 9 (20.5%) |
| Diabetes | 3 (8.1%) | 5 (11.4%) |
| Diabetic neuropathy,
grade 1 | 1 (2.7%) | 2 (4.5%) |
The response and progression were assessed by the
International Myeloma Working Group criteria (10). Adverse events (AEs) were assessed
according to the National Cancer Institute Common Terminology
Criteria for AEs version 3.0 (11).
The primary aim of this was to investigate the comparative
incidence of PN, and the comparative efficacy, following treatment
with scBor and ivBor. Grading of neuropathic pain, a symptom of PN,
was as follows: Grade 1, pain not interfering with functioning;
grade 2, moderate pain, in which pain or analgesics are interfering
with functioning, but not interfering with activities of daily
living (ADL); grade 3, severe pain, in which pain or analgesics are
severely interfering with ADL; grade 4, disabling pain (11). Efficacy was predominantly determined
by the complete remission rate or very good partial remission
(CR/VGPR) (10), progression-free
survival and overall survival rate (OS) after a median follow-up
time of 13 (6–16) and 16 months (3–19) in the
scBor and ivBor groups, respectively.
Sprague Dawley (SD) rat model
Due to an absence of evidence of PN histopathology
in patients, an in vivo model of PN was established in adult
SD rats. A total of 18 SD female rats (weight, 200±5 g; age, 2
months; sourced from the Animal Laboratory, Nantong University,
Nantong, China) were randomly assigned to 6 groups of 3 rats as
follows: i) scBor; ii) ivBor; iii) scBor combined with thalidomide;
iv) ivBor combined with thalidomide; v) thalidomide only; and vi)
untreated control group. These rats were maintained at 24°C with a
12/12 h light:dark cycle, and were administered food and water at
regular intervals. A dose of 1.3 mg/m2 (0.2 mg/kg)
bortezomib (Takeda Oncology) was administered to the relevant
groups on days 1, 4, 8 and 11, and 100 mg (10.5 mg/kg) thalidomide
(Changzhou Pharmaceutical Factory) was administered daily to the
relevant groups. Bortezomib was administered via subcutaneous
abdominal or tail vein injection, and thalidomide was administered
orally. On the 14th day of treatment, rats were
sacrificed by cervical dislocation and sciatic nerve samples were
extracted by the Animal Laboratory, Nantong University,. These were
examined to determine changes with transmission electron microscopy
(TEM).
Statistical methods
Data analysis was performed with the Statistical
Package for Social Science software (SPSS version 17.0; SPSS, Inc.,
Chicago, IL, USA). Continuous variables are expressed as median and
range and were compared using a t-test. Categorical variables are
reported as percentages and compared using a χ2 test.
Overall survival rate, determined from diagnosis to mortality, was
estimated by the Kaplan-Meier method and curve comparison was
conducted using log-rank analysis. P<0.05 was considered to
indicate a statistically significant difference.
Results
The median number of cycles of bortezomib
administered to patients were 5.5 (3–8) and 6
(3–10) in the scBor and ivBor groups,
respectively. This included 33 of 37 (89.2%) scBor-treated patients
that had completed ≥4 cycles of treatment, with comparable numbers
of 40 of 44 (90.9%) patients administered ivBor. Patients who had
PN or neuropathic pain of grade ≥2 (10) at baseline were excluded from the
study. Among the 37 and 44 participating patients, 28 (75.6%) and
37 (84.1%) achieved VGPR or better (P=0.350), including 13 (35.1%)
and 17 (38.6%) with CR, from the scBor and ivBor groups,
respectively (P=0.749). The median time to reach VGPR was 2 months
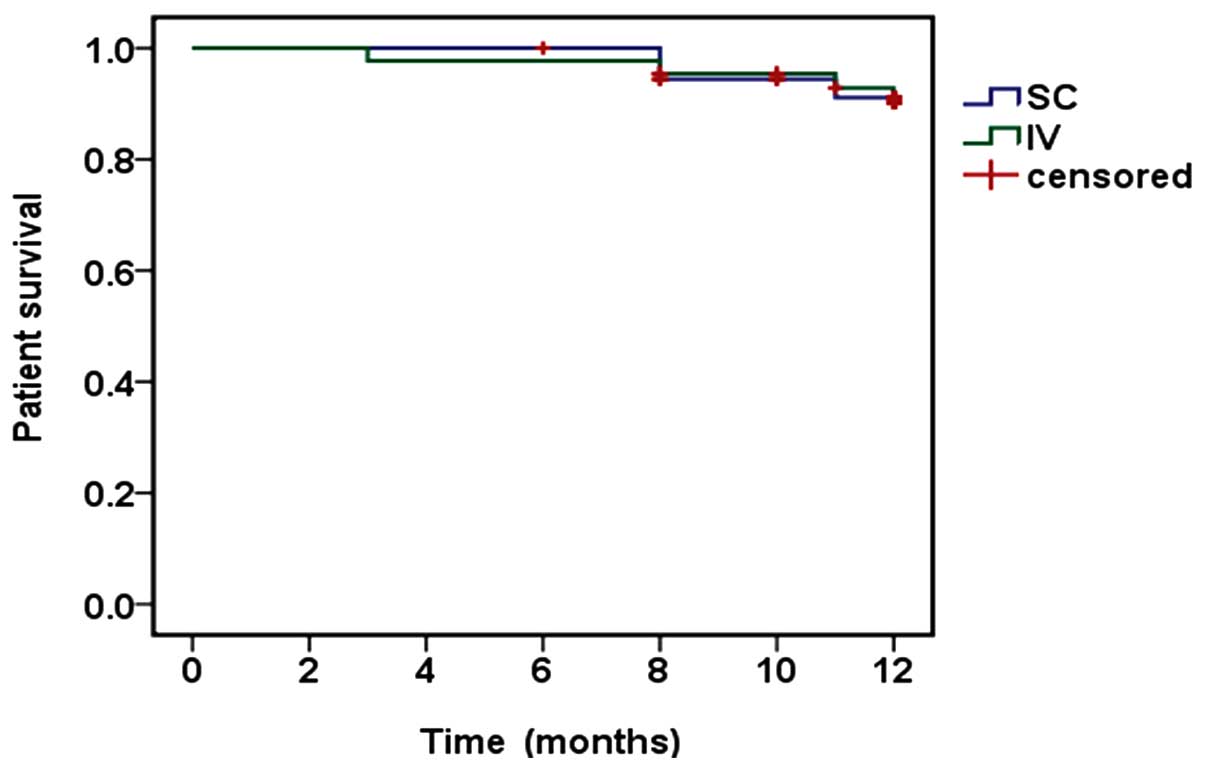
in both groups. At the final time point, 3 years after the study
commencement, 34 (91.9%) and 40 (90.9%) patients survived for ≥1
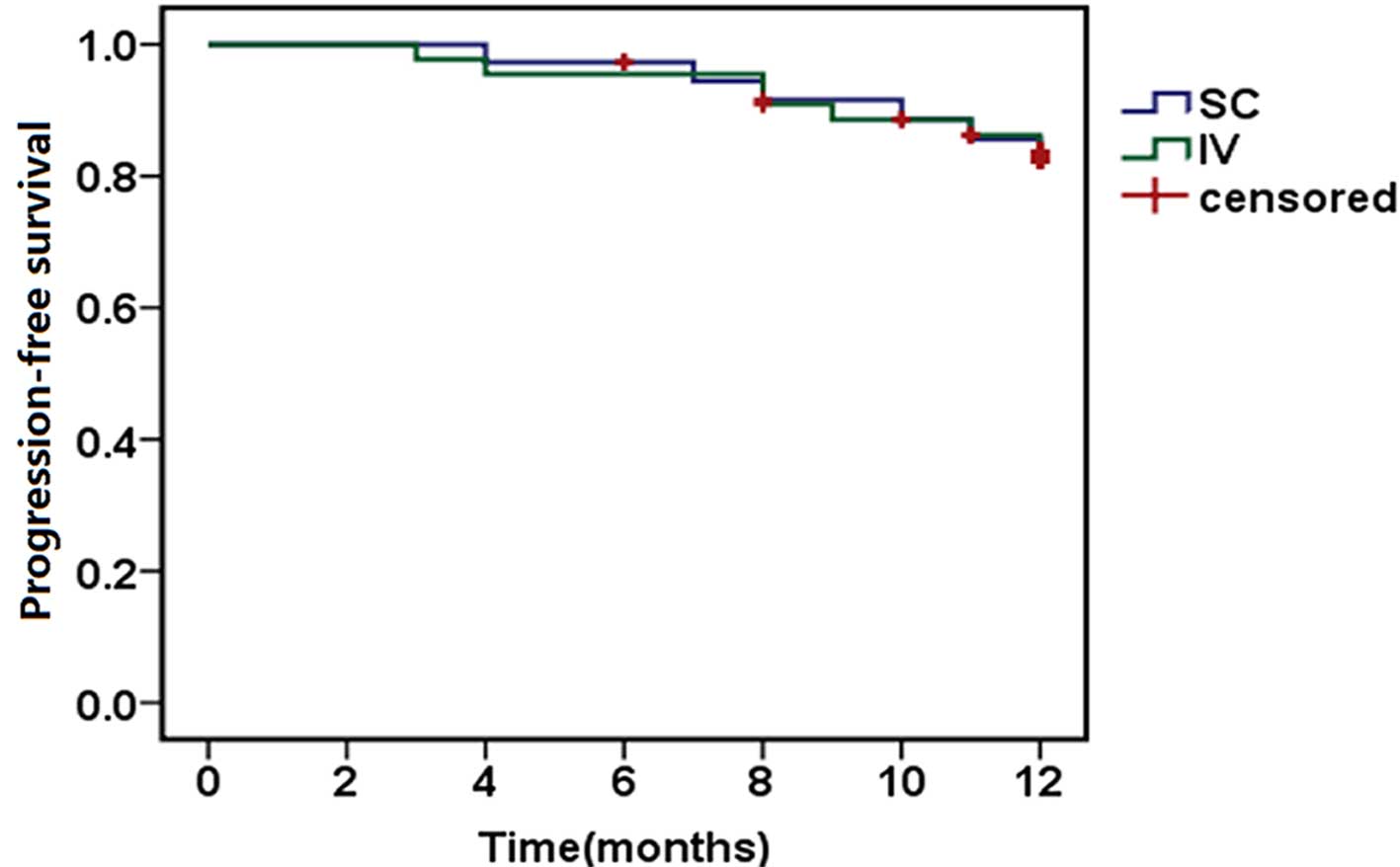
year (P=0.926; Fig. 1) and 31
(83.8%) and 37 (84.1%) reached 1-year progression-free survival
(P=0.921; Fig. 2), in the scBor and
ivBor groups, respectively. It is of note that 6 patients (2 scBor
and 4 ivBor) succumbed to MM by the end of the study. These data
collectively suggest an equivalent efficacy of bortezomib
administered by either route.
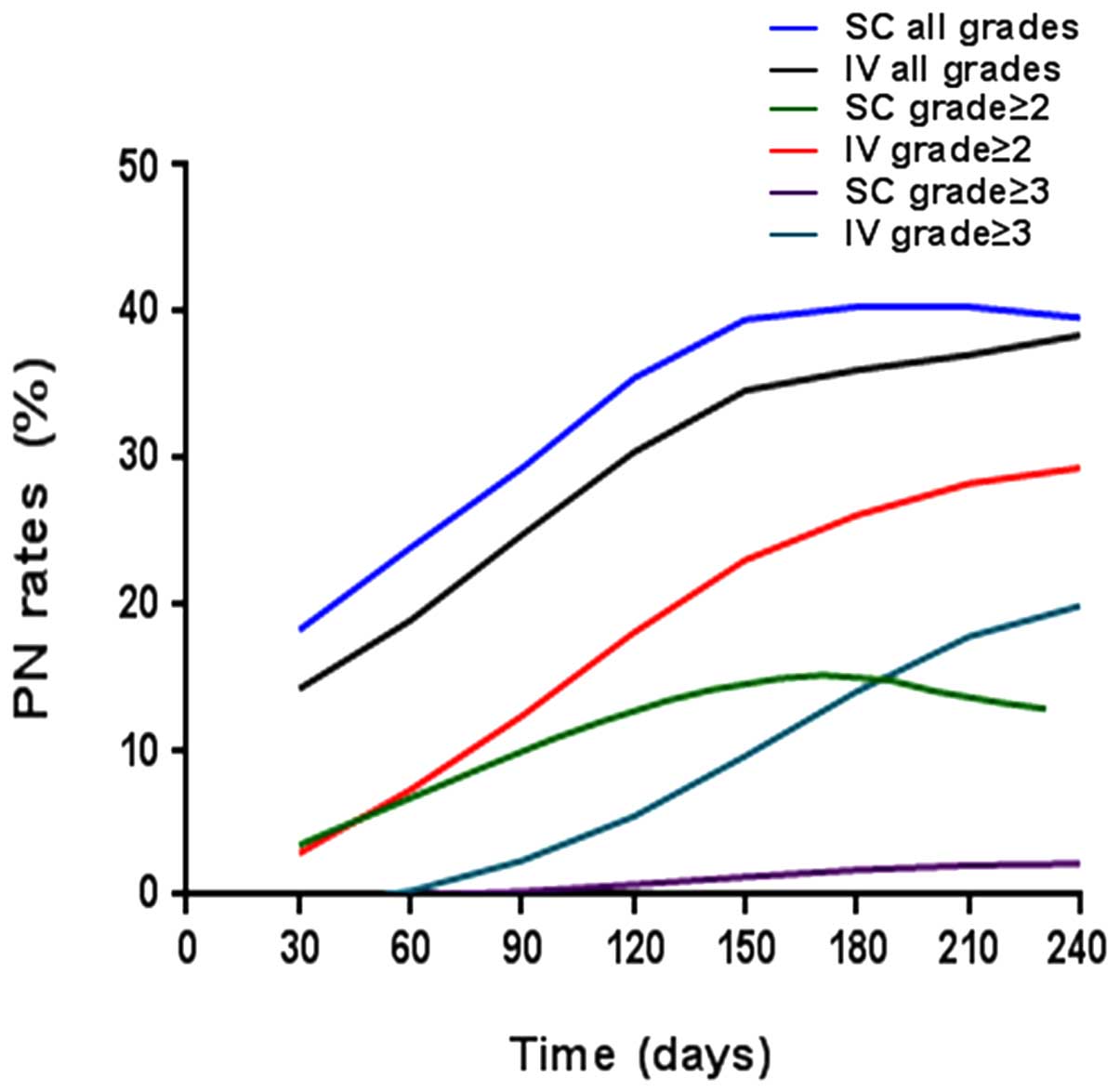
Following supplementation with thalidomide and
dexamethasone, the incidence of PN, the most detrimental adverse
event, arising due to the treatment remained lower in the
scBor-treated group than the ivBor-treated group (all cases: 51.3
vs. 61.3%, P=0.371; grade ≥2: 35.1 vs. 56.8%, P=0.052; grade ≥3:
2.7 vs. 20.5%, P=0.015, respectively; Fig. 3). Following treatment with
thalidomide, the median time until onset of any grade of PN was 3.0
(1–7)
and 4.0 (1–10) months, median time until onset of
grade ≥2 was 3.5 (2–11) and 4.0 (2–12) months
in the scBor and ivBor groups, respectively, and time until the
onset of grade ≥3 PN was 5.5 (4–10) months
in the ivBor group (as no patients demonstrated grade ≥3 PN in the
scBor group). In the scBor and ivBor groups, 28 (75.7%) and 29
(65.9%) patients, respectively, were additionally administered
fursultimine or mecobalamine upon the development of PN. A total of
0 and 3 (6.8%) patients in the scBor and ivBor groups,
respectively, discontinued thalidomide use or were administered a
reduced dose of 50 mg thalidomide for ~1 month to prevent or
attenuate severe PN. Other common side effects were
thrombocytopenia, anemia and feeble and gastrointestinal symptoms,
including nausea and vomiting (Table
II).
| Table II.Hematology parameters and rate of
other adverse events, expressed as no. cases (% of total
cases). |
Table II.
Hematology parameters and rate of
other adverse events, expressed as no. cases (% of total
cases).
|
| Subcutaneous
bortezomib (n=37 patients) | Intravenous
bortezomib (n=44 patients) |
|---|
|
|
|
|
|---|
| Side effects | All grades | Grade ≥3 | All grades | Grade ≥3 |
|---|
| Hematology
laboratory data |
|
|
|
|
| White
blood cell count | 19 (51.4%) | 2 (5.4%) | 20 (45.5%) | 9 (20.5%) |
|
Hemoglobin level decrease | 28 (75.7%) | 17 (45.9%) | 35 (79.5%) | 22 (50.0%) |
|
Platelet count decrease | 17 (45.9%) | 9 (24.3%) | 26 (59.1%) | 17 (38.6%) |
| Diarrhea | 4 (10.8%) | 0 (0.0%) | 5 (11.4%) | 0 (0.0%) |
| Abdominal
bloating | 4 (10.8%) | 0 (0.0%) | 7 (15.9%) | 0 (0.0%) |
|
Nausea/vomiting | 7 (18.9%) | 0 (0.0%) | 9 (20.5%) | 0 (0.0%) |
| Constipation | 13 (35.1%) | 0 (0.0%) | 15 (34.1%) | 2 (4.5%) |
| Fatigue | 17 (45.9%) | 2 (5.4%) | 29 (65.9%) | 3 (6.8%) |
| Fever | 7 (18.9%) | 0 (0.0%) | 10 (22.7%) | 2 (4.5%) |
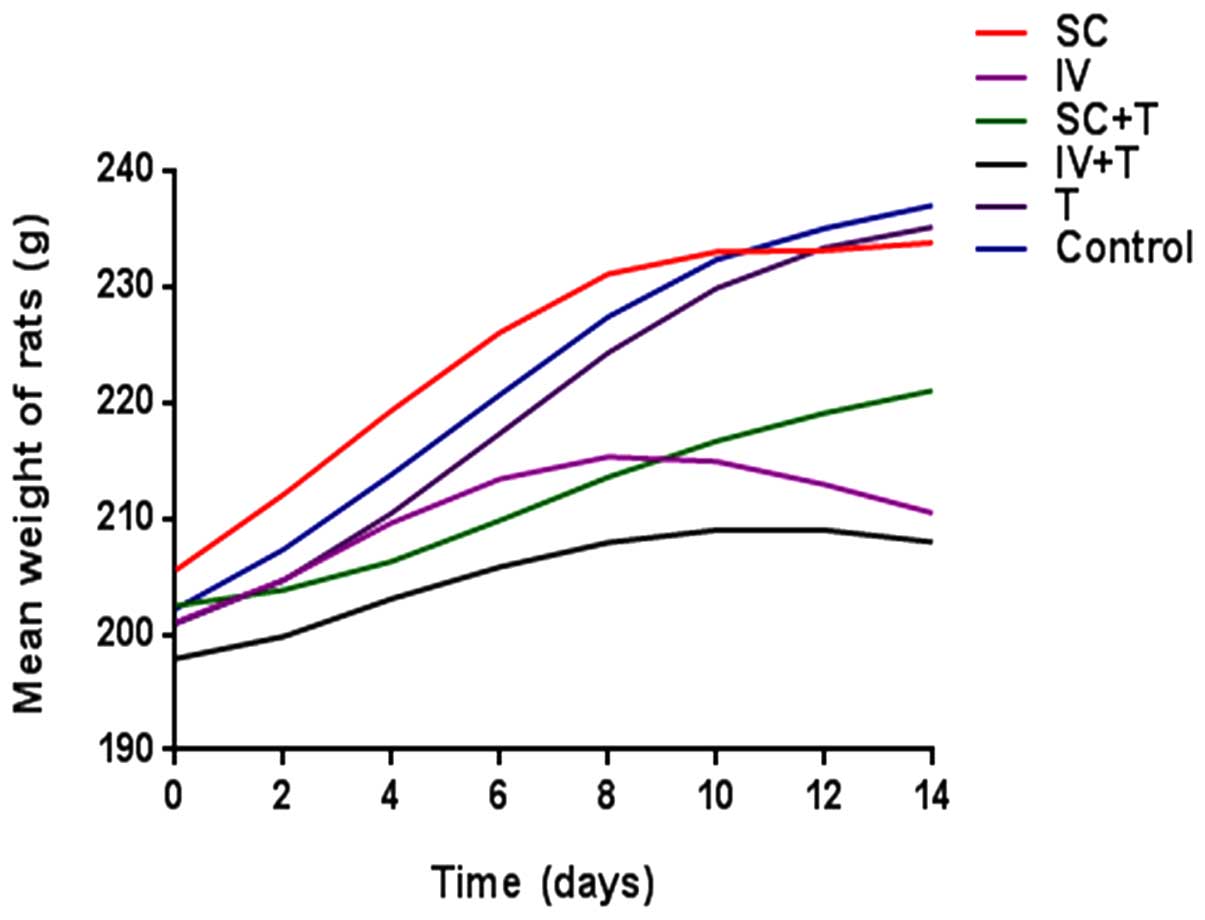
Adult SD rats subjected to ivBor treatment gained
weight more slowly (Fig. 4) and were
less active compared with the untreated control group, in both the
presence and absence of thalidomide treatment, indicating systemic
poisoning. There were no evident symptoms of systemic poisoning in
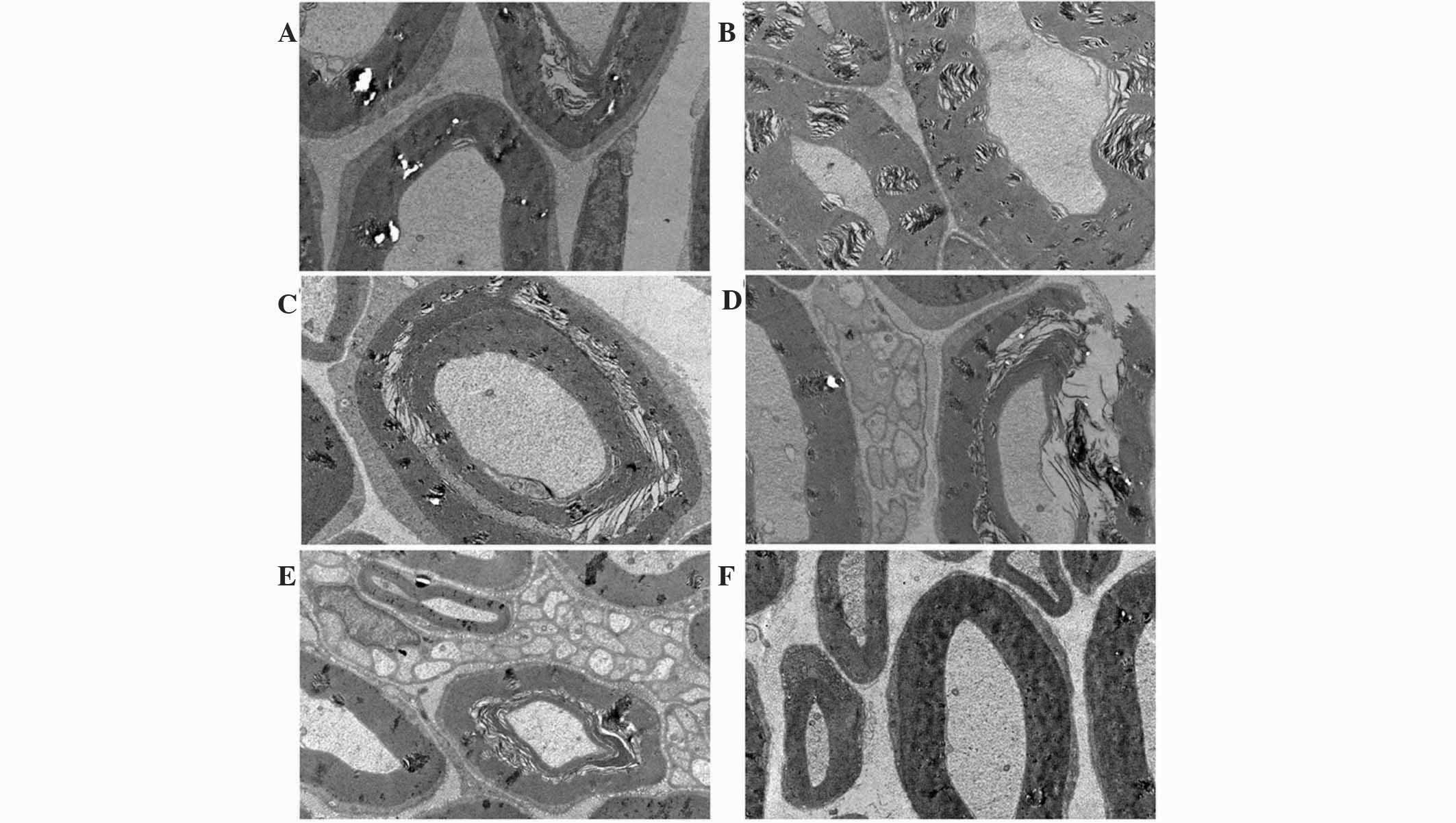
the scBor-treated and control groups of rats. TEM images indicated
PN due to the layered structures (Fig.
5A and B), discontinuous (Fig.
5C) or ruptured tissue (Fig. 5D)
of the myelin sheath and vacuolation (Fig. 5E). Furthermore, these observations
were more common in the ivBor-treatment group than the scBor group,
in both the presence and absence of thalidomide. In addition, only
minor changes to the dorsal root nerve of scBor-treated rats were
observed.
Discussion
The present study revealed the superior efficacy,
and lower incidence and severity of PN following treatment with
scBor compared with ivBor when combined with thalidomide and
dexamethasone. Despite several minor differences between this and
previous therapies, the similarity between the scBor and ivBor
groups across several efficacy indicators (VGPR, CR and 1-year
overall survival/progression-free survival) was apparent, and
revealed a significant improvement compared with a single-agent
therapy (3,7). This efficacy may be associated with a
higher percentage of patients receiving additional
cyclophosphamide, a lower percentage of patients with an ISS stage
III (12) or an age ≥65 years old
and a lower level of β2 microglobulin in the scBor-treated
group.
The intravenous method of administration is the most
common method of bortezomib treatment. However, subcutaneous
injection of bortezomib is becoming increasingly used, and the side
effects of scBor single treatment are well understood (3,7,13,14). A
previous study by Arnulf et al (7) of treatment with bortezomib alone
demonstrated that the incidence of PN at all grades, grade ≥2 and
grade ≥3 were 38 and 53%, 24 and 41% and 6 and 16% in the scBor and
ivBor groups, respectively. This was in agreement with the 51.3 and
61.3%, 35.1 and 56.8% and 2.7 and 20.5% observed in the scBor and
ivBor groups, respectively, in the present study. Garderet et
al (15) demonstrated a
cumulative, dose-associated incidence of grade ≥3, exacerbated PN
following treatment with bortezomib and thalidomide combinatorial
treatment; this presented at an incidence of 29% for VTD treatment
and 12% for thalidomide and dexamethasone treatment. The median
time of onset of all grades of PN of the patients in the present
study was similar, and there were no cases of grade ≥3 PN
associated with scBor treatment. These data suggested a decrease in
severity of PN following scBor treatment, which may be associated
with a lower maximum plasma concentration of bortezomib,
neuroprotective effects and thalidomide withdrawal or with dose
reduction when severe PN appeared in 3 cases (3). PN occurred more frequently following
subcutaneous delivery of bortezomib, but was less severe following
this method of bortezomib treatment. In addition,
bortezomib-associated PN typically became apparent by the end of
therapy cycles 4 or 5, was dose-associated and was reversible in
the majority of patients. The baseline characteristics of the age
or number or type of prior therapies were not risk factors
associated with PN, and the efficacy of bortezomib was not
adversely affected by the grade ≥2 PN (16) or the dose regimen (17). Furthermore, there were no obvious
ISRs in the current patients, and the low severity of ISRs was
similar to that of a previous report (18). Subcutaneous administration of
bortezomib therefore provides an important alternative method of
treatment, particularly for the elderly or patients with poor
vascular conditions, due to its improved safety profile.
Detailed information with regard to other side
effects of bortezomib have been sufficiently documented whether
this is administered independently or as part of a combination
therapy (18–23). Upon treatment with the VTD
combination therapy, a decreased white blood cell count, hemoglobin
level and platelet count, and gastrointestinal symptoms were the
most common side effects in both groups, but these were not severe
in the present study. These data were consistent with previous
studies (22,23) and presented additional information
about the scBor severity as part of a VTD combination therapy.
From the results of previous in vivo studies,
it has been hypothesized that bortezomib predominantly causes
direct sciatic nerve and dorsal root ganglia toxicity due to
ubiquitin aggregates accumulating in the cytoplasm (24,25). In
the current study, TEM images of the sciatic nerve of the SD rats
indicated that changes to the myelin sheath were less common
following scBor compared with ivBor treatment. Furthermore, PN is
more severe in combination treatments containing thalidomide;
however, this effect was lessened with scBor combination compared
with the ivBor combination treatment. Symptoms of systemic
poisoning, such as a slower weight increase and lower activity,
were more evident following ivBor treatment, in both the presence
and absence of thalidomide.
In conclusion, treatment with scBor demonstrated a
lower incidence and severity of PN compared with ivBor
administration, but did not adversely affect the efficacy of
treatment when combined with thalidomide and dexamethasone.
Previous studies have indicated that a weekly dose of bortezomib
should be used within combinatorial treatments in order to achieve
the lowest PN rates (26–28). However, the most efficient dose
schedule of bortezomib under varying ISS stages and patient
demographics requires additional research.
References
|
1
|
Phekoo KJ, Schey SA, Richards MA, Bevan
DH, Bell S, Gillett D and Møller H: Consultant Haematologists,
South Thames Haematology Specialist Committee: A population study
to define the incidence and survival of multiple myeloma in a
National Health Service Region in UK. Br J Haematol. 127:299–304.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Pantani L, Zamagni E, Zannetti BA, Pezzi
A, Tacchetti P, Brioli A, Mancuso K, Perrone G, Rocchi S, Tosi P
and Cavo M: Bortezomib and dexamethasone as salvage therapy in
patients with relapsed/refractory multiple myeloma: Analysis of
long-term clinical outcomes. Ann Hematol. 93:123–128. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Moreau P, Pylypenko H, Grosicki S,
Karamanesht L, Leleu X, Grishunina M, Rekhtman G, Masliak Z, Robak
T, Shubina A, et al: Subcutaneous versus intravenous administration
of bortezomib in patients with relapsed multiple myeloma: A
randomised, phase 3, non-inferiority study. Lancet Oncol.
12:431–440. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Soriano GP, Besse L, Li N, Kraus M, Besse
A, Meeuwenoord N, Bader J, Everts B, den Dulk H, Overkleeft HS,
Florea BI and Driessen C: Proteasome inhibitor-adapted myeloma
cells are largely independent from proteasome activity and show
complex proteomic changes, in particular in redox and energy
metabolism. Leukemia. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ri M: Mechanism of action and determinants
of sensitivity to the proteasome inhibitor bortezomib in multiple
myeloma therapy. Rinsho Ketsueki. 57:537–45. 2016.PubMed/NCBI
|
|
6
|
Dimopoulos MA, Beksac M, Benboubker L,
Roddie H, Allietta N, Broer E, Couturier C, Mazier MA, Angermund R
and Facon T: Phase II study of bortezomib-dexamethasone alone or
with added cyclophosphamide or lenalidomide for sub-optimal
response as second-line treatment for patients with multiple
myeloma. Haematologica. 98:1264–72. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Arnulf B, Pylypenko H, Grosicki S,
Karamanesht L, Leleu X, van de Velde H, Feng H, Cakana A, Deraedt W
and Moreau P: Updated survival analysis of a randomized phase III
study of subcutaneous versus intravenous bortezomib in patients
with relapsed multiple myeloma. Haematologica. 97:1925–1928. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Glasmacher A, Hahn C, Hoffmann F, Naumann
R, Goldschmidt H, von Lilienfeld-Toal M, Orlopp K, Schmidt-Wolf I
and Gorschlüter M: A systematic review of phase-II trials of
thalidomide monotherapy in patients with relapsed or refractory
multiple myeloma. Br J Haematol. 132:584–593. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Palumbo A, Davies F, Kropff M, Bladé J,
Delforge M, da Costa F Leal, Sanz R Garcia, Schey S, Facon T,
Morgan G and Moreau P: Consensus guidelines for the optimal
management of adverse events in newly diagnosed,
transplant-ineligible patients receiving melphalan and prednisone
in combination with thalidomide (MPT) for the treatment of multiple
myeloma. Ann Hematol. 89:803–811. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Durie BG, Harousseau JL, Miguel JS, Bladé
J, Barlogie B, Anderson K, Gertz M, Dimopoulos M, Westin J,
Sonneveld P, Ludwig H, et al: International uniform response
criteria for multiple myeloma. Leukemia. 20:1467–1473. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
National Cancer Institute, . Common
terminology criteria for adverse events, version 3.0. https://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/ctcaev3.pdfAccessed.
April 11–2011
|
|
12
|
Greipp PR, San MJ, Durie BG, Crowley JJ,
Barlogie B, Bladé J, Boccadoro M, Child JA, Avet-Loiseau H, Kyle
RA, Lahuerta JJ, et al: International staging system for multiple
myeloma. J Clin Oncol. 23:3412–20. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hoy SM: Subcutaneous bortezomib: In
multiple myeloma. Drugs. 73:45–54. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Grosicki S: Subcutaneous bortezomib as a
new promising way to successful maintenance therapy in multiple
myeloma. Wiad Lek. 65:167–173. 2012.(In Polish). PubMed/NCBI
|
|
15
|
Garderet L, Iacobelli S, Moreau P, Dib M,
Niederwieser D, Masszi T, Fontan T, Michallet M, Gratwohl A, Lafon
I, et al: Superiority of the triple combination of
bortezomib-thalidomide-dexamethasone over the dual combination of
thalidomide-dexamethasone in patients with multiple myeloma
progressing or relapsing after autologous transplantation: The
MMVAR/IFM 2005-04 Randomized phase III trial from the chronic
leukemia working party of the European group for blood and marrow
transplantation. J Clin Oncol. 30:2475–2482. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Tacchetti P, Terragnac C, Galli M, Zamagni
E, Petrucci MT, Pezzi A, Montefusco V, Martello M, Tosi P, Baldini
L, et al: Bortezomib- and thalidomide-induced peripheral neuropathy
in multiple myeloma: Clinical and molecular analyses of a phase 3
study. Am J Hematol. 89:1085–1091. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Richardson PG, Sonneveld P, Schuster MW,
Stadtmauer EA, Facon T, Harousseau JL, Ben-Yehuda D, Lonial S,
Goldschmidt H, Reece D, et al: Reversibility of symptomatic
peripheral neuropathy with bortezomib in the phase III APEX trial
in relapsed multiple myeloma: Impact of a dose-modification
guideline. Br J Haematol. 144:895–903. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lamm W, Drach-Schauer B, Eder S and Drach
J: Bortezomib administered subcutaneously is well tolerated in
bortezomib-based combination regimens used in patients with
multiple myeloma. Oncology. 85:223–227. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
San Miguel JF, Schlag R, Khuageva NK,
Dimopoulos MA, Shpilberg O, Kroptt M, Spicka I, Petrucci MT,
Palumbo A, Samoilova OS, et al: Bortezomib plus melphalan and
prednisone for initial treatment of multiple myeloma. N Engl J Med.
359:906–917. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wright JJ: Combination therapy of
bortezomib with novel targeted agents: An emerging treatment
strategy. Clinical Cancer Research. 16:4094–4104. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
San Miguel JF, Schlag R, Khuageva NK,
Dimopoulos MA, Shpilberg O, Kropff M, Spicka I, Petrucci MT, et al:
Continued overall survival benefit after 5 years' follow-up with
bortezomib-melphalan-prednisone (VMP) versus melphalan-prednisone
(MP) in patients with previously untreated multiple myeloma and no
increased risk of second primary malignancies: Final results of the
phase 3 VISTA trial. Blood. 118:4762011.PubMed/NCBI
|
|
22
|
Hrusovsky I, Emmerich B, von Rohr A,
Voegeli J, Taverna C, Olie RA, Pliskat H, Frohn C and Hess G:
Bortezomib retreatment in relapsed multiple myeloma - results from
a retrospective multicentre survey in Germany and Switzerland.
Oncology. 79:247–54. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Sher T, Ailawadhi S, Miller KC, Manfredi
D, Wood M, Tan W, Wilding G, Czuczman MS, Hernandez-llizaliturri
FJ, Hong F, et al: A steroid-independent regimen of bortezomib,
liposomal doxorubicin and thalidomide demonstrate high response
rates in newly diagnosed multiple myeloma patients. Br J Haematol.
154:104–110. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Cavaletti G, Gilardini A, Canta A,
Rigamonti L, Rodriguez-Menendez V, Ceresa C, Marmirili P, Bossi M,
Oggioni N, D'Incalci M and De Coster R: Bortezomib-induced
peripheral neurotoxicity: A neurophysiological and pathological
study in the rat. Exp Neurol. 204:317–325. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Csizmadia V, Raczynski A, Csizmadia E,
Fedyk ER, Rottman J and Alden CL: Effect of an experimental
proteasome inhibitor on the cytoskeleton, cytosolic protein
turnover and induction in the neuronal cells in vitro.
Neurotoxicology. 29:232–243. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Mangiacavalli S, Pochintesta L, Pascutto
C, Cocito F, Cazzola M, Corso A and Pompa A: Good clinical activity
and favorable toxicity profile of once weekly bortezomib,
fotemustine and dexamethasone (B-MuD) for the treatment of relapsed
multiple myeloma. Am J Hematol. 88:102–106. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Bringhen S, Larocca A, Rossi D, Cavalli M,
Genuardi M, Ria R, Gentili S, Patriarca F, Nozzoli C, Levi A, et
al: Efficacy and safety of once-weekly bortezomib in multiple
myeloma patients. Blood. 116:4745–4753. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Moore S, Atwal S, Sachchithanantham S,
Streetly M, Khan I, Percy L, Narat S, Rabin N, Johnston R, D'Sa S,
et al: Weekly intravenous bortezomib is effective and well
tolerated in relapsed/refractory myeloma. Eur J Haematol.
90:420–425. 2013. View Article : Google Scholar : PubMed/NCBI
|