Introduction
An aneurysm is defined as an increase in the size of
an artery by >50% of the normal arterial diameter. According to
the affected segment of the aorta, aneurysmal diseases are divided
into thoracic, thoracoabdominal and abdominal aortic aneurysms
(AAAs). Worldwide, the prevalence of AAAs may be as high as 8%,
depending on the criteria used for diagnosis (1).
Since the introduction of endovascular repair of
aortic aneurysms by Parodi et al in 1991 (2), this technique has resulted in lower
short-term mortality and shorter hospital stays than open repair.
Although endovascular and open repair of AAAs result in similar
long-term survival overall, endovascular repair has been shown to
increase the long-term survival of younger patients (3). In patients randomized to open or
endovascular AAA repair, all-cause perioperative mortality and
AAA-related mortality at short- and intermediate-term follow-up was
lower in patients who underwent endovascular repair (4).
Due to the attractive outcomes of endovascular
repair of aortic aneurysms, the overall use of the endovascular
procedure has risen sharply in the last decade. Epidemiology of
aortic aneurysm repair in the United States showed that
endovascular aneurysm repair (EVAR) increased from 5.2 to 74% of
the total number of AAA repairs from 2000 to 2010, even though the
total number of AAAs remained stable at 45,000 cases per year
(5). There was a 72% decline in open
repair during the study period. The national trends were similar
for the use of open and endovascular repair for thoracic aortic
pathologies between 2000 and 2010; the rate of open repair
decreased from 2.5 to 2.2 per 100,000 beneficiaries, and the rate
of endovascular repair of thoracic aortic aneurysms increased
markedly from 0 to 0.8 per 100,000 beneficiaries (6).
There has been little analysis of these national
trends in Asian countries. Therefore, the present study aimed to
evaluate the national trends for the treatment of aneurysms in
Korea.
Materials and methods
Data collection
Data from the Health Insurance Review and Assessment
Service (HIRA) were used to evaluate the trends of aneurysm repair
in Korea. Korea has a universal health coverage system, the
National Health Insurance, which covers ~98% of the overall Korean
population. Claims data of HIRA are collected from healthcare
service providers when they seek reimbursements for healthcare
services that the National Health Insurance Corporation covers.
These national data are collated from healthcare providers across
Korea, and correspond to the number of claims that are submitted by
patients for inclusive healthcare services (7).
The Electronic Data Interchange (EDI) database of
HIRA contains operation and management codes. The number of
aneurysm repairs was collected from the EDI codes of HIRA. Table I shows the EDI codes for aortic
aneurysm repair. Codes for the open repair of aneurysms include
O0223, O0224, O2031-O2035, and O2037-O2039; whereas codes O2031,
O2032, and O2033 are allocated for the open repair of thoracic
aortic aneurysms. The open repair of AAAs with/without involvement
of the iliac arteries corresponds to codes O0223, O0224 and O2034.
Codes O2037 and O2038 are designated for the open repair of
unilateral- and bilateral-isolated iliac artery aneurysms,
respectively. O2039 includes the open repair of all splanchnic
artery aneurysms of the celiac, hepatic, splenic, mesenteric and
renal arteries. O2035 indicates the open repair of other arterial
aneurysms, with the exception of aneurysms originating from the
cardiac and intracranial arteries. Endovascular repair of thoracic
aneurysms and AAAs were allocated the codes M6611 and M6612;
whereas M6613 denotes the endovascular repair of other arterial
aneurysms, with the exception of aneurysms originating from the
cardiac and intracranial arteries.
 | Table I.EDI codes for the open and
endovascular repair of aneurysms. |
Table I.
EDI codes for the open and
endovascular repair of aneurysms.
| EDI codes | Type of repair |
|---|
| Open repairs |
|
|
O0223 | Abdominal aorta,
suprarenal |
|
O0224 | Abdominal aorta,
infrarenal |
|
O2031 | Ascending aorta |
|
O2032 | Aortic arch |
|
O2033 | Descending aorta |
|
O2034 | Abdominal aorta
involving iliac artery |
|
O2035 | Other arteries |
|
O2037 | Isolated iliac
artery, bilateral |
|
O2038 | Isolated iliac
artery, unilateral |
|
O2039 | Splanchnic
artery |
| Endovascular
repair |
|
|
M6611 | Placement of stent
graft, aorta |
|
M6612 | Placement of stent
graft, aorta involving iliac artery |
|
M6613 | Placement of stent
graft, other arteries |
For the evaluation of aneurysm repair for a recent
10 year-period, data from the EDI database of HIRA collected
between 2004 and 2013 was used. The total number of aneurysm
repairs was calculated for this period and, from this dataset, the
trends for open and endovascular repair of aneurysms were analyzed.
The present study was approved by the Kyung Hee University Hospital
at Gangdong Institutional Review Board (Seoul, Korea
Statistical analysis
A linear-by-linear association was performed to
determine the trends of aneurysm repair during the evaluation
period. P<0.05 (two-sided) was considered to indicate a
statistically significant difference. Data were analyzed using SPSS
19.0 statistical software (SPSS Inc., Chicago, IL, USA).
Results
Aneurysm repair
A total of 32,130 patients underwent aneurysm repair
between 2004 and 2013. Open repair was performed in 23,774
patients, and endovascular repair in 8,356. The number of patients
treated with the respective techniques for each year is detailed in
Table II. The proportion of
patients who underwent open repair decreased from 94.0% in 2004 to
54.9% in 2013. At the same time, the proportion of patients who
underwent endovascular repair increased from 6.0% in 2004 to 45.1%
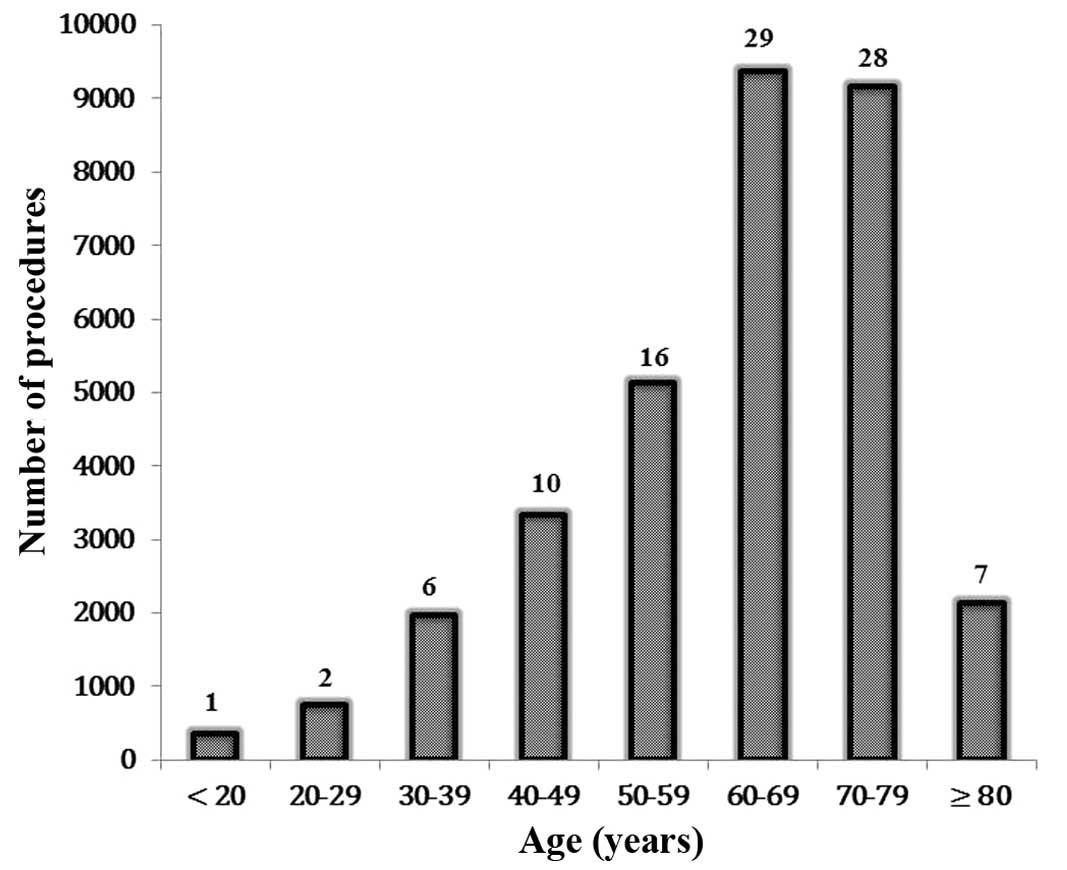
in 2013. The age distribution of patients is shown in Fig. 1. The prevalence of aneurysm repair
increased with age: 16% of patients were in their fifties, 29% were
in their sixties, and 28% were in their seventies.
| Table II.Distribution of open and endo repair
of aneurysm each year for 10 years (2004–2013). |
Table II.
Distribution of open and endo repair
of aneurysm each year for 10 years (2004–2013).
| Year | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 |
|---|
| Open | 1,759 | 3,444 | 2,232 | 2,424 | 2,895 | 2,078 | 2,091 | 2,288 | 2,350 | 2,213 |
| (%) | 94.0 | 93.4 | 89.7 | 86.3 | 79.1 | 75.0 | 68.3 | 64.8 | 55.7 | 54.9 |
| Endo | 113 | 242 | 257 | 386 | 763 | 693 | 971 | 1,242 | 1,870 | 1,819 |
| (%) | 6.0 | 6.6 | 10.3 | 13.7 | 20.9 | 25.0 | 31.7 | 35.2 | 44.3 | 45.1 |
| Total | 1,872 | 3,686 | 2,489 | 2,811 | 3,658 | 2,771 | 3,062 | 3,530 | 4,220 | 4,032 |
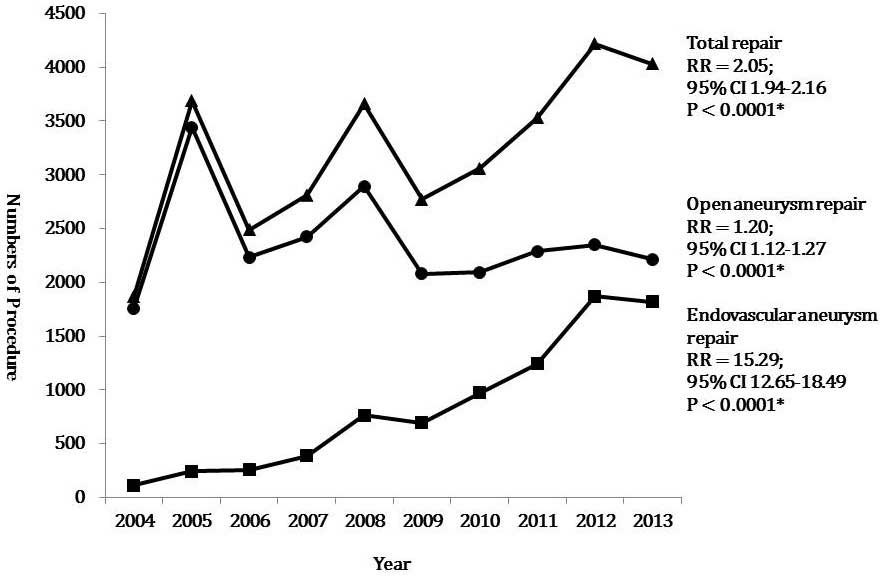
Trends in aneurysm repair
The number of patients who underwent aneurysm repair
during the study period is presented in Fig. 2. The total number of aneurysm repairs
increased significantly from 1,872 in 2004 to 4,032 in 2013
[relative risk (RR) 2.05, 95% confidence interval (CI) 1.94–2.16).
During the study period, the number of patients who underwent open
repair significantly increased from 1,759 in 2004 to 2,213 in 2013
(RR 1.20, 95% CI: 1.12–1.27), with an overall downward trend.
However, the number of patients who underwent endovascular repair
significantly increased from 113 in 2004 to 1,819 in 2013 (RR
15.29, 95% CI: 12.65–18.49). These trends were all statistically
significant (P<0.0001).
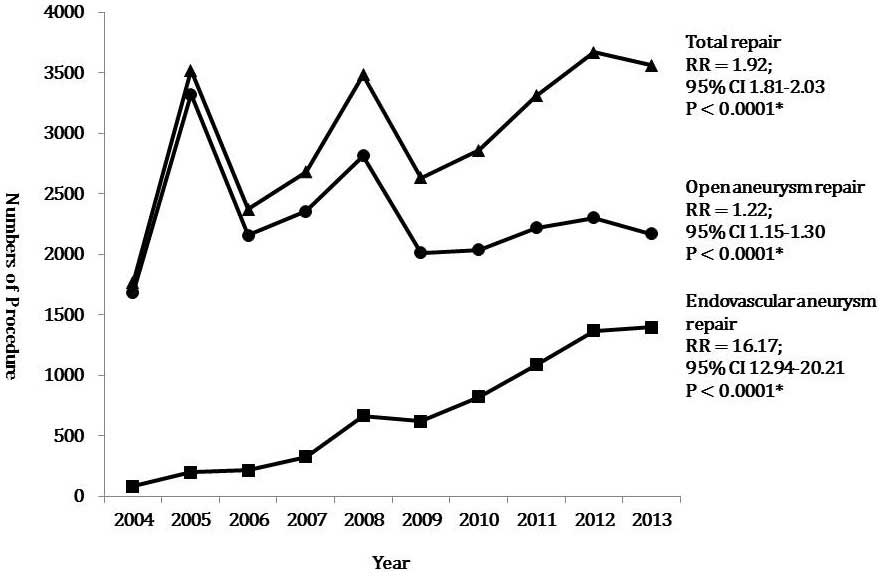
Trends in aortic aneurysm repair
The number of patients who underwent aortic aneurysm
repair, excluding those who experienced aneurysms at other sites
during the study period, is displayed in Fig. 3. The total number of aortic aneurysm
repairs increased significantly from 1,765 in 2004 to 3,565 in 2013
(RR 1.92, 95% CI: 1.81–2.03). During the study period, the number
of open repairs significantly increased from 1,683 in 2004 to 2,169
in 2013 (RR 1.22, 95% CI: 1.15–1.30), with an overall downward
trend. However, the number of endovascular repairs significantly
increased from 82 in 2004 to 1,396 in 2013 (RR 16.17, 95% CI:
12.94–20.21). These trends were all statistically significant
(P<0.0001).
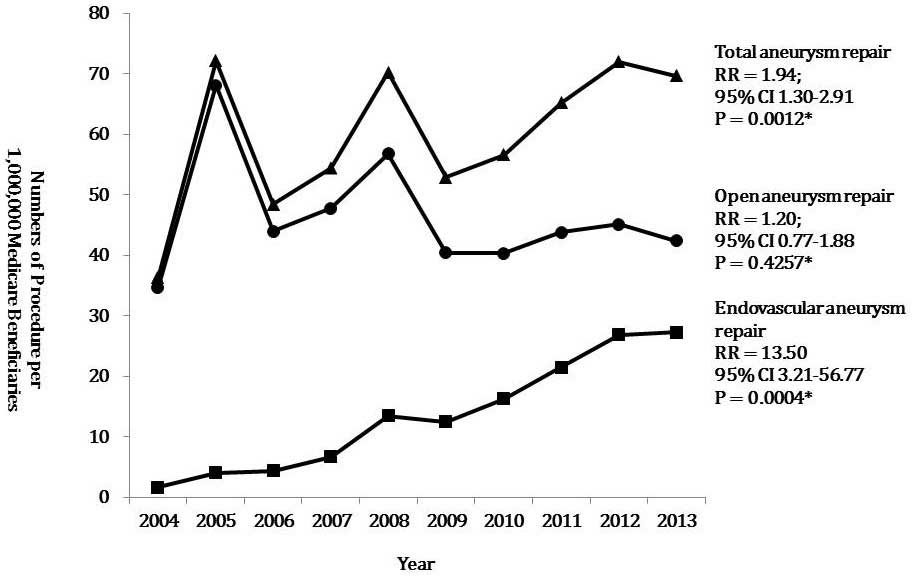
Aortic aneurysm repair per 1,000,000
Medicare Beneficiaries
Population-adjusted frequencies for total, open, and
endovascular repair of aortic aneurysms over 10 years are shown in
Fig. 4. The total number of aneurysm
repairs per 1,000,000 Medicare Beneficiaries significantly
increased during the study period, from 39 procedures in 2004 to 70
in 2013 (RR 1.94, 95% CI, 1.30–2.91; P=0.0012). At the same time,
the number of open repairs increased from 35 procedures in 2004 to
42 in 2013 (RR 1.20, 95% CI, 0.77–1.88; P=0.4257). However, the
number of endovascular repairs per 1,000,000 Medicare Beneficiaries
significantly increased, from two procedures in 2004 to 27 in 2013
(RR 13.50, 95% CI, 3.21–56.77; P=0.0004).
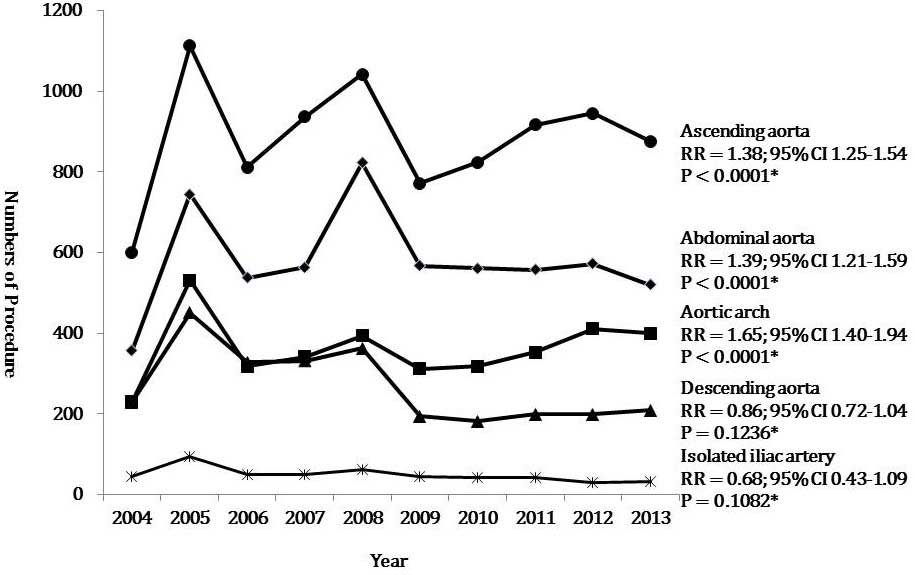
Trends in open aortic aneurysm
repair
Changes in the frequency of open repair of aneurysms
at each aortic level and in the isolated iliac artery are displayed
in Fig. 5. Open repair of the
ascending aorta was most commonly performed. The number of
ascending aortic aneurysm repairs increased significantly from 601
in 2004 to 876 in 2013 (RR 1.38, 95% CI: 1.25–1.54; P<0.0001).
The open repair of AAAs was the second most common procedure, with
the number of procedures significantly increasing from 356 in 2004
to 520 in 2014 (RR 1.39, 95% CI: 1.21–1.59; P<0.0001), with
sharp increases in 2005 and 2008. The number of open repairs of the
aortic arch performed significantly increased from 230 in 2004 to
399 in 2014 (RR 1.65, 95% CI: 1.40–1.94; P<0.0001). However, the
number of open repairs of descending aortic aneurysms and isolated
iliac artery aneurysms performed decreased from 299 to 208 (RR
0.86, 95% CI: 0.72–1.04; P=0.1236) and from 43 to 31 (RR 0.68, 95%
CI: 0.43–1.09; P=0.1082) between 2004 and 2013, respectively.
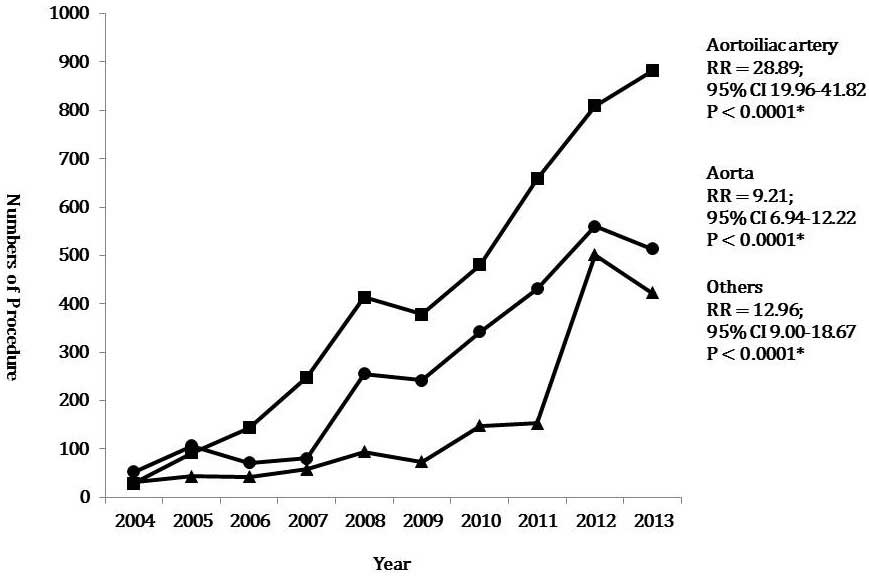
Trends in endovascular aneurysm
repair
Endovascular repair of aneurysms at all levels
dramatically significantly increased from 2004 to 2013 (Fig. 6). The number of endovascular repairs
for aortoiliac artery aneurysms significantly increased from 29 in
2004 to 882 in 2013 (RR 28.89 CI: 19.96–41.82). The number of
endovascular repairs performed for other aortic aneurysms,
including thoracic aortic aneurysms and AAAs using the tube type of
stent graft, significantly increased from 53 in 2004 to 514 in 2013
(RR 9.21, 95% CI: 6.94–12.22). The number of endovascular repairs
of other aneurysms, with the exception of aortoiliac and aortic
aneurysms, also significantly increased from 31 in 2004 to 423 in
2013 (RR 12.96, 95% CI: 9.00–18.67). These trends were all
statistically significant (P<0.0001).
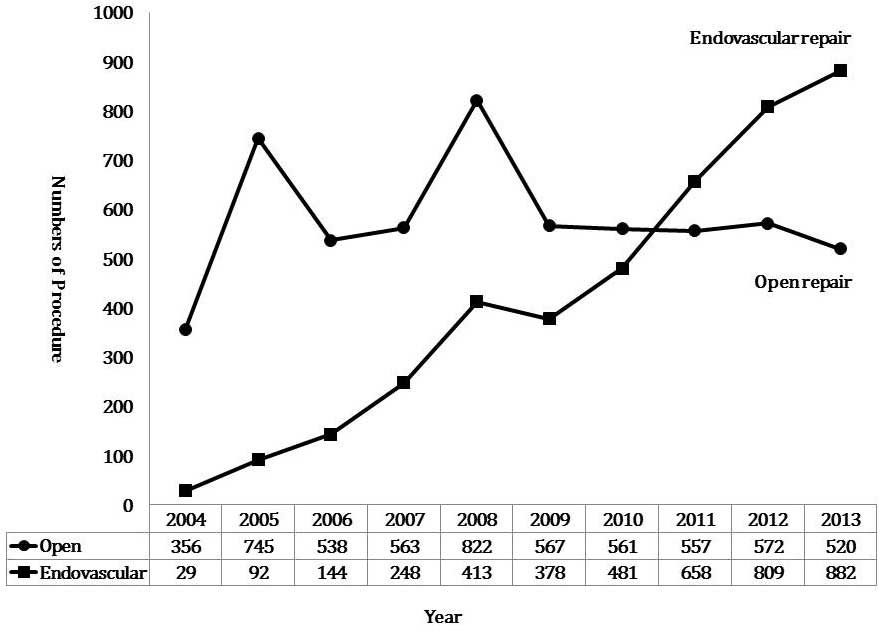
Trends in open and endovascular
abdominal aortic aneurysm repair
The number of patients who underwent open or
endovascular repairs of AAAs is displayed in Fig. 7. The total number of AAA repairs was
385 in 2004 and 1402 in 2013. With a marked increase in the
endovascular repair of AAAs and the downward trend of open AAA
repair, endovascular repair overtook open repair as the more
popular technique used between 2010 and 2011. Notably, endovascular
repair was performed 1.7 times more often than open repair in
2013.
Discussion
There is a global trend of increasing prevalence of
endovascular repair for the treatment of aortic aneurysms. A recent
epidemiological study in the US reported that the overall
prevalence of endovascular aortic aneurysm repair has risen sharply
from 5.2% in 2000 to 74% in 2010 (8). In a German study, the rate of treatment
by EVAR increased from 24.0 to 40.3% in males and from 17.3 to
31.0% in females between 2006 and 2009 (9). In the present study, the rate of
endovascular repair of aortic aneurysms increased 16.17-fold during
the study period.
Population-adjusted frequencies of aneurysm repair
differ from country to country. According to an epidemiological
study in the US, the number of AAA repairs conducted was 14.22 per
100,000 (5). However, in the present
study, the total number of aneurysm repairs conducted per 1,000,000
Medicare Beneficiaries was 39 in 2004 and 70 in 2013. Aneurysm
repair is performed 2.0–3.6 times more frequently in the US than in
Korea.
Several hypotheses have been suggested for the lower
rate of aneurysmal repair in Korea. Firstly, the overall incidence
of aortic aneurysms is lower in Korea than in Western countries.
Ultrasound screening and autopsy series have indicated that the
prevalence of AAAs (≥3 cm) is 3–10% for patients aged >50 years
old in Western countries (10). In a
Veterans Affairs screening study of >73,000 patients aged 50–79
years old, the prevalence of AAAs ≥3 cm was 4.6% (11). In the Asian population, the reported
prevalence of AAAs varies. Spark et al (12) suggested that the prevalence of AAAs
in the Asian population was lower than that in the Caucasian
population. Although a screening study of the general population in
Korea demonstrated that the prevalence of AAAs was 4.5% in a
high-risk group (13), another
screening study during echocardiograms indicated that 0.2% of the
study population was newly diagnosed with AAAs (14).
A second explanation for the lower rate of
aneurysmal repair in Korea is that there is no nationwide screening
program for AAAs. In the US, the Centers for Medicare and Medicaid
Services provide free ultrasound screening for AAAs to certain
beneficiaries for whom AAA screening may be advantageous, including
people who have a family history of AAAs, and men aged 65–75 years
old who have smoked ≥100 cigarettes in their lifetime (15). Thirdly, the deployment of medical
resources for vascular surgeries in Korea may be different than in
Western countries. The Department of Health in the Korean
government has focused on the treatment of patients with cancer.
The budget for health has been allocated to screen for and treat
cancer more so than vascular disease. The deployment of medical
resources in Korea may be further evaluated by the health policy
authorities.
Despite an overall downward trend in prevalence, the
frequency of open repair of aortic aneurysms increased during the
study period (1.22-fold). The increased rate of open repair of
aortic aneurysms may be associated with the increasing frequency of
open repair of ascending aortic aneurysms (RR 1.38, 95% CI:
1.25–1.54), AAAs (RR 1.39, 95% CI: 1.21–1.59, P<0.0001), and
aortic arch aneurysms (RR 1.65, 95% CI: 1.40–1.94).
The number of open repairs for descending thoracic
aortic aneurysms and isolated iliac artery aneurysms decreased from
299 to 208 (RR 0.86, 95% CI: 0.72–1.04) and from 43 to 31 (RR 0.68,
95% CI: 0.43–1.09) between 2004 and 2013, respectively. This may be
associated with the dramatic increase in endovascular repairs of
these aneurysms. Endovascular repair of descending thoracic aortic
aneurysms is less invasive than open repair and may result in a
lower mortality rate, as evidenced by single-center studies or
industry-sponsored registries (16,17).
Although population-based data from England showed that operative
mortality for degenerative descending thoracic aneurysms was
similar after either thoracic endovascular aortic/aneurysm repair
or open repair (18), endovascular
repair is predominantly used for descending thoracic aortic
aneurysms.
The iliac branch device (IBD) technique has been
introduced as an appealing and effective solution to avoid
complications during the repair of aortoiliac aneurysms with
extensive iliac involvement, or of isolated iliac artery aneurysms.
Perlani et al (19) reported
that the estimated patency rate of the internal iliac branch was
91.4% at 5 years, and the rate of freedom from any re-intervention
was 90% at 1 year and 81.4% at 5 years. Oderich et al
(20) suggested the use of the novel
surgeon-modified hypogastric branch stent graft to preserve pelvic
perfusion in the circumstance that a commercial IBD is unavailable.
Furthermore, Fatima et al (21) published various methods of pelvic
revascularization in patients with aortoiliac aneurysms involving
one or both common iliac arteries, such as flared iliac stent
grafting, the sandwich technique, external-to-internal iliac
arterial stenting, double bifurcated stent grafting, or novel
hybrid revascularization. In Korea, there are no commercially
available IBDs. Therefore, pelvic revascularization is achieved
with the surgeon-modified IBD or the novel endovascular or hybrid
procedures suggested by Fatima et al (21).
The present study revealed that the endovascular
repair of AAAs overtook open repair as the most commonly utilized
technique between 2010 and 2011. These results are consistent with
a previous epidemiologic study in the US that reported that
endovascular repair overtook the open repair of AAAs between 2005
and 2006 (5). This 5-year gap may be
related to the late adoption of endovascular treatment for aortic
aneurysms and the administrative policies in Korea.
Several limitations of the present study should be
acknowledged. As the present study is a retrospective analysis
based on an administrative database, there is an intrinsic limit to
the number of variables that can be measured. Follow-up data and
long-term outcomes were unavailable. In addition, further
evaluation is required after more detailed data are collected, such
as the number of ruptured and unruptured aortic aneurysms, the
prevalence of co-morbidities, the duration of hospital stays, and
the rates of mortality according to treatment modality.
In conclusion, a total of 32,130 patients underwent
aneurysm repair between 2004 and 2013. The frequency of open repair
increased 1.2-fold with an overall downward trend. The prevalence
of endovascular repair markedly increased 15.3-fold. Although the
frequency of open repair of aortic aneurysms increased at the level
of the ascending aorta, aortic arch, and abdominal aorta, the
frequency of this technique decreased for descending thoracic
aortic aneurysms and isolated iliac artery aneurysms. In Korea, the
endovascular repair of AAAs overtook open repair as the most
commonly utilized technique between 2010 and 2011.
References
|
1
|
Norman PE and Powell JT: Abdominal aortic
aneurysm: The prognosis in women is worse than in men. Circulation.
115:2865–2869. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Parodi JC, Palmaz JC and Barone HD:
Transfemoral intraluminal graft implantation for abdominal aortic
aneurysms. Ann Vasc Surg. 5:491–499. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lederle FA, Freischlag JA, Kyriakides TC,
Matsumura JS, Padberg FT Jr, Kohler TR, Kougias P, Jean-Claude JM,
Cikrit DF and Swanson KM: OVER Veterans Affairs Cooperative Study
Group: Long-term comparison of endovascular and open repair of
abdominal aortic aneurysm. N Engl J Med. 367:1988–1997. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Dangas G, O'Connor D, Firwana B, Brar S,
Ellozy S, Vouyouka A, Arnold M, Kosmas CE, Krishnan P, Wiley J, et
al: Open versus endovascular stent graft repair of abdominal aortic
aneurysms: A meta-analysis of randomized trials. JACC Cardiovasc
Interv. 5:1071–1080. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Dua A, Kuy S, Lee CJ, Upchurch GR Jr and
Desai SS: Epidemiology of aortic aneurysm repair in the United
States from 2000 to 2010. J Vasc Surg. 59:1512–1517. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jones DW, Goodney PP, Nolan BW, Brooke BS,
Fillinger MF, Powell RJ and Stone DH: National trends in
utilization, mortality and survival after repair of type B aortic
dissection in the medicare population. J Vasc Surg. 60:11–19. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kim L, Kim JA and Kim S: A guide for the
utilization of health insurance review and assessment service
national patient samples. Epidemiol Health. 36:e20140082014.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Dua A, Kuy S, Lee CJ, Upchurch GR Jr and
Desai SS: Epidemiology of aortic aneurysm repair in the United
States from 2000 to 2010. J Vasc Surg. 59:1512–1517. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Santosa F, Moysidis T, Nowak T, Heilmaier
C, Berg C, Luther B and Kröger K: Endovascular abdominal aneurysm
repair: Trends in Germany. Vasa. 41:268–274. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wilmink AB and Quick CR: Epidemiology and
potential for prevention of abdominal aortic aneurysm. Br J Surg.
85:155–162. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lederle FA, Johnson GR, Wilson SE, Chute
EP, Littooy FN, Bandyk D, Krupski WC, Barone GW, Acher CW and
Ballard DJ: Prevalence and associations of abdominal aortic
aneurysm detected through screening. Ann Intern Med. 126:441–449.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Spark JI, Baker JL, Vowden P and Wilkinson
D: Epidemiology of abdominal aortic aneurysms in the Asian
community. Br J Surg. 88:382–384. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Joh JH, Ahn HJ and Park HC: Reference
diameters of the abdominal aorta and iliac arteries in the Korean
population. Yonsei Med J. 54:48–54. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Oh SH, Chang SA, Jang SY, Park SJ, Choi
JO, Lee SC, Park SW, Oh JK and Kim DK: Routine screening for
abdominal aortic aneurysm during clinical transthoracic
echocardiography in a Korean population. Echocardiography.
27:1182–1187. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Dillavou ED, Muluk SC and Makaroun MS:
Improving aneurysm-related outcomes: Nationwide benefits of
endovascular repair. J Vasc Surg. 43:446–451; discussion 451–452.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Matsumura JS, Cambria RP, Dake MD, Moore
RD, Svensson LG and Snyder S: TX2 Clinical Trial Investigators:
International controlled clinical trial of thoracic endovascular
aneurysm repair with the Zenith TX2 endovascular graft: 1-year
results. J Vasc Surg. 47:247–257; discussion 257. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Makaroun MS, Dillavou ED, Wheatley GH and
Cambria RP: Gore TAG Investigators: Five-year results of
endovascular treatment with the Gore TAG device compared with open
repair of thoracic aortic aneurysms. J Vasc Surg. 47:912–918. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
von Allmen RS, Anjum A and Powell JT:
Outcomes after endovascular or open repair for degenerative
descending thoracic aortic aneurysm using linked hospital data. Br
J Surg. 101:1244–1251. 2014. View
Article : Google Scholar : PubMed/NCBI
|
|
19
|
Parlani G, Verzini F, De Rango P,
Brambilla D, Coscarella C, Ferrer C and Cao P: Long-term results of
iliac aneurysm repair with iliac branched endograft: A 5-year
experience on 100 consecutive cases. Eur J Vasc Endovasc Surg.
43:287–292. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Oderich GS and Ricotta JJ II: Novel
surgeon-modified hypogastric branch stent graft to preserve pelvic
perfusion. Ann Vasc Surg. 24:278–286. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Fatima J, Correa MP, Mendes BC and Oderich
GS: Pelvic revascularization during endovascular aortic aneurysm
repair. Perspect Vasc Surg Endovasc Ther. 24:55–62. 2012.
View Article : Google Scholar : PubMed/NCBI
|