Introduction
Recurrent spontaneous miscarriage (RSM), defined as
three or more consecutive losses before 20 weeks of gestation with
the same partner (1), comprise a
multifactorial condition enhanced by a variety of genetic,
endocrine, anatomic, immunological, infectious, environmental,
thrombophilic and metabolic factors (2). Regardless of extensive research
undertaken in this field, the underlying cause of the majority
(≤50%) of RSM cases remains unknown and hence poses a clinical
challenge (3).
Toll-like receptors (TLRs), a recently identified
group of vertebrate receptors, serve a pivotal role in immune
responses. There are 10 TLRs expressed in humans (4), and Toll-like receptor 4 (TLR4) is one
of the most actively investigated TLRs. TLR4 serves an essential
role in the activation and regulation of the innate and acquired
immune responses through the recognition of specific molecular
patterns of pathogens and endogenous peptides (5).
Single-nucleotide polymorphisms (SNPs) are present
in a number of TLR genes and have been implicated in the loss of
self-tolerance, which may lead to autoimmunity and chronic
inflammation (6). A number of
studies have suggested that TLR4 polymorphisms are
associated with the development of chronic inflammatory conditions
(7,8), chronic granulomatous conditions
(9) and cardivascular diseases
(10).
To the best of our knowledge, there have been no
previous studies on the association between the human TLR4
gene and RSM in Uygur women in Xinjiang. The aim of the present
study was to investigate the association between the human
TLR4 gene and RSM using a haplotype-based case-control study
that employed SNPs in conjunction with separate analyses that
examined the data with regard to Uygur and Han women.
Materials and methods
Subjects
Subjects diagnosed with RSM were recruited at the
First Affiliated Hospital of Xinjiang Medical University in Urumqi,
China, between 2012 and 2014. A total of 306 RSM patients were
enrolled in the present study, with a Uygur/Han ratio of 1.01. RSM
was diagnosed based on the following criteria: Patients who had
experienced the spontaneous loss of three or more consecutive
pregnancies prior to 20 weeks of gestation were included in the RSM
group. Patients diagnosed with chromosomal abnormalities, uterine
abnormalities, hereditary thrombophilia, endocrinologic disorders,
immunologic factors and infections were excluded. A total of 306
age-matched healthy individuals (Uygur/Han ratio, 1.03) were
enrolled as controls. There was no history of abortions or
fertility treatments and no normal menstrual cycles for the
controls. Informed consent was obtained from each of the subjects
in accordance with the protocol approved by the Human Studies
Committee of Xingjiang Medical University.
Genotyping
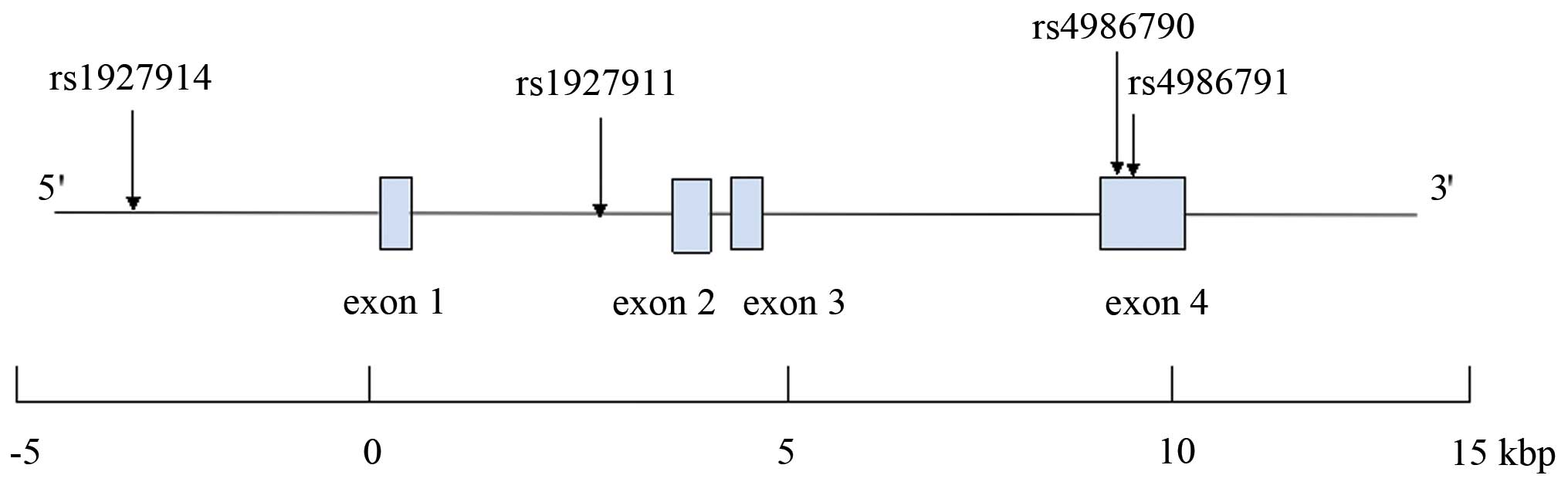
The human TLR4 gene is located on chromosome
9q33.1, spans ~17 kilobase pairs and contains four exons. There are
920 SNPs for the human TLR4 gene listed in the National
Center for Biotechnology Information SNP database Build 130
(http://www.ncbi.nlm.nih.gov/SNP). Data
for tag SNPs was screened using the International HapMap Project
(http://www.hapmap.org/index.html.ja)
using a cutoff level of r2 ≥0.5. According to the above
criteria, rs1927914 (SNP1), rs1927911 (SNP2), rs4986790 (SNP3) and
rs4986791 (SNP4) were selected for the present study. The structure
of the human TLR4 gene is presented in Fig. 1.
Blood samples were collected from each participant
and genomic DNA was extracted from peripheral blood leukocytes by
phenol and chloroform extraction. DNA sequencing using the Sanger
dideoxy method was performed by Polymorphic DNA Technologies
(Alameda, CA, USA). The four SNPs that were used for complete
sequencing of the TLR4 region included a portion of the
upstream region, introns and exons, and these were analyzed in
patients and controls from the cohort. Sequencing reactions were
performed by O&E High-Tech Corporation in Beijing, China, and
sequencing primers were designed using Primer Premier 5.0 software
(Palo Alto, CA, USA).
Genotyping of novel SNPs
The detailed of genotyping of novel SNP have been
previously described (11). Briefly,
DNA sequencing of the complete TLR4 region was performed
using a polymerase chain reaction direct sequencing method, which
identified a heterozygous variant in subjects with RSM and
controls. The sense primer for SNP1 was
5′TAGCATGAGAAATGAGGAAGTAAGGG3′ and the antisense primer was
5′GAGCTATGATGAGGATTGAAAATGTGG3′. The sense primer for SNP2 was
5′TAGCTGGCTTCTGCAAGGAAT3′ and the antisense primer was
5′GGAGACTGTCTGGCAGTCAAGATGT3′. The sense primer for SNP3 was
5′GTCCCTGAACCCTATGAACTTTATCC3′ and the antisense primer was
5′TCCCACCTTTGTTGGAAGTGAAAG3′. The sense primer for SNP4 was
5′CTGGTGAGTGTGACTATTGAAAGGG3′ and the antisense primer was
5′TTAGTACCTGAAGACTGGAGAGTGAG3′. Genotypes were determined
automatically by the signal processing algorithms of Genotyping
Console software 4.1 (Cleveland, OH, USA). To aid in the comparison
of the results, each scoring method were saved in two separate
output files.
Biochemical analysis
Serum concentrations of cholesterol and glucose were
measuring using the standard methods employed by the Clinical
Laboratory Department of the First Affiliated Hospital of Xinjiang
Medical University.
Statistical analysis
All continuous variables were expressed as the mean
± standard deviation. The Mann-Whitney U test was used to compare
differences in continuous variables between RSM patients and
controls. The Fisher's exact test was used to calculate differences
in categorical variables. The Hardy-Weinberg equilibrium was
analyzed using χ2 analysis. The Fisher's exact test was
used to calculate differences in the distribution of genotypes and
alleles between the RSM patients and controls. According to the
genotype data resulting from the genetic variations, linkage
disequilibrium analysis and haplotype-based case-control analysis
was performed using the expectation maximization algorithm and
SNPAlyze version 3.2 (Dynacom Co., Ltd., Yokohama, Japan). The four
SNPs were used to perform pair-wise linkage disequilibrium
analysis. D >0.5 was used to assign SNP locations to one
haplotype block. SNPs with r2 <0.5 were selected as
tagged. A permutation test was used to calculate the frequency
distribution of the haplotypes and P-values in the haplotype-based
case-control analysis. The contribution of major risk factors was
assessed using logistic regression analysis. P<0.05 was
considered to indicate a statistically significant difference.
Statistical analyses were performed using SPSS software for Windows
(version 12; SPSS Inc., Chicago, IL, USA).
Results
Clinical characteristics
Table I presents the
clinical characteristics of the study participants. In Uygur women,
the age of menarche, systolic blood pressure, diastolic blood
pressure and spontaneous miscarriages were significantly higher in
RSM patients compared with the controls (P<0.05). In Han women,
systolic blood pressure, number of pregnancies, spontaneous
miscarriages and the frequency of drinking were significantly
higher in RSM patients compared with the controls (P<0.05).
There were no significant differences noted between RSM patients
and the controls with regards to age, body mass index, pulse rate,
serum cholesterol, serum glucose and the frequency of smoking in
Uygur and Han women.
 | Table I.Characteristics of study
participants. |
Table I.
Characteristics of study
participants.
|
| Uygur | Han |
|---|
|
|
|
|
|---|
| Characteristic | RSM patients | Controls | P-value | RSM patients | Controls | P-value |
|---|
| Number of
subjects | 154 | 155 | – | 152 | 151 | – |
| Age (years) | 35.2±3.7 | 35.1±4.5 | 0.859 | 35.6±4.1 | 35.7±3.8 | 0.643 |
| Body mass index
(kg/m2) | 23.2±2.9 | 22.8±2.7 | 0.261 | 22.5±4.4 | 21.6±3.0 | 0.066 |
| Menarche
(years) | 11.8±2.6 | 12.4±3.9 | 0.002a | 12.3±3.9 | 12.5±4.2 | 0.127 |
| Systolic blood
pressure (mmHg) | 110.8±15.2 | 119.3±14.3 |
<0.001a | 113.1±14.7 | 120.8±13.6 |
<0.001a |
| Diastolic blood
pressure (mmHg) | 71.8±12.5 | 75.2±13.9 |
<0.001a | 75.5±9.7 | 76.6±11.4 | 0.232 |
| Pulse rate
(beats/min) | 75.8±8.1 | 75.1±7.2 | 0.356 | 75.1±6.3 | 74.6±5.8 | 0.438 |
| Cholesterol
(mmol/l) | 5.3±1.1 | 4.7±0.9 | 0.061 | 5.2±1.0 | 4.8±1.1 | 0.132 |
| Glucose
(mmol/l) | 5.2±0.6 | 5.1±0.7 | 0.677 | 5.4±0.3 | 5.3±0.8 | 0.547 |
| Number of
pregnancies | 4.5±0.7 | 4.1±0.5 | 0.125 | 4.2±0.8 | 1.8±0.9 |
<0.001a |
| Spontaneous
miscarriages | 4.1±0.9 | 0±0.0 |
<0.001a | 3.8±0.7 | 0±0.0 |
<0.001a |
| Smoking (%) | 1.9 | 2.6 | 0.500 | 3.3 | 3.3 | 0.621 |
| Drinking (%) | 12.3 | 13.5 | 0.321 | 21.1 | 14.6 | 0.046a |
Distribution of genotypes
Table II presents
the distribution of the genotypes and alleles of the four SNPs. For
each SNP, the genotype distributions in the controls were not
significantly different from the Hardy-Weinberg equilibrium values
(data not shown). In Uygur women, there were significant
differences between the distributions of the rs1927914, rs1927911
and rs4986790 SNPs between the RSM patients and the controls
(P=0.001, P<0.001 and P=0.015, respectively). In Han women,
there were significant differences between the distributions of the
rs1927914 and rs1927911 SNPs between the RSM patients and the
controls (P<0.001 and P<0.001, respectively).
| Table II.Genotype and allele distributions in
RSM patients and controls. |
Table II.
Genotype and allele distributions in
RSM patients and controls.
|
| Uygur | Han |
|---|
|
|
|
|
|---|
|
| RSM patients | Controls | P-value | RSM patients | Controls | P-value |
|---|
| rs1927914
(SNP1) |
|
|
Genotype |
|
|
A/A | 88 (57.1%) | 56 (36.1%) | 0.001a | 90 (59.2%) | 54 (35.8%) |
<0.001a |
|
A/G | 49 (31.8%) | 65 (41.9%) |
| 48 (31.6%) | 64 (42.4%) |
|
|
G/G | 17 (11.1%) | 34 (22.0%) |
| 14 (9.2%) | 33 (21.8%) |
|
|
Allele |
|
|
A | 225 (73.1%) | 177 (57.1%) |
<0.001a | 228 (75.0%) | 172 (57.0%) |
<0.001a |
|
G | 83 (26.9%) | 133 (42.9%) |
| 76 (25.0%) | 130 (43.0%) |
|
| rs1927911
(SNP2) |
|
|
Genotype |
|
|
G/G | 90 (58.4%) | 55 (35.5%) |
<0.001a | 91 (59.9%) | 55 (36.4%) |
<0.001a |
|
G/A | 47 (30.5%) | 73 (47.1%) |
| 45 (29.6%) | 70 (46.4%) |
|
|
A/A | 17 (11.1%) | 27 (17.4%) |
| 16 (10.5%) | 26 (17.2%) |
|
|
Allele |
|
|
G | 227 (73.7%) | 183 (59.0%) |
<0.001a | 227 (73.7%) | 180 (59.6%) |
<0.001a |
|
A | 81 (26.3%) | 127 (41.0%) |
| 81 (26.3%) | 122 (40.4%) |
|
| rs4986790
(SNP3) |
|
|
Genotype |
|
|
A/A | 142 (92.3%) | 152 (98.1%) | 0.015a | 148 (97.4%) | 149 (98.7%) | 0.345 |
|
A/G | 12 (7.7%) | 3 (1.9%) |
| 4 (2.6%) | 2 (1.3%) |
|
|
G/G | 0 (0.0%) | 0 (0.0%) |
| 0 (0.0%) | 0 (0.0%) |
|
|
Allele |
|
|
A | 296 (96.1%) | 307 (99.0%) | 0.016a | 296 (98.7%) | 300 (99.3%) | 0.340 |
|
G | 12 (3.9%) | 3 (1.0%) |
| 4 (1.3%) | 2 (0.7%) |
|
| rs4986791
(SNP4) |
|
|
Genotype |
|
|
C/C | 154 (100%) | 155 (100%) | – | 152 (100%) | 151 (100%) | – |
|
C/T | 0 (0%) | 0 (0%) |
| 0 (0%) | 0 (0%) |
|
|
T/T | 0 (0%) | 0 (0%) |
| 0 (0%) | 0 (0%) |
|
|
Allele |
|
|
C | 308 (100%) | 310 (100%) | – | 304 (100%) | 302 (100%) | – |
|
T | 0 (0%) | 0 (0%) |
| 0 (0%) | 0 (0%) |
|
Risk factors and SNPs
Parameters in Table I
that exhibited significant differences between the RSM patients and
the controls were used for the logistic regression analysis. In
Uygur women, parameters used included SNPs (rs1927914, rs1927911
and rs4986790), the age of menarche, systolic blood pressure,
diastolic blood pressure and spontaneous miscarriages. As shown in
Table III, results of the logistic
regression analysis indicated that the distributions of rs1927914,
rs1927911 and rs4986790 SNPs were significantly different in the
RSM patients compared with the control individuals (P=0.012,
P=0.024 and P=0.035, respectively). In addition, systolic blood
pressure differed significantly between the RSM patients and the
controls (P=0.011, P=0.021 and P=0.032, respectively) in Uygur
women.
| Table III.Odds ratios and 95% confidence
intervals for each risk factor and SNP associated with RSM in Uygur
women. |
Table III.
Odds ratios and 95% confidence
intervals for each risk factor and SNP associated with RSM in Uygur
women.
|
| Uygur |
|---|
|
|
|
|---|
| Risk factor | Odd ratios | 95% confidence
interval | P-value |
|---|
| rs1927914
(SNP1) | 6.86 | 1.934–46.950 | 0.012a |
|
Menarche (years) | 0.731 | 0.343–1.524 | 0.419 |
|
Systolic blood pressure
(mmHg) | 1.135 | 1.029–1.249 | 0.011a |
|
Diastolic blood pressure
(mmHg) | 1.046 | 1.017–1.065 | 0.003a |
|
Spontaneous miscarriages | 0.672 | 0.413–1.089 | 0.121 |
| rs1927911
(SNP2) | 4.824 | 1.203–19.672 | 0.024a |
|
Menarche (years) | 1.771 | 1.070–2.931 | 0.026a |
|
Systolic blood pressure
(mmHg) | 2.421 | 1.091–5.297 | 0.021a |
|
Diastolic blood pressure
(mmHg) | 0.673 | 0.383–1.182 | 0.172 |
|
Spontaneous miscarriages | 0.616 | 0.225–1.683 | 0.345 |
| rs4986790
(SNP3) | 8.272 | 1.168–40.358 | 0.035a |
|
Menarche (years) | 1.121 | 0.351–3.562 | 0.852 |
|
Systolic blood pressure
(mmHg) | 2.487 | 1.089–5.745 | 0.032a |
|
Diastolic blood pressure
(mmHg) | 1.405 | 0.648–3.031 | 0.386 |
|
Spontaneous miscarriages | 2.619 | 1.006–6.811 | 0.047a |
In Han women, parameters used included SNPs
(rs1927914 and rs1927911), systolic blood pressure, number of
pregnancies, spontaneous miscarriages and the frequency of
drinking. As shown in Table IV,
results of the logistic regression analysis indicated that the
distributions of rs1927914 and rs1927911 SNPs were significantly
different in the RSM patients compared with the control individuals
(P=0.021 and P=0.004, respectively) in Han women.
| Table IV.Odds ratios and 95% confidence
intervals for each risk factor and SNP associated with RSM in Han
women. |
Table IV.
Odds ratios and 95% confidence
intervals for each risk factor and SNP associated with RSM in Han
women.
|
| Han |
|---|
|
|
|
|---|
| Risk factor | Odd ratios | 95% confidence
interval | P-value |
|---|
| rs1927914
(SNP1) | 6.431 | 1.321–31.347 | 0.021a |
|
Systolic blood pressure
(mmHg) | 1.967 | 1.071–3.589 | 0.037a |
| Number
of pregnancies | 1.185 | 0.597–2.358 | 0.634 |
|
Spontaneous miscarriages | 0.412 | 0.113–1.514 | 0.186 |
|
Drinking (%) | 1.579 | 0.807–3.076 | 0.183 |
| rs1927911
(SNP2) | 2.234 | 1.271–3.917 | 0.004a |
|
Systolic blood pressure
(mmHg) | 1.127 | 1.029–1.235 | 0.008a |
| Number
of pregnancies | 1.156 | 0.933–1.435 | 0.187 |
|
Spontaneous miscarriages | 1.046 | 1.022–1.074 | 0.001a |
|
Drinking (%) | 1.970 | 0.632–6.145 | 0.249 |
Haplotypes
Since most of the D-values of linkage disequilibrium
for the human TLR4 gene in the controls were >0.5 (data
not shown), this indicated that the four SNPs were located in one
haplotype block. Since all of the r2 values were <0.5
(data not shown), this suggests that every SNP would be useful for
the haplotype-based case-control study. Since rs4986791 (SNP4) has
no allele distributions in RSM patients and the controls in this
study, haplotypes were constructed using SNP1, SNP2 and SNP3. The
distributions of the individual haplotypes for these combinations
of the three SNPs were analyzed, and the results are presented in
Table V. In Uygur women,
significantly higher frequencies were noted for the A-G-G haplotype
(SNP1-SNP2-SNP3; P=0.016) in RSM patients compared with the
controls.
| Table V.Haplotype analysis in RSM patients
and controls. |
Table V.
Haplotype analysis in RSM patients
and controls.
|
| Haplotype | Frequency in
Uygur |
| Frequency in
Han |
|
|---|
|
|
|
|
|
|
|
|---|
| No. | SNP1 | SNP2 | SNP3 | RSM patients | Controls | P-value | RSM patients | Controls | P-value |
|---|
| H1 | G | A | A | 0.164 | 0.236 | 0.756 | 0.177 | 0.282 | 0.412 |
| H2 | G | G | A | 0.086 | 0.187 | 0.298 | 0.067 | 0.145 | 0.398 |
| H3 | G | G | G | 0.019 | 0.006 | 0.540 | 0.006 | 0.003 | 0.158 |
| H4 | A | A | A | 0.099 | 0.174 | 0.389 | 0.086 | 0.122 | 0.415 |
| H5 | A | G | A | 0.632 | 0.393 | 0.633 | 0.658 | 0.445 | 0.406 |
| H6 | A | G | G | 0.020 | 0.004 | 0.016a | 0.006 | 0.003 | 0.137 |
Discussion
RSM is a reproductive problem, which affects 1–3% of
couples trying to conceive (12).
Epidemiological studies have suggested that RSM comprises a
multifactorial condition enhanced by a variety of genetic and
environmental factors (13). A
number of studies have suggested that RSM is associated with
genetic disorders that include skewed X chromosome inactivation
(14), HLA-G (15), age-related aneuploidy (16), autoimmune disorders (17) and acquired or inherited thrombophilia
(18). In addition, several studies
have shown that nutritional and lifestyle factors, smoking, and
diet (19,20) contribute to RSM pathogenesis. For
instance, obesity has a greater incidence in RSM patients compared
with controls (21). Furthermore, a
woman's medical history (3) is
important since the risk of RSM is increased by previous
miscarriages (20% after one miscarriage, 28% after two
miscarriages) and age (40% risk for 40 year-old women, and 80% for
women 45 and older). Considering all these risk factors, the
related data (including age, body mass index, number of pregnancies
and number of spontaneous miscarriages) has been collected and
presented in Table I. Then, the
relationship between these risk factors and RSM is analyzed using
logistic regression and presented in Tables III and IV.
TLR4 is present in numerous cell types and signals
the innate immune response. TLR4 expression has been investigated
in tumor cells or cell lines, including extranodal marginal zone
B-cell lymphomas, gastric carcinoma, hepatocellular carcinoma
cells, pituitary epithelial tumor cell lines, colon cancer cells
and human prostate epithelial PC3 cells (22). The innate immune system is the first
line of defense against microbial infection and TLR4 serves as the
first point of defense in the innate immune system. TLR4 is one of
the most extensively investigated TLRs and recognizes endotoxic
lipopoly saccharide (LPS) in the outer membrane of Gram-negative
bacteria with its co-receptor MD-2 (23). TLR4 is critical in the recognition of
viruses and bacteria, serving as a key immune system effector.
Excessive signaling in response to LPS frequently results in
uncontrolled amplification of inflammatory responses, leading to
fatal septic shock (24,25).
Dysregulation of TLR4 signalling owing to SNPs may
alter the ligand binding and balance between pro- and
anti-inflammatory cytokines, thereby modulating the risk of chronic
inflammatory and immune disorders. Consequently, several studies
have shown that common SNPs of a series of low penetrance alleles
of TLR4, modified during the above mentioned processes, are likely
to serve an important role in cancer susceptibility (26,27). Two
SNPs of the human TLR4, A299G (ref SNP ID: rs4986790, SNP3) and
T399I (ref SNP ID: rs4986791, SNP4), have been identified and
suggested to be associated with LPS hyporesponsiveness (28,29).
Furthermore, two non-synonymous polymorphisms of TLR4 (Asp299Gly
and Thr399Ile) have been suggested to alter the function of the
receptor (30,31) and have been related to the
development of chronic inflammatory conditions (32). In addition, Hirschfeld et al
(33) reported that there was no
association between fetal TLR4 polymorphisms, Asp299Gly and
Thr399Ile, known to blunt LPS responsiveness, and the risk of
idiopathic, chromosomally normal miscarriage. However, how the SNPs
affect the function of TLR4 remains largely unknown.
The aim of the present study was to assess the
association between the human TLR4 gene and RSM in Uygur and
Han women in Xinjiang by using a haplotype-based case-control
study. The results of the genotype distributions and logistic
regression analysis indicated that rs1927914, rs1927911 and
rs4986790 are most likely associated with RSM in Uygur women, while
rs1927914 and rs1927911 are most likely associated with RSM in Han
women. Additionally, logistic regression analysis indicated that
systolic blood pressure is one of the risk factors for RSM
patients, which is consistent with results of a previous study
(34).
It has been demonstrated that haplotypes can provide
valuable information that can be used for predicting the severity
and prognosis of certain genetic disorders (35). With the dramatic increase in the
number of available SNP markers, haplotyping based on genotype data
has become an important component of genetic studies in general and
has shown that these types of studies have a number of advantages
over analyses that are just based on individual SNPs (36). In the present study, haplotypes for
the human TLR4 gene were successfully established that were
created from the combinations of the three SNPs. In the present
haplotype analysis, there was a significantly higher frequency of
the A-G-G haplotype (SNP1-SNP2-SNP3) in RSM patients compared with
the controls in Uygur women. Therefore, it can be suggested that
the result indicates that the A-G-G haplotype (SNP1-SNP2-SNP3) is
the susceptibility haplotype for RSM in Uygur women, and it can be
proposed that the A-G-G haplotype (SNP1-SNP2-SNP3) should be
regarded as the genetic marker for RSM in Uygur women in Xinjiang.
In addition, for SNP3, the G allele is the risk allele while the A
allele is the safe allele for RSM in Uygur women.
To date, to the best of our knowledge, there have
been no previous studies that have reported data on the association
between TLR4 and RSM in Uygur women. Therefore, the current results
provide novel data on the possibility that the TLR4 gene is
most likely associated with RSM, and rs4986790 may be the
nationality-specific genetic marker for RSM for Uygur women.
In conclusion, the present study examined the
association between the human TLR4 gene and RSM. The present
results indicate that rs1927914, rs1927911, rs4986790 and the A-G-G
haplotype of the human TLR4 gene may be genetic markers for
RSM in Uygur women in Xinjiang. In addition, the results suggest
that rs1927914 and rs1927911 of the human TLR4 gene are most
likely associated with RSM in Han women. Further studies are
required to elucidate the functional association of TLR4 with RSM
progression.
References
|
1
|
Rai R and Regan L: Recurrent miscarriage.
Lancet. 368:601–611. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Cramer DW and Wise LA: The epidemiology of
recurrent pregnancy loss. Semin Reprod Med. 18:331–339. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ford HB and Schust DJ: Recurrent pregnancy
loss: Etiology, diagnosis, and therapy. Rev Obstet Gynecol.
2:76–83. 2009.PubMed/NCBI
|
|
4
|
Akira S and Takeda K: Functions of
toll-like receptors: Lessons from KO mice. C R Biol. 327:581–589.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kawai T and Akira S: The role of
pattern-recognition receptors in innate immunity: Update on
Toll-like receptors. Nat Immunol. 11:373–384. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Marshak-Rothstein A: Toll-like receptors
in systemic autoimmune disease. Nat Rev Immunol. 6:823–835. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Schroder NW and Schumann RR: Single
nucleotide polymorphisms of toll-like receptors and susceptibility
to infectious disease. Lancet Infect Dis. 5:156–164. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Horie Y, Meguro A, Ota M, Kitaichi N,
Katsuyama Y, Takemoto Y, Namba K, Yoshida K, Song YW, Park KS, et
al: Association of TLR4 polymorphisms with Behcet's disease in a
Korean population. Rheumatology (Oxford). 48:638–642. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Pabst S, Baumgarten G, Stremmel A, Lennarz
M, Knüfermann P, Gillissen A, Vetter H and Grohé C: Toll-like
receptor (TLR) 4 polymorphisms are associated with a chronic course
of sarcoidosis. Clin Exp Immunol. 143:420–426. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Frantz S, Ertl G and Bauersachs J:
Mechanisms of disease: Toll-like receptors in cardiovascular
disease. Nat Clin Pract Cardiovasc Med. 4:444–454. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Varshney RK, Kudapa H, Roorkiwal M, Thudi
M, Pandey MK, Saxena RK, Chamarthi SK, Mohan SM, Mallikarjuna N,
Upadhyaya H, et al: Advances in genetics and molecular breeding of
three legume crops of semi-arid tropics using next-generation
sequencing and high-throughput genotyping technologies. J Biosci.
37:811–820. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sierra S and Stephenson M: Genetics of
recurrent pregnancy loss. Semin Reprod Med. 24:17–24. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Cramer DW and Wise LA: The epidemiology of
recurrent pregnancy loss. Semin Reprod Med. 18:331–339. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kuo PL, Huang SC, Chang LW, Lin CH, Tsai
WH and Teng YN: Association of extremely skewed X-chromosome
inactivation with Taiwanese women presenting with recurrent
pregnancy loss. J Formos Med Assoc. 107:340–343. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Pfeiffer KA, Fimmers R, Engels G, van der
Ven H and van der Ven K: The HLA-G genotype is potentially
associated with idiopathic recurrent spontaneous abortion. Mol Hum
Reprod. 7:373–378. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hodes-Wertz B, Grifo J, Ghadir S, Kaplan
B, Laskin CA, Glassner M and Munné S: Idiopathic recurrent
miscarriage is caused mostly by aneuploid embryos. Fertil Steril.
98:675–680. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Finan RR, Al-Irhayim Z, Mustafa FE,
Al-Zaman I, Mohammed FA, Al-Khateeb GM, Madan S, Issa AA and Almawi
WY: Tumor necrosis factor-alpha polymorphisms in women with
idiopathic recurrent miscarriage. J Reprod Immunol. 84:186–192.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Paidas MJ, Ku DH, Langhoff-Roos J and
Arkel YS: Inherited thrombophilias and adverse pregnancy outcome:
Screening and management. Semin Perinatol. 29:150–163. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Metwally M, Saravelos SH, Ledger WL and Li
TC: Body mass index and risk of miscarriage in women with recurrent
miscarriage. Fertil Steril. 94:290–295. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Dasarathy J, Gruca LL, Bennett C, Parimi
PS, Duenas C, Marczewski S, Fierro JL and Kalhan SC: Methionine
metabolism in human pregnancy. Am J Clin Nutr. 91:357–365. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
O'Dwyer V, Monaghan B, Fattah C, Farah N,
Kennelly MM and Turner MJ: Miscarriage after sonographic
confirmation of an ongoing pregnancy in women with moderate and
severe obesity. Obes Facts. 5:393–398. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Bulut Y, Faure E, Thomas L, Karahashi H,
Michelsen KS, Equils O, Morrison SG, Morrison RP and Arditi M:
Chlamydial heat shock protein 60 activates macrophages and
endothelial cells through toll-like receptor 4 and MD2 in a
MyD88-dependent pathway. J Immunol. 168:1435–1440. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Poltorak A, He X, Smirnova I, Liu MY, Van
Huffel C, Du X, Birdwell D, Alejos E, Silva M, Galanos C, et al:
Defective LPS signalingin C3H/HeJ and C57BL/10ScCr mice: Mutations
in Tlr4 gene. Science. 282:2085–2088. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Angus DC, Linde-Zwirble WT, Lidicker J,
Clermont G, Carcillo J and Pinsky MR: Epidemiology of severe sepsis
in the United States: Analysis of incidence, outcome, and
associated costs of care. Crit Care Med. 29:1303–1310. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Rangel-Frausto MS: Sepsis: Still going
strong. Arch Med Res. 36:672–681. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Zidi S, Verdi H, Yilmaz-Yalcin Y, Yazici
AC, Gazouani E, Mezlini A, Atac FB and Yacoubi-Loueslati B:
Involvement of Toll-like receptors in cervical cancer
susceptibility among Tunisian women. Bull Cancer. 101:E31–E35.
2014.PubMed/NCBI
|
|
27
|
He C, Tu H, Sun L, Xu Q, Gong Y, Jing J,
Dong N and Yuan Y: SNP interactions of Helicobacter pylori-related
host genes PGC, PTPN11, IL1B, and TLR4 in susceptibility to gastric
carcinogenesis. Oncotarget. 6:19017–19026. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Rallabhandi P, Bell J, Boukhvalova MS,
Medvedev A, Lorenz E, Arditi M, Hemming VG, Blanco JC, Segal DM and
Vogel SN: Analysis of TLR4 polymorphic variants: New insights into
TLR4/ MD-2/CD14 stoichiometry, structure, and signaling. J Immunol.
177:322–332. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Figueroa L, Xiong Y, Song C, Piao W, Vogel
SN and Medvedev AE: The Asp299Gly polymorphism alters TLR4
signaling by interfering with recruitment of MyD88 and TRIF. J
Immunol. 188:4506–4515. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Arbour NC, Lorenz E, Schutte BC, Zabner J,
Kline JN, Jones M, Frees K, Watt JL and Schwartz DA: TLR4 mutations
are associated with endotoxin hyporesponsiveness in humans. Nat
Genet. 25:187–191. 2000. View
Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ferwerda B, McCall MB, Verheijen K,
Kullberg BJ, van der Ven AJ, Van der Meer JW and Netea MG:
Functional consequences of Toll-like receptor 4 polymorphisms. Mol
Med. 14:346–352. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Radstake TR, Franke B, Hanssen S, Netea
MG, Welsing P, Barrera P, Joosten LA, van Riel PL and van den Berg
WB: The toll-like receptor 4 Asp299Gly functional variant is
associated with decreased rheumatoid arthritis disease
susceptibility but does not influence disease severity and/or
outcome. Arthritis Rheum. 50:999–1001. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Hirschfeld AF, Jiang R, Robinson WP,
McFadden DE and Turvey SE: Toll-like receptor 4 polymorphisms and
idiopathic chromosomally normal miscarriage. Hum Reprod.
22:440–443. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Almawi WY, Saldanha FL, Mahmood NA,
Al-Zaman I, Sater MS and Mustafa FE: Relationship between VEGFA
polymorphisms and serum VEGF protein levels and recurrent
spontaneous miscarriage. Hum Reprod. 28:2628–2635. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Chen CK, Yu HT, Soong YK and Lee CL: New
perspectives on preimplantation genetic diagnosis and
preimplantation genetic screening. Taiwan J Obstet Gynecol.
53:146–150. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Stein CM and Elston RC: Finding genes
underlying human disease. Clin Genet. 75:101–106. 2009. View Article : Google Scholar : PubMed/NCBI
|