Introduction
Venous malformations (VM) is the most common
vascular malformation in clinical practice, and its incidence is
1/5,000–1/10,000 with 40% in the head and neck (1). The most common treatment methods at
present include surgical excision, freezing, laser, injection
sclerotherapy and microwave irradiation (2,3). The
above methods are effective in treating low reflux VM with limited
scope of lesion. However, there is a lack of effective means to
treat with the deep and extensive high-return flow VM that are
involved at multiple anatomical partitions. At present, the
predominant way to treat with the high-return flow VM is
comprehensive sequence therapy that focuses on digital subtraction
angiography (DSA)-guided anhydrous ethanol injection sclerotherapy
(4).
In the present study, we applied radiofrequency (RF)
ablation in addition to the anhydrous ethanol injection
sclerotherapy and achieved very good curative effects without any
obvious adverse reactions.
Patients and methods
Patients
A total of 41 patients diagnosed with head and neck
VM in the Department of Stomatology, Xuzhou Hospital Affiliated to
Southeast University (Jiangsu, China) were enrolled in the study.
Of the 41 patients, 15 were male and 26 female, with an age range
of 5–61 years. The sites of lesions included: tongue, parotid,
neck, cheek, lower eyelid, forehead, lips and throat. The average
volume of tumor was 5.0×2.0×1.5–16.0×12.0×5.0 cm. Inclusion
criteria of the study were: i) Patients that were confirmed with
type III, or type IV VM under image classification (5), and had received no treatment before
surgery; ii) patients without history of serious cardiovascular and
cerebrovascular disease and alcohol allergy; iii) patients that
were confirmed with normal preoperative blood routine, liver
function, renal function, electrocardiogram and chest X-ray
examination; and iv) all of the enrolled patients were quite clear
of the content of the study and provided written informed consent.
The patients were randomly divided into the anhydrous ethanol
injection + RF group (treatment group) and pure anhydrous ethanol
injection group (control group). Table
I presents the general information and the tumor diameter of
the two groups of patients. After statistical comparison, it was
found that the differences between the two groups were not
statistically significant (P>0.05), with comparability. The
study was approved by the Ethics Committee of the Central Hospital
of Xuzhou. Written informed consent was obtained from all the
participants or their families prior to the start of the study.
 | Table I.Distribution of patients and control
groups according to site of lesion. |
Table I.
Distribution of patients and control
groups according to site of lesion.
|
|
| Gender (case) |
|
| Site of focus
(case) |
|---|
|
|
|
|
|
|
|
|---|
| Group | Case | Male | Female | Average age (years,
mean ± SD) | Diameter of tumor
(cm, mean ± SD) | Tongue | Parotid | Cheek | Lip | Throat | Forehead | Lower eyelid | Neck |
|---|
| Treatment | 19 | 6 | 13 | 33.3±17.6 | 9.9±1.6 | 4 | 2 | 4 | 4 | 1 | 1 | 1 | 2 |
| Control | 22 | 9 | 13 | 35.7±13.9 | 9.5±2.0 | 6 | 3 | 5 | 3 | 2 | 1 | 1 | 1 |
Treatment methods
Patients in the control group were treated using
DSA-guided anhydrous ethanol injection sclerotherapy. Treatment was
conducted under general or local anesthesia. During the operation,
pulmonary arterial pressure was examined. With use of no. 7
butterfly needle a puncture was made into the deep part of the
tumor cavity through the skin, then contrast agent was injected
(30% meglumine diatrizoate) after blood reflux and reflux venous
development was observed. DSA was performed according to the
recorded dose of contrast agent and then rapidly absolute ethyl
alcohol was injected several times at rate of 0.5 ml/sec. After 15
min, another DSA was performed, with injection pressure at
13.3–26.7 kPa, each injection for 0.5–1.5 ml. This was repeated
once again 2–5 min later. The injection amount of absolute ethyl
alcohol was about 1/2–1/3 of the contrast agent. The maximum dose
for one injection was not over 1 ml/kg. After injection, the
patients' blood pressure and heart rate were observed. The patients
with 0.5 ml/kg injection, were monitored for their blood pressure
and the urine volume. Equilibrium liquid, dexamethasone, sodium
bicarbonate and proper amount of antibiotics were injected i.v. to
prevent the occurrence of edema, renal function damage, infection
and other adverse reactions.
Patients in the treatment group were
treated by RF before anhydrous ethanol injection sclerotherapy
RF was performed under local anesthesia. R-2000BD1
bipolar radiofrequency thermal coagulation was applied with the
therapy apparatus (Beijing BNS Medical Co., Ltd., Beijing, China).
The electrode needle was punctured into the tumor through the head
and neck skin or oral mucosa. The area of abundant blood supply was
identified according to the impedance value of the puncture region
detected by the computer. After the needle core was removed, blood
return could be seen. Then RF was performed in this region. The RF
output power was 30–40 W, and the total heating coagulation of a
single lesion lasted for 10–15 min. Multiple heat coagulation could
be carried out and each heat coagulation area had some overlap. The
normal tissues (0.5–1.0 mm) were taken in the tumor within the
treatment range, as the standard. After treatment, the RF ablation
therapeutic instrument was adjusted into needle tract mode, pulled
out the electrode needle, pressed to stop bleeding, and observed
the changes of vital signs in the operation. Deep VMs can be
treated by puncture under the guidance of color Doppler ultrasound.
One month later, proper amount of anhydrous ethanol hardener was
injected according to the change of tumor size. Methods referred to
the control group.
Evaluation on clinical curative
effects
Evaluation was made according to the grading
standard of Achauer et al (6): level I (poor), tumor shrank by 0–25%;
level II (moderate), tumor shrank by 26–50%; level III (good),
tumor shrank by 51–75%; level IV (superior), tumor shrank by
76–100%. Level III and IV were considered to be effective; level I
and II were considered to be non-effective. The treatment was
continued with the aforesaid method if it was effective. The
general and side adverse reactions of the patients were closely
monitored during treatment. All patients had local swelling and
pain after operation, which was relieved within 3–5 days. It was
considered to be a reaction of hardening agent or physical
treatment mechanism. Thus, it was not included as an adverse
reaction.
Statistical processing
SPSS 17.0 (Chicago, IL, USA) was used for
statistical analysis. Measurement data were presented as mean ±
standard deviation and the t-test was used for comparisons. The
χ2 test was used for comparison of countable data.
P<0.05 was considered to be statistically significant.
Results
Curative effects
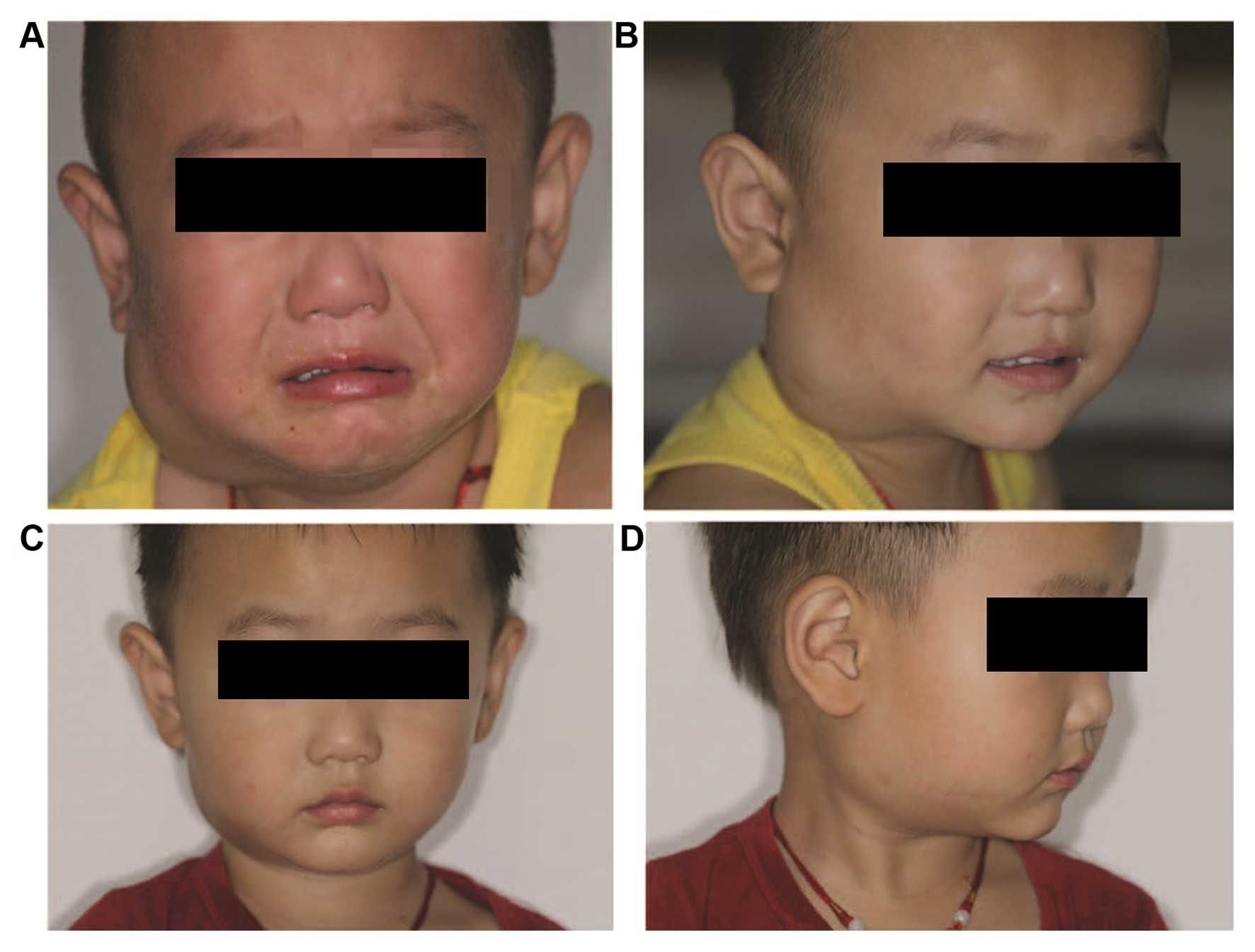
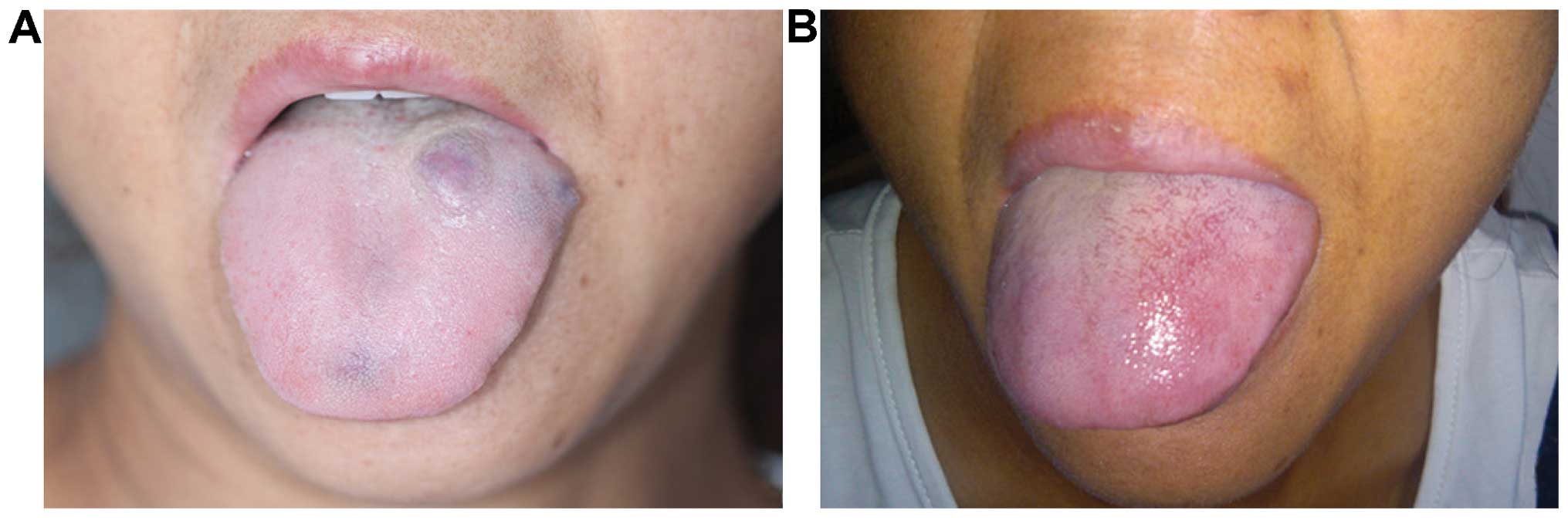
The curative effects of the two groups are shown in
Table II. In the treatment group
the treatment times were significantly less than those of the
control group (P<0.05). The results of MRI examinations were
compared before treatment and 8 weeks after the last treatment to
obtain the final efficacy. It was found that the effective rate of
the treatment group was significantly better than the control group
(P<0.05). Figs. 1–3 show typical cases.
| Table II.Clinical effects of the two
groups. |
Table II.
Clinical effects of the two
groups.
|
|
|
| Clinical curative
effect evaluation |
|---|
|
|
|
|
|
|---|
| Group | Case | Treatment times | Superior (case) | Good (case) | Moderate (case) | Poor (case) | Effective rate
(%) |
|---|
| Treatment | 19 |
1.84±0.83a | 13 | 5 | 1 | 0 | 94.7b |
| Control | 22 | 2.55±0.96 | 8 | 10 | 4 | 0 | 81.8 |
Complications
Throughout the course of treatment, a total of 8
patients had local mucosa or skin necrosis, which healed after
local dressing. In the treatment group, 2 patients had bleeding in
puncture point, but were well controlled after pressing; 1 patient
with pharyngeal VM had fever, accompanied with nausea and vomiting,
and was relieved after expectant treatment. In the control group,
one patient had hemoglobinuria, which disappeared 3 days later, and
no renal function damage was found during the follow-up period; 3
patients with deep VM in parotid region, after the second
sclerotherapy, had the symptoms of disappearing forehead lines and
shallowing nasolabial groove. After neurotrophic drug treatment and
functional treatment, 2 patients returned to normal while the other
case has failed to recover after 11-month follow-up. Table III provides details regarding
complications.
| Table III.The post-treatment reaction and
complication of the two groups. |
Table III.
The post-treatment reaction and
complication of the two groups.
| Complication | Treatment group
(n=19) (%) | Control group (n=22)
(%) |
|---|
| Fever | 0 (0) | 1 (4.55) |
| Nausea/vomiting | 0 (0) | 1 (4.55) |
| Skin, mucosal
necrosis | 2 (10.53) | 6 (27.27) |
| Hemoglobinuria | 0 (0) | 1 (4.55) |
| Facioplegia | 1 (5.26) | 2 (9.09) |
| Hemorrhage | 2 (10.53) | 0 (0) |
Discussion
In recent years, sclerotherapy has replaced surgical
treatment and has become the major treatment method for VMs
(7). The most commonly used
hardeners in China include pingyangmycin, anhydrous ethanol,
lauromacrogol, and recently, it has been reported that bleomycin
has positive effects in the treatment of VMs. For the superficial
VM with limited lesion (8),
intra-tumoral injection of the above hardeners could achieve very
good curative effects. However, the patients whose lesions occur in
the head and neck featured by complicated anatomic structure are
usually dispersed high reflux VM. For this type of patients, the
comprehensive sequence therapy that focuses on DSA-guided anhydrous
ethanol injection sclerotherapy is usually considered to be quite
effective (9–11). Anhydrous ethanol is a powerful
hardening agent that could denature the hemoglobin by damaging the
vascular endothelial cells and form permanent thrombosis and
fibrosis. It has been confirmed that anhydrous ethanol has better
embolization effects on the VM reflux vein and cavity than other
hardening agents (12). Although its
curative effects are significant, its damage on the surrounding
tissues cannot be ignored. It is always accompanied with serious
complications, including pulmonary embolism, hemoglobinuria, renal
failure, upper respiratory tract obstruction and permanent facial
paralysis (13,14). A basic study has reported that
ethanol can disrupt the formation of motor root myelin sheath of
the facial nerves and may have a permanent effect on the nervous
system (15).
RF ablation is a type of physical therapy. It has
been confirmed to be effective and safe in the treatment of
vascular disease. Therefore, it has been considered to be quite
suitable for the treatment of giant vascular lesions (d >5 cm)
(8,16). The application of pure RF in head and
neck VM has been previously reported (17,18). A
retrospective study found that applying RF in large scale VM could
significantly reduce the dosage of traditional hardening agent, and
also effectively reduce the bleeding during operation (17). However, to the best of our knowledge,
no report on the combined use of RF and traditional treatment
method is available. In the current study, we applied RF and
DSA-guided anhydrous ethanol injection sclerotherapy in treatment
with the high-return flow VM. According to the literature, the
effective rate of pure hardener on VM was 75–95% (19). In our study, the effective rate of
the control group was 81.8% while the effective rate of the
treatment group was 94.7%, significantly higher than the control
group. Additionally, the treatment times of the treatment group
were less than those of the control group.
Selecting the appropriate dose of anhydrous ethanol
according to the volume of tumor is significant for preventing side
effects (19,20). Excessive anhydrous ethanol injection
may lead the anhydrous ethanol flow back to the supplying artery,
and result in the necrosis of skin and mucous membrane. Applying RF
ablation to reduce the volume of tumor, then combining with
anhydrous ethanol injection may reduce the number and dosage of
injection, and decrease the risks of side reactions. In the present
study, the incidence of adverse reaction of the control group
reached 50%, significantly higher than that of the treatment group,
especially in the parotid region. The bipolar radiofrequency
temperature control and thermal coagulation therapy apparatus can
preliminarily determine the location of puncture needle by
measuring the impedance of the needle, thereby avoiding damage to
the nerve tissue (impedance, 400–550) (21). Thus, the particular performance of RF
may avoid damaging the facial nerve and reducing the occurrence of
facial paralysis. However, these findings remain to be corroborated
in larger cohorts.
The results of the present study have shown that RF
combined anhydrous ethanol injection sclerotherapy cannot only
improve the effect of local treatment, but also reduce the
incidence of adverse reactions. However, prior to treatment,
attention should be paid to its indications and contraindications:
i) for the VM in parotid region involving facial nerve, attention
must be paid to the depth and direction of RF puncture needle
insertion. Cautious control of the temperature to prevent the
occurrence of facial paralysis. While injecting anhydrous ethanol
into this region, we shall embolize the reflux vein as far as
possible and eliminate the tumor cavity by heat coagulation; ii)
for the VM in pharynx oralis, attention should be paid to the
prevention of the upper airway obstruction resulting from tissue
swelling and necrosis; and iii) for the VM in eyelid, attention
should be paid to the temperature of heat coagulation. The
temperature must not be extremely high, or it may injury the
eyeball. In conclusion, RF combined DSA-guided anhydrous ethanol
injection sclerotherapy provides a new way for treatment of
high-return flow VM.
Acknowledgements
The present study was supported by the Jiangsu
Province Special Program of Medical Science (BL2013008).
References
|
1
|
Dubois J and Garel L: Imaging and
therapeutic approach of hemangiomas and vascular malformations in
the pediatric age group. Pediatr Radiol. 29:879–893. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hou R, Guo J, Hu K, Yang Y, Wang L, Kong
L, Liu G and Lei D: A clinical study of ultrasound-guided
intralesional injection of bleomycin A5 on venous malformation in
cervical-facial region in China. J Vasc Surg. 51:940–945. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Dompmartin A, Vikkula M and Boon LM:
Venous malformation: Update on aetiopathogenesis, diagnosis and
management. Phlebology. 25:224–235. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yakes WF, Gibson MD and Parker SH: Alcohol
embolotherapy of vascular malformations. Semin Interv Cardiol.
6:146–161. 1989. View Article : Google Scholar
|
|
5
|
Puig S, Casati B, Staudenherz A and Paya
K: Vascular low-flow malformations in children: current concepts
for classification, diagnosis and therapy. Eur J Radiol. 53:35–45.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Achauer BM, Chang CJ and Vander Kam VM:
Management of hemangioma of infancy: review of 245 patients. Plast
Reconstr Surg. 99:1301–1308. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Greene AK and Alomari AI: Management of
venous malformations. Clin Plast Surg. 38:83–93. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Garg S, Kumar S and Singh YB:
Intralesional radiofrequency in venous malformations. Br J Oral
Maxillofac Surg. 53:213–216. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Eivazi B and Werner JA: Venous and
arteriovenous malformations in the head and neck region.
Therapeutic options and challenges. HNO. 62:19–24. 2014.(In
German). View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Judith N, Ulrike E, Siegmar R, Matthias N
and Jürgen H: Current concepts in diagnosis and treatment of venous
malformations. J Craniomaxillofac Surg. 42:1300–1304. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Meng J, Zhuang QW, Gu QP, Zhang J, Li ZP
and Si YM: Digital subtraction angiography (DSA) guided sequential
sclerotherapy for maxillofacial vein malformation. Eur Rev Med
Pharmacol Sci. 18:1709–1712. 2014.PubMed/NCBI
|
|
12
|
Goyal M, Causer PA and Armstrong D: Venous
vascular malformations in pediatric patients: comparison of results
of alcohol sclerotherapy with proposed MR imaging classification.
Radiology. 223:639–644. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lee KB, Kim DI, Oh SK, Do YS, Kim KH and
Kim YW: Incidence of soft tissue injury and neuropathy after
embolo/sclerotherapy for congenital vascular malformation. J Vasc
Surg. 48:1286–1291. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Odeyinde SO, Kangesu L and Badran M:
Sclerotherapy for vascular malformations: Complications and a
review of techniques to avoid them. J Plast Reconstr Aesthet Surg.
66:215–223. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Komatsu S, Sasaki Y and Shiota K: A
quantitative study of the facial nerve in mice prenatally exposed
to ethanol. Congenit Anom (Kyoto). 43:41–45. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zou H, Yan J, Wu YX, Ou X, Li XW, Xia F,
Ma KS and Bie P: The new technology of enhanced radiofrequency
ablation is safe and effective for treating giant hepatic
hemangioma. Zhonghua Gan Zang Bing Za Zhi. 20:261–265. 2012.(In
Chinese). PubMed/NCBI
|
|
17
|
Kim AH, Ko HK, Won JY and Lee DY:
Percutaneous radiofrequency ablation: A novel treatment of facial
venous malformation. J Vasc Surg. 50:424–427. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Civelek S, Sayin I, Ercan I, Cakir BO and
Turgut S: Bipolar radiofrequency-induced interstitial
thermoablation for oral cavity vascular malformations: Preliminary
results in a series of 5 children. Ear Nose Throat J. 91:488–492.
2012.PubMed/NCBI
|
|
19
|
Lee CH and Chen SG: Direct percutaneous
ethanol instillation for treatment of venous malformation in the
face and neck. Br J Plast Surg. 58:1073–1078. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Liu Y, Liu D, Wang Y, Zhang W and Zhao F:
Clinical study of sclerotherapy of maxillofacial venous
malformation using absolute ethanol and pingyangmycin. J Oral
Maxillofac Surg. 67:98–104. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Oturai AB, Jensen K, Eriksen J and Madsen
F: Neurosurgery for trigeminal neuralgia: comparison of alcohol
block, neurectomy, and radiofrequency coagulation. Clin J Pain.
12:311–315. 1996. View Article : Google Scholar : PubMed/NCBI
|