Introduction
In conventional in vitro fertilization (IVF),
the incidence of total fertilization failure (TFF) has been
reported to range from 5 to 10% (1).
Considering the stress and financial costs associated with
fertility treatment, TFF is a catastrophic event for patients who
already have been under fertility-induced pressure. Various methods
have been explored to avoid this undesirable IVF result.
Rescue intracytoplasmic sperm injection (R-ICSI), in
which ICSI is performed on oocytes that have failed to fertilize,
has been proposed to counteract TFF. Although sporadic cases of
success have been reported (2,3), the
effectiveness of R-ICSI is not satisfactory due to oocyte aging
in vitro, that is, a delayed ICSI procedure and
asynchronized endometrium (4,5). In
order that R-ISCI is conducted within the oocyte fertilization
window, Chen and Kattera (6) removed
granulosa cells from around oocytes after co-culturing the
cumulus-oocyte complex (COC) with sperm for 6 h to determine the
fertilization status. The unfertilized oocytes, defined by those
being without the presence of the second polar body, were subjected
to R-ICSI at 6 h post-insemination. This insemination method has
been appraised and adopted by numerous clinics recently, not only
due to the advantage of averting TFF, but also the theoretical
benefit of reducing potential damage caused by sperm metabolic
waste products such as free oxygen radicals (7,8).
However, the efficacy of the short co-culture time
with sperm remains unclear. The removal of early cumulus cells may
impact embryo development (9), and
the effectiveness of early R-ICSI remains debatable (10). The aim of the present study was to
evaluate the impact of a short insemination time on embryo
development, assess the reliability of the fertilization checking
procedure prior to the appearance of pronuclei and elucidate the
role of R-ICSI.
Subjects and methods
Patients
This study was a prospective cohort pair control
study. From December 2013 to May 2014, a total of 165 cycles were
included in the study. This study was conducted in accordance with
the Declaration of Helsinki, and with approval from the Ethics
Committee of the Third Affiliated Hospital of Zhengzhou University
(Zhengzhou, China). Written informed consent was obtained from all
participants.
The inclusion criteria were as follows: Patients had
>9 eggs, were aged <38 years, and had normal semen samples
according to WHO criteria 5th edition (11). The eggs of each patient were divided
into one half for conventional IVF (insemination time, 20 h) and
the other half for short insemination (insemination time, 5 h).
R-ICSI was performed where TFF was deemed to have occurred in the
short insemination group following the early fertilization check.
Embryo transfers were divided randomly into two groups depending on
whether the transferred embryos originated from the conventional or
the short insemination.
Ovarian stimulation and oocyte
retrieval
All patients underwent controlled ovarian
stimulation using gonadotropin-releasing hormone analog
(Diphreline; Ipsen, Paris, France) and the gonadotropins human
menopausal gonadotropins (Lizhu Group Co., Ltd., Zhuhai, China) and
Gonal-F (Merck Serono, Geneva, Switzerland). The standard or short
stimulation protocols were used according to the patient's age or
ovarian reserve function. Patients with antral follicle count (AFC)
>6 or aged <35 years old were treated with the long protocol,
and patients with AFC ≤6 or aged ≥35 years old were treated with
the short protocol. Drug dosage was adjusted according to
ultrasound monitoring results and serum estradiol levels. Human
chorionic gonadotropin (HCG; Lizhu Group Co., Ltd.) or recombinant
HCG (Merck Serono, Geneva, Switzerland) was administered when ≥2
follicles measured 18 mm in diameter. Oocyte retrieval was
performed by guided transvaginal ultrasonography 38 h later.
Sperm preparation
Semen samples were collected by masturbation after
3–5 days of abstinence. After liquefaction, semen samples were
prepared by gradient centrifugation. Finally, the sperm pellet was
suspended and used for oocyte insemination.
Insemination and fertilization
assessment
After egg retrieval, COCs were cut to similar sizes
with insulin needles and placed in 100 µl G-IVF™ (Ovoil; Vitrolife
AB, Göteborg, Sweden) droplets covered by mineral oil (Ovoil;
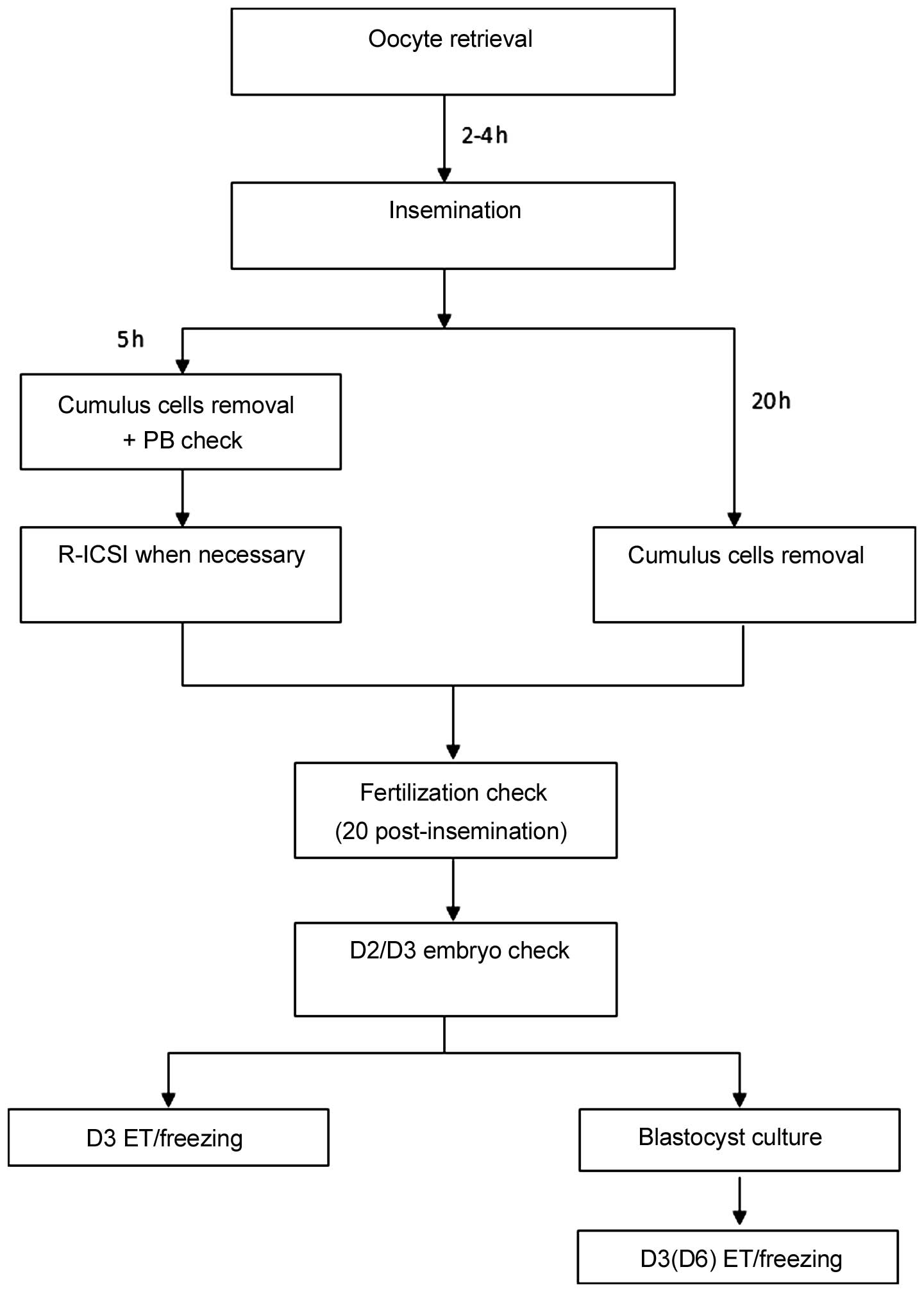
Vitrolife AB). Each oocyte was inseminated with 40,000 motile
spermatozoa 2–4 h later. Cohort eggs were divided into two, with
one half for conventional insemination and the other half for short
insemination. Cumulus cells were removed at 5 or 20 h post
insemination for the short insemination and conventional
insemination groups, respectively. Oocytes were then placed in G-1
(Ovoil; Vitrolife AB) medium at 37°C in a humidified atmosphere of
6% CO2.
An early fertilization check was conducted in the
short insemination group. Oocytes were checked for the release of
the second polar body and perivitelline space (PVS) following the
removal of cumulus cells. Early fertilization was determined to
have occurred when two distinct PBs and evident PVS were observed
in an oocyte. If none of the oocytes showed the signs of early
fertilization, R-ICSI was performed subsequently as previously
described (6). All eggs were checked
for the appearance of pronuclei at 17–20 h after insemination. The
time sequence of the study is shown in Fig. 1.
Embryonic development and embryo
transfer
Each embryo was observed daily and assessed using
the following scoring system: Grade 1, number of cells ≥4 on day 2,
or number of cells ≥6 on day 3 with even size blastomeres,
integrated zona pellucida, regular morphology, clear cytoplasm, the
absence of particles and <5% fragments; grade 2, number of cells
≥4 on day 2, or number of cells ≥6 on day 3 with slightly unevenly
size blastomeres, and 6–20% fragments; grade 3, significantly
unevenly size blastomeres, and 21–50% fragments; grade 4, abnormal
rate of embryo development, severely unequal cell size, significant
cytoplasmic particles, and a great quantity of vacuole fragments
(>50%). Grades 1 and 2 were defined as high-quality embryos, and
grades 1–3 were defined as utilizable embryos. Embryos were
selected randomly from either the conventional or short
insemination group. One or two utilizable embryos were selected for
transfer. The luteal phase was supported by estradiol valerate and
intramuscular progesterone injection.
Pregnancy and follow-up
Clinical pregnancy was defined as the detection of
the gestational sac by ultrasound at 28 days after embryo transfer.
Luteal support was continued until 10 weeks of gestation.
Statistical analysis
Statistical analysis was performed using SPSS
version 17.0 statistical analysis software (SPSS, Inc., Chicago,
IL, USA). Results are expressed as mean ± standard deviation or
percentage. The Chi-square test was used for comparisons of
percentages and Student's t-test was used for the comparison of
mean values. P<0.05 was considered to indicate a statistically
significant difference.
Results
General data
In total, there were 165 patients in this study, of
which 95 had tubal factors, 19 had male factors, 4 had
endometriosis, 4 had polycystic ovary syndrome, 21 had unexplained
infertility and 22 had complex factors. There were 85 (51.5%)
patients with primary infertility and 80 (48.5%) patients with
secondary infertility.
From 165 egg collections, 2,465 eggs were retrieved.
Cohort eggs from each egg collection were divided for the short
insemination and conventional insemination groups in a principle of
50/50%. The details of fertilization and further development
parameters are summarized in Table
I. No significant differences were observed in fertilization,
abnormal fertilization and embryo quality.
 | Table I.Comparison of parameters between the
two different types of insemination, including R-ICSI cycles. |
Table I.
Comparison of parameters between the
two different types of insemination, including R-ICSI cycles.
| Parameter | Short insemination
group (n=165) | Conventional
insemination group (n=165) | P-value |
|---|
| 2PN rate (%) | 769/1,227 (62.7) | 750/1,238 (60.6) | 0.286 |
| Polyspermy rate
(%) | 104/1,227 (8.5) | 87/1,238 (7.0) | 0.179 |
| Cleavage rate
(%) | 764/769 (99.3) | 745/750 (99.3) | 0.968 |
| Viable embryo rate
(%) | 623/769 (81.0) | 603/750 (80.4) | 0.762 |
| High quality embryo
rate (%) | 364/769 (47.3) | 321/750 (42.8) | 0.076 |
| Blastocyst formation
rate (%) | 177/363 (48.8) | 195/358 (54.5) | 0.125 |
Outcome of the two different types of
insemination
When the 11 patients who underwent R-ICSI cycles
were excluded, there were no significant differences in all
treatment parameters between the two different types of
insemination (Table II).
| Table II.Comparison of parameters between the
two different types of insemination, excluding R-ICSI cycles. |
Table II.
Comparison of parameters between the
two different types of insemination, excluding R-ICSI cycles.
| Parameter | Short insemination
group (n=154) | Conventional
insemination group (n=154) | P-value |
|---|
| 2PN rate (%) | 722/1,145 (63.1) | 724/1,158 (62.5) | 0.790 |
| Polyspermy rate
(%) | 103/1,145 (9.0) | 86/1,158 (7.4) | 0.170 |
| Cleavage rate
(%) | 719/722 (99.6) | 719/724 (99.3) | 0.481 |
| Viable embryo rate
(%) | 585/722 (81.0) | 583/724 (80.5) | 0.809 |
| High quality embryo
rate (%) | 343/722 (47.5) | 310/724 (42.8) | 0.073 |
| Blastocyst formation
rate (%) | 174/348 (50.0) | 187/344 (54.4) | 0.251 |
The embryo transfers of 69 of the 165 cycles (41.8%)
were cancelled due to elevated progesterone level, ovarian hyper
stimulation syndrome or insufficient endometrial thickness. There
were 201 embryos transferred in 96 cycles, of which 49 cycles
involved the transfer of embryos from the short insemination group
and 47 cycles were with embryos from the conventional insemination
group. No significant differences were identified between the two
groups in terms of age, number of eggs, number of embryos and good
embryo rate. Clinical pregnancy and implantation rates were not
significantly different between the patients with embryos
transferred from the short insemination and conventional
insemination groups (57.1 vs. 55.3%, and 34.7 vs. 36%,
respectively; Table III).
| Table III.Comparison of the embryo transfer
results from the two different insemination groups. |
Table III.
Comparison of the embryo transfer
results from the two different insemination groups.
| Parameter | Short insemination
group (n=49) | Conventional
insemination group (n=47) | P-value |
|---|
| Age, years | 29.6±3.9 | 29.5±3.9 | 0.865 |
| Clinical pregnancy
rate (%) | 28/49 (57.1) | 26/47
(55.3) | 0.875 |
| Implantation rate
(%) | 35/101 (34.7) | 36/100
(36.0) | 0.842 |
R-ICSI cycles
In the short insemination group, R-ICSI was
performed due to no oocyte activation being observed in 11 cycles
(6.7%), of which 6 cycles had fertilization of the patient's eggs
in the 20 h insemination group. In the other 5 cycles, the
patient's eggs were not fertilized after 20 h insemination either.
Following R-ICSI, 19 of 36 eggs were normally fertilized.
Subsequently, 7 embryos were transferred in 4 fresh cycles.
Discussion
Conventionally, oocytes have been co-cultured with
sperm overnight, for 16–20 h. This long insemination time has been
adopted as a routine practice most probably for the reason of
accommodating a fertilization check in the morning of day 1 rather
than to accommodate the demands of the biological clock. It has
been reported that a co-incubation time as short as 30 sec is long
enough to obtain fertilization in human IVF (12). The long period of co-incubation may
generate high levels of reactive oxygen species, which may damage
embryos by hardening the zona pellucida and affect embryo
development (13). Some reports
suggest that a sperm-oocyte exposure time of 1–6 h improves the
rates of fertilization, polyspermy, good-quality embryos,
implantation, clinical pregnancy and ongoing pregnancy (7,8).
However, the advantages of a short insemination time have not been
observed consistently and conflicting results have been reported
(14–16). Although a meta-analysis of short
insemination in IVF indicated that a reduced gamete exposure time
is beneficial to clinical outcome, it also pointed out that the
conclusion was compromised by design differences between studies
(17).
In order to have a good control of the heterogeneity
of patient characteristics, which may impact on the result of IVF
treatments, sibling oocytes of each patient were assigned to either
the short or the conventional insemination group in the present
study. Sibling oocytes were randomized to the short insemination
group or the conventional insemination group. This meant that the
two groups were identical regarding factors such as etiology and
the duration of the infertility, age of the women and ovarian
stimulation protocol. No advantage of a short co-incubation time
was found regarding fertilization rate, embryo cleavage rate or
quality of the embryos, which is consistent with previous studies
(14–16,18).
Conversely, there are some discrepancies between this study and
others, showing conflicting results (13,19).
This could be explained by differences in the sperm density used
for insemination, patient profiles, insemination method and the
times of removal of cumulus cells and fertilization assessment. In
comparison with the previous studies, the present study benefitted
from a standard insemination protocol. A standard 100-µl drop size
of culture media was used for insemination and 40,000 sperm for
insemination, and all COCs after egg collection were trimmed to a
similar size with insulin needles to control the variation
introduced by the amount of sperm trapped in the cumulus.
Furthermore, blastocyst culture, a less objective parameter than
cleavage evaluation, was used to assess embryo quality. This study
showed that the method of insemination did not affect the potential
for blastocyst formation. Finally, the embryo development data were
consistent with the clinical pregnancy outcomes, showing no
difference between the two insemination groups, indicating that
reducing the time of insemination does not improve embryo
development, the embryo utilization rate or the clinical outcomes
of IVF.
It has been always challenging for practitioners of
artificial reproductive technology (ART) to predict fertilization
results for IVF. The average fertilization rate after standard IVF
is 60–70%. TFF occurs in 5–10% of IVF cycles (1) and only 1–3% of ICSI cycles (20,21). In
part due to the advantage of the low TFF rate of ICSI, the use of
ICSI increased from 39.6% of ART cycles in 1997 to 58.9% in 2004
(USA 57.5%, Australia/New Zealand 58.6%, Europe 59.3%) (22). In some countries, ICSI has been
considered as the only insemination method regardless semen quality
(23). While considering the extra
cost and the potential risk of birth defects associated with ICSI,
IVF should be considered as the primary insemination method for
non-male factor infertility (24).
Alternatively, when conventional IVF is not successful,
re-insemination of unfertilized IVF oocytes by ICSI can be
considered. Since oocyte aging is so important for the outcome of
re-insemination, it has been advised that R-ICSI should be
performed as early as possible (10,19,25,26).
Chen and Kattera shortened the period of co-incubation of gametes
(6). Cumulus cells were removed 6 h
after insemination to observe the polar body status, and oocytes
with no signs of activation were submitted to R-ICSI once
fertilization failure was identified.
In the present study, the eggs from each patient
were divided into one half for conventional insemination and the
other half for short insemination combined with R-ICSI if required.
There were 11 cycles in which R-ICSI was performed due to TFF
occurring in the eggs with the short insemination time. In 5 out
the 11 R-ICSI cycles, TFF occurred concurrently in the patient's
eggs in the conventional insemination group. Four patients had
R-ICSI embryos transferred. Only one of them achieved an ectopic
pregnancy. It is worthwhile to mention that of the 11 R-ICSI
cycles, there were 6 cycles in which ICSI was performed
unnecessarily as satisfactory fertilization results were obtained
in the cohort eggs from the conventional insemination. Thus, for
the purpose of TFF detection, this early fertilization check has
100% sensitivity and 45.5% specificity. This indicates that the
occurrence of TFF was overestimated by the early fertilization
check. Although the short insemination combined with R-ICSI had
very high sensitivity for the prevention of TFF, the poor
specificity should be noted, as such rescue attempts had the
potential for tripronucleated zygote formation. Secondly,
unnecessary micro-manipulation and checking might put extra stress
on the eggs.
Attention to the short insemination method has been
increasing, particularly in China, a developing country, where the
stimulatory drugs account for up to 80% of the total IVF treatment
cost, indicating that cycle cancellation for the reason of TFF may
stop patients coming back for further IVF treatment due to the lack
of affordability (27). The short
insemination combined with R-ICSI appears to be a practical method
to ease the stress from TFF. Nevertheless, this method of
alleviating TFF has the disadvantages of potentially injecting
fertilized eggs, unnecessary ICSI being conducted, higher
polyspermy rates (28), and the
requirement for extra embryologists to cover evening or later
shifts. Considering those hidden costs, cost-effectiveness studies
are required to be conducted before concluding the role of
R-ICSI.
In conclusion, the present study demonstrates that a
short insemination time does not improve embryo development and
pregnancy rates. Short insemination combined with early R-ICSI may
be a method to prevent TFF, albeit with poor accuracy.
References
|
1
|
Mahutte NG and Arici A: Failed
fertilization: Is it predictable? Curr Opin Obstet Gynecol.
15:211–218. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Yuzpe AA, Liu Z and Fluker MR: Rescue
intracytoplasmic sperm injection (ICSI)-salvaging in vitro
fertilization (IVF) cycles after total or near-total fertilization
failure. Fertil Steril. 73:1115–1119. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lundin K, Sjögren A and Hamberger L:
Reinsemination of one-day-old oocytes by use of intracytoplasmic
sperm injection. Fertil Steril. 66:118–121. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sermondade N, Hugues JN, Cedrin-Durnerin
I, Poncelet C, Benzacken B, Lévy R and Sifer C: Should all embryos
from day 1 rescue intracytoplasmic sperm injection be transferred
during frozen-thawed cycles? Fertil Steril. 94:1157–1158. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ming L, Liu P, Qiao J, Lian Y, Zheng X,
Ren X, Huang J and Wu Y: Synchronization between embryo development
and endometrium is a contributing factor for rescue ICSI outcome.
Reprod Biomed Online. 24:527–531. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Chen C and Kattera S: Rescue ICSI of
oocytes that failed to extrude the second polar body 6 h
post-insemination in conventional IVF. Hum Reprod. 18:2118–2121.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kattera S and Chen C: Short coincubation
of gametes in in vitro fertilization improves implantation and
pregnancy rates: A prospective, randomized, controlled study.
Fertil Steril. 80:1017–1021. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Dirnfeld M, Shiloh H, Bider D, Harari E,
Koifman M, Lahav-Baratz S and Abramovici H: A prospective
randomized controlled study of the effect of short coincubation of
gametes during insemination on zona pellucida thickness. Gynecol
Endocrinol. 17:397–403. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wei D, Zhang C, Yin B, Wang P, Xie J, Song
X, Liu Q, Hu L, Zhang Y and Hao H: Early cumulus cell removal could
reduce the available embryo rate in human IVF. J Assist Reprod
Genet. 28:1213–1216. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Nagy ZP, Rienzi LF, Ubaldi FM, Greco E,
Massey JB and Kort HI: Effect of reduced oocyte aging on the
outcome of rescue intracytoplasmic sperm injection. Fertil Steril.
85:901–906. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
World Health Organization, . WHO
Laboratory Manual for the Examination and Processing of Human
Semen. 5th. Geneva: pp. 10–44. 2010
|
|
12
|
Bungum M, Bungum L and Humaidan P: A
prospective study, using sibling oocytes, examining the effect of
30 seconds versus 90 minutes gamete co-incubation in IVF. Hum
Reprod. 21:518–523. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Gianaroli L, Magli M Cristina, Ferraretti
AP, Fiorentino A, Tosti E, Panzella S and Dale B: Reducing the time
of sperm-oocyte interaction in human in-vitro fertilization
improves the implantation rate. Hum Reprod. 11:166–171. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lundqvist M, Johansson U, Lundkvist O,
Milton K, Westin C and Simberg N: Reducing the time of
co-incubation of gametes in human in-vitro fertilization has no
beneficial effects. Reprod Biomed Online. 3:21–24. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lin SP, Lee RK, Su JT, Lin MH and Hwu YM:
The effects of brief gamete co-incubation in human in vitro
fertilization. J Assist Reprod Genet. 17:344–348. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Barraud-Lange V, Sifer C, Pocaté K, Ziyyat
A, Martin-Pont B, Porcher R, Hugues JN and Wolf JP: Short gamete
co-incubation during in vitro fertilization decreases the
fertilization rate and does not improve embryo quality: A
prospective auto controlled study. J Assist Reprod Genet.
25:305–310. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zhang XD, Liu JX, Liu WW, Gao Y, Han W,
Xiong S, Wu LH and Huang GN: Time of insemination culture and
outcomes of in vitro fertilization: A systematic review and
meta-analysis. Hum Reprod Update. 19:685–695. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Coskun S, Roca GL, Elnour AM, al Mayman H,
Hollanders JM and Jaroudi KA: Effects of reducing insemination time
in human in vitro fertilization and embryo development by using
sibling oocytes. J Assist Reprod Genet. 15:605–608. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Zhang NY, Sun HX, Hu YL, Wang B and Xu ZP:
Combination of short-period sperm-oocyte coincubation and early
rescue intracytoplasmic sperm injection after total failure of in
vitro fertilization. Zhonghua Nan Ke Xue. 15:538–541. 2009.(In
Chinese). PubMed/NCBI
|
|
20
|
Cheng D, Li J, Guo CC and Xiong CL: Failed
fertilization after ICSI: Causes and countermeasures. Zhonghua Nan
Ke Xue. 17:1131–1134. 2011.(In Chinese). PubMed/NCBI
|
|
21
|
Flaherty SP, Payne D and Matthews CD:
Fertilization failures and abnormal fertilization after
intracytoplasmic sperm injection. Hum Reprod. 13:155–164. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Andersen A Nyboe, Carlsen E and Loft A:
Trends in the use of intracytoplasmatic sperm injection marked
variability between countries. Hum Reprod Update. 14:593–604. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kupka MS, Ferraretti AP, de Mouzon J, Erb
K, D'Hooghe T, Castilla JA, Calhaz-Jorge C, De Geyter C and
Goossens V: European IVF-monitoring consortium, for the European
society of human reproduction and embryology: Assisted reproductive
technology in Europe, 2010: Results generated from European
registers by ESHRE†. Hum Reprod. 29:2099–2113. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Davies MJ, Moore VM, Willson KJ, Van Essen
P, Priest K, Scott H, Haan EA and Chan A: Reproductive technologies
and the risk of birth defects. N Engl J Med. 366:1803–1813. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Liu W, Liu J, Zhang X, Han W, Xiong S and
Huang G: Short co-incubation of gametes combined with early rescue
ICSI: An optimal strategy for complete fertilization failure after
IVF. Hum Fertil (Camb). 17:50–55. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kuczyński W, Dhont M, Grygoruk C,
Pietrewicz P, Redzko S and Szamatowicz M: Rescue ICSI of
unfertilized oocytes after IVF. Hum Reprod. 17:2423–2427. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Chambers GM, Hoang VP, Sullivan EA,
Chapman MG, Ishihara O, Zegers-Hochschild F, Nygren KG and Adamson
GD: The impact of consumer affordability on access to assisted
reproductive technologies and embryo transfer practices: An
international analysis. Fertil Steril. 101:191–198.e4. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Xiong S, Han W, Liu JX, Zhang XD, Liu WW,
Liu H and Huang GN: Effects of cumulus cells removal after 6 h
co-incubation of gametes on the outcomes of human IVF. J Assist
Reprod Genet. 28:1205–1211. 2011. View Article : Google Scholar : PubMed/NCBI
|