Introduction
Acquired hemophilia A (AHA) is a relatively rare and
life-threatening bleeding disorder caused by spontaneous
development of autoantibodies against factor VIII (FVIII). The
reported annual incidence of AHA is of the order of 1.5 individuals
per million (1). The disease most
commonly presents as spontaneous excessive hemorrhage in muscles,
skin or soft tissues, or uncontrolled bleeding during surgery. To
date, the pathogenesis of AHA remains unclear. There is no apparent
underlying cause in ~50% of the reported cases; other cases are
typically associated with autoimmune disorders, malignancy, adverse
drug reactions and various skin diseases (2).
In 1993, a 78-year old male patient developed
generalized lymphadenopathy accompanied with a disproportionately
elevated serum IgG4 level. The IgG4-related disease has attracted
increasing attention ever since (3).
In addition to the elevated IgG4 levels, the disease is
characterized by lymph node involvement due to lymphoplasmacytic
infiltration with IgG4-positive plasma cells, marked interstitial
fibrosis, eosinophilic infiltration and obliterative phlebitis of
the terminal venules (4).
IgG4-related disease is a fibroinflammatory systemic
disease which affects multiple organs, including the biliary
system, salivary glands, lymph nodes, pancreas, retroperitoneum,
periorbital tissue, lungs, meninges, aorta, breast, prostate,
thyroid gland, pericardium, skin and kidney (3,5–12). Owing to multisystemic involvement,
clinical manifestation of IgG4-related disease varies widely, and
depends on the severity of the affected organs. An extensive
literature search revealed only two documented cases of AHA with
co-existing IgG4 related disease (13,14).
Herein, a rare case of IgG4 -related AHA with multisystemic
involvement is described that presented with a myriad of clinical
characteristics. The clinical relevance of AHA has been discussed
to provide a better understanding of this rare disorder.
Case report
A 55-year-old Chinese male, who provided written
informed consent, presented at Shanxi DAYI Hospital of Shanxi
Medical University (Shanxi, China) in November 2014 with a history
of chronic cough since half a year ago with no obvious cause. The
cough tended to aggravate at night. In the previous 1 month there
was progressive aggravation of cough, which could be induced by
cooking fumes or pungent odor. Six days prior to admission, the
patient caught a cold with further aggravation of cough, but
without fever, hemoptysis, chest pain, palpitations and sweating.
The patient did not respond to antibiotic therapy prescribed at a
local health clinic. On examination, the patient was not febrile
(36.5°C), and his vitals were stable with a systolic blood pressure
of systolic 141 mmHg and diastolic 94 mmHg. There were no signs of
inflammation of pharyngeal mucosa or tonsillar enlargement. His
systemic examination was unremarkable except for the presence of a
small palpable submandibular lymph node and an enlarged left
inguinal lymph node measuring 3×1 cm. His abdomen was soft,
non-tender with non-palpable liver and spleen. The result of
bronchial provocation test was positive and the patient was
diagnosed as having bronchial asthma.
The patient had a significant past medical history,
including hospitalization for autoimmune hepatitis with serum
alanine aminotransferase (ALT) 421 IU/ml and aspartate
aminotransferase (AST) 600 IU/ml. Anti-smooth muscle antibody was
positive (titre, 1:100). Abdominal computed tomography (CT) showed
multiple enlarged lymph nodes in the ligament of liver and stomach,
around the abdominal aorta and bilateral inguinal regions, with the
left inguinal region being more affected. The upper pancreatic bile
duct was widened, indicating a possibility of cholecystitis or
cholangitis. Furthermore, there was thickening and consolidation in
the wall of left ureter, indicating a possibility of a space
occupying lesion (SOL) of the ureter, accompanied with an
inflammatory response in the renal pelvis and the upper ureter.
Magnetic resonance cholangiopancreatography revealed
multiple gallbladder and bile duct calculi, intra- and extrahepatic
bile duct dilation, and abnormal signals in caput pancreatis
accompanied with multiple enlarged small lymph nodes around the
abdominal artery. Based on these findings, the patient was
diagnosed with gallbladder and cystic duct calculi, acute
cholecystitis and acute pancreatitis. The symptoms of the patient
improved with anti-inflammatory drugs and supportive treatment,
with restoration of normal serum ALT (25.2 IU/ml) and AST (19.4
IU/ml) levels.
To rule out the possibility of SOL in the left
ureter, the patient underwent cystoscopic examination with double J
tube placement. However, there was no evidence of SOL. The patient
also had urticaria, diabetes and low triiodothyronine (T3)
levels.
Positron emission tomography (PET)/CT performed
three months prior to admission showed abnormal hypermetabolic
signals in multiple organ systems (including bone marrow, multiple
lymph nodes, parotid gland, lung, gallbladder, bile duct, pancreas,
prostate and testis), left hydronephrosis and dilatation of the
upper left ureter. Assays for serum lupus anticoagulant
combination, antinuclear antibody, antineutrophil cytoplasmic
antibodies, immunoglobulin and complement levels were all negative.
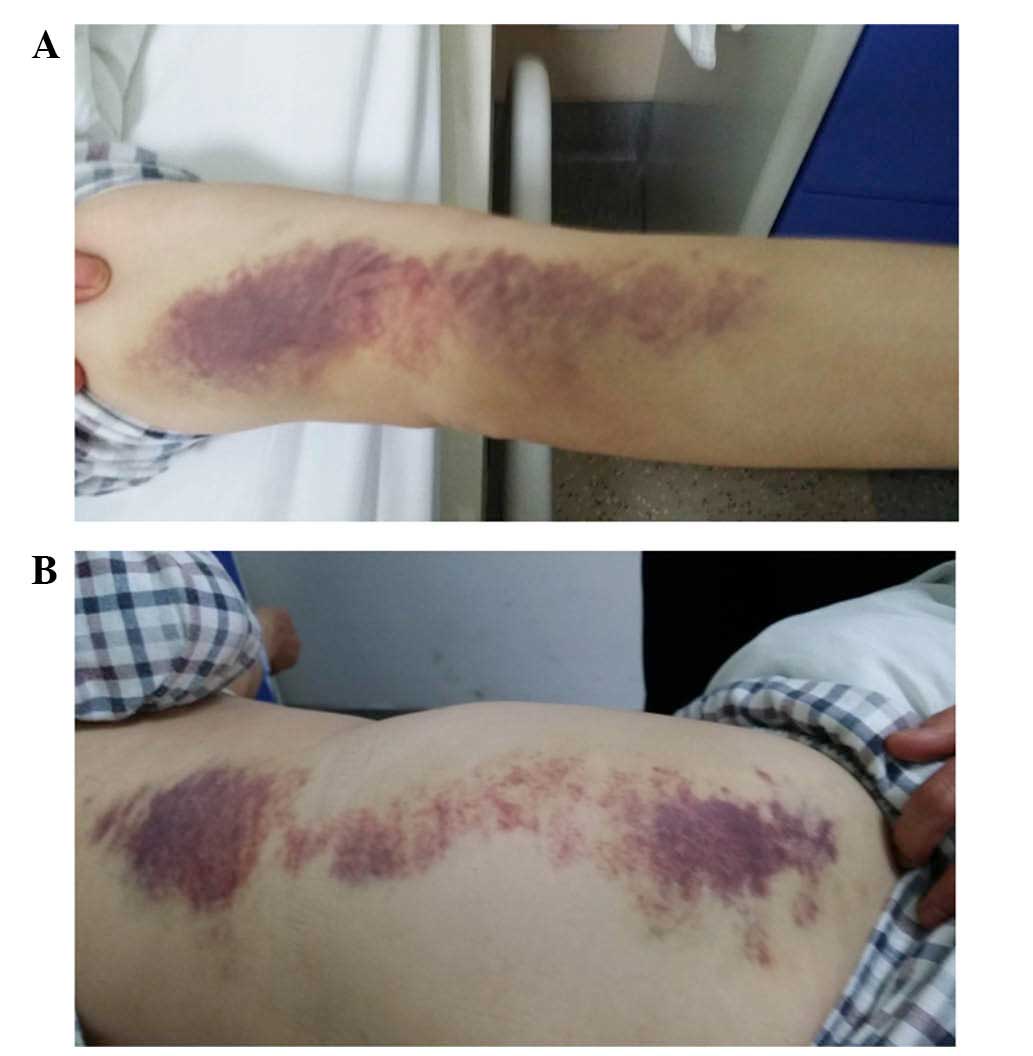
Three days after admission, the patient developed subcutaneous
hemorrhages and pain in the right hip (Fig. 1). Ultrasound examination revealed a
subdermal hematoma over the right hip measuring 9×3x5 cm. On
detailed enquiry, the patient revealed a past history of
spontaneous bleeding in bilateral upper extremities 2 months prior
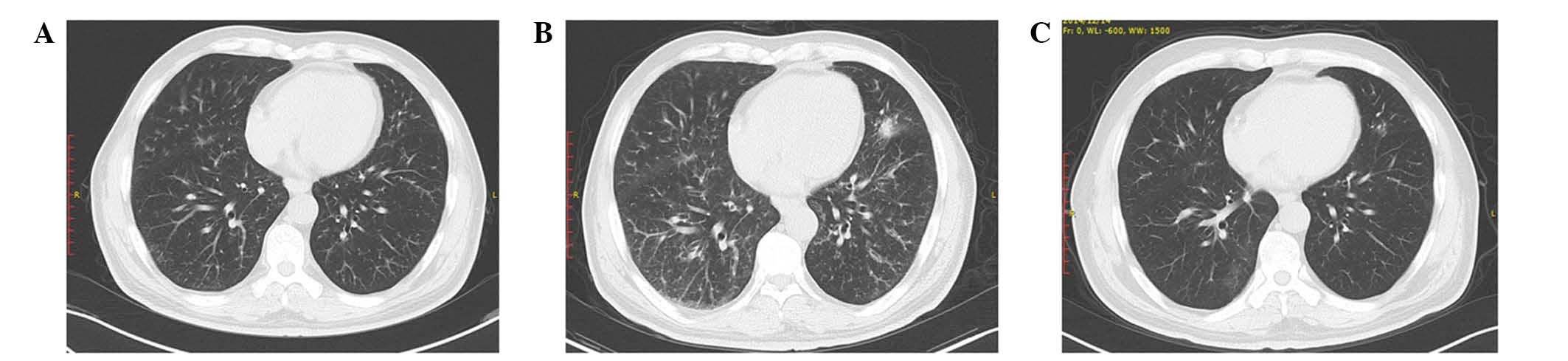
to admission. Chest CT showed multiple diffuse nodular lesions with
thickening of bronchovascular bundles, and multiple scattered high
density spots in both lung lobes. In addition, there was multiple
lymph node enlargement in the mediastinum and pulmonary hila
(Fig. 2).
Laboratory investigations at admission showed
activated partial prothrombin time (APTT) of 120.0 sec (normal
range, 24.0–40.0 sec), but with normal prothrombin time, thrombin
time and fibrinogen levels. The platelet count was also normal.
Coagulation factor assay revealed a markedly decreased factor VIII
(FVIII) activity at 0.5% (normal range, 60–150%), and a high-titer
of FVIII inhibitor at 27.2 Bethesda units/ml (BU/ml) (normal range,
0–0.6 BU/ml). In addition, serum IgG4 level was markedly increased
(>4.03 g/l).
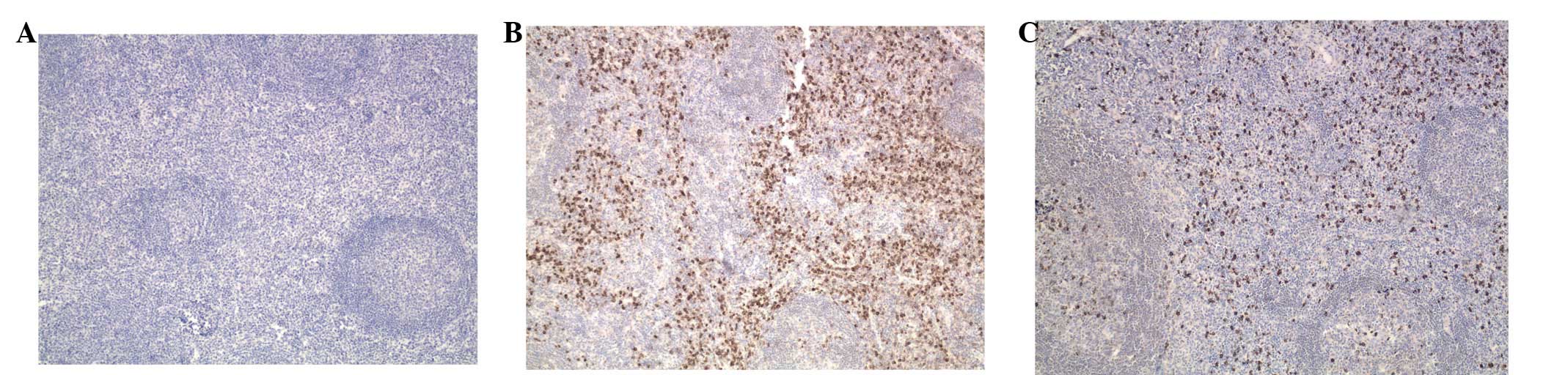
Left inguinal lymph node biopsy revealed capsular
thickening, marked lymphoplasmacytic infiltration with irregular
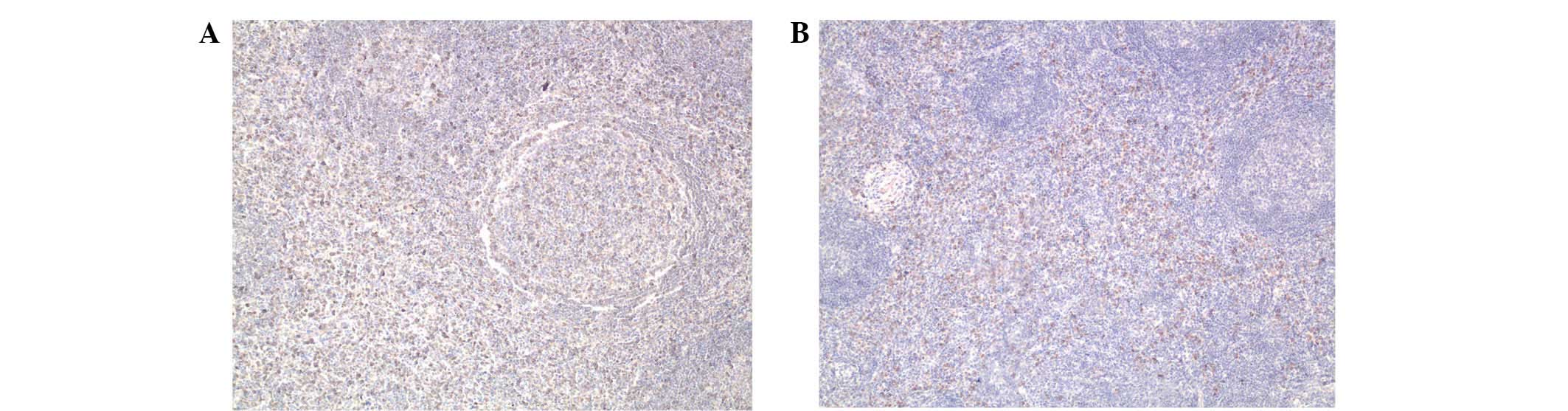
fibrosis and obliterative phlebitis (Fig. 3). Further positive immunostaining for
human herpes virus type 8, Lambda and Kappa light chains showed
reactive lymphoid hyperplasia in the nodular lesion (Fig. 4). In addition, immunohistochemical
staining for IgG4 revealed numerous IgG4-positive plasma cells
[>100 cells/human plasma fibronectin (HPF)] in the nodular
lesion, with an increased IgG4/IgG ratio of >40% (Fig. 5). A diagnosis of IgG4-related AHA was
rendered.
IgG4-related disease is responsive to corticosteroid
therapy. The patient was treated with oral prednisone (initial
dose, 40 mg/day; maintenance dose, 15 mg/day; cat. no. H33021207;
Zhejiang Xianju Pharmaceutical Co., Ltd., Taizhou, China). After
one week of treatment, the patient's symptoms were relieved. After
2 weeks of treatment, the activated partial thromboplastin time was
within the normal range. Furthermore, one month after treatment,
chest CT scan showed clearing of the nodular lesions and lymph
nodes. There was no instance of relapse during follow-up (Table I) after one and three months.
 | Table I.Key laboratory parameters on follow up
in IgG4-related acquired hemophilia. |
Table I.
Key laboratory parameters on follow up
in IgG4-related acquired hemophilia.
| Follow-up | CRP (mg/l) | ESR (mm/h) | IgG (g/l) | IgG4 (g/l) | APTT (sec) | FVIII (%) | FVIII inhibitor
(BU/ml) |
|---|
| Normal range | 0–8 | 0–20 | 7.51–15.6 | 0.03–2.01 | 25.1–36.5 | 50–150 | 0–0.6 |
| Nov 2014 | <2.5 | 66 | 21.40 | >4.030 | 120.0 | 0.5 | 27.2 |
| Dec 2014 | <2.5 | 8 | 14.80 | >4.030 | 31.7 | 50.0 | 8.0 |
| Mar 2015 | <2.5 | 6 | 12.0 | >4.040 | 30.0 | 70.8 | <0.6 |
Discussion
Since the first reported case of IgG4-related
disease in 1993 (3), there have been
numerous reports of complicated diseases overlapping this clinical
entity (14,15). Although the understanding of
IgG4-related disease has rapidly increased, its etiology remains
elusive. According to the clinicopathological characteristics of
IgG4-related disease, its proposed comprehensive diagnostic
criteria consists of the following (14,16): i)
Diffuse or localized swelling or masses in single or multiple
organs on clinical examination; ii) elevated serum IgG4 level (≥135
mg/dl); and iii) marked lymphocyte and plasmacyte infiltration,
fibrosis and infiltration of IgG4-positive plasma cells with a
ratio of IgG4/IgG positive cells >40%, and >10 IgG4-positive
plasma cells/HPF on histopathological examination.
AHA is a rare but life-threatening hemorrhagic
disorder caused by the presence of spontaneous antibodies against
FVIII (17). Although IgG4-related
disease can potentially affect any organ besides co-existence with
other complicated diseases; it is extremely rare for this condition
to overlap AHA disease. Only two documented cases of AHA
overlapping with IgG4 related disease have been identified in the
literature (13,14). In the present case, the patient was
hospitalized because of developing bronchial asthma. Subsequently,
multiple subcutaneous hemorrhages occurred. The patient was
diagnosed with AHA based on the laboratory findings that included
markedly increased APTT, markedly decreased factor VIII (FVIII)
activity, and a high-titer of FVIII inhibitor. Notably, the
clinicopathological characteristics of the patient fulfilled all
the diagnostic criteria of IgG4-related disease described above. A
review of the patient's past history revealed multiple organ
diseases, including gallbladder and cystic duct calculi, acute
cholecystitis, acute pancreatitis, urticaria, diabetes and low T3
syndrome. Considering that IgG-4-related disease could affect any
organ and can present with myriad manifestations, it is suggested
that the multiple organ disease identified in this patient was
caused by IgG4-related AHA. The specific treatment of IgG4-related
AHA resulted in the following response: i) The manifestations of
IgG4-related AHA, such as cough, nausea, abdominal pain and
subcutaneous hemorrhage, were completely resolved; ii) blood
glucose level and thyroid function were restored to normal range
and remained stable, unlike that in IgG4-related disease only,
which frequently involves the pancreas and thyroid gland, causing
diabetes and low T3 syndrome; iii) the specific serological markers
of IgG4-related AHA, such as IgG, APTT, FVIII and FVIII inhibitor
were within normal range; iv) the abnormal hypermetabolic signals
in multiple organ systems identified by PET/CT were alleviated.
IgG4-related disease is a glucocorticoid-responsive
disorder (18), and this was well
manifested in the present case. The initial findings of multiple
diffuse nodular lesions with thickening of bronchovascular bundles
and scattered high-density spots were markedly diminished in both
lung lobes, and there was a decrease in the lymph nodes. The
patient's symptoms further improved and there was no relapse on
follow-up. The efficacy of glucocorticoid treatment in multiple
organ diseases in this patient was consistent with the diagnosis of
IgG4-related AHA.
However, the serum IgG4 level remained high even
after glucocorticoid treatment, which was not consistent with most
of the other documented cases. Although IgG4-related disease
typically demonstrates high serum IgG4 levels, approximately 20% of
patients with biopsy-proven IgG4-related disease may have normal
serum IgG4 level (15,19,20). A
review of the literature revealed a case report wherein a patient
was diagnosed with IgG4-related sclerosing disease, despite serum
IgG4 levels remaining normal. The patient responded to
corticosteroid treatment (prednisolone) with alleviation of
pulmonary lesions and improved renal function; however, the serum
IgG4 level increased (6). A
plausible explanation for the seronegativity of the patient may be
that active synthesis blocked IgG4 secretion, and then
corticosteroid treatment suppressed the synthesis, which restored
IgG4 secretion from the plasma cells. Thus, IgG4-related disease
may have various pathological features, and is likely to be
associated with a variable response to treatment. The current
patient is currently being followed-up with monitoring of
serological markers, including IgG4.
In conclusion, the present study describes the first
reported case of IgG4-related AHA in a 55-year-old male who
presented with unusual clinical features and systemic
manifestations. Awareness of such an entity is necessary as it is a
curable disease, and timely treatment could be life-saving.
Corticosteroids remain the mainstay of the treatment. Documentation
of such rare cases will help in further characterizing the
pathogenesis of this rare disorder.
Acknowledgements
The authors thank Medjaden Bioscience Limited for
scientific editing of the manuscript.
References
|
1
|
Collins P, Macartney N, Davies R, Lees S,
Giddings J and Majer R: A population based, unselected, consecutive
cohort of patients with acquired haemophilia A. Br J Haematol.
124:86–90. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Aljasser MI, Sladden C, Crawford RI and Au
S: Bullous pemphigoid associated with acquired hemophilia a: A rare
association of autoimmune disease. J Cutan Med Surg. 18:123–126.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Suzuki S, Kida S, Ohira Y, Ohba T, Miyata
M, Nishimaki T, Morito T, Kasukawa R, Hojyo H and Wakasa H: A case
of Sjögren's syndrome accompanied by lymphadenopathy and IgG4
hypergammaglobulinemia. Ryumachi. 33:249–254. 1993.PubMed/NCBI
|
|
4
|
Zen Y, Inoue D, Kitao A, Onodera M, Abo H,
Miyayama S, Gabata T, Matsui O and Nakanuma Y: IgG4-related lung
and pleural disease: A clinicopathologic study of 21 cases. Am J
Surg Pathol. 33:1886–1893. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ryu JH, Sekiguchi H and Yi ES: Pulmonary
manifestations of immunoglobulin G4-related sclerosing disease. Eur
Respir J. 39:180–186. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Khosroshahi A and Stone JH: A clinical
overview of IgG4-related systemic disease. Curr Opin Rheumatol.
23:57–66. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Raissian Y, Nasr SH, Larsen CP, Colvin RB,
Smyrk TC, Takahashi N, Bhalodia A, Sohani AR, Zhang L, Chari S, et
al: Diagnosis of IgG4-related tubulointerstitial nephritis. J Am
Soc Nephrol. 22:1343–1352. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Khosroshahi A, Deshpande V and Stone JH:
The clinical and pathological features of IgG (4)-related disease.
Curr Rheumatol Rep. 13:473–481. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Zen Y and Nakanuma Y: IgG4-related
disease: A cross-sectional study of 114 cases. Am J Surg Pathol.
34:1812–1819. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kamisawa T and Okamoto A: Autoimmune
pancreatitis: Proposal of IgG4-related sclerosing disease. J
Gastroenterol. 41:613–625. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hamano H, Kawa S, Ochi Y, Unno H, Shiba N,
Wajiki M, Nakazawa K, Shimojo H and Kiyosawa K: Hydronephrosis
associated with retroperitoneal fibrosis and sclerosing
pancreatitis. Lancet. 359:1403–1404. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Takeda S, Haratake J, Kasai T, Takaeda C
and Takazakura E: IgG4-associated idiopathic tubulointerstitial
nephritis complicating autoimmune pancreatitis. Nephrol Dial
Transplant. 19:474–476. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Nagao Y, Yamanaka H and Harada H: A
patient with hypereosinophilic syndrome that manifested with
acquired hemophilia and elevated IgG4: A case report. J Med Case
Rep. 6:632012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sugino K, Gocho K, Ishida F, Kikuchi N,
Hirota N, Sato K, Sano G, Isobe K, Sakamoto S, Takai Y, et al:
Acquired hemophilia A associated with IgG4-related lung disease in
a patient with autoimmune pancreatitis. Intern Med. 51:3151–3154.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sekiguchi H, Horie R, Aksamit TR, Yi ES
and Ryu JH: Immunoglobulin G4-related disease mimicking asthma. Can
Respir J. 20:87–89. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Umehara H, Okazaki K, Masaki Y, Kawano M,
Yamamoto M, Saeki T, Matsui S, Yoshino T, Nakamura S, Kawa S, et
al: Comprehensive diagnostic criteria for IgG4-related disease
(IgG4-RD), 2011. Mod Rheumatol. 22:21–30. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kessler CM: Acquired factor VIII
autoantibody inhibitors: Current concepts and potential therapeutic
strategies for the future. Haematologica. 85:(10 Suppl). S57–S61;
discussion 61–63. 2000.
|
|
18
|
Umehara H, Okazaki K, Masaki Y, Kawano M,
Yamamoto M, Saeki T, Matsui S, Sumida T, Mimori T, Tanaka Y, et al:
A novel clinical entity, IgG4-related disease (IgG4RD): General
concept and details. Mod Rheumatol. 22:1–14. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kamisawa T, Takuma K, Tabata T, Inaba Y,
Egawa N, Tsuruta K, Hishima T, Sasaki T and Itoi T: Serum
IgG4-negative autoimmune pancreatitis. J Gastroenterol. 46:108–116.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ebbo M, Daniel L, Pavic M, Sève P, Hamidou
M, Andres E, Burtey S, Chiche L, Serratrice J, Longy-Boursier M, et
al: IgG4-related systemic disease: Features and treatment response
in a French cohort: Results of a multicenter registry. Medicine
(Baltimore). 91:49–56. 2012. View Article : Google Scholar : PubMed/NCBI
|