Introduction
Hair is considered to be a primary component of an
individual's general appearance. Androgenetic alopecia (AGA), or
male-pattern hair loss, is the most common form of alopecia in men,
affecting ~50% of the male population (1). AGA is an androgen-related condition in
genetically predisposed individuals (2). AGA results in the progressive
conversion of scalp terminal hair into vellus hair over the frontal
and vertex scalp in genetically susceptible men (3). Men typically present with hairline
recession at the temples and vertex balding while women normally
diffusely thin over the top of their scalps (4).
AGA is caused by androgen-dependent miniaturization
of scalp hair follicles, with scalp dihydrotestosterone (DHT)
implicated as a contributing cause (5). The condition does not occur in men with
a genetic deficiency of the enzyme steroid 5α-reductase (5αR) type
II, which converts testosterone to DHT, implicating DHT in its
pathogenesis. Of two 5αR isoenzymes in humans, type I predominates
in the skin, including the scalp, whereas type II is present in
hair follicles as well as the prostate (5). Finasteride, an inhibitor of type II
5αR, decreases serum and scalp DHT by inhibiting the conversion of
testosterone to DHT (5); ~3% of
patients experience sexual dysfunction. These include decreased
libido, diminished sexual function (impotence), decreased
ejaculation volume and ejaculation disorder (6). These side effects subside with
continued treatment or treatment discontinuation. Thus, the
application of herbal drugs in improving alopecia is a research
topic worth exploring.
Hair loss has become a growing problem and people
look for alternatives to treat hair loss. In recent years,
pharmacological studies have found various herbal ingredients that
are anti-androgenic, inhibit 5αR, promote growth factor expression
in hair follicles, regulate the endocrine system and enhance
microcirculation (7,8). The dietary supplement L-carnitine
induces hair growth in vitro (9), but it is not approved by the Food and
Drug Administration. An extract of Grateloupia elliptica has
the potential to treat alopecia via the proliferation of dermal
papilla, 5αR inhibition, increase of prostaglandin E2 production,
decrease of lipopolysaccharide-stimulated pro-inflammatory
cytokines and inhibitory activity against Pityrosporum ovale
(10). However, few clinical trials
have investigated the effects of promoting hair growth in humans
with herbal medicines.
BeauTop contains six herbal ingredients, including
Ginseng Radix, Astragali Radix, Angelicae Sinensis
Radix, Ligustri Fructus, Rehmannia glutinosa and
Eclipta prostrata Linn. BeauTop has been proven to enhance
hair follicle activities, and has been confirmed in a previous
animal study to be non-toxic (tested by Taipei Medical University,
Taipei, Taiwan), effective in enhancing growth factors that
regulate hair follicle life cycles, and promoting hair follicle
activity (11). These animal studies
demonstrated that BeauTop's mechanism of action in improving
androgenetic alopecia is possibly associated with the growth
factors responsible for promoting or diminishing hair follicle
activity or apoptosis. These include vascular endothelial growth
factor (VEGF), epidermal growth factor (EGF), and fibroblast growth
factors (FGF-5 and FGF-7). However, no clinical trial on the
effects of inhibiting human alopecia or promoting hair growth has
been reported. Therefore, the aim of the present study was to
evaluate the treatment effects of BeauTop in alopecia by observing
its effectiveness in improving androgenetic alopecia.
Materials and methods
Trial product
BeauTop contains selected ingestible herbal
ingredients announced by the Department of Health, Taiwan. These
include Ginseng Radix, Astragali Radix, Angelicae
Sinensis Radix, Ligustri Fructus, Rehmannia
glutinosa and Eclipta prostrata Linn. It was developed
by Brion Research Institute of Taiwan and was produced by Sun Ten
Pharmaceutical (Taipei, Taiwan) according to Good Medical Practice
guidelines. An initial clinical observation reported effects in
strengthening hair roots, preventing alopecia and promoting hair
growth (11). The present study
evaluated the effects of BeauTop in treating androgenetic alopecia.
The drug ingredient for the control group was corn starch. The
drugs for the control and experimental groups were identical in
color and taste.
Experimental design
This was a pilot study. Dermatologists evaluated and
selected suitable participants for this study using the Norwood
scale or Ludwig scale. For participants that were determined to
have androgenetic alopecia by the dermatologists, photos were taken
and recorded using a hair imaging analyzer (DELTA 20T;
Dermatoscope, Hiene, Germany). The conditions of hair growth and
hairs in specific areas were observed using a partial magnifying
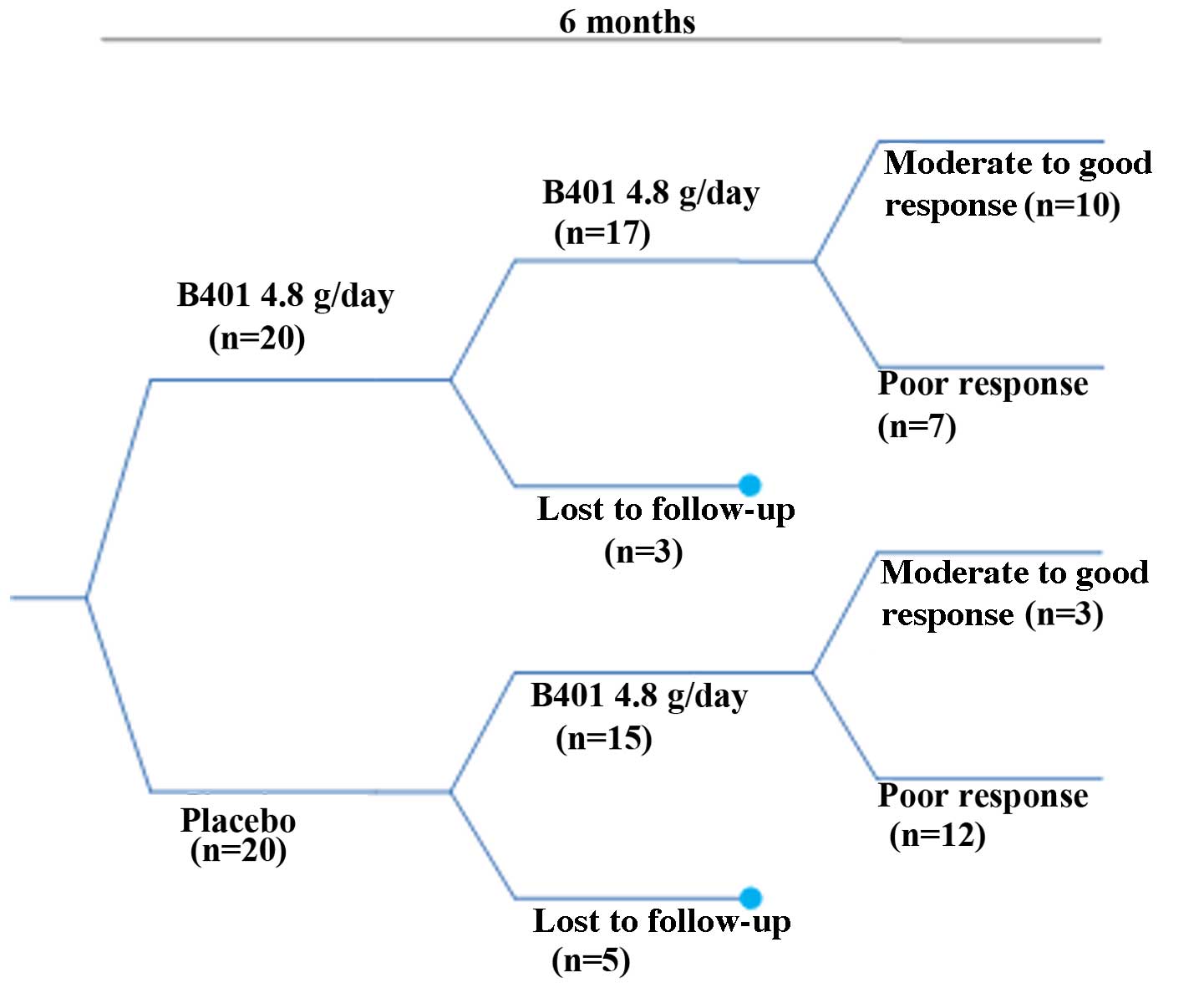
glass. In total, as shown Fig. 1, 40
participants with androgenetic alopecia were selected. Participants
were allocated to a treatment group and a placebo group through a
double-blind and randomized assignment. Overall, 20 participants
were in the active treatment group and received the herbal drug
BeauTop. Four tablets of BeauTop were administered daily before
breakfast and lunch (8 tablets, 4.8 g of Beautop daily) for 6
months. In addition, 20 participants were in the control group.
Four placebo tablets were administered daily before breakfast and
lunch for 6 months. Monthly visits were scheduled for photos and
hair improvement recordings. For each participant, photos were
taken 7 times (at the start of treatment and at months 1, 2, 3, 4,
5 and 6). The study was approved by the Chung Shan Medical
University Hospital (Taichuang, Taiwan) Institutional Review
Board.
Inclusion criteria
The evaluation was performed by dermatologists from
Chung Shan Medical University Hospital. Male androgenetic alopecia
was characterized by the recession of the frontal hairline and a
distinctive ‘M shape’ hair pattern, which progresses to the crown.
The Norwood-Hamilton scale outlines the different stages of male
pattern hair loss. The Norwood-Hamilton scale was used to determine
the extent of hair loss in men. Female androgenetic alopecia is
characterized by diffuse thinning of hair on the crown and frontal
areas. Hair density becomes reduced but does not lead to complete
baldness, and the appearance of the hairline remains normal. There
are several scales to determine the stages in women's hair loss,
and the Ludwig Scale is a commonly used method for creating a
uniform analysis of hair loss in women. The Ludwig scale was used
to determine the extent of hair loss in females in the present
study.
Exclusion criteria
Participants were excluded if they had endocrine or
metabolic disorders, tumors requiring treatment, alopecia of an
unknown cause, a swollen, infected, irritated or painful scalp,
other diseases that rendered them unable to receive the treatment,
Stage V or higher in males with alopecia, Stage II or higher in
females with alopecia, or if they were determined by physicians to
be unsuitable for receiving the treatment.
Withdrawal criteria
Patients withdrew from treatment if they experienced
side effects, including hypertrichosis, hypertension or dry mouth
In the case of a severe adverse reaction, the drug was discontinued
following evaluation by the dermatologist and the conventional
treatment method was implemented.
Index (treatment effect) evaluation
methods
Primary (treatment effect) index: The
Norwood-Hamilton scale was used to assess the improvement of
alopecia in males, and the Ludwig scale was used to assess the
improvement of alopecia in females. Secondary (treatment effect)
index: Improvement in the number of hairs shed (using participant's
self-report of daily number of hairs shed, which is the sum of the
number of hairs collected after shampooing and on the pillow) and
the observation of possible darkening of white hair roots. Changes
were recorded as significantly worse, moderately worse, minimally
worse, no change, minimally improved, moderately improved and
significantly improved, according to a previous study (12).
Laboratory examination
An initial thyroid stimulating hormone
[triiodothyronine (T3), thyroxine (T4) and thyroid-stimulating
hormone (TSH)] assessment was performed to screen out participants
with abnormal thyroid function. Participants were required to visit
the hospital once monthly for evaluation and observation. During
visits in weeks 0, 4, 8, 12, 16, 20 and 24, routine physical
examinations were performed (measurements for blood pressure,
height and weight). Liver function [aspartate transaminase (AST),
alanine aminotransferase (ALT) and gamma-glutamyl transpeptidase
(r-GT)] and renal function [creatinine and blood urea nitrogen
(BUN)] were assessed to ensure drug safety. During the 6-month
trial period, participants underwent four blood draws of 20 cc each
(including 5 cc for a stock serum study). General examination at
months 0, 1, 2, 3, 4, 5 and 6 included measurements for thyroid
stimulating hormone, liver and renal function examination, and
measurements of serum iron, serum ferritin, complete blood count,
red blood cells, hemoglobin (Hb) and hematocrit.
Statistical analysis
The Kolmogorov-Smirnov test was performed to
determine whether the continuous data were normally distributed.
Results are presented as the mean ± standard deviation for normally
distributed data, and as the median (interquartile range) for
non-normally distributed data. To examine the differences of the
continuous variable distributions between the treatment group and
the control group (including age, weight, blood pressure and
biochemical indexes), the Student's t-test was performed for
normally distributed data, and the Wilcoxon rank-sum test was
performed for non-normally distributed data. All data were analyzed
with SAS 9.2 software (SAS Institute, Cary, NC, USA).
Results
Patient characteristics
A total of 40 participants were selected for this
study. The basic information and pretreatment blood biochemical
values are shown in Table I. In
total, 32 participants completed the trial. Eight participants
withdrew from the study, including 5 males (4 in the placebo group
and 1 in the treatment group) and 3 females (2 in the treatment
group and 1 in the placebo group). Telephone interviews were
conducted for the eight participants to establish the causes of
withdrawal. All withdrawn participants indicated that no
abnormality was shown after receiving BeauTop; 4 participants
withdrew due to insufficient treatment effect (no perceived
increase in hair growth), and 4 participants could not attend the
hospital visits because of busy schedules or a change of work
location. Among these, 2 participants who were in the treatment
group indicated that they experienced increased hair growth.
 | Table I.Baseline demographic characteristics
(week 0). |
Table I.
Baseline demographic characteristics
(week 0).
|
| Treatment
(n=20) | Placebo (n=20) | P-value |
|---|
| Age, years | 39.85±8.77 | 35.30±7.19 | 0.081 |
| Male, n (%) | 16 (80.0%) | 15 (75.0%) | 1.000 |
| ALT | 29.15±22.91 | 23.05±11.28 | 0.295 |
| AST | 22.60±9.75 | 20.95±5.05 | 0.508 |
| r-GT | 43.00±52.55 | 24.53±21.79 | 0.160 |
| BUN | 12.55 (4.78) | 13.40 (3.96) | 0.597 |
| Creatinine | 0.75±0.14 | 0.77±0.15 | 0.700 |
| Iron | 84.60±32.01 | 100.37±39.60 | 0.179 |
| Ferritin | 156.51±91.83 | 207.97±141.74 | 0.184 |
| T3 | 109.07 (22.73) | 102.49 (18.51) | 0.115 |
| T4 | 6.68 (1.25) | 6.84 (1.66) | 0.813 |
| TSH | 1.15±0.53 | 0.41±1.19 | 0.380 |
| WBC | 6.77 (2.09) | 6.27 (2.14) | 0.199 |
| RBC | 5.00 (0.44) | 4.94 (0.53) | 0.338 |
| Hb | 15.20 (1.30) | 14.60 (1.80) | 0.204 |
| Hct | 44.00 (2.70) | 42.90 (4.40) | 0.444 |
| DHEA | 218.05
(190.70) | 176.50
(117.70) | 0.727 |
| Testosterone | 3.22±2.38 | 3.11±1.63 | 0.877 |
| Estradiol | 50.32±40.78 | 44.96±23.30 | 0.616 |
Hair growth results
The treatment effect is most marked in Stages III
and IV of alopecia. Of the 32 participants who completed the trial,
26 were male and 6 were female. The participants were allocated
into treatment and placebo groups through double-blind and
randomized allocation. In total, 17 participants were in the
treatment group and 15 participants were in the placebo group. The
results were encoded, de-identified and analyzed by a third party.
Hair growth was observed using a dermatoscope and clinical photos
and was scored by three dermatologists. The results revealed that
for the treatment group receiving BeauTop, 9 of the 17 participants
(52.9%) showed increased hair growth. In the placebo group, 2 of
the 15 participants (13%) showed increased hair growth. A
chi-square test was performed, which indicated that a significant
difference existed between the treatment group and the placebo
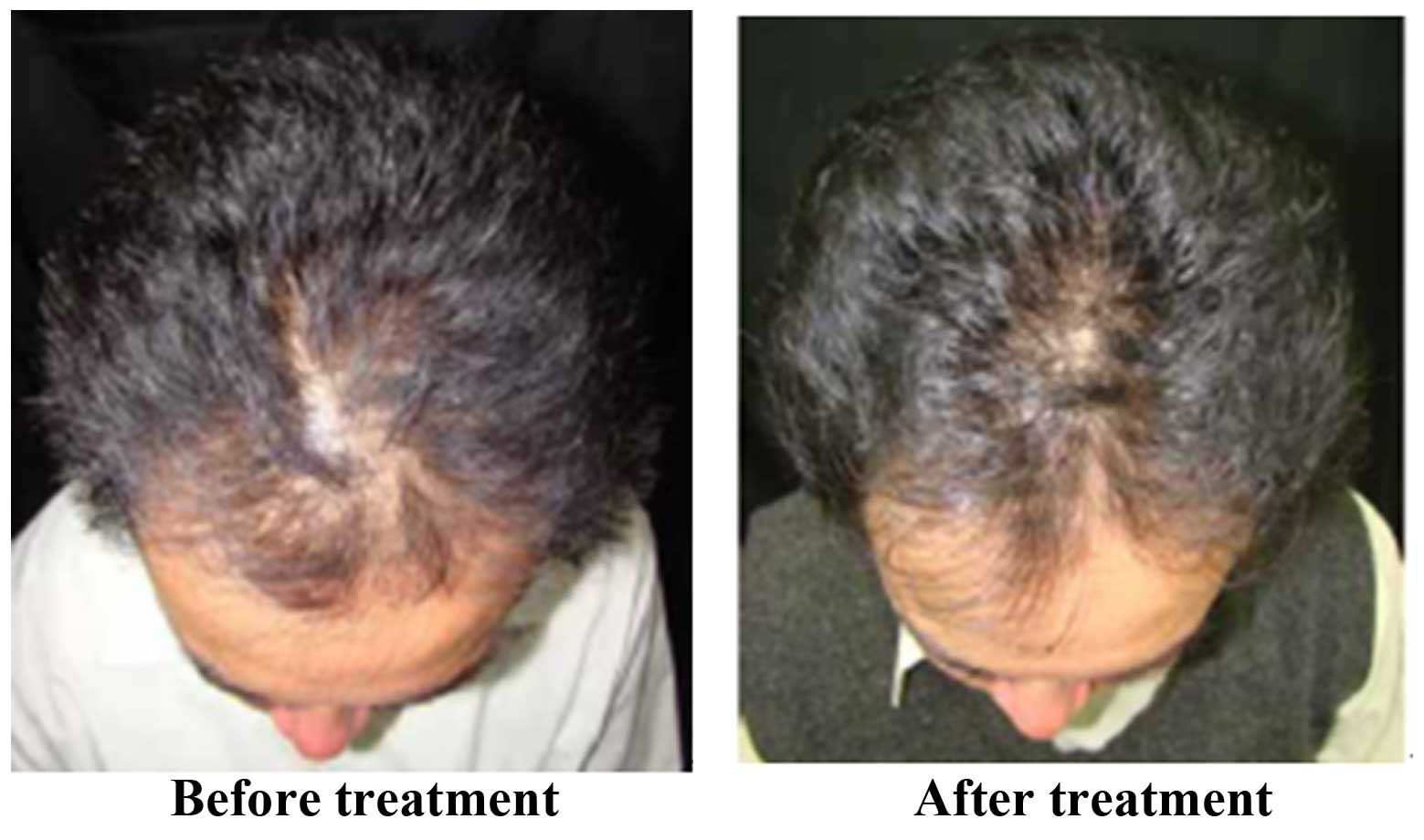
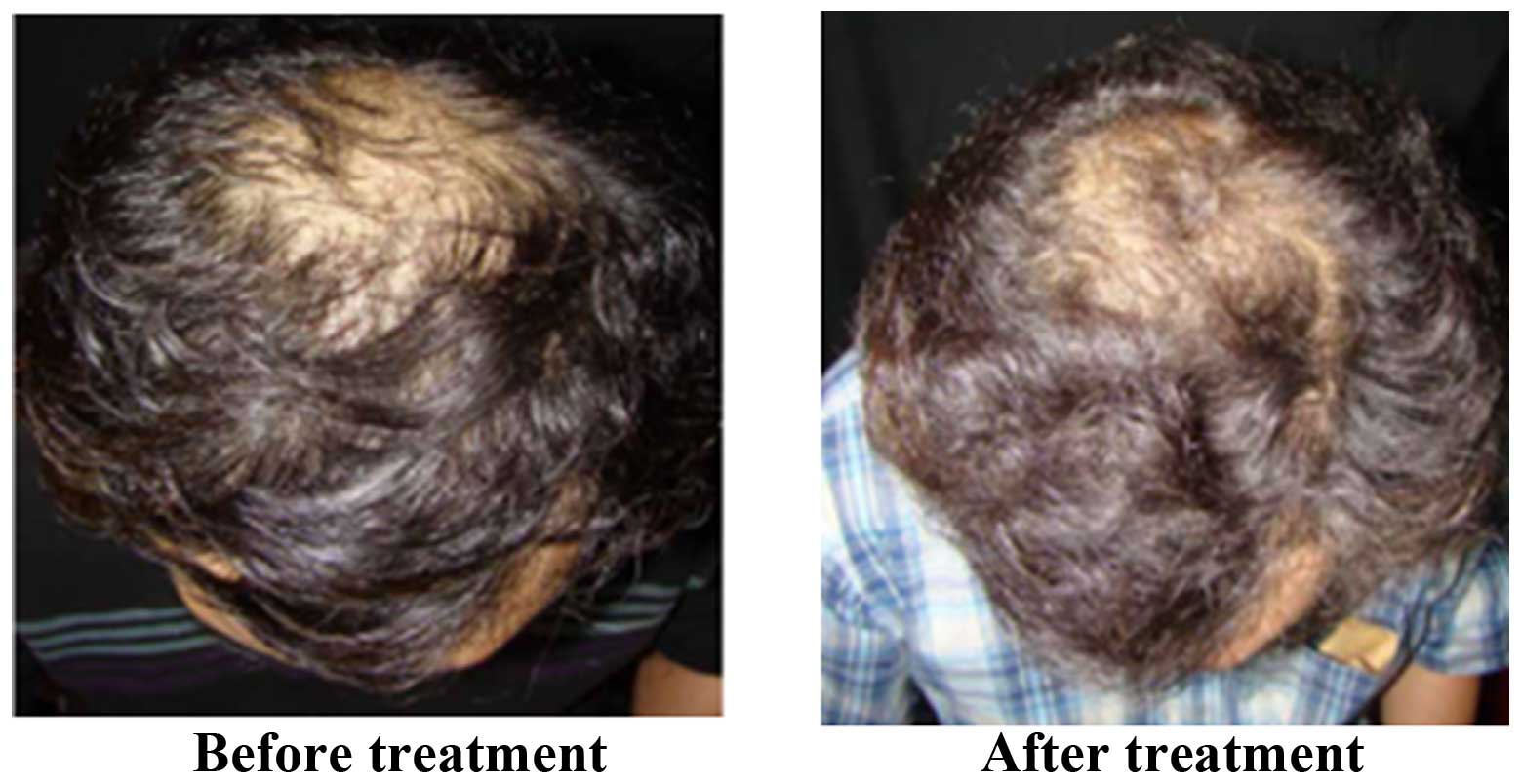
group, reaching 0.01<P<0.025 (Table II). Fig.
2 shows images of patients with significant improvement in hair
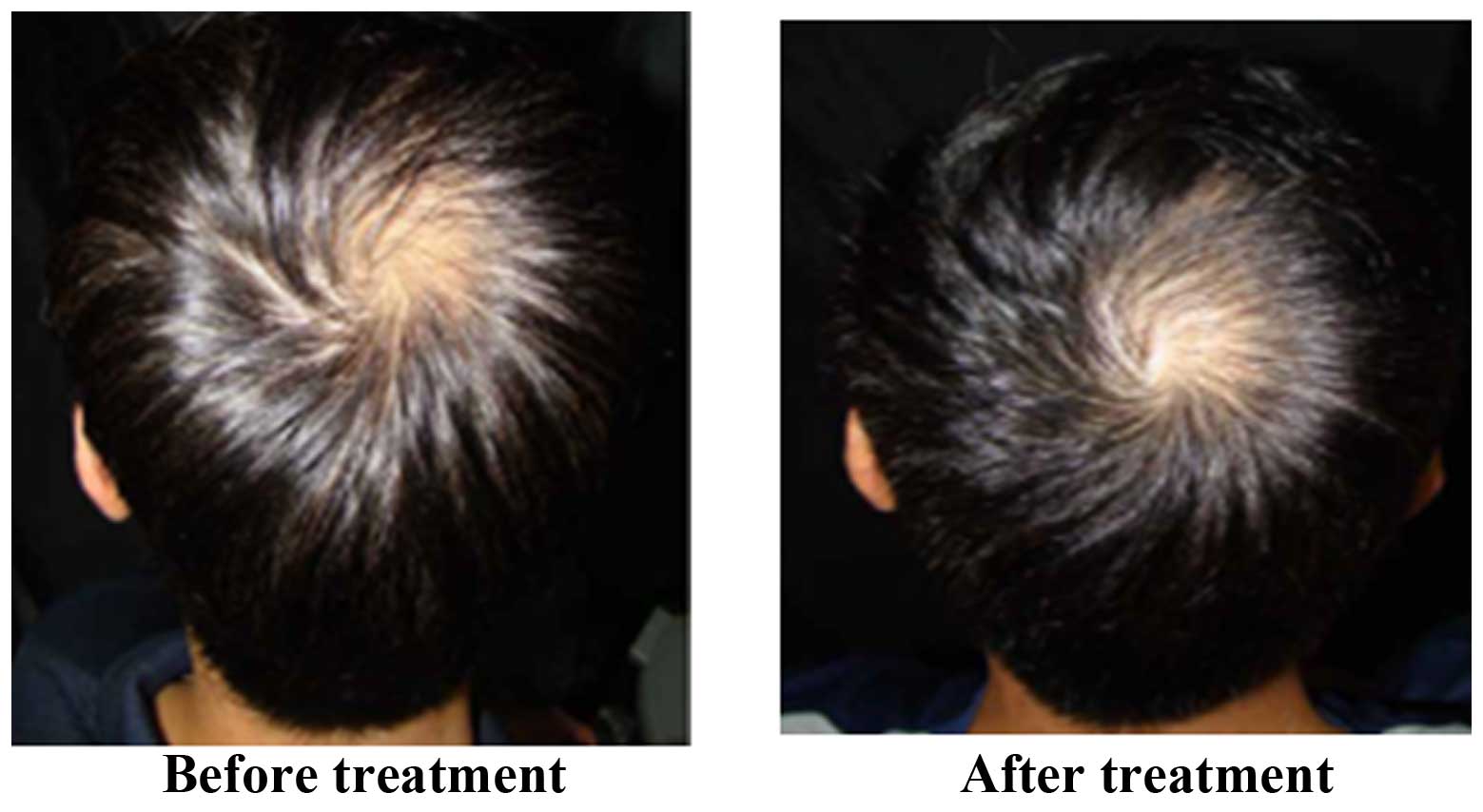
growth. Fig. 3 shows images of
patients with moderate improvement in hair growth. Fig. 4 shows images of patients with minimal
improvement in hair growth. During the trial period, blood
biochemical examination results for participants in the treatment
and placebo groups were normal, and no adverse reactions
occurred.
| Table II.Effect of using BeauTop on improving
androgenetic alopecia after 6 months. |
Table II.
Effect of using BeauTop on improving
androgenetic alopecia after 6 months.
|
| Significantly
worse | Moderately
worse | Minimally
worse | No change | Minimally
improved | Moderately
improved | Significantly
improved |
|---|
| BeauTop, n (%) (17
participants) | (0/17) 0% | (0/17) 0% | (0/17) 0% | (8/17) 47.1% | (1/17) 5.9% | (5/17) 29.4% | (3/17) 17.6% |
| Placebo, n (%) (15
participants) | (0/15) 0% | (1/15) 7% | (4/15) 27% | (8/15) 53% | (2/15) 13% | (0/15) 0% | (0/15) 0% |
Blood examination
The pretreatment and post-treatment blood
examination results for items including liver function, renal
function and hormone levels [dehydroepiandrosterone (DHEA),
testosterone, and estradiol] were not significantly different
(Tables III–VIII). The average WBC count for the
treatment group was significantly elevated on week 4 compared with
the control group (6770 vs. 7560/mm3; P<0.014) and
significantly decreased at week 24 (6240/mm3;
P<0.493).
| Table III.Blood examination results at week
4. |
Table III.
Blood examination results at week
4.
|
| Treatment
(n=20) | Placebo (n=20) | P-value |
|---|
| ALT,
IU/la | 27.85±20.18 | 21.85±10.22 | 0.245 |
| AST,
IU/la | 21.75±10.31 | 20.68±5.41 | 0.687 |
| r-GT,
U/la | 49.80±73.43 | 24.11±23.29 | 0.150 |
| BUN,
mg/dlb | 14.01 (3.97) | 14.50 (3.64) | 0.444 |
| Creatinine,
mg/dla | 0.73±0.16 | 0.82±0.18 | 0.120 |
| Iron,
mg/dla | 99.80±37.60 | 98.16±33.66 | 0.887 |
| Ferritin,
ng/mla | 142.01±84.34 | 200.93±141.97 | 0.128 |
| WBC, 103/mm3
b | 7.56 (2.20) | 5.70 (1.81) | 0.014 |
| RBC, million/mm3
b | 4.97 (0.59) | 4.94 (0.65) | 0.802 |
| Hb,
g/dlb | 14.95 (2.30) | 14.90 (2.20) | 0.933 |
| Hct, %b | 43.45 (4.95) | 43.70 (4.60) | 1.000 |
| DHEA,
ng/mlb | 198.15
(141.80) | 194.00
(132.00) | 0.845 |
| Testosterone,
ng/mla | 3.02±2.13 | 3.04±1.94 | 0.976 |
| Estradiol,
ng/mla | 51.81±58.95 | 45.43±33.46 | 0.679 |
| Table VIII.Blood examination results at week
24. |
Table VIII.
Blood examination results at week
24.
|
| Treatment
(n=17) | Placebo (n=15) | P-value |
|---|
| ALT,
IU/la | 24.71±9.63 | 21.93±11.60 | 0.466 |
| AST,
IU/la | 20.65±4.53 | 20.07±6.35 | 0.766 |
| r-GT,
U/la | 38.47±41.45 | 27.60±35.10 | 0.433 |
| BUN,
mg/dlb | 13.52 (5.22) | 14.70 (3.63) | 0.352 |
| Creatinine,
mg/dla | 0.75±0.13 | 0.73±0.14 | 0.687 |
| Iron,
mg/dla | 87.24±27.35 | 122.07±54.27 | 0.036 |
| Ferritin,
ng/mla | 153.45±100.30 | 184.31±104.87 | 0.402 |
| WBC, 103/mm3
b | 6.24 (1.88) | 5.89 (1.01) | 0.493 |
| RBC, million/mm3
b | 5.06 (0.45) | 4.76 (0.58) | 0.172 |
| Hb,
g/dlb | 15.10 (1.70) | 14.60 (1.80) | 0.352 |
| Hct, %b | 44.00 (3.60) | 42.80 (3.50) | 0.444 |
| DHEA,
ng/mlb | 230.30 (53.10) | 211.90 (94.00) | 0.681 |
| Testosterone,
ng/mla | 3.36±1.90 | 7.46±17.36 | 0.378 |
| Estradiol,
ng/mla | 40.45±11.44 | 53.27±25.47 | 0.089 |
Discussion
Hernandez (13)
indicated that DHT serves an important role in androgenetic
alopecia and speculated that DHT is contained in the scalp and
spreads to blood vessels. Finasteride blocks the conversion of
testosterone to DHT, and rapidly reduces the DHT content in the
blood and scalp by ≤60%; however, it is only effective for treating
androgenetic alopecia (5). The
treatment effect is maintained with continuous administration and
diminishes completely after 6 to 12 months of discontinuation
(14). Similar to DHT, DHEA is a
potent androgen (14), and
decreasing the concentrations of both substances helps prevent
alopecia. The results of this study indicate that BeauTop has
minimal effects on DHEA, testosterone and estradiol. DHEA and
testosterone were not significantly different between the treatment
and control groups; however, there was a trend observed in
estradiol on week 20 between the treatment and control groups. This
suggests that the mechanism of action of BeauTop varies from that
of finasteride. Further research is required to establish its
mechanism of action.
The results of the present study indicate that the
effect of treatment is most marked at stages III and IV, supporting
the concept of early treatment typically acknowledged by
dermatologists. The poor treatment effect for stage II is
associated with the difficulty of new hair growth in the frontal
area. In addition, the superior treatment effect at stage VI is
attributable to the complete baldness on the crown where the growth
of any fine hair is easily noticed. The optimal age for treatment
is ~40 years of age, possibly because people at this age have
greater concerns for alopecia, and are therefore more attentive to
factors that affect hair health, including diet, sleep, mood and
scalp hygiene. This speculation is supported by the poor treatment
effect in 20-year-old patients (inattentive to previously-described
factors that affect alopecia). Furthermore, blood examination of
DHEA, testosterone and estradiol confirms that no pre-treatment and
post-treatment difference exists between male and female
participants receiving BeauTop. Evidently, BeauTop is suitable for
male and female patients.
BeauTop is formulated from the following six herbal
ingredients: Ginseng Radix, Astragali Radix,
Angelicae Sinensis Radix, Ligustri Fructus,
Rehmannia glutinosa and Eclipta prostrata Linn. One
study reported the effects of saponin from Ginseng Radix
rubra on extracellular matrix metabolism. Saponin stimulates
fibronectin synthesis through the changes of transforming growth
factor-β receptor expression in fibroblasts (15) A formulation containing Radix
Ginseng and Radix Notoginseng was reported to promote
human umbilical vein endothelial cells (HUVEC) proliferation and
secretion of VEGF, as well as the expression of VEGF receptor 2
(VEGFR2) protein, which may be one of the underlying mechanisms of
Radix Ginseng and Radix Notoginseng formula in
promoting angiogenesis (16).
Astragali Radix enhances the immunity of the human body
(17). Angiogenesis serves an
important role in a wide range of physiological processes and a
number of diseases are associated with the dysregulation of
angiogenesis. Astragali Radix, commonly used in traditional
Chinese medicine, is a potential candidate for treating such
diseases. It is understood that Radix Astragali extract
(RAE) treatment stimulates HUVEC to proliferate (18). It was shown that RAE enhances VEGF
mRNA expression and that a specific blocker of VEGFR2 (KDR/Flk)
inhibited RAE-induced HUVEC proliferation. These data suggest that
RAE is a potent stimulator of angiogenesis and that its
pro-angiogenic effects involve the VEGF-KDR/Flk and PI3K-Akt-eNOS
signaling pathways (18).
Angelicae Sinensis Radix is being commonly used to promote
blood circulation (19) in the
treatment of menstrual disorders. In recent decades there have been
a number of reports of the pharmacological functions and activities
of Rehmannia glutinosa and its active principles on the
blood system, anti-inflammatory responses and the immune system
(20,21). One study indicates that Rehmannia
glutinosa oligosaccharide (RGO) may increase the viability and
proliferative capacity and alleviate
H2O2-induced apoptosis of human
adipose-derived mesenchymal stem cells via the paracrine release of
VEGF and hepatocyte growth factor. These results indicate that RGO
application will enhance stem cell viability and improve their
effects in cell therapy (22).
Butanol extract from Eclipta prostrata Linn has an
anti-oxidative effect on cesarean-derived rats, and saponin is a
primary ingredient in butanol extract, which has been found to have
in vitro anti-oxidative effects (23,24).
Further study is required to determine whether these effects are
associated with BeauTop's effect on improving androgenetic
alopecia.
The expressions of the growth factors during the
study period indicated that VEGF, EGF and FGF-7 in the BT group on
day 8 presented higher area percentage compared with the control,
respectively. However, the area percentage of FGF-5 in the BT-3
group was even lower than the control on day 12. According to the
experimental data, it was presumed that BT, may induce EGF and
FGF-7 production at the depilation area of hair follicle on day 8
(P<0.05), and reduce FGF-5 production on day 12 (P<0.05).
Further human research is required to establish whether the
mechanism of action in animal studies applies to improving of human
androgenetic alopecia. From these data, it can be suggested that
BeauTop had the potential to improve androgenetic alopecia in males
and females via the induction of several growth factors (VEGF, EGF
and FGF).
In the present study, the average WBC count for the
treatment group compared with the control group was significantly
increased on week 4, and significantly decreased on week 24.
However, the WBC count was in the normal range. Danggui Buxue Tang
(DBT), a Chinese medicinal decoction that is being commonly used as
hematopoietic medicine to treat woman with menopausal
irregularities, contains two herbs: Astragali Radix and
Angelicae Sinensis Radix (25). Pharmacological results indicate that
DBT can stimulate the production of erythropoietin (EPO), a
specific hematopoietic growth factor, in cultured cells (26). This study found an increase in the
mRNA and protein expression of hypoxia-inducible factor-1α
(HIF-1α). In addition, activation of the Raf/MEK/ERK signaling
pathway by DBT could enhance the translation of HIF-1α, suggesting
dual actions of DBT in stimulating EPO expression in kidney cells.
These results provide one of the molecular mechanisms of this
ancient herbal decoction DBT and its hematopoietic function
(26). Because the Hb values of
patients in the present study were within the normal range, there
was no significant difference between the treatment and control
groups. In this study, no adverse reaction occurred in participants
receiving BeauTop, suggesting that the drug is safe to consume.
A previous study revealed that patients who received
1 mg finasteride/day for one year reported improved hair growth
compared with the placebo on the basis of improvements in scalp
hair growth and their satisfaction with the appearance of hair
(27). Within the treatment group,
56% of subjects reported no change in hair growth, 22% reported
minimal improvement and 22% reported moderate improvement (27). Another study indicated that patients
who received finasteride 1 mg/day for long-term treatment over five
years experienced durable improvements in scalp hair growth, and a
slowed further progression of hair loss occurred without treatment
(12). Within the treatment group,
no change in hair growth occupied 42%, minimally improved hair
growth occupied 22%, moderately improved hair growth occupied 21%
and significantly improved hair growth occupied 5% (12).
The current study showed that BeauTop improved
androgenetic alopecia after six months; 47.1% experienced no
change, 5.9% experienced minimally improved, 29.4% experienced
moderately improved and 17.6% experienced significantly improved
hair growth. The difference between studies with patients receiving
finasteride treatment and the present study was that the duration
of the present study using BeauTop was 6 months, whereas the
research periods on finasteride were 1 or 5 years (28). BeauTop is superior to finasteride
(1-year and 5-year treatments) in producing a significant
improvement in androgenetic alopecia. BeauTop is comparable with
finasteride in producing moderate improvement on androgenetic
alopecia, and is slightly inferior in producing minimal
improvement. Female pattern hair loss is the most common cause of
hair loss in women, and prevalence increases with advancing age
(28). While a number of women using
oral anti-androgens and topical minoxidil will regrow some hair,
the effect of improvement in hair loss is limited (28). Previous studies have indicated that
the optimum treatment period is between 1 and 2 years (5,27).
Previous animal studies have demonstrated that BeauTop's mechanism
of action in improving androgenetic alopecia is possibly associated
with the VEGF, EGF, FGF-5 and FGF-7 (11), and from this randomized double-blind
placebo-controlled clinical trial, it can be suggested that BeauTop
effectively improves male and female androgenetic alopecia. Future
studies on BeauTop are required to observe its effects on improving
androgenetic alopecia after treatment for >1 year, and to
determine whether the effect continue after drug discontinuation.
In conclusion, BeauTop effectively improves male and female
androgenetic alopecia.
Acknowledgements
Our special thanks to the non-profit organization
Brion Research Institute of Taiwan and Chung Shan Medical
University (grant no. CSMU-INT-104-03) for its sponsorship, which
contributed to the completion of this study.
Glossary
Abbreviations
Abbreviations:
|
5αR
|
5α-reductase
|
|
AGA
|
androgenetic alopecia
|
|
ALT
|
alanine aminotranferease
|
|
AST
|
aspartate aminotransferase
|
|
BUN
|
blood urea nitrogen
|
|
DBT
|
danggui buxue tang
|
|
DHEA
|
dehydroepiandrosterone
|
|
DHT
|
dihydrotestosterone
|
|
EGF
|
epidermal growth factor
|
|
EPO
|
erythropoietin
|
|
FGF
|
fibroblast growth factors
|
|
Hct
|
hematocrit
|
|
Hb
|
hemoglobin
|
|
HIF-1α
|
hypoxia-inducible factor-1α
|
|
r-GT
|
gamma-glutamyl transpeptidase
|
|
TSH
|
thyroid stimulating hormone
|
|
VEGF
|
vascular endothelial growth factor
|
|
WBC
|
white blood cell
|
References
|
1
|
Piraccini BM and Alessandrini A:
Androgenetic alopecia. G Ital Dermatol Venereol. 149:15–24.
2014.PubMed/NCBI
|
|
2
|
Otberg N, Finner AM and Shapiro J:
Androgenetic alopecia. Endocrinol Metab Clin North Am. 36:379–398.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sinclair R: Male pattern androgenetic
alopecia. BMJ. 317:865–869. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Leavitt M: Understanding and management of
female pattern alopecia. Facial Plast Surg. 24:414–427. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kaufman KD, Olsen EA, Whiting D, Savin R,
DeVillez R, Bergfeld W, Price VH, Van Neste D, Roberts JL,
Hordinsky M, et al: Finasteride in the treatment of men with
androgenetic alopecia. Finasteride Male Pattern Hair Loss Study
Group. J Am Acad Dermatol. 39:578–589. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rahimi-Ardabili B, Pourandarjani R,
Habibollahi P and Mualeki A: Finasteride induced depression: A
prospective study. BMC Clin Pharmacol. 6:72006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kumar N, Rungseevijitprapa W, Narkkhong
NA, Suttajit M and Chaiyasut C: 5α-reductase inhibition and hair
growth promotion of some Thai plants traditionally used for hair
treatment. J Ethnopharmacol. 139:765–771. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Nahata A and Dixit VK: Evaluation of
5α-reductase inhibitory activity of certain herbs useful as
antiandrogens. Andrologia. 46:592–601. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Foitzik K, Hoting E, Förster T, Pertile P
and Paus R: L-carnitine-L-tartrate promotes human hair growth in
vitro. Exp Dermatol. 16:936–945. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kang JI, Kim SC, Han SC, Hong HJ, Jeon YJ,
Kim B, Koh YS, Yoo ES and Kang HK: Hair-loss preventing effect of
grateloupia elliptica. Biomol Ther (Seoul). 20:118–124. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lee, CY, Yang CY, Lin CC, Yu, MN, Sheu SJ
and Kuan YH: Hair growth is promoted by BeauTop via the expression
of epidermal growth factor and fibroblast growth factor-7. Mol Med
Rep. (In press).
|
|
12
|
Finasteride Male Pattern Hair Loss Study
Group, . Long-term (5-year) multinational experience with
finasteride 1 mg in the treatment of men with androgenetic
alopecia. Eur J Dermatol. 12:38–49. 2002.PubMed/NCBI
|
|
13
|
Hernandez BA: Is androgenic alopecia a
result of endocrine effects on the vasculature? Med Hypotheses.
62:438–441. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Labrie F, Luu-The V, Martel C,
Chernomoretz A, Calvo E, Morissette J and Labrie C:
Dehydroepiandrosterone (DHEA) is an anabolic steroid like
dihydrotestosterone (DHT), the most potent natural androgen, and
tetrahydrogestrinone (THG). J Steroid Biochem Mol Biol. 100:52–58.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kanzaki T, Morisaki N, Shiina R and Saito
Y: Role of transforming growth factor-beta pathway in the mechanism
of wound healing by saponin from Ginseng Radix rubra. Br J
Pharmacol. 125:255–262. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lei Y, Tian W, Zhu LQ, Yang J and Chen KJ:
Effects of radix ginseng and radix notoginseng formula on secretion
of vascular endothelial growth factor and expression of vascular
endothelial growth factor receptor-2 in human umbilical vein
endothelial cells. Zhong Xi Yi Jie He Xue Bao. 8:368–372. 2010.(In
Chinese). View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Jin R and Kurashige S: Effects of Chinese
herbs on macrophage functions in N-butyl-N-butanolnitrosoamine
treated mice. Immunopharmacol Immunotoxicol. 18:105–114. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zhang Y, Hu G, Lin HC, Hong SJ, Deng YH,
Tang JY, Seto SW, Kwan YW, Waye MM, Wang YT and Lee SM: Radix
Astragali extract promotes angiogenesis involving vascular
endothelial growth factor receptor-related phosphatidylinositol
3-kinase/Akt-dependent pathway in human endothelial cells.
Phytother Res. 23:1205–1213. 2009. View
Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yim TK, Wu WK, Pak WF, Mak DH, Liang SM
and Ko KM: Myocardial protection against ischaemia-reperfusion
injury by a Polygonum multiflorum extract supplemented ‘Dang-Gui
decoction for enriching blood’, a compound formulation, ex vivo.
Phytother Res. 14:195–199. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zhang RX, Li MX and Jia ZP: Rehmannia
glutinosa: Review of botany, chemistry and pharmacology. J
Ethnopharmacol. 117:199–214. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Zhang X, Zhang A, Jiang B, Bao Y, Wang J
and An L: Further pharmacological evidence of the neuroprotective
effect of catalpol from Rehmannia glutinosa. Phytomedicine.
15:484–490. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zhang Y, Wang Y, Wang L, Zhang Y, Qin Y,
Chen T, Han W and Chen G: Effects of Rehmannia glutinosa
oligosaccharide on human adipose-derived mesenchymal stem cells in
vitro. Life Sci. 91:1323–1327. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kim DI, Lee SH, Hong JH, Lillehoj HS, Park
HJ, Rhie SG and Lee GS: The butanol fraction of Eclipta prostrata
(Linn) increases the formation of brain acetylcholine and decreases
oxidative stress in the brain and serum of cesarean-derived rats.
Nutr Res. 30:579–584. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kim DI, Lee SH, Choi JH, Lillehoj HS, Yu
MH and Lee GS: The butanol fraction of Eclipta prostrata (Linn)
effectively reduces serum lipid levels and improves antioxidant
activities in CD rats. Nutr Res. 28:550–554. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zierau O, Zheng KY, Papke A, Dong TT, Tsim
KW and Vollmer G: Functions of Danggui Buxue Tang, a Chinese herbal
decoction containing Astragali Radix and Angelicae Sinensis Radix,
in uterus and liver are both estrogen receptor-dependent and
-independent. Evid Based Complement Alternat Med. 438–531.
2014.
|
|
26
|
Zheng KY, Choi RC, Xie HQ, Cheung AW, Guo
AJ, Leung KW, Chen VP, Bi CW, Zhu KY, Chan GK, et al: The
expression of erythropoietin triggered by danggui buxue tang, a
Chinese herbal decoction prepared from radix Astragali and radix
Angelicae Sinensis, is mediated by the hypoxia-inducible factor in
cultured HEK293T cells. J Ethnopharmacol. 132:259–267. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Stough DB, Rao NA, Kaufman KD and Mitchell
C: Finasteride improves male pattern hair loss in a randomized
study in identical twins. Eur J Dermatol. 12:32–37. 2002.PubMed/NCBI
|
|
28
|
Dinh QQ and Sinclair R: Female pattern
hair loss: Current treatment concepts. Clin Interv Aging.
2:189–199. 2007.PubMed/NCBI
|