Introduction
Atherosclerosis is a chronic inflammation of the
vascular wall that results in the development of plaques and
subsequent stenosis of the arteries (1,2). A
number of cytokines are involved in atherosclerosis-related
inflammation; these include tumor necrosis factor alpha (TNF-α),
interleukin (IL)-6 and monocyte chemoattractant protein-1 (MCP-1).
These factors induce the expression of intercellular adhesion
molecule 1 (ICAM-1), vascular cell adhesion molecule 1 (VCAM-1) and
E-selectin adhesion molecules and lipid homeostasis (3,4). Other
important cytokines responsible for the cross-talk phenomenon that
occurs between inflammatory cells and intrinsic factor wall cells
are IL-1β and platelet-derived growth factor cross-reactive
material (1). Inflammation
associated with atherosclerosis is mediated via the nuclear factor
κB (NF-κB) signaling pathway, implying that substances inhibiting
or activating this factor serve an important role in atherogenesis
(5). Sirtuin-1 (SIRT1), adiponectin
and calprotectin (S100A8/A9) are characterized as factors able to
modulate either the NF-κB signaling pathway or toll-like receptor 4
(TLR-4) (6–9). Furthermore, they are considered to be
important elements for the molecular pathogenesis of
atherosclerosis (4–6,10,11).
SIRT1 is highly expressed in endothelial cells where it controls
angiogenesis through a broad variety of transcriptional regulators,
including p53, fork-head box O (FoxO), NF-κB, promyelocytic
leukemia protein and activated receptor-γ. SIRT1 serves a crucial
role in endothelial homeostasis and it is suggested that
overexpression of SIRT1 may contribute to vasoprotection (12,13). In
a previous experimental study, it was demonstrated that activation
of SIRT1 is associated with a reduction in atherosclerotic lesion
macrophage content, as well as atherosclerotic lesion size in
aortic arches (6). Furthermore,
SIRT1 transgenic apolipoprotein E null (apoE−/−) mice
had fewer atherosclerotic lesions, indicating that
endothelium-specific SIRT1 overexpression may suppress
atherogenesis by influencing endothelial cell survival and
function, mediated through regulating the level of nitric oxide
synthase (NOS)-3 (14).
The level of adiponectin is negatively associated
with visceral fat area and body mass index increase; this explains
the marked reduction of adiponectin levels in a number of obese and
insulin-resistant states (15).
Observational human studies, despite their insufficiency, indicate
that low adiponectin levels are associated with cardiometabolic
disorders (16). Furthermore, a low
level of adiponectin is presented as a risk factor for the
occurrence of atherosclerotic diseases (3). Previous studies using animal models
provide conclusions that adiponectin possesses anti-atherogenic
properties, which inhibit the formation of atherosclerotic lesions,
and overexpression of adiponectin protects against atherosclerosis
(4,5).
The S100A8/A9 heterodimer protein is formed of the
monomers S100A8 and S100A9, belonging to the S100 family. S100A8
and S100A9 are characterized by their ability to interact with
numerous effector proteins, mostly in a calcium
(Ca2+)-dependent manner (17,18). The
S100A8/A9 complex has the ability to bind to the endothelium, a
process enabled by an interaction between S100A9 and heparin
sulphate proteoglycans, but also the S100A8/A9 complex with
carboxylated N-glycans, expressed by endothelial cells during
inflammation (19). The serum level
of S100A8/A9 is associated with an early risk of acute coronary
syndromes and the severity of coronary artery disease in diabetic
individuals. Previous small sub-group studies also indicate that
S100A8/A9 may be a marker of subclinical atherosclerosis, as its
elevation in serum corresponds with intima media thickness in
patients with diabetes but without any history of previous
cardiovascular diseases (CVD) (10,11).
Another identified factor in atherogenesis is
vascular contractility, as it is considered clinically relevant
that arterial hypertension aggravates atherosclerosis (20). Essential hypertension is the
consequence of increased peripheral vascular resistance in
resistant arteries. Arteries in hypertensive individuals present
increased reactivity to contractive stimulus in comparison to
healthy individuals, however the exact cause remains unclear
(21,22). Hypertension increases oxidative
stress in the vascular wall, contributing to changes in metabolism,
subsequent endothelium dysfunction and proliferation of vascular
smooth muscle cells (VSMCs) (20).
Furthermore, hypertension causes an increase in the level of
acute-phase proteins that are circulating in the bloodstream, which
have been demonstrated to activate the inflammation process through
TLR-4 signaling (21).
Structurally, resveratrol belongs to a group of
polyphenols that have been described to have a number of beneficial
effects on the cardiovascular system and have been proved to be
potent activators of SIRT1 and adiponectin (23). Additionally, the present study
hypothesized that it may have a regulatory effect on S100A8/A9 in
the endothelium. Resveratrol exerts protective properties against
atherosclerosis-associated endothelial dysfunction and senescence
by upregulating endothelial NOS and SIRT1 (12). Anti-inflammatory features of the
aforementioned polyphenol are described as the ability to scavenge
free radicals, as well as inhibit the NF-κB signaling pathway
(24).
Vasoprotective properties of resveratrol are well
documented by in vitro and animal model studies; therefore
the present study used a rat model to assess the effect of 4-week
oral administration of resveratrol on serum concentrations of
SIRT1, adiponectin and S100A8/A9. Another aim of the present study
was to determine whether resveratrol contributes to decreased
vascular reactivity and define the mechanisms underlying the
resveratrol-induced relaxation of VSMCs.
Materials and methods
Animals
A total of 17 male Wistar rats (Hodowla Zwierząt
Laboratoryjnych, Brwinów, Poland) weighing 250–350 g were selected
for the study. The rats were maintained in 12-h light and dark
cycles at 20–21°C and a humidity of 50–60%. Ad libitum access to
food and drinking water during the day and night was provided. The
rats were randomly grouped into a treatment (n=9) and control group
(n=8). The treatment group was administered resveratrol orally for
a period of 4 weeks and the control group was administered a
placebo (water). Blood sampling for biochemical tests was performed
0, 2 and 4 weeks before the initiation of resveratrol pretreatment
via catheter placed in femoral vein. Following 4 weeks of
resveratrol pretreatment rats were anesthetized with 120 mg/kg
urethane (Honeywell International Inc., Seelze, Germany)
intraperitoneally, and subsequently sacrificed by cervical
dislocation. The pharmacometric section of the present study was
performed on isolated rat-tail artery, as a recognized model of
resistance artery (25). The
protocol of the present study was approved by the Ethics Committee
for Experiments on Animals (University of Technology and Life
Sciences, Bydgoszcz, Poland). All experiments were carried out in
accordance with the U.S. National Institutes of Health
guidelines.
Drugs and solutions
Resveratrol (Tocris Bioscience, Bristol, UK) at a
dose of 10 mg/kg was administered orally through orogastric
catheter. Dose was selected based on a previous trial (26). Reagents used during pharmacometric
tests included: A-7 hydrochloride
[N-(10-Aminodecyl)-5-chloro-1-naphthalenesulfonamide hydrochloride]
and Krebs-Henseleit solution [NaCl (71.8 mM), KCl (4.7 mM),
CaCl2 (1.7 mM), NaHCO3 (28.4 mM),
MgSO4 (2.4 mM), KH2PO4 (1.2 mM)
and glucose (11.1 mM)]. Resveratrol and A-7 hydrochloride were
purchased from Tocris Bioscience (Bristol, UK), and Krebs-Henseleit
solution was purchased from Sigma-Aldrich; Merck KGaA (Darmstadt,
Germany).
Study design and conduction
The trial was divided in two sections. The first
part consisted of the oral pretreatment of rats with 10 mg/kg
resveratrol solution daily (treatment group) or the same volume of
water (control group) for 4 weeks. Blood sampling was performed on
day 0 and 2 and 4 weeks following the initiation of the trial.
Blood was collected into a sample tube containing clotting
activator and subsequently subjected to centrifugation at room
temperature for 15 min at 160 × g. The supernatant was stored at
−86°C. Serum concentrations of S100A8/A9, SIRT1 and adiponectin
were evaluated using a number of commercially available ELISA kits.
These were a sirtuin ELISA kit (cat. no. 201-11-1498; Shanghai
Sunred Biological Technology Co., Ltd.; Shanghai, China), a
calprotectin ELISA kit (cat. no. EIA-5111; DRG International, Inc.,
Springfield, NJ, USA) and an adiponectin ELISA kit (cat. no.
E091-R; Mediagnost GmbH, Reutlingen, Germany).
The procedure for the pharmacometric trial was
adapted from a previous study (27).
Sections of rat tail arteries (2.5–3.0-cm long), without
significant branching, were dissected, subjected to the
introduction of a cannula through the proximal section and placed
vertically in a 20-ml Multi Chamber Tissue Bath System (TSZ-04;
Experimetria Ltd., Budapest, Hungary). Subsequently, the cannula
was connected to a perfusion device (Zalimp, Warsaw, Poland) and
the artery was strained with 500 mg weight. During the initial part
of the assay, the vessel was stabilized in oxygenated
Krebs-Henseleit solution (Merck KGaA) at a temperature 37.0°C and
pH 7.4. Perphusate flow was performed using a peristaltic pump with
flow gradually increased from 0.25–1.0 ml/min, until a perfusion
pressure between 2–4 kPa was achieved. Artery contraction was
induced by injection of phenylephrine (PHE) (Merck KGaA) into the
lumen of the vessel. PHE is a full α1-adrenergic receptor agonist,
in the control conditions and in the presence of A-7 hydrochloride
(Tocris Bioscience). A-7 hydrochloride at a dose of 3 µM/l was
selected, as it is a potent calmodulin antagonist that is
characterized by the ability to inhibit calmodulin-activated
phosphodiesterase (PDE) activity with an IC50 of 3.0 µM
(28).
Vascular smooth muscle cells contractility was
determined as an increase in continuously measured perfusion
pressure. Perfusion pressure was measured on BPR-01 and BPR-02
transducers (Experimetria Ltd.) connected to a digital recorder
(Graphtec Midi Logger GL820; Grapthec Corp., Yokohama, Japan).
Statistical analysis
Statistical analysis was performed using SPSS
version 23.0 software (IBM SPSS, Armonk, NY, USA). The Shapiro-Wilk
test was used to determine normal distribution of the investigated
variables. To compare the differences between two mean values a
one-way analysis of variance test was used. Results were presented
as mean ± standard deviation. P<0.05 was considered to represent
a statistically significant difference. Concentration-response
curves (CRCs) were calculated according to the van Rossum method
(29). The maximal response of
tissue (Emax) was calculated as a percent of the maximal
response for PHE. Half maximal effective concentration
(EC50) was estimated using classical pharmacologic
methods with pD2 as the negative logarithm of the EC50,
similarly to previous studies (30).
The number of CRCs and Emax were used in all
calculations estimating the statistical significance.
Results
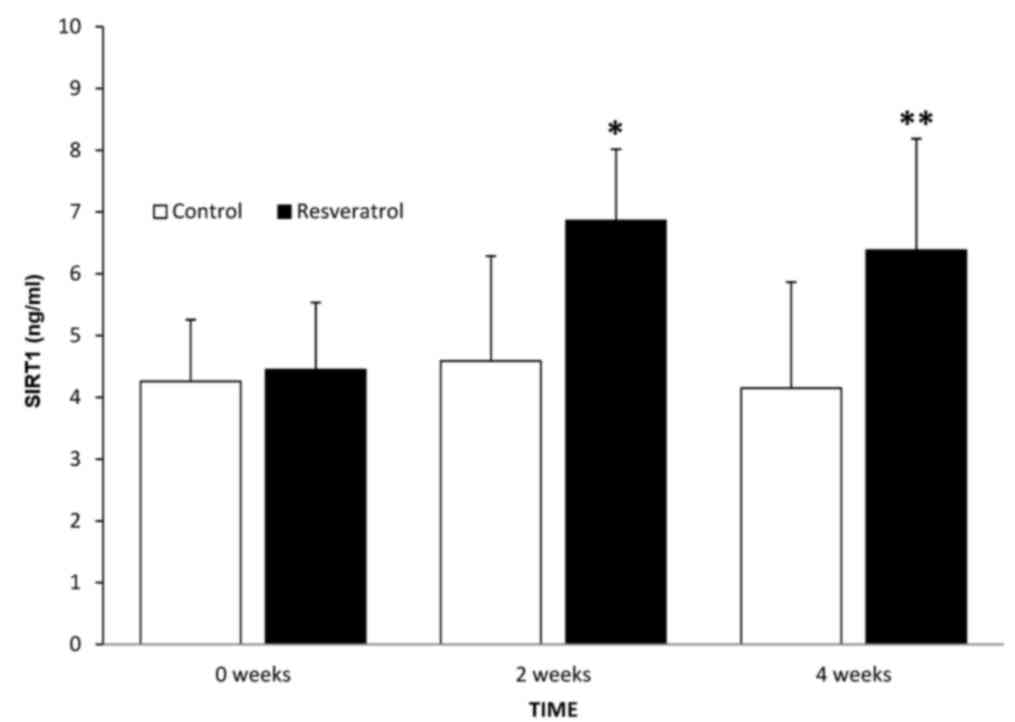
Effect of resveratrol administration
on serum SIRT1 concentration
Initial values of SIRT1 in the control and treatment
groups were 4.26 and 4.45 ng/ml, respectively (P=0.765). After 2
weeks, a significant increase was observed compared with the
control group (P=0.026). Values of serum SIRT1 in the control and
treatment groups following 2 weeks of treatment were 4.59 and 6.86
ng/ml, respectively. Following 4 weeks there was no increase in the
treatment group compared with the treatment group at 2 weeks
(P=0.547), but there was a significant difference between the
control and treatment groups following 4 weeks of treatment
(P=0.011). The levels of SIRT1 in the serum of control and
treatment groups were 4.15 and 6.38 ng/ml, respectively, at 4 weeks
(Fig. 1).
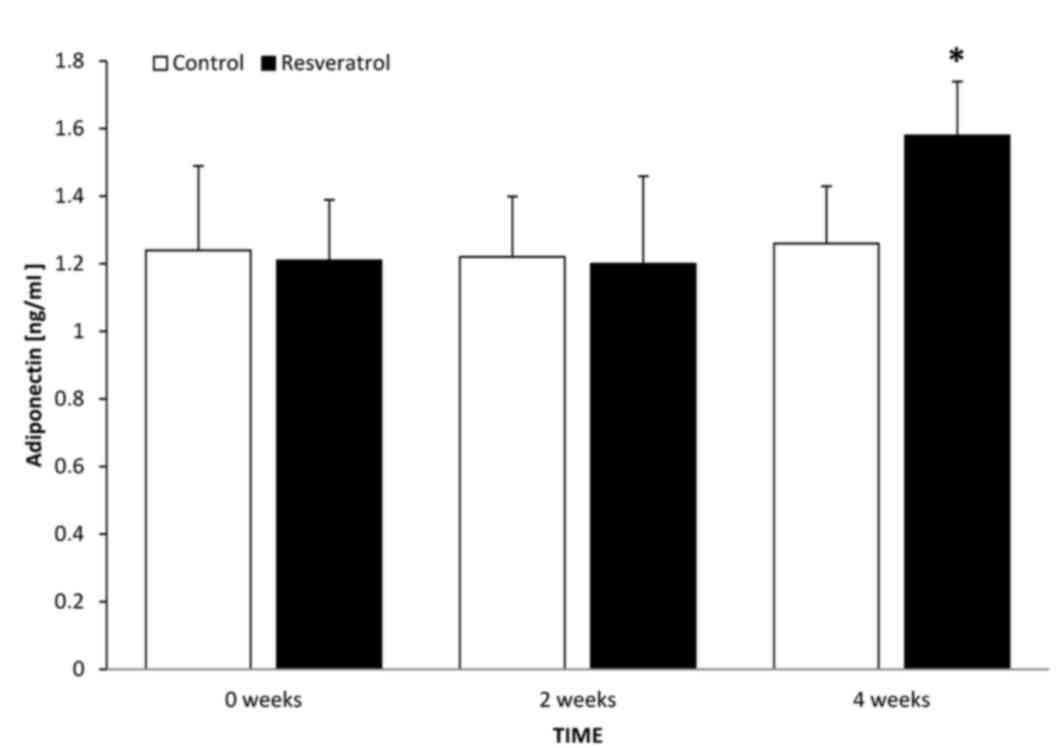
Effect of resveratrol administration
on serum adiponectin concentration
The levels of adiponectin in the control and
treatment groups at time 0 were 1.24 and 1.21 ng/ml, respectively
(P=0.827). After 2 weeks, there was no difference in adiponectin
level in the treatment group compared with the treatment group at
time 0, or with the corresponding control group at 2 weeks
(P=0.886). The levels of serum adiponectin in the control and
treatment groups following 2 weeks of treatment were 1.22 and 1.2
ng/ml, respectively. Following 4 weeks, there was a significant
increase in the treatment group compared with the treatment group
at 2 weeks (P=0.036) and a significant difference between the
control and treatment groups at 4 weeks (P=0.026). The levels of
serum adiponectin in the control and treatment groups following 4
weeks of treatment were 1.26 and 1.58 ng/ml, respectively (Fig. 2).
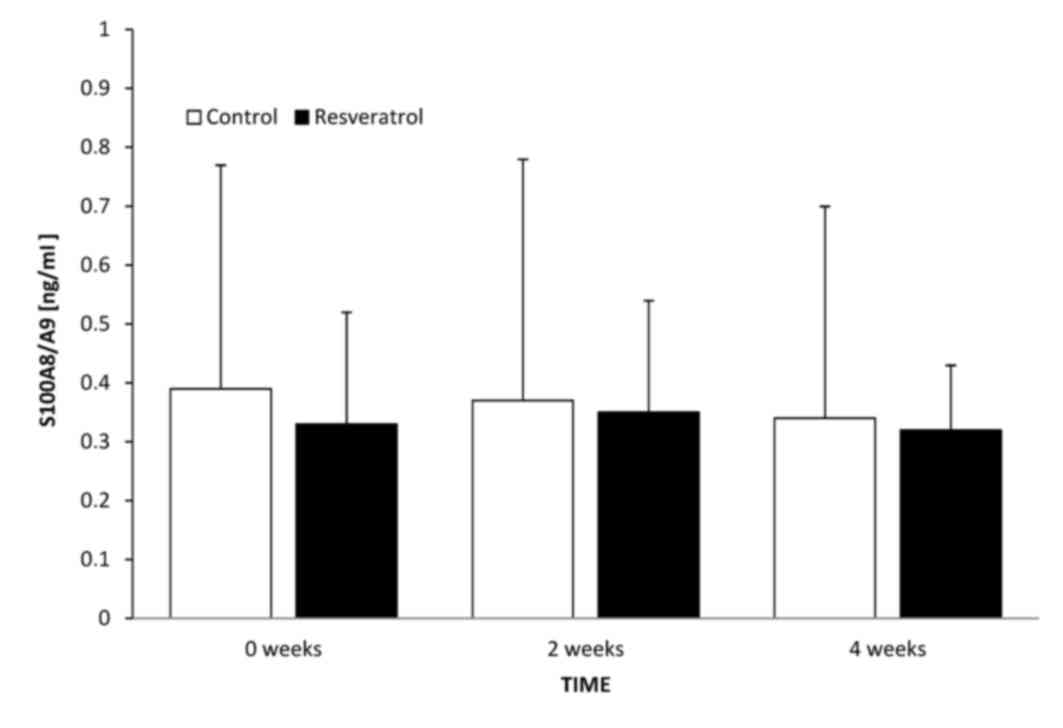
Effect of resveratrol administration
on serum S100A8/A9 concentration
The levels of S100A8/A9 in control and treatment
groups at time 0 were 0.39 and 0.33 ng/ml, respectively (P=0.935).
After 2 weeks, there was no significant difference between the
treatment group at 2 weeks and the treatment group at time 0
(P=0.811), or between this and the control group at 2 weeks
(P=0.827). In the control and treatment groups 2 weeks after the
initiation of the study, the levels of serum adiponectin were 0.37
and 0.35 ng/ml, respectively. After 4 weeks, there was no
significant difference in the treatment group at this time point
compared with the treatment group at 2 weeks (P=0.607), or with the
control group at 4 weeks (P=0.796). The levels of serum adiponectin
in the control and treatment groups 4 weeks from the initiation of
the study were 0.34 vs. 0.32 ng/ml, respectively (Fig. 3).
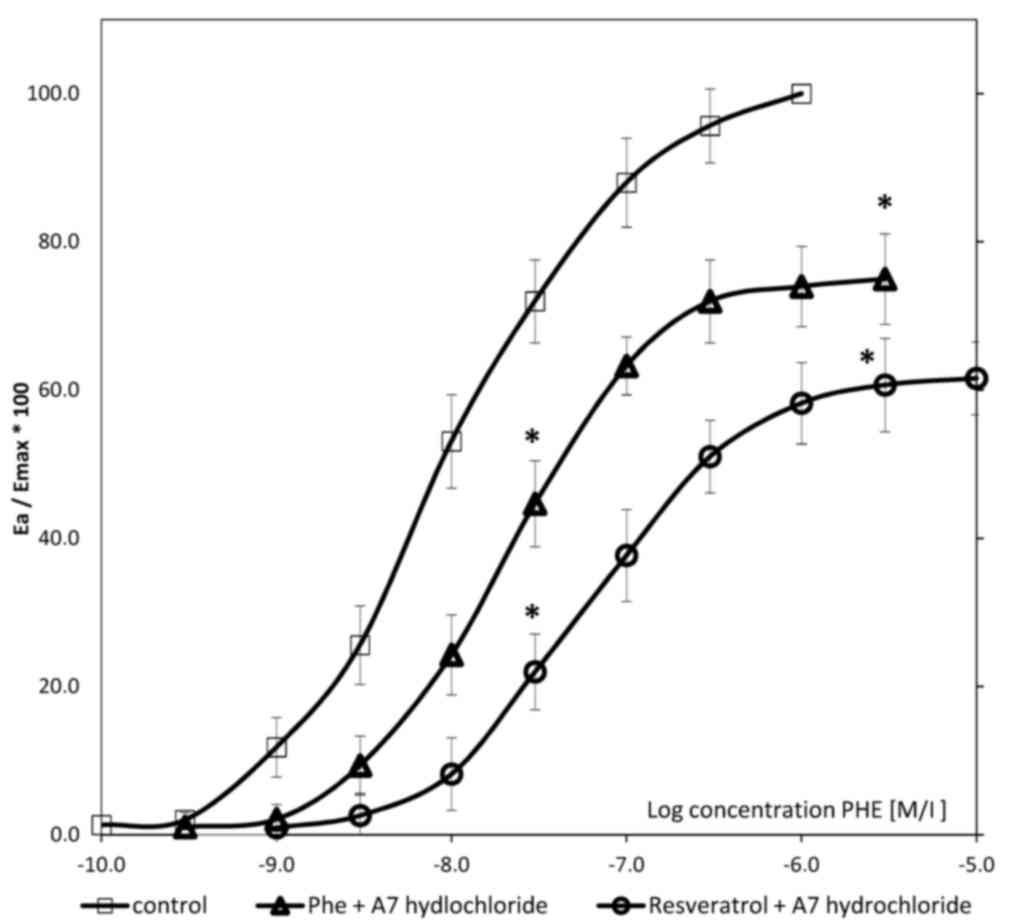
Effect of 4-week resveratrol
administration on VSMC contractility in the presence of A-7
hydrochloride
CRCs calculated for arteries with endothelium
derived from rats following 4 weeks of treatment with resveratrol
in the presence of 3 µM A7-hydrochloride shifted to the right in
both the PHE control and PHE/A7-hydrochloride treatment groups,
with the maximal response decrease of 25% (P<0.001) and 38.4%
(P<0.001), respectively. The EC50 value in arteries
with vascular endothelium calculated for PHE in rats following 4
weeks of resveratrol administration in the presence of
A7-hydrochloride was 7.25±(0.24)x10−7 M/l, whereas
control values for PHE control and PHE/A7-hydrochloride were
3.85(±0.51)x10−8 M/l and 7.25±(0.24)x10−7
M/l, respectively. In both cases, the increase of the
EC50 value was statistically significant (P<0.001;
Fig. 4; Table I).
 | Table I.Maximal relative response for
phenylephrine in relation to the absence and presence of
A7-hydrochloride in resveratrol-treated and control groups. |
Table I.
Maximal relative response for
phenylephrine in relation to the absence and presence of
A7-hydrochloride in resveratrol-treated and control groups.
| Group | na | Emax,
% | P-value vs.
control |
|---|
| Control-PHE (10
µM) | 12 | 100 | – |
|
PHE/A7-hydrochloride (3 µM) | 18 | 75.0±6.1 | P<0.001 |
| Resveratrol
pretreated rats + A7-hydrochloride (3 µM) | 22 | 61.6±4.9 | P<0.001 |
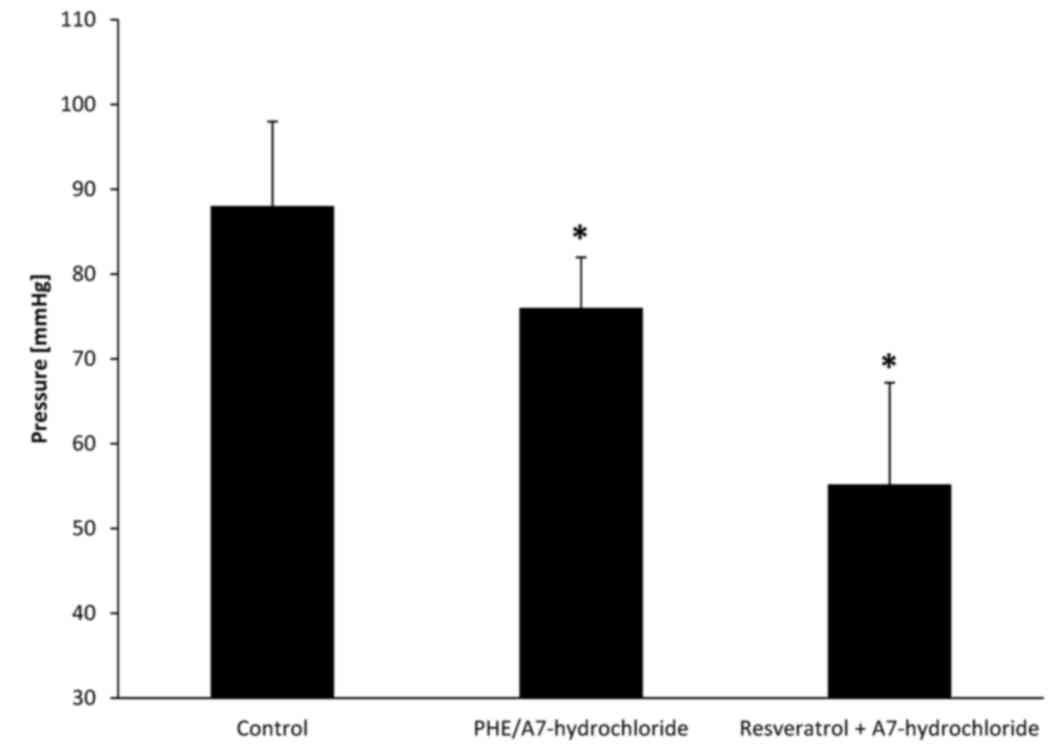
Effect of resveratrol on perfusion
pressure in the presence and absence of A7 hydrochloride
There was a significant reduction in perfusion
pressure in resveratrol-pretreated rat arteries in the presence of
A7-hydrochloride compared with the PHE control and
PHE/A7-hydrochloride groups (P=0.032; Fig. 5). Perfusion pressures in PHE control,
PHE/A7-hydrochloride and resveratrol-pretreated groups were 88±10,
76±6 and 55.2±12 mmHg, respectively.
Discussion
During in vitro and animal studies,
resveratrol previously demonstrated the ability to modulate
inflammation in the human body by regulating pro- and
anti-inflammatory cytokines (31).
Long-term human studies indicate that resveratrol improves the
inflammatory status, lipid profile and quality of life of patients
undergoing primary prevention of CVD (32–34).
Resveratrol inhibits the activation of inflammation-related
transcription factors including NF-κB (33). Resveratrol reduces the serum
concentrations of the inflammatory cytokines chemokine ligand 3,
IL-1β and TNF-α (32). In the
current study, resveratrol was demonstrated to increase serum
concentration levels of factors associated with atherosclerosis,
including SIRT1 and adiponectin, but this polyphenol did not
significantly affect the S100A8/A9 serum levels (P>0.05).
Furthermore, the effect on VSMC contractility was assessed and the
mechanisms underlying the reduction of the aforementioned
atherosclerosis-associated factors were evaluated. The results of
the present study reveal that resveratrol may act as an inhibitor
of Ca2+/calmodulin cyclic nucleotide PDE and contribute
to decrease the contractility of vessels.
Resveratrol administration reduces vascular
contractility; results of the pharmacological section of this study
indicate that resveratrol pretreated rat arteries require higher
concentrations of phenylephrine to induce a contraction. Presence
of A7-hydrochloride in experimental vessels inhibits
Ca2+/calmodulin cyclic nucleotide PDE1 (28), indicating that resveratrol mechanisms
of action are only partially dependent on the aforementioned PDE1
enzyme. The shape of the CRCs we acquired indicates that there is a
synergistic interaction between resveratrol and PDE1. In the
present study, rats that were administered 10 mg/kg resveratrol
daily for 4 weeks had significantly lower vascular reactivity in
the presence of A7-hydrochloride (P<0.05), which indicates that
resveratrol inhibits PDE1.
Resveratrol is described by Park et al
(35) to be a potent antagonist of
cAMP phosphodiesterases (including PDE1-4) that inhibits these
enzymes in a concentration-dependent manner. The results of the
study demonstrate that resveratrol is potentially a direct
inhibitor of PDEs (35), appearing
to be consistent with results of the present study. Specifically,
conclusions were generated on the basis of the shape of the CRCs
obtained. The ‘functional reserve’ of resveratrol (additional
decrease of vessel reactivity in the presence of A7-hydrochloride)
suggests that resveratrol may not only induce vasorelaxation via
the cyclic guanosine monophosphate (cGMP)-dependent pathways. Kline
and Karpinski (36) described the
ability of resveratrol to induce NOS-3 in direct and indirect
manners through the 5′ adenosine monophosphate-activated protein
kinase (AMPK), SIRT1 and nuclear factor erythroid 2-related factor
2 pathways; but it is also stated that resveratrol acts directly on
VSMCs by blocking the L-type calcium channel and inhibiting
intracellular Ca2+ release.
Rat model studies indicate that hypertension is
associated with the increase of PDE1 expression and activation
(37). Inhibition of PDE1 is
associated with the decrease of contractile response of the
arteries, which is caused by the increase of intracellular
concentrations of cGMP in VSMCs. (38). Phosphodiesterase 1C (PDE1C) is
potentially implicated in the pathogenesis of atherosclerosis. This
subtype of PDE1 is expressed in proliferating smooth muscle cells
(39). Inhibition of PDE1C by
resveratrol may produce additional beneficial effects due to
inhibition of VSMCs proliferation that appears to be one of the
crucial elements of atherogenesis (40).
Resveratrol administration increases the serum
concentration of SIRT1; previous animal model studies confirm that
SIRT1 is a potential target against atherosclerosis and its
upregulation serves an important role in molecular mechanisms of
endothelial activation (12,13). In the present study, 4-week oral
resveratrol treatment in rat models was observed to increase the
level of SIRT1 in serum. The results obtained in the current study
appear to be compatible with previously conducted trials assessing
SIRT1 expression via immunochemistry methods. Thompson et al
(41) identified that resveratrol
pretreatment of human VSMCs at a dose 3–100 µM significantly
increases SIRT1 expression. Kao et al (24) also observed an increase of SIRT1 mRNA
in human umbilical vein endothelial cells following pretreatment
with different doses of resveratrol (10–100 µM).
The molecular mechanisms of SIRT1 action are linked
with the prevention of atherosclerosis in a number of experimental
models. SIRT1 deacetylates RelA/p65 at K310 and suppresses its
binding to naked DNA in human aortic endothelial cells;
subsequently this interferes with NF-κB signal activation, thereby
preventing the expression of genes responsible for synthesis of
adhesion molecules, VCAM-1 and ICAM-1 (8,42).
Furthermore, previously described NF-κB signaling pathway
suppression by SIRT1 contributes to inhibition of pro-inflammatory
cytokine synthesis, including TNF-α, IL-1β, IL-6 and MCP-1
(6). SIRT1 activation may also
suppress angiotensin II type I receptor expression in VSMCs
contributing to the mechanism by preventing the increase of blood
pressure and vessel contraction (43).
Resveratrol, also known as a polyphenolic
SIRT1-activating compound, exhibits vasoprotective properties via
SIRT1 dependent pathways (13). The
exact mechanism of SIRT1 activation by the aforementioned
polyphenol remains unclear, however it is considered that
resveratrol activates SIRT1 indirectly (44,45). The
induction of AMPK by resveratrol appears to be a potential
mechanism of SIRT1 activation. AMPK affects the intracellular
AMP-to-ATP concentration ratio, which indirectly increases the
level of nicotinamide adenine dinucleotide (NAD+).
Increased NAD+ concentrations potentially increase SIRT1
activity, as NAD+ is substrate for the aforementioned
deacetylase (46). The results of
the present study indicate that 4-week resveratrol pretreatment
significantly increases the level of adiponectin in serum
(P<0.05). A shorter period of therapy (2 weeks) did not cause a
significant change in serum concentrations of adiponectin
(P>0.05). Induction of adiponectin expression by resveratrol was
also described in previous animal studies and Rivera et al
(26) obtained comparable results.
In their study, 8 weeks of 10 mg/kg resveratrol pretreatment daily
caused an increase in the adiponectin serum concentration in obese
Zucker rats, although this increase was not observed in lean
heterozygous littermates (22).
Beaudoin et al (47)
demonstrated that 6 weeks of high-dose resveratrol administration
(200 mg/kg daily) increases the adiponectin concentration and its
release from adipose tissue in Zucker rats. Gómez-Zorita et
al (48) demonstrated similar
results to Beaudoin et al (47) following 6 weeks of 15 mg/kg
resveratrol administration daily. By contrast, Palsamy and
Subramanian (49) did not observe a
significant increase of plasma adiponectin levels following 30 days
of low-dose resveratrol treatment (5 mg/kg) in a healthy population
of Wistar rats. However, an increase was observed in a diabetic
population of Wistar rats (49).
The molecular mechanisms of adiponectin involvement
in the process of atherogenesis are not fully elucidated.
Adiponectin inhibits atherogenesis by suppressing the nuclear
translocation of NF-κB lowering the endothelial synthesis of
pro-inflammatory chemokine IL-8 (7).
Additionally, adiponectin attenuates TNF-α-induced expression of
adhesion molecules on vascular endothelial cells, preventing
monocyte adhesion, the initial step of atherogenesis (16).
Resveratrol is considered to upregulate SIRT1, FoxO1
and adiponectin transcription via interconnecting gene modulation
pathways (50). Induction of
adiponectin may be dependent on a SIRT1-independent mechanism,
potentially mediated by downregulation of the
phosphoinositide-dependent kinase 1/protein kinase B signaling
pathway that leads to FoxO1 activation, or by activation of the
AMPK signaling pathway. Resveratrol upregulates adiponectin
indirectly by acting on the level of disulfide bond-A
oxidoreductase-like protein (23).
Resveratrol administration does not affect S100A8/A9
serum concentrations. Despite the anti-atherogenic properties of
resveratrol and the involvement of S100A8/A9 in the process of
atherosclerosis, results acquired in the present study indicate
that long-term administration of resveratrol in rat models does not
influence the S100A8/A9 serum concentration. Furthermore, to the
best of our knowledge, similar studies assessing the effect of
resveratrol administration on serum levels of S100A8/A9 have not
yet been completed.
S100A8/A9 is present in atherosclerotic plaques and
has been demonstrated to interact with a number of cell types
involved in the atherosclerosis (23). S100A8/A9 acts as a ligand of
proatherogenic receptors including TLR-4 and receptors for advanced
glycation end products (8,9). In human microvascular endothelial
cells, S100A8/A9 induces a specific inflammatory response through
an increased transcription of pro-inflammatory IL-8 and chemokine
(C-X-C motif) ligand 1 and the decrease of endothelial permeability
(19). S100A8/A9 promotes the
binding of inflammatory cells to the vascular endothelium through
the upregulation of adhesion molecules VCAM-1 and ICAM-1 and
increase of CD11b-CD18 binding capacity of leukocytes to
endothelial ICAM-1 (51).
Resveratrol inhibits the activation of NF-κB,
interferon regulatory factor 3 and activator protein 1 (AP-1) by
suppressing the adaptor protein toll
receptor-domain-containing-adaptor-inducing interferon-beta and
TANK-binding kinase (52). AP-1 is
potentially required for transcription of S100A8 and S100A9,
containing common binding sites for transcription factors, such as
AP-1 and CCAAT-enhancer-binding proteins (53). Taken together, resveratrol, via
inhibition of AP-1, may have an inhibitory effect on the expression
of S100A8 and S100A9; however, this was not confirmed by the
decrease in serum concentrations. In conclusion, resveratrol
presents the ability to interact with modulators of NF-κB and TLR-4
that are involved in the atherogenesis (53). The results of the current trial
suggest that long-term resveratrol administration may improve the
atherosclerosis. Nonetheless, pre-clinical trials need to be
followed by long-term human studies to confirm the anti-atherogenic
properties of resveratrol.
Acknowledgements
The present study was funded from a statutory grant
(grant no. 632) from the Department of Pharmacology and
Therapeutics, Faculty of Medicine, Collegium Medicum in Bydgoszcz,
Nicolaus Copernicus University, Toruń, Poland.
References
|
1
|
Libby P: Inflammation in atherosclerosis.
Arterioscler Thromb Vasc Biol. 32:2045–2051. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hansson GK and Hermansson A: The immune
system in atherosclerosis. Nat Immunol. 12:204–212. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Shimada K, Miyazaki T and Daida H:
Adiponectin and atherosclerotic disease. Clin Chim Acta. 344:1–12.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lima Freitas LC, Braga VA, do Socorro de
França Silva M, Cruz JC, Sousa Santos SH, de Oliveira Monteiro MM
and Balarini CM: Adipokines, diabetes and atherosclerosis: An
inflammatory association. Front Physiol. 6:3042015.PubMed/NCBI
|
|
5
|
Wang X, Chen Q, Pu H, Wei Q, Duan M, Zhang
C, Jiang T, Shou X, Zhang J and Yang Y: Adiponectin improves
NF-κB-mediated inflammation and abates atherosclerosis progression
in apolipoprotein E-deficient mice. Lipids Health Dis. 15:332016.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Chen YX, Zhang M, Cai Y, Zhao Q and Dai W:
The Sirt1 activator SRT1720 attenuates angiotensin II-induced
atherosclerosis in apoE-/− mice through inhibiting vascular
inflammatory response. Biochem Biophys Res Commun. 465:732–738.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kobashi C, Urakaze M, Kishida M, Kibayashi
E, Kobayashi H, Kihara S, Funahashi T, Takata M, Temaru R, Sato A,
et al: Adiponectin inhibits endothelial synthesis of interleukin-8.
Circ Res. 97:1245–1252. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Michelsen KS, Wong MH, Shah PK, Zhang W,
Yano J, Doherty TM, Akira S, Rajavashisth TB and Arditi M: Lack of
Toll-like receptor 4 or myeloid differentiation factor 88 reduces
atherosclerosis and alters plaque phenotype in mice deficient in
apolipoprotein E. Proc Natl Acad Sci USA. 101:10679–10684. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gebhardt C, Németh J, Angel P and Hess J:
S100A8 and S100A9 in inflammation and cancer. Biochem Pharmacol.
72:1622–1631. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Schiopu A and Cotoi OS: S100A8 and S100A9:
DAMPs at the crossroads between innate immunity, traditional risk
factors, and cardiovascular disease. Mediators Inflamm.
2013:8283542013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Altwegg LA, Neidhart M, Hersberger M,
Müller S, Eberli FR, Corti R, Roffi M, Sütsch G, Gay S, von
Eckardstein A, et al: Myeloid-related protein 8/14 complex is
released by monocytes and granulocytes at the site of coronary
occlusion: A novel, early, and sensitive marker of acute coronary
syndromes. Eur Heart J. 28:941–948. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ota H, Eto M, Ogawa S, Iijima K, Akishita
M and Ouchi Y: SIRT1/eNOS axis as a potential target against
vascular senescence, dysfunction and atherosclerosis. J Atheroscler
Thromb. 17:431–435. 2010. View
Article : Google Scholar : PubMed/NCBI
|
|
13
|
Brandes RP: Activating SIRT1: A new
strategy to prevent atherosclerosis? Cardiovasc Res. 80:163–164.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhang QJ, Wang Z, Chen HZ, Zhou S, Zheng
W, Liu G, Wei YS, Cai H, Liu DP and Liang CC: Endothelium-specific
overexpression of class III deacetylase SIRT1 decreases
atherosclerosis in apolipoprotein E-deficient mice. Cardiovasc Res.
80:191–199. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Okauchi Y, Kishida K, Funahashi T, Noguchi
M, Ogawa T, Ryo M, Okita K, Iwahashi H, Imagawa A, Nakamura T, et
al: Changes in serum adiponectin concentrations correlate with
changes in BMI, waist circumference, and estimated visceral fat
area in middle-aged general population. Diabetes Care. 32:e1222009.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lim S, Quon MJ and Koh KK: Modulation of
adiponectin as a potential therapeutic strategy. Atherosclerosis.
233:721–728. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Korndörfer IP, Brueckner F and Skerra A:
The crystal structure of the human (S100A8/S100A9)2 heterotetramer,
calprotectin, illustrates how conformational changes of interacting
alpha-helices can determine specific association of two EF-hand
proteins. J Mol Biol. 370:887–898. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Donato R: Intracellular and extracellular
roles of S100 proteins. Microsc Res Tech. 60:540–551. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Viemann D, Strey A, Janning A, Jurk K,
Klimmek K, Vogl T, Hirono K, Ichida F, Foell D, Kehrel B, et al:
Myeloid-related proteins 8 and 14 induce a specific inflammatory
response in human microvascular endothelial cells. Blood.
105:2955–2962. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Alexander RW: Theodore Cooper Memorial
Lecture. Hypertension and the pathogenesis of atherosclerosis.
Oxidative stress and the mediation of arterial inflammatory
response: A new perspective. Hypertension. 25:155–161. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bomfim GF, Dos Santos RA, Oliveira MA,
Giachini FR, Akamine EH, Tostes RC, Fortes ZB, Webb RC and Carvalho
MH: Toll-like receptor 4 contributes to blood pressure regulation
and vascular contraction in spontaneously hypertensive rats. Clin
Sci (Lond). 122:535–543. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Doyle AE and Fraser JR: Vascular
reactivity in hypertension. Circ Res. 9:755–761. 1961. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Wang A, Liu M, Liu X, Dong LQ, Glickman
RD, Slaga TJ, Zhou Z and Liu F: Up-regulation of adiponectin by
resveratrol: The essential roles of the Akt/FOXO1 and AMP-activated
protein kinase signaling pathways and DsbA-L. J Biol Chem.
286:60–66. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kao CL, Chen LK, Chang YL, Yung MC, Hsu
CC, Chen YC, Lo WL, Chen SJ, Ku HH and Hwang SJ: Resveratrol
protects human endothelium from H(2)O(2)-induced oxidative stress
and senescence via SirT1 activation. J Atheroscler Thromb.
17:970–979. 2010. View
Article : Google Scholar : PubMed/NCBI
|
|
25
|
Grześk G, Kozinski M, Tantry US, Wicinski
M, Fabiszak T, Navarese EP, Grzesk E, Jeong YH, Gurbel PA and
Kubica J: High-dose, but not low-dose, aspirin impairs
anticontractile effect of ticagrelor following ADP stimulation in
rat tail artery smooth muscle cells. Biomed Res Int.
2013:9282712013. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Rivera L, Morón R, Zarzuelo A and Galisteo
M: Long-term resveratrol administration reduces metabolic
disturbances and lowers blood pressure in obese Zucker rats.
Biochem Pharmacol. 77:1053–1063. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Grześk G, Wiciński M, Malinowski B, Grześk
E, Manysiak S, Odrowąż-Sypniewska G, Darvish N and Bierwagen M:
Calcium blockers inhibit cyclosporine A-induced hyperreactivity of
vascular smooth muscle cells. Mol Med Rep. 5:1469–1474.
2012.PubMed/NCBI
|
|
28
|
Itoh H and Hidaka H: Direct interaction of
calmodulin antagonists with Ca2+/calmodulin-dependent cyclic
nucleotide phosphodiesterase. J Biochem. 96:1721–1726. 1984.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Grześk E, Malinowski B, Wiciński M,
Szadujkis-Szadurska K, Sinjab TA, Manysiak S, Tejza B, Słupski M,
Odrowąż-Sypniewska G and Grześk G: Cyclosporine-A, but not
tacrolimus significantly increases reactivity of vascular smooth
muscle cells. Pharmacol Rep. 68:201–205. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Grześk E, Szadujkis-Szadurska K, Wiciński
M, Malinowski B, Sinjab TA, Tejza B, Pujanek M, Janiszewska E,
Kopczyńska A and Grześk G: Effect of
2,4,6-trimethyl-N-[3-(trifluoromethyl)phenyl]benzene-sulfonamide on
calcium influx in three contraction models. Biomedical Rep.
4:117–121. 2016.
|
|
31
|
Gupta SC, Tyagi AK, Deshmukh-Taskar P,
Hinojosa M, Prasad S and Aggarwal BB: Downregulation of tumor
necrosis factor and other proinflammatory biomarkers by
polyphenols. Arch Biochem Biophys. 559:91–99. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Tomé-Carneiro J, Gonzálvez M, Larrosa M,
Yáñez-Gascón MJ, García-Almagro FJ, Ruiz-Ros JA, Tomás-Barberán FA,
García-Conesa MT and Espín JC: Resveratrol in primary and secondary
prevention of cardiovascular disease: A dietary and clinical
perspective. Ann N Y Acad Sci. 1290:37–51. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Tomé-Carneiro J, Gonzálvez M, Larrosa M,
Yáñez-Gascón MJ, García-Almagro FJ, Ruiz-Ros JA, Tomás-Barberán FA,
García-Conesa MT and Espín JC: Grape resveratrol increases serum
adiponectin and downregulates inflammatory genes in peripheral
blood mononuclear cells: A triple-blind, placebo-controlled,
one-year clinical trial in patients with stable coronary artery
disease. Cardiovasc Drugs Ther. 27:37–48. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Militaru C, Donoiu I, Craciun A, Scorei
ID, Bulearca AM and Scorei RI: Oral resveratrol and calcium
fructoborate supplementation in subjects with stable angina
pectoris: Effects on lipid profiles, inflammation markers and
quality of life. Nutrition. 29:178–183. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Park SJ, Ahmad F, Philp A, Baar K,
Williams T, Luo H, Ke H, Rehmann H, Taussig R, Brown AL, et al:
Resveratrol ameliorates aging-related metabolic phenotypes by
inhibiting cAMP phosphodiesterases. Cell. 148:421–433. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Kline LW and Karpinski E: The
Resveratrol-induced Relaxation of Cholecystokinin Octapeptide- or
KCl-induced Tension in Male Guinea Pig Gallbladder Strips Is
Mediated Through L-type Ca2+Channels. J Neurogastroenterol Motil.
21:62–68. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Evgenov OV, Busch CJ, Evgenov NV, Liu R,
Petersen B, Falkowski GE, Petho B, Vas A, Bloch KD, Zapol WM and
Ichinose F: Inhibition of phosphodiesterase 1 augments the
pulmonary vasodilator response to inhaled nitric oxide in awake
lambs with acute pulmonary hypertension. Am J Physiol Lung Cell Mol
Physiol. 290:L723–L729. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Giachini FR, Lima VV, Carneiro FS, Tostes
RC and Webb RC: Decreased cGMP level contributes to increased
contraction in arteries from hypertensive rats: Role of
phosphodiesterase 1. Hypertension. 57:655–663. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Rybalkin SD, Rybalkina I, Beavo JA and
Bornfeldt KE: Cyclic nucleotide phosphodiesterase 1C promotes human
arterial smooth muscle cell proliferation. Circ Res. 90:151–157.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Bischoff E: Potency, selectivity, and
consequences of nonselectivity of PDE inhibition. Int J Impot Res.
16:(Suppl 1). S11–S14. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Thompson AM, Martin KA and Rzucidlo EM:
Resveratrol induces vascular smooth muscle cell differentiation
through stimulation of SirT1 and AMPK. PLoS One. 9:e854952014.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Stein S, Schäfer N, Breitenstein A, Besler
C, Winnik S, Lohmann C, Heinrich K, Brokopp CE, Handschin C,
Landmesser U, et al: SIRT1 reduces endothelial activation without
affecting vascular function in ApoE-/− mice. Aging (Albany NY).
2:353–360. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Miyazaki R, Ichiki T, Hashimoto T, Inanaga
K, Imayama I, Sadoshima J and Sunagawa K: SIRT1, a longevity gene,
downregulates angiotensin II type 1 receptor expression in vascular
smooth muscle cells. Arterioscler Thromb Vasc Biol. 28:1263–1239.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Higashida K, Kim SH, Jung SR, Asaka M,
Holloszy JO and Han DH: Effects of resveratrol and SIRT1 on PGC-1α
activity and mitochondrial biogenesis: A reevaluation. PLoS Biol.
11:e10016032013. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Li J, Feng L, Xing Y, Wang Y, Du L, Xu C,
Cao J, Wang Q, Fan S, Liu Q and Fan F: Radioprotective and
antioxidant effect of resveratrol in hippocampus by activating
Sirt1. Int J Mol Sci. 15:5928–5939. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Cantó C, Gerhart-Hines Z, Feige JN,
Lagouge M, Noriega L, Milne JC, Elliott PJ, Puigserver P and Auwerx
J: AMPK regulates energy expenditure by modulating NAD+ metabolism
and SIRT1 activity. Nature. 458:1056–1060. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Beaudoin MS, Snook LA, Arkell AM, Simpson
JA, Holloway GP and Wright DC: Resveratrol supplementation improves
white adipose tissue function in a depot-specific manner in Zucker
diabetic fatty rats. Am J Physiol Regul Integr Comp Physiol.
305:R542–R551. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Gómez-Zorita S, Fernández-Quintela A, Lasa
A, Hijona E, Bujanda L and Portillo MP: Effects of resveratrol on
obesity-related inflammation markers in adipose tissue of
genetically obese rats. Nutrition. 29:1374–1380. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Palsamy P and Subramanian S: Resveratrol
protects diabetic kidney by attenuating hyperglycemia-mediated
oxidative stress and renal inflammatory cytokines via Nrf2-Keap1
signaling. Biochim Biophys Acta. 1812:719–731. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Cdos Costa S, Rohden F, Hammes TO, Margis
R, Bortolotto JW, Padoin AV, Mottin CC and Guaragna RM: Resveratrol
upregulated SIRT1, FOXO1, and adiponectin and downregulated
PPARγ1-3 mRNA expression in human visceral adipocytes. Obes Surg.
21:356–361. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Newton RA and Hogg N: The human S100
protein MRP-14 is a novel activator of the beta 2 integrin Mac-1 on
neutrophils. J Immunol. 160:1427–1435. 1998.PubMed/NCBI
|
|
52
|
Kim MH, Yoo DS, Lee SY, Byeon SE, Lee YG,
Min T, Rho HS, Rhee MH, Lee J and Cho JY: The TRIF/TBK1/IRF-3
activation pathway is the primary inhibitory target of resveratrol,
contributing to its broad-spectrum anti-inflammatory effects.
Pharmazie. 66:293–300. 2011.PubMed/NCBI
|
|
53
|
Sunahori K, Yamamura M, Yamana J, Takasugi
K, Kawashima M, Yamamoto H, Chazin WJ, Nakatani Y, Yui S and Makino
H: The S100A8/A9 heterodimer amplifies proinflammatory cytokine
production by macrophages via activation of nuclear factor kappa B
and p38 mitogen-activated protein kinase in rheumatoid arthritis.
Arthritis Res Ther. 8:R692006. View
Article : Google Scholar : PubMed/NCBI
|