Introduction
T/natural killer (NK)-cell neoplasms are rare,
highly aggressive, insensitive to chemotherapy, and show poor
prognosis and early relapse among lymphatic malignancies. They have
an association with Epstein-Barr virus (EBV) infection, and
EBV+ T/NK-cell neoplasms are particularly prevalent
among Asian and South American populations (1). T-cell and NK-cell neoplasms constitute
<10% of all non-Hodgkin lymphomas (NHLs) (2). The World Health Organization (WHO) 2008
classification of mature T-cell and NK-cell neoplasms includes
peripheral T-cell lymphomas not otherwise specified (PTCL-NOS),
extranodal NK/T lymphoma (ENKTL), and two newly listed EBV-positive
lymphoproliferative disorders (LPDs), namely systemic EBV-T-cell
lymphoproliferative disorders of childhood and
hydroa-vacciniforme-like lymphoma (3).
The overlapping expression or coexpression of
immunophenotypes in NK and T cells frequently confuses the
diagnosis. ENKTL can be divided into two subtypes: Nasal (76.1%)
and extra-nasal (23.9%) (4). The
therapeutic effects and prognosis of nasal ENKTL (median survival
time, 86.5 months) are better than those for extra-nasal ENKTL
(median survival time, 8.6 months) (4). Approximately 80% of nasal ENKTL
presents as a localized disease, whereas at ≥60% extra-nasal ENKTL
is detected at an advanced stage (5). A previous study showed that the
advanced disease presentation, highly aggressive clinical course
and poor prognosis of extra-nasal ENKTL are analogous to aggressive
NK-cell leukemia (ANKL) (6).
PTCL-NOS can be classified into heterogeneous categories; EBV has
been detected in ~40% of PTCL-NOS cases (3). EBV-associated T/NK-LPDs are associated
with several disorders and diseases, for example, chronic active
EBV infection, EBV-associated hemophagocytic lymphohistiocytosis
(EBV-HLH), hypersensitivity to mosquito bites, PTCL-NOS, ANKL and
ENKTL (nasal type) (7,8).
In the present study, EBV+ T/NK-cell
neoplasms such as ENKTL (extra-nasal), PTCL-NOS and EBV-LPDs
(monoclonal) (9), were selected for
investigation because they share similar clinical features and
immune phenotypes, being highly invasive with poor prognosis. Nasal
ENKTL was excluded from this study because its treatment and
prognosis differ markedly from the extra-nasal ENKTL (4). The aim was to determine the clinical
features, prognosis and relative risk factors, such as fever,
complete blood count (CBC), lactate dehydrogenase (LDH) and
immunophenotyping (CD5/CD20) of these neoplasms.
Materials and methods
Patients
A total of 42 inpatients with EBV+
T/NK-cell neoplasms from May 2005 to July 2015 in the Department of
Hematology of Xiangya Hospital of Central South University
(Changsha, China) were reviewed. Patients with primary
immunodeficiency, HIV infection, previous solid cancers and
lymphoma were excluded. In addition, patients with acute or recent
EBV infection were excluded. All included patients had
immunohistochemical results for CD5/CD20 and were detected to be
EBV-encoded RNA (EBER)-positive by in situ hybridization
(ISH). The study was approved by the Ethics Committee of the
Xiangya Hospital of Central South University.
Patient demographics and clinical
characteristics
A total of 42 cases were included, 20 males and 22
females (male to female ratio, 1:1.1). The median age was 38 years
(range, 15–80 years). The involved organs included the lymph nodes,
lymph organs and extranodal organs such as the skin, soft tissues,
digestive tract, liver, spleen and bone marrow or multiple organs.
The primary symptoms included fever, fatigue, emaciation,
lymphadenectasis, hepatosplenomegaly and local damage, among which
fever was the most common symptom. The staging of all diseases was
performed according to the Ann Arbor (AA) staging system (Table I).
 | Table I.Characteristics of EBV+
mature NK/T-cell neoplasms. |
Table I.
Characteristics of EBV+
mature NK/T-cell neoplasms.
|
Characteristics | No. (%) |
|---|
| Gender |
|
|
Male | 20 (48) |
|
Female | 22 (52) |
| Age (years) |
|
|
0–30 | 17 (41) |
|
31–60 | 19 (45) |
|
≥60 | 6 (14) |
| Involved
organs |
|
| LD | 10 (24) |
|
Extra-nodal organs | 9 (21) |
|
Multiple organs | 23 (55) |
| AA stage |
|
|
I/II | 18 (43) |
|
III/IV | 2 (57) |
| B symptoms |
|
|
Yes | 25 (60) |
| No | 17 (40) |
| Diagnosis |
|
|
EBV-LPDs | 16 (38) |
|
ENKTL | 8 (20) |
|
PTCL-NOS | 5 (12) |
|
ANKL | 4 (9.5) |
|
LGLL | 4 (9.5) |
|
EBV-PTLD | 2 (5) |
|
EATL | 3 (6) |
| IPI scores |
|
|
0–1 | 15 (36) |
|
2–3 | 19 (45) |
| 4 | 8 (19) |
| Fever |
|
|
Yes | 20 (48) |
| No | 22 (52) |
| CBC |
|
| N | 8 (19) |
| H | 18 (43) |
| P | 16 (38) |
| LDH |
|
|
High | 29 (69) |
|
Normal | 13 (31) |
| CD5a |
|
|
Negative | 12 (29) |
|
Positive | 29 (69) |
| CD20 |
|
|
Negative | 32 (76) |
|
Positive | 10 (24) |
| Prognoses |
|
|
Following | 10 (24) |
|
Mortality | 28 (66) |
|
Lost | 4 (10) |
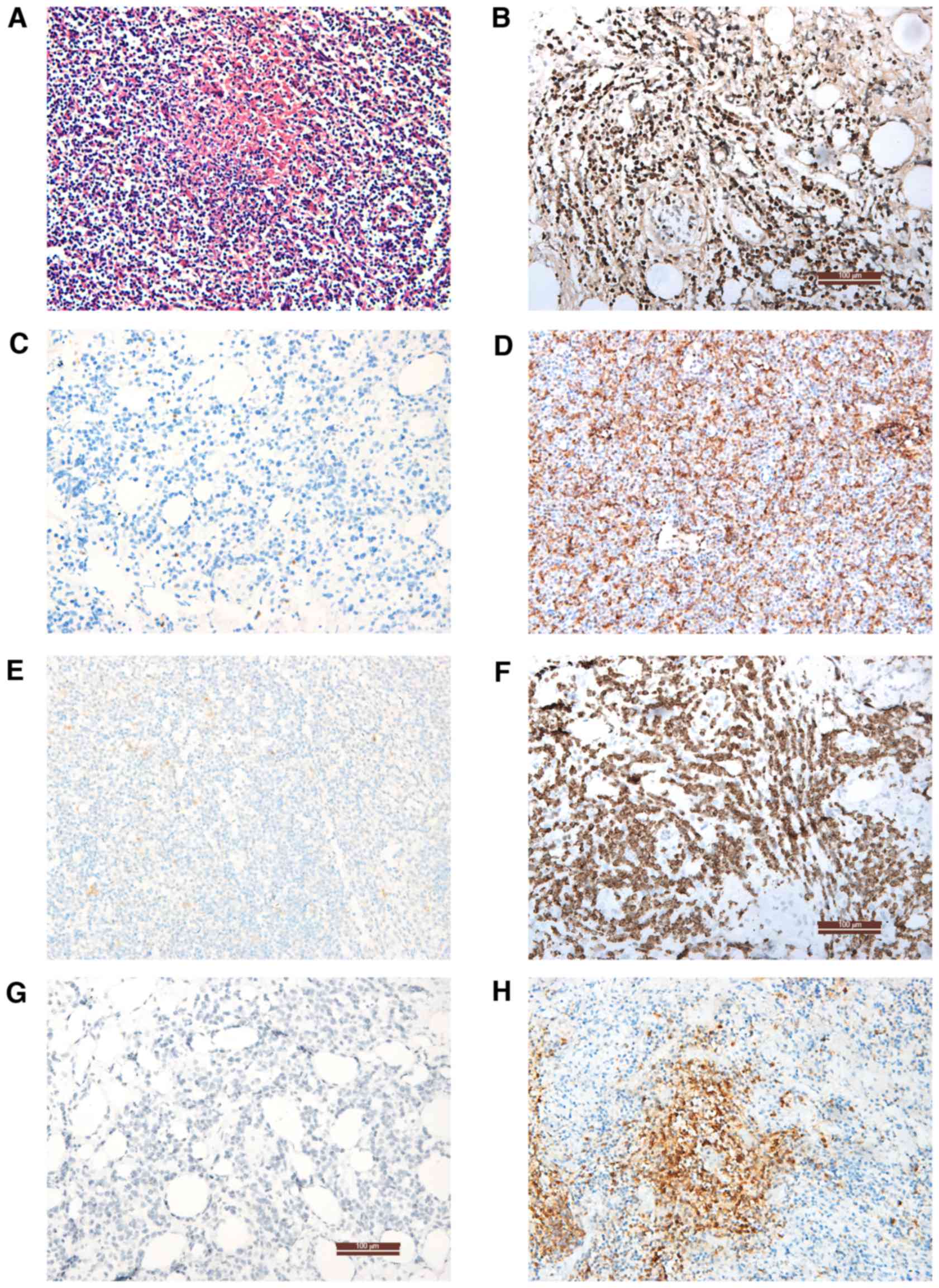
Auxiliary examinations
Computed tomography, ultrasound and positron
emission tomography-computed tomography were used to scan the whole
body, particularly the nasopharynx, neck, chest and abdomen, to
determine the lesion area and select it for biopsy and pathological
examination. When the T/NK-cell neoplasms involved the bone marrow,
bone marrow aspiration and biopsy were performed for morphological,
immunological, genetic and molecular biology analysis. The status
of CD3, CD3ε, CD5, CD56, CD79a, B-cell lymphoma (Bcl)-2, Bcl-6 and
CD20 were examined on paraffin sections (fixed with 4%
paraformaldehyde at 4°C for 24 h) using primary antibodies (cat.
nos. ZM-0417, TA506064, ZM-0280, ZM-0057, ZA-0293, ZM-0010 and
ZM-0011, respectively; 1:1,000; Origene Technologies, Inc.,
Rockville, MD, USA) at 4°C for 24 h. Samples were subsequently
incubated goat anti-rabbit IgG (GA1014) and goat anti-mouse IgG
(GA1004; both 1:4,000; both Boster Biological Technolog,
Pleasanton, CA, USA) secondary antibodies at 37°C for 30 min. The
results were observed using a light microscope. Representative
images of the analyses are shown in Fig.
1. EBER was tested by ISH in all cases as previously described
(10). Other observation indexes
included the CBC (Automatic Hematology Analyzer LH 780; Beckman
Coulter, Inc., Brea, CA, USA) and serum LDH (Reagent Kit for LDH
Test; Shanghai Zhicheng Biological Technology Co., Ltd., Shanghai
China), assays which were conducted according to the manufacturer's
protocol and were provided by the Clinical Laboratory of Xiangya
Hospital.
Diagnosis, treatment and
follow-up
The diseases were diagnosed on the basis of clinical
features and auxiliary examination results, and according to the
WHO classification (11) and NCCN
Guidelines (12). The disease degree
and prognosis were evaluated, and 3 years of follow-up were
completed. Patients were classified according to their
International Prognostic Index (IPI) scores from 0 to 5. IPI scores
were calculated based on the following variables: A (age ≥60 years
old), L (elevated serum LDH level above normal), P (ECOG
performance ≥2), S (AA stage ≥3) and E (extra-nodal sites ≥2)
(13). All patients received
pegaspargase-containing regimens, Patients of stage III/IV received
the modified SMILE protocol: Methotrexate (Pfizer Inc., New York,
NY, USA) 2 g/m2 on day 1, dexamethasone (Qilu
Pharmaceutical Co., Ltd., Jinan, China) 40 mg/day on days 2–4,
ifosfamide (Baxter Oncology GmbH, Frankfurt, Germany) 1.5
g/m2/day on days 2–4, etoposide (Qilu Pharmaceutical
Co., Ltd.) 100 mg/m2/day on days 2–4 and pegaspargase
(Jiangsu Hengrui Medicine Co., Ltd., Lianyungang China) 3,750 IU on
days and 14 at least for 6 cycles. Patients of stage stage I/II
were treated with the CHOP protocol combined with pegaspargase:
Cyclophosphamide (Baxter Oncology GmbH) 750 mg/m2 on day
1, adriamycin 40 mg/m2 on day 1, navelbine (Laboratoires
Pierre Fabre, Paris, France) 25 mg/m2 on day 1,
prednisone 60 mg/m2/day on days 1–5, pegaspargase
(Tianjin Lisheng Pharmaceutical Co., Ltd., Tianjin, China) 3,750 IU
on day 5 for 4 to 6 cycles (12,14).
Statistical analysis
Data were analyzed using SPSS 19.0 statistical
software (IBM SPSS, Armonk, NJ, USA). The χ2 test and
Fisher's exact probability test were used to compare frequencies.
One-way analysis of variance was used to test the measurement data.
The rank-sum test was applied to ranked data. Overall survival (OS)
and survival distributions were estimated by the Kaplan-Meier
method and Cox regression. All P-values are 2-tailed, and P<0.05
was considered to indicate a statistically significant result.
Results
Disease distribution according to age,
gender and involved organs
The patients were divided into three groups
according to age: 0–30 years, 31–60 years and >60 years. The
patients aged 0–60 years accounted for 86% of the total. The
frequency of males and females in the three groups exhibited
significant differences (P=0.036; Table
II). The morbidity of men in the 31–60 years group was
significantly higher compared with that in the other groups
(P=0.029). Patients were predominantly ≤60 years old, and in the
31–60 years group, there were more men than women. Of the 42 cases,
lymph node as the only involved organ was found in 10 (24%) cases,
and 23 (55%) cases had multi-organ involvement. The disease staging
results based on the AA staging system were as follows: Stage I,
n=6; stage II, n=12; stage III, n=4; and stage IV, n=20 (Table II).
| Table II.Numbers of males and females in the
three age groups. |
Table II.
Numbers of males and females in the
three age groups.
|
| Gender |
|
|---|
|
|
|
|
|---|
| Age (years) | Female | Male | P-value |
|---|
| 0~30 | 11 | 6 | 0.036 |
| 31–60 | 6 | 13 |
|
| 60+ | 5 | 1 |
|
Association between AA stage and
fever, LDH, CBC and immunophenotyping (CD5/CD20)
In the present study, 20 (48%) cases had fever
symptoms, of which 5 were stage I/II, and 15 cases were stage
III/IV. Of the remaining 22 cases, 13 were stage I/II and 9 were
stage III/IV. The difference in disease stage for patients with and
without fever was significant (P=0.024).
The 42 cases were divided into three groups based on
the CBC: 8 normal, 18 hemocytopenia and 16 pancytopenia. With
regard to the AA stage, 14 of the 16 pancytopenia patients were
stage III/IV, while only 3 of the 8 patients with a normal CBC were
stag III/IV, which was a significant difference (P=0.005).
The serum LDH level was elevated in 29 cases, 9 of
whom were stage I/II and 20 of whom were stage III/IV. The
remaining 13 cases included 9 of stage I/II and 4 of stage III/IV.
The frequency of elevated LDH in stage III/IV patients was higher
compared with that in stage I/II patients (P=0.020).
There were 10 cases positive for CD20 expression (B
cell line), of which 2 cases were stage I/II and 8 cases were stage
III/IV. The results revealed no significant difference in AA stage
between the CD20+ and CD20− groups (P=0.084).
Furthermore, there were 12 CD5− cases, 29
CD5+ cases and data was lost for one case. The ratio of
AA stage prevalence was found to be significantly different between
the CD5+ and CD5− groups (P=0.031; Tables I and III).
| Table III.Statistical analysis for various
factors according to IPI score and AA stage. |
Table III.
Statistical analysis for various
factors according to IPI score and AA stage.
|
| IPI score | AA stage |
|---|
|
|
|
|
|---|
| Items | (Mean ± SD) | P-value | I/II | III/IV | P-value |
|---|
| CBCa |
| 0.046 |
|
| 0.005 |
| N | 1.38±1.92 |
| 5 | 3 |
|
| H | 1.78±1.40 |
| 11 | 7 |
|
| P | 2.63±1.09 |
| 2 | 14 |
|
| LDH |
| 0.001 |
|
| 0.020 |
|
High | 2.48±1.24 |
| 9 | 20 |
|
|
Normal | 1.00±1.41 |
| 9 | 4 |
|
| Fever |
| 0.022 |
|
| 0.024 |
|
Yes | 2.55±1.10 |
| 5 | 15 |
|
| No | 1.55±1.60 |
| 13 | 9 |
|
| CD5 |
| 0.15 |
|
| 0.031 |
|
Positive | 1.86±1.51 |
| 15 | 14 |
|
|
Negative | 2.58±1.16 |
| 2 | 10 |
|
| CD20 |
| 0.95 |
|
| 0.084 |
|
Positive | 2.00±1.70 |
| 2 | 8 |
|
|
Negative | 2.03±1.40 |
| 16 | 16 |
|
Association of IPI scores with fever,
LDH, CBC and immunophenotyping (CD5/CD20)
The mean IPI scores were calculated in different
groups according to the factors fever, LDH, CBC and
immunophenotyping (CD5/CD20). The results demonstrated that the
mean IPI scores in patients with fever (P=0.022), increased LDH
levels (P=0.001) and pancytopenia (P=0.046) were higher compared
with those in patients no fever, a normal LDH level and normal CBC,
respectively. There was no significant difference in mean IPI score
in the CD20+/CD20−,
CD5+/CD5− and CBC groups (Tables I and III; Fig.
1).
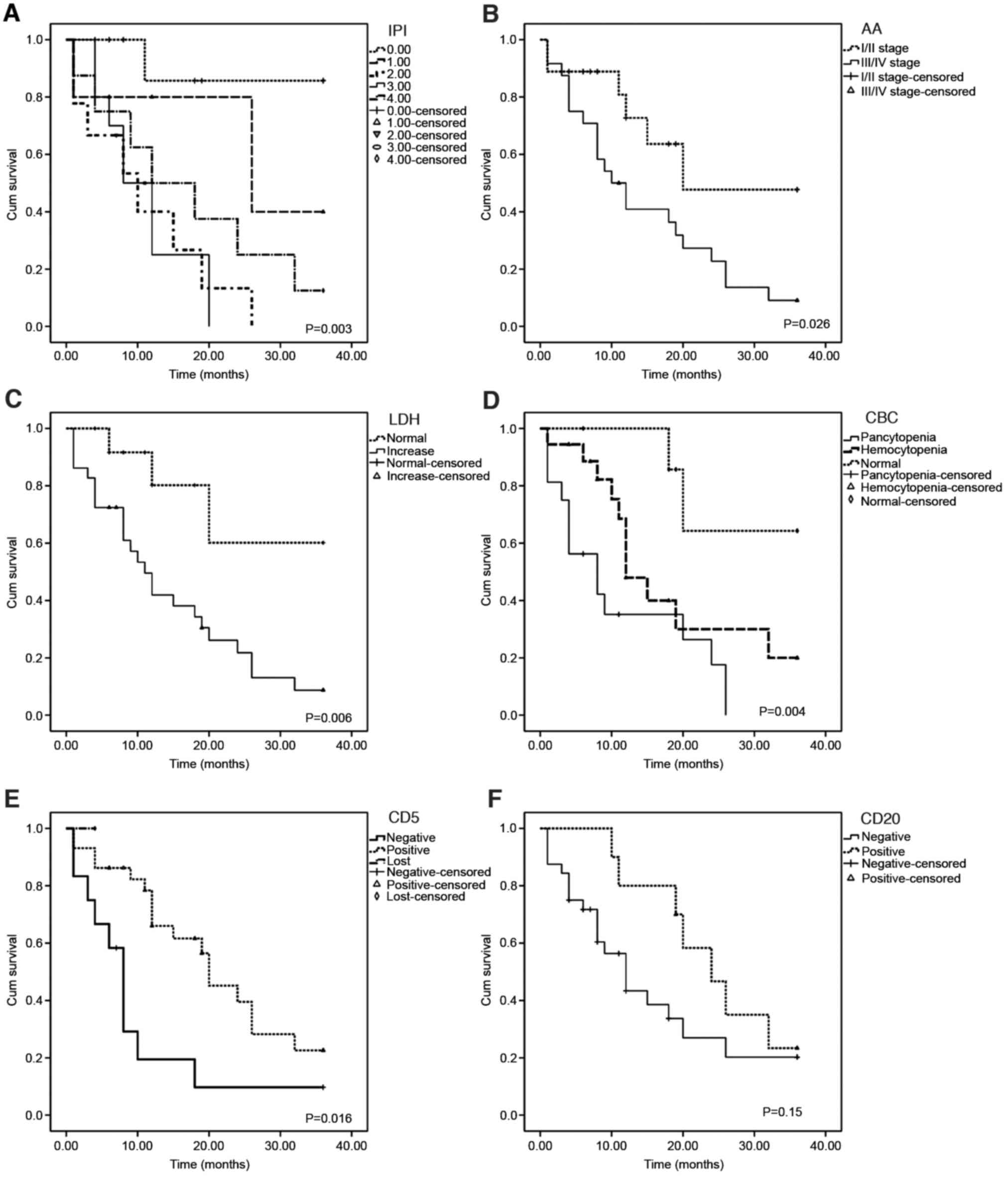
Association of various factors with OS
and mean survival time
The factors of gender, age, fever, LDH, CBC, AA
stage, immunophenotyping (CD5/CD20) and IPI scores in relation to
OS were analyzed using the Kaplan-Meier method. This analysis
revealed that the OS rate was correlated with CD5 expression, CBC,
LDH, AA stage and IPI score (Table
IV and Fig. 2). Cox regression
models were used to estimate the risk factors and adjust for
potential confounding factors. CD5− status (P=0.003),
pancytopenia (P=0.003) and IPI scores (P=0.017) were found to be
associated risk factors. In addition, statistical results indicated
a longer mean survival time in the CD5+,
CD20+ and CBC-N groups, and no significant difference
was identified in survival time between patients with increased and
normal LDH levels, or the groups with and without fever (Table IV).
| Table IV.Association of various factors with
overall survival and mean survival time. |
Table IV.
Association of various factors with
overall survival and mean survival time.
| A, Association with
overall survival |
|---|
|
|---|
| Factor | Overall survival
(χ2) | P-value |
|---|
| CD5 | 8.28 | 0.016 |
| CBC | 11.13 | 0.004 |
| LDH | 7.58 | 0.006 |
| CD20 | 2.07 | 0.150 |
| Gender | 1.098 | 0.295 |
| Fever | 1.318 | 0.251 |
| AA stage | 4.936 | 0.026 |
| Age groups | 1.934 | 0.380 |
| IPI scores | 15.68 | 0.003 |
|
| B, Association with
mean survival time |
|
| Factor | Survival time
(months, mean ± SD) | P-value |
|
| CD5(+/−) | 16.90±10.89 vs.
9.17±9.61 | 0.039 |
| CD20(+/−) | 23.30±9.32 vs.
11.59±10.04 | 0.002 |
| LDH
(high/normal) | 13.14±10.59 vs.
17.15±11.80 | 0.279 |
| CBC (N/H/P) | 23.63±11.13 vs.
14.39±10.16 vs. 9.75±9.07 | 0.011 |
Discussion
The clinical features of lymphoid neoplasms are
diverse, and typical manifestations or pathological characteristics
are lacking, which may delay diagnosis (15–18).
With the implementation of new genomic sequencing strategies, the
number of T/NK-cell lymphomas identified is likely to increase,
particularly that of EBV+ T/NK-cell neoplasms. The
molecular pathogenesis is difficult to understand due to their
complex and overlapping morphological and immunophenotypic
characteristics (1). Such lymphomas
have attracted an increasing amount of attention and consensus in
regard to treatment (6,7,14,19).
However, as of yet, there is no standard staging system.
In the present study, it was found that the most
common involved organ was the lymph node, followed by the skin and
tissues of the digestive tract and respiratory tract, which might
be associated with the routes of EBV infection and invasion.
Generally, primary infected B cells activate T cells and NK cells
to recognize infected B cells, which causes T/NK cell infection
during clearance (10,12,20–22).
More than half the cases in the present study had multiple organ
involvements, consistent with EBV+ T/NK-cell neoplasms
being highly aggressive and associated with poor prognosis. A
previous study indicated that the exact mechanism by which EBV
infects T/NK cells is associated with CD8+ T cells
(20). In a previous study of
lymphoma, the median age of all patients was ~50 years, and the
male/female ratio was nearly 2 (23). In the present study, EBV+
T/NK-cell neoplasms occurred at a younger median age (38 years),
occurring preferentially in middle-aged men and young women.
Fever, asthenia, anorexia and jaundice associated
with hepatosplenomegaly are the main clinical features of T/NK-cell
neoplasms (4,21). At present, malignancies are the most
common causes of fever of undetermined origin in adults (18–20,22). In
the present study, almost half the patients had fever, which is
possibly associated with inflammatory response syndrome induced by
cytokines such as interleukin (IL)-1β, IL-10, IL-13, IL-15 and
tumor necrosis factor (TNF) (24).
Previous studies have shown that the secretion of cytokines and
chemotactic factors results in increases in EBV-LPDs (25), EBV latent membrane protein 1 induces
Th1 factor secretion (e.g., TNF-α and interferon) via TNF
receptor-associated factor and NF-κB in lymphoepithelioid lymphoma
and T/NK LPDs, leading to cytokine storms, tissue damage and fever
(24–26).
In the present study, there was no significant
difference in IPI scores or AA stage between CD20+ and
CD20− patients; however, CD20 expression was found to be
associated with OS by Kaplan-Meier analysis, and the mean survival
time in CD20+ patients was longer than that in
CD20− patients. A previous report suggested that
CD20+ expression in EBV+ T/NK lymphoma
indicates a better prognosis (27).
Several studies concerning CD20+ or CD79a+
T/NK-cell lymphomas, or CD79a+CD20+ T-cell
lymphomas have been conducted (27–29).
CD20+ expression in T/NK lymphoma confused the
diagnosis. In the present study, one case with CD20+
expression was diagnosed among EBV-LPDs involving the B, T and NK
cell lines. It is possible that EBV-infected cells with dual
expression are progenitor cells. Novel methods may be useful for
diagnosis.
CD5− status has been suggested to be an
adverse prognostic factor (30), and
the downregulation of CD5 expression in EBV-HLH has been reported
to be associated with the serum levels of cytokines, and T cell
activation and proliferation (31).
In the present study, the IPI scores of CD5− patients
were clearly higher than those in CD5+ patients, and the
mean survival time of CD5− patients was shorter;
moreover, an association between CD5 expression and OS was
identified. Thus, CD5− status could be considered to
indicate poor prognosis and an aggressive clinical course for
targeting with molecular therapy, comparable to MYC and BCL2
(32).
LDH reflects not only the tumor burden but also the
host response. Increased LDH levels have been found to be
associated with aggressiveness, resistance to chemotherapy and poor
survival (33). Lu et al
(34) used LDH-5 as a criterion in
clinical trials for the stratification of patients with these
malignancies. The upregulation of LDH in cancer cells is associated
with the use of the glycolytic metabolism to meet energy
requirements and reduce dependence on oxygen via the tricarboxylic
acid cycle (35). LDH is regarded as
a significant prognostic factor in diffuse large B cell lymphoma
(36) and follicular lymphoma
(37). In the present study, an
increased LDH level indicated a low OS, which also indicates a poor
prognosis in patients with T/NK-cell neoplasms.
Lymphoid neoplasms are heterogeneous, and 15–63% of
them involve the bone marrow during the later period of the disease
(38). Thus, these neoplasms involve
the peripheral blood or bone marrow, resulting in hypocytosis or
pancytopenia. Abnormal CBCs were detected in 81% of patients in the
present study, of which pancytopenia accounted for 40% and was
associated with AA stage, IPI scores, OS and mean survival time,
indicating that it is a prognostic factor.
In previous studies on T/NK-cell lymphoma, in
patients who accepted chemotherapy alone, the 5-year OS rate of AA
stage I/II was only 13–35%. The majority of the patients who
achieved complete remission by chemotherapy experienced relapse
(39), although the recommended
asparaginase (ASP)-containing regimens showed prominent activity
against NK/T lymphoma (40,41). However, the efficacy of
ASP-containing chemotherapies in improving OS remains unclear due
to the lack of contemporaneous comparison. The high incidence of
primary drug resistance in ENKL or ANKL may be due to the high
expression of P-glycoprotein, a product of the multi-drug
resistance gene, on neoplastic cells (8,42). In
the present study, the 3-year OS was low (17%). The possible causes
are as follows: EBV+ T/NK-cell neoplasms are highly
aggressive, and ENKTL (nasal type) cases with comparatively better
prognoses were excluded. A total of 10 cases were in follow-up; 4
were lost during chemotherapy.
The statistical analysis results indicated that the
AA stage was an inferior factor with regard to OS and mean survival
time in the present study. The AA staging system was originally
designed for Hodgkin's lymphoma (21,43) and
was conventionally used for EBV+ T/NK-cell neoplasms
without considering the tumor size and invasion of contiguous
structures. It has been suggested that the IPI score is not a
perfect prognostic factor for NK/T lymphoma because of the lack of
blood cell counts (44). The
prognosis should be considered differently on the basis of
different disease categories, such as the involved extranodal
sites, LDH level, B symptoms, performance status, local tumor
invasiveness, regional lymph node metastasis and pretreatment
plasma EBV-DNA quantities (45)
representing tumor burden.
The definitions and terminology, particularly for
EBV+ T/NK-cell neoplasms in adults, remain
controversial. The diagnosis and treatment protocols are
complicated. Thus, it may be necessary to design an appropriate
staging system to effectively stratify tumor burden and survival
risk and thus guide treatment decisions. Fever and CBC may be
regarded as a complement to IPI scores and AA staging. The results
of the present study indicated an association of CD5 and CD20 with
prognosis. Efforts to identify pathological predictors of prognosis
and potential therapeutic targets in different categories are
recommended.
Acknowledgements
The authors thank American Journal Experts (Durham,
NS, USA) for English language editing. The authors are grateful to
the Pathology Department of Xiangya Hospital for kindly assisting
with immunohistochemistry experiment and to the Clinical Laboratory
of Xiangya Hospital for the assistance with CBC and LDH
examination.
References
|
1
|
Campo E, Swerdlow SH, Harris NL, Pileri S,
Stein H and Jaffe ES: The 2008 WHO classification of lymphoid
neoplasms and beyond: Evolving concepts and practical applications.
Blood. 117:5019–5032. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Vose J, Armitage J and Weisenburger D:
International T-Cell Lymphoma Project: International peripheral
T-cell and natural killer/T-cell lymphoma study: Pathology findings
and clinical outcomes. J Clin Oncol. 26:4124–4130. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mitrovic Z, Perry AM, Suzumiya J, Armitage
JO, Au WY, Coiffier B, Holte H, Jaffe ES, Monserrat E, Rajan SK, et
al: The prognostic significance of lymphopenia in peripheral T-cell
and natural killer/T-cell lymphomas: A study of 826 cases from the
International Peripheral T-cell Lymphoma Project. Am J Hematol.
87:790–794. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Jo JC, Yoon DH, Kim S, Lee BJ, Jang YJ,
Park CS, Huh J, Lee SW, Ryu JS and Suh C: Clinical features and
prognostic model for extranasal NK/T-cell lymphoma. Eur J Haematol.
89:103–110. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ko YH, Ree HJ, Kim WS, Choi WH, Moon WS
and Kim SW: Clinicopathologic and genotypic study of extranodal
nasal-type natural killer/T-cell lymphoma and natural killer
precursor lymphoma among Koreans. Cancer. 89:2106–2116. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Suzuki R: NK/T-cell lymphomas:
Pathobiology, prognosis and treatment paradigm. Curr Oncol Rep.
14:395–402. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kawa K: Epstein-Barr virus-associated
diseases in humans. Int J Hematol. 71:108–117. 2000.PubMed/NCBI
|
|
8
|
Oshimi K: Progress in understanding and
managing natural killer-cell malignancies. Br J Haematol.
139:532–544. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Park S and Ko YH: Epstein-Barr
virus-associated T/natural killer-cell lymphoproliferative
disorders. J Dermatol. 41:29–39. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Garady C, Saieg MA, Ko HM, Geddie WR,
Boerner SL and da Cunha Santos G: Epstein-Barr virus encoded RNA
detected by in situ hybridization using cytological preparations.
Cytopathology. 25:101–107. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Swerdlow SH, Campo E, Pileri SA, Harris
NL, Stein H, Siebert R, Advani R, Ghielmini M, Salles GA, Zelenetz
AD and Jaffe ES: The 2016 revision of the world health organization
classification of lymphoid neoplasms. Blood. 127:2375–2390. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zelenetz AD, Gordon LI, Wierda WG,
Abramson JS, Advani RH, Andreadis CB, Bartlett N, Bellam N, Byrd
JC, Czuczman MS, et al: Non-Hodgkin's lymphomas, version 2.2014. J
Natl Compr Canc Netw. 12:916–946. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
International Non-Hodgkin's Lymphoma
Prognostic Factors Project, . A predictive model for aggressive
Non-Hodgkin's lymphoma. N Engl J Med. 329:987–994. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kwong YL, Pang AW, Leung AY, Chim CS and
Tse E: Quantification of circulating Epstein-Barr virus DNA in
NK/T-cell lymphoma treated with the SMILE protocol: Diagnostic and
prognostic significance. Leukemia. 28:865–870. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hong J, Park S, Baek HL, Jung JH, Kang IG,
Sym SJ, Park J, Ahn JY, Cho EK, Kim ST, et al: Tumor cell nuclear
diameter and CD30 expression as potential prognostic parameter in
patients with extranodal NK/T-cell lymphoma, nasal type. Int J Clin
Exp Pathol. 5:939–947. 2012.PubMed/NCBI
|
|
16
|
Krenacs L, Smyth MJ, Bagdi E, Krenacs T,
Kopper L, Rudiger T, Zettl A, Muller-Hermelink HK, Jaffe ES and
Raffeld M: The serine protease granzyme M is preferentially
expressed in NK-cell, gamma delta T-cell, and intestinal T-cell
lymphomas: Evidence of origin from lymphocytes involved in innate
immunity. Blood. 101:3590–3593. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Taylor GS, Long HM, Brooks JM, Rickinson
AB and Hislop AD: The immunology of Epstein-Barr virus-induced
disease. Annu Rev Immunol. 33:787–821. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Bajor-Dattilo EB, Pittaluga S and Jaffe
ES: Pathobiology of T-cell and NK-cell lymphomas. Best Pract Res
Clin Haematol. 26:75–87. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Cai Q, Chen K and Young KH: Epstein-Barr
virus-positive T/NK-cell lymphoproliferative disorders. Exp Mol
Med. 47:e1332015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yuling H, Ruijing X, Li L, Xiang J, Rui Z,
Yujuan W, Lijun Z, Chunxian D, Xinti T, Wei X, et al: EBV-induced
human CD8+ NKT cells suppress tumorigenesis by EBV-associated
malignancies. Cancer Res. 69:7935–7944. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Wang RC, Chang ST, Hsieh YC, Huang WT, Hsu
JD, Tseng CE, Wang MC, Hwang WS, Wang J and Chuang SS: Spectrum of
Epstein-Barr virus-associated T-cell lymphoproliferative disorder
in adolescents and young adults in Taiwan. Int J Clin Exp Pathol.
7:2430–2437. 2014.PubMed/NCBI
|
|
22
|
Liaw CC, Chen JS, Wang CH, Chang HK and
Huang JS: Tumor fever in patients with nasopharyngeal carcinoma:
Clinical experience of 67 patients. Am J Clin Oncol. 21:422–425.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kim TM, Park YH, Lee SY, Kim JH, Kim DW,
Im SA, Kim TY, Kim CW, Heo DS, Bang YJ, et al: Local tumor
invasiveness is more predictive of survival than international
prognostic index in stage I(E)/II(E) extranodal NK/T-cell lymphoma,
nasal type. Blood. 106:3785–3790. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Mazodier K, Marin V, Novick D, Farnarier
C, Robitail S, Schleinitz N, Veit V, Paul P, Rubinstein M,
Dinarello CA, et al: Severe imbalance of IL-18/IL-18BP in patients
with secondary hemophagocytic syndrome. Blood. 106:3483–3489. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kimura H, Hoshino Y, Hara S, Sugaya N,
Kawada J, Shibata Y, Kojima S, Nagasaka T, Kuzushima K and
Morishima T: Differences between T cell-type and natural killer
cell-type chronic active Epstein-Barr virus infection. J Infect
Dis. 191:531–539. 2005. View
Article : Google Scholar : PubMed/NCBI
|
|
26
|
Chuang HC, Lay JD, Chuang SE, Hsieh WC,
Chang Y and Su IJ: Epstein-Barr virus (EBV) latent membrane
protein-1 down-regulates tumor necrosis factor-alpha (TNF-alpha)
receptor-1 and confers resistance to TNF-alpha-induced apoptosis in
T cells: Implication for the progression to T-cell lymphoma in
EBV-associated hemophagocytic syndrome. Am J Pathol. 170:1607–1617.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Jiang QP, Liu SY, Yang YX, Tan XX, Peng J,
Xiong ZT and Li Z: CD20-positive NK/T-cell lymphoma with indolent
clinical course: Report of case and review of literature. Diagn
Pathol. 7:1332012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Gill HS, Lau WH, Chan AC, Leung RY, Khong
PL, Leung AY and Kwong YL: CD20 expression in natural killer T cell
lymphoma. Histopathology. 57:157–159. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Huang YH, Huang CT, Tan SY and Chuang SS:
Primary gastric extranodal natural killer/T-cell lymphoma, nasal
type, with acquisition of CD20 expression in the subcutaneous
relapse: Report of a case with literature review. J Clin Pathol.
68:943–945. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Chuang WY, Chang H, Shih LY, Wang PN,
Chang YS, Lin TL, Hung YS, Yeh CJ, Ueng SH, Tang TC, et al: CD5
positivity is an independent adverse prognostic factor in elderly
patients with diffuse large B cell lymphoma. Virchows Arch.
467:571–582. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Wada T, Sakakibara Y, Nishimura R, Toma T,
Ueno Y, Horita S, Tanaka T, Nishi M, Kato K, Yasumi T, et al:
Down-regulation of CD5 expression on activated CD8+ T cells in
familial hemophagocytic lymphohistiocytosis with perforin gene
mutations. Hum Immunol. 74:1579–1585. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Karsan A, Gascoyne RD, Coupland RW,
Shepherd JD, Phillips GL and Horsman DE: Combination of t(14;18)
and a Burkitt's type translocation in B-cell malignancies. Leuk
Lymphoma. 10:433–441. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Adida C, Haioun C, Gaulard P, Lepage E,
Morel P, Briere J, Dombret H, Reyes F, Diebold J, Gisselbrecht C,
et al: Prognostic significance of survivin expression in diffuse
large B-cell lymphomas. Blood. 96:1921–1925. 2000.PubMed/NCBI
|
|
34
|
Lu R, Jiang M, Chen Z, Xu X, Hu H, Zhao X,
Gao X and Guo L: Lactate dehydrogenase 5 expression in Non-Hodgkin
lymphoma is associated with the induced hypoxia regulated protein
and poor prognosis. PLoS One. 8:e748532013. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Serganova I, Rizwan A, Ni X, Thakur SB,
Vider J, Russell J, Blasberg R and Koutcher JA: Metabolic imaging:
A link between lactate dehydrogenase A, lactate, and tumor
phenotype. Clin Cancer Res. 17:6250–6261. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Sehn LH, Berry B, Chhanabhai M, Fitzgerald
C, Gill K, Hoskins P, Klasa R, Savage KJ, Shenkier T, Sutherland J,
et al: The revised international prognostic index (R-IPI) is a
better predictor of outcome than the standard IPI for patients with
diffuse large B-cell lymphoma treated with R-CHOP. Blood.
109:1857–1861. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Buske C, Hoster E, Dreyling M, Hasford J,
Unterhalt M and Hiddemann W: The follicular lymphoma international
prognostic index (FLIPI) separates high-risk from intermediate- or
low-risk patients with advanced-stage follicular lymphoma treated
front-line with rituximab and the combination of cyclophosphamide,
doxorubicin, vincristine, and prednisone (R-CHOP) with respect to
treatment outcome. Blood. 108:1504–1508. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Tomita N, Taguri M, Hashimoto C, Takasaki
H, Fujimaki K, Motomura S, Koharazawa H, Takemura S, Fujita H,
Yamazaki E, et al: Evaluation of soluble interleukin-2 receptor and
serum lactate dehydrogenase in malignant lymphoma. Ann Hematol.
94:1935–1937. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Chauchet A, Michallet AS, Berger F,
Bedgedjian I, Deconinck E, Sebban C, Antal D, Orfeuvre H, Corront
B, Petrella T, et al: Complete remission after first-line
radio-chemotherapy as predictor of survival in extranodal NK/T cell
lymphoma. J Hematol Oncol. 5:272012. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Dearden CE, Johnson R, Pettengell R,
Devereux S, Cwynarski K, Whittaker S and McMillan A: British and
Committee for Standards in Haematology: Guidelines for the
management of mature T-cell and NK-cell neoplasms (excluding
cutaneous T-cell lymphoma). Br J Haematol. 153:451–485. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Zelenetz AD, Abramson JS, Advani RH,
Andreadis CB, Byrd JC, Czuczman MS, Fayad L, Forero A, Glenn MJ,
Gockerman JP, et al: NCCN clinical practice guidelines in oncology:
Non-Hodgkin's lymphomas. J Natl Compr Canc Netw. 8:288–334. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Kwong YL: Natural killer-cell
malignancies: Diagnosis and treatment. Leukemia. 19:2186–2194.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Cheung MM, Chan JK and Wong KF: Natural
killer cell neoplasms: A distinctive group of highly aggressive
lymphomas/leukemias. Semin Hematol. 40:221–232. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Federico M, Rudiger T, Bellei M, Nathwani
BN, Luminari S, Coiffier B, Harris NL, Jaffe ES, Pileri SA, Savage
KJ, et al: Clinicopathologic characteristics of angioimmunoblastic
T-Cell lymphoma: Analysis of the international peripheral T-cell
lymphoma project. J Clin Oncol. 31:240–246. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Wang ZY, Liu QF, Wang H, Jin J, Wang WH,
Wang SL, Song YW, Liu YP, Fang H, Ren H, et al: Clinical
implications of plasma Epstein-Barr virus DNA in early-stage
extranodal nasal-type NK/T-cell lymphoma patients receiving primary
radiotherapy. Blood. 120:2003–2010. 2012. View Article : Google Scholar : PubMed/NCBI
|