Introduction
It is estimated that ~400 million people worldwide
are chronically infected with hepatitis B virus (HBV) (1,2).
Patients with chronic hepatitis B (CHB) are at increased risk of
developing end-stage liver diseases, including liver cirrhosis,
liver failure and hepatocellular carcinoma (HCC) (3). Therefore, the goal of anti-HBV
treatment is to suppress HBV replication in a sustained manner, to
achieve hepatitis B e antigen (HBeAg) sero-conversion among
patients with CHB that are HBeAg sero-positive, and to the improve
quality of life and survival of patients by preventing progression
to end-stage liver disease (4).
The progression of chronic HBV infection has been
determined and divided into three phases, consisting of the immune
tolerant, immune clearance and residual or inactive phases. This
division is based on HBV DNA viral load, HBeAg and serum levels of
alanine aminotransferase (ALT) (4).
Patients with CHB in the immune tolerant phase are usually young
and HBeAg sero-positive with a high HBV DNA load, but have
persistently normal ALT levels (PNALT). During the immune clearance
phase, patients with CHB often exhibit elevated serum levels of
ALT, complicated by hepatic decompensation in certain cases
(5). ALT elevation is considered to
be the result of the host immune response against HBV-infected
hepatocytes (6). Higher ALT levels,
therefore, usually reflect more extensive hepatocyte damage due to
an increased immune response, which leads to liver fibrosis and
marked disease progression. Clinical CHB management guidelines
suggest that antiviral treatment should be commenced if patients
exhibit persistently elevated ALT levels, defined as >2 times
the upper limit of normal (ULN), for at least one month between
observations (4). For patients with
PNALT or persistently or intermittently mildly elevated ALT
(PIEALT), no drug treatments are recommended unless they exhibit
symptoms of advanced fibrosis or liver cirrhosis (5).
Monitoring the progress of liver fibrosis in
patients remains clinically challenging. Currently, liver biopsy is
the gold standard for evaluating liver fibrosis (7). However, liver biopsy has also been
criticized as it leads to sampling errors, underestimation of liver
fibrosis and potentially severe complications (8). It is also unrealistic to perform liver
biopsies on a large population. Therefore, it is important to
identify patients with CHB and PNALT at high risk of developing
liver fibrosis. However, the current predictors of liver fibrosis,
such as age, sex, serum ALT level and HBV DNA viral load, in
patients with CHB and PNALT or mildly elevated ALT are limited
(9,10).
In the present study, liver biopsies were performed
in patients with CHB and PNALT or PIEALT in order to explore the
predictors for liver fibrosis in patients with CHB and PNALT or
PIEALT.
Materials and methods
Patients
A total of 305 patients with CHB were analyzed in
the present study. The patients were treated and enrolled between
February 2011 and September 2015 in the Department of Medicine, The
Sixth People's Hospital of Qingdao (Qingdao, China). The
Institutional Review Board of the Sixth People's Hospital of
Qingdao approved the study and all patients provided written
informed consent prior to enrollment. Chronic HBV infection was
defined as sero-positive for hepatitis B surface antigen (HBsAg)
for ≥6 months (5). The inclusion
criteria were as follows: i) Diagnosis with chronic HBV infection
and ii) ALT values <80 IU/l on ≥3 separate occasions (≥1 month
between each observation). The exclusion criteria were as follows:
i) The presence of hepatitis C or D, or human immunodeficiency
virus co-infection; ii) medical evidence of liver disease due to
alternative etiology; iii) use of hepatotoxic drugs or heavy
alcohol consumption (>30 g/day) (11); iv) patient had already received
antiviral therapy or liver protectant reagents and v) ALT levels
detected <3 times prior to liver biopsy.
Patient evaluation
Patient information, including age, sex and body
mass index (BMI) was recorded. Serum HBV DNA viral load, serum HBV
markers and ALT levels were measured in all patients. Patients who
presented with liver fibrosis [liver stiffness (LS) >6.35 kPa]
underwent liver biopsy (9). ALT and
aspartate transaminase (AST) levels were determined using the
Olympus AU5400 biochemical analyzer (Olympus Corporation, Tokyo,
Japan). The ULN for ALT was 40 U/l. Patients were categorized as
PIEALT if they had ≥3 ALT values (≥1 month between each
observation) <80 IU/l, and ≥1 ALT value of >40 IU/l in the
previous 6 months. Patients were categorized as PNALT if they had
≥3 ALT values <40 IU/l over the previous 6 months.
Evaluation of HBV markers
HBsAg (cat no. 6C36-44), HBsAb (cat no. 7C18-25),
HBeAg (cat no. 6C32-25), HBeAb (cat no. 6C34-20) and HBcAb (cat no.
8L44-25) were detected using Abbott ELISA kits (Roche Molecular
Diagnostics, Pleasanton, CA, USA.).
Evaluation of serum HBV DNA
levels
Serum HBV DNA levels were measured by quantitative
polymerase chain reaction, using the Cobas Ampliprep/Cobas TaqMan,
version 2.0 (Roche Molecular Diagnostics), according to the
manufacturer's protocol. The manufacturer reports an HBV DNA linear
range of 20 to 1.7×108 IU/ml (1 IU/ml = 5.82 copies/ml)
(12).
Liver biopsy
Liver biopsy was performed using a 16-gauge Menghini
biopsy needle (Aspen Medical Europe, Ltd., Ashby-de-la-Zouch, UK).
For diagnosis, ≥20 mm liver tissue was obtained (13). All liver tissues were fixed at 4%
paraformaldehyde in 0.1 M phosphate buffer for 24 h and embedded in
paraffin wax. Then the paraffin-embedded sample were sliced into
4-µm sections and mounted onto glass slides. After dewaxing, the
slide was dipped into a Coplin jar containing Mayer's hematoxylin
and agitated for 30 sec. Then the slide was dipped into 1% eosin Y
solution for 10–30 sec with agitation. The sections were dehydrated
with two changes of 95% alcohol and two changes of 100% alcohol for
30 sec each. The alcohol was extracted with two washes of xylene.
Slides were observed under a light microscope. Liver fibrosis was
staged according to the METAVIR scoring system as follows: No
fibrosis (F0), mild fibrosis (portal fibrosis without septa, F1),
moderate fibrosis (portal fibrosis with few septa, F2), severe
fibrosis (numerous septa without cirrhosis, F3) or cirrhosis (F4).
The scores were determined by a liver pathologist without knowledge
of LS value (14). Liver fibrosis
was diagnosed when METAVIR score ≥F1 and advanced liver fibrosis
was diagnosed when METAVIR score ≥F2.
Evaluation of LS
Fibroscan, also known as transient elastography
(TE), was performed by three trained operators, following the
manufacturer's protocol. The operators used Fibroscan
(FibroScan® 502 Touch system; Echosens, Paris, France)
equipped with a standard probe. The procedure was performed as
previously described (15). A result
was considered reliable if: i) ≥10 successful shots of TE; ii) the
success rate was ≥60% and iii) the inter-quartile median ratio was
<30%. The results of TE are expressed in kPa.
Statistical analysis
The measurement units are expressed as the mean ±
standard deviation for normally distributed data and median (range)
for data with a non-normal distribution. Categorical data are
expressed as percentages. Univariate and multivariate analyses were
used to evaluate the predictors of liver fibrosis and advanced
liver fibrosis. The χ-squared test was applied to compare liver
fibrosis METAVIR scores. To determine the performance of ALT and
HBV DNA in predicting clinical outcomes, the area under the
receiver operating characteristic curve (AUROC) and logistic
regression were calculated. This was also performed for a combined
formulation of ALT and HBV DNA, according to the following formula:
−2.632 + (0.93 × ALT) + (0.258 × DNA)-(0.995 × sex) (male = 1,
female = 2). All analyses were performed using SPSS version 13.0
(SPSS, Inc., Chicago, IL, USA). P<0.05 was considered to
indicate a statistically significant difference.
Results
Demographics and clinical
characteristics
A total of 305 patients with CHB were included in
the current study (Table I). Of
these, there were 104 patients in the PNALT group with a mean age
of 33.48±9.31 years. There were 201 patients in the PIEALT group
with a mean age of 34.03±9.18 years. There were 49 (47.1%) and 104
males (51.7%) in the PNALT and PIEALT groups, respectively. There
were no significant differences between the sex and ages of the
patients in the two groups. However, HBV DNA viral load in the
PNALT group was significantly lower compared with the PIEALT group
(4.57±1.68 log10 vs. 5.71±1.69 log10 IU/ml;
P<0.001). BMI was significantly lower in the PNALT group
compared with the PIEALT group (21.44±2.53 vs. 23.06±3.65;
P<0.001). LS measured by TE was significantly higher in the
PIEALT group compared with the PNALT group (8.34±2.37 vs. 7.22±1.41
kPa; P<0.001).
 | Table I.Demographics and clinical
characteristics. |
Table I.
Demographics and clinical
characteristics.
| Characteristics | PNALT group
(n=104) | PIEALT group
(n=201) | P-values |
|---|
| Sex, male (%) | 49 (47.1) | 104 (51.7) | 0.444 |
| Age, years | 33.48±9.31 | 34.03±9.18 | 0.616 |
| HBeAg, positive
(%) | 41 (39.4) | 97 (48.3) | 0.142 |
| HBV DNA,
log10 IU/ml | 4.57±1.68 | 5.71±1.69 | <0.001 |
| BMI | 21.44±2.53 | 23.06±3.65 | <0.001 |
| LS, kPa | 7.22±1.41 | 8.34±2.37 | <0.001 |
Evaluation of the association between
sex, ALT levels and LS
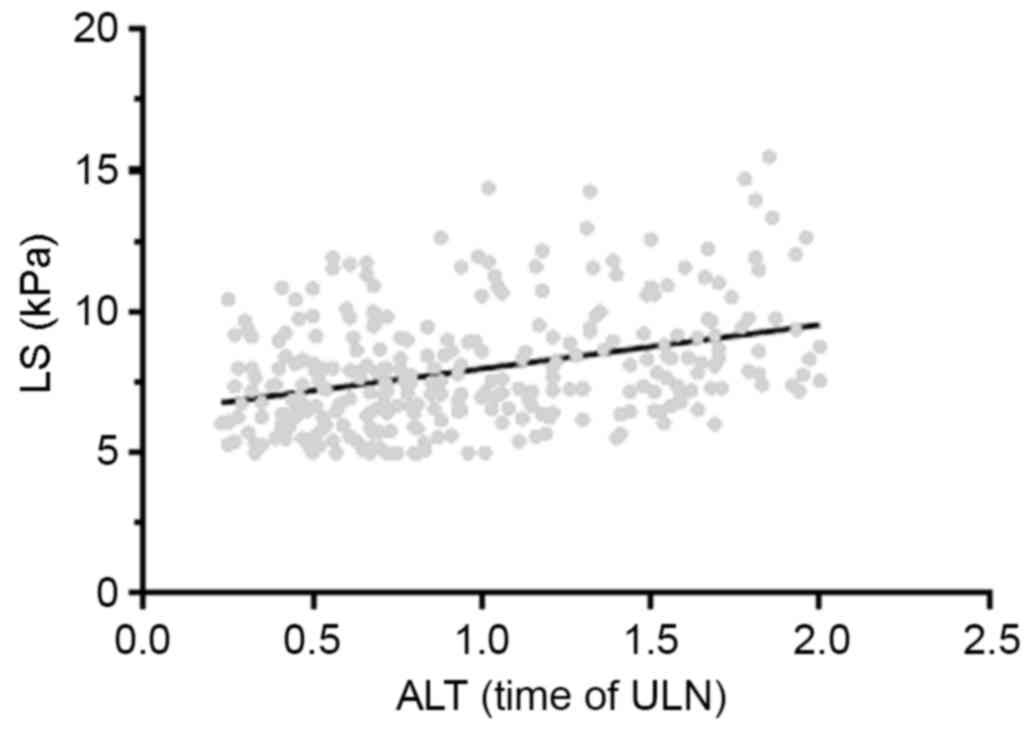
ALT levels in the 305 patients were positively
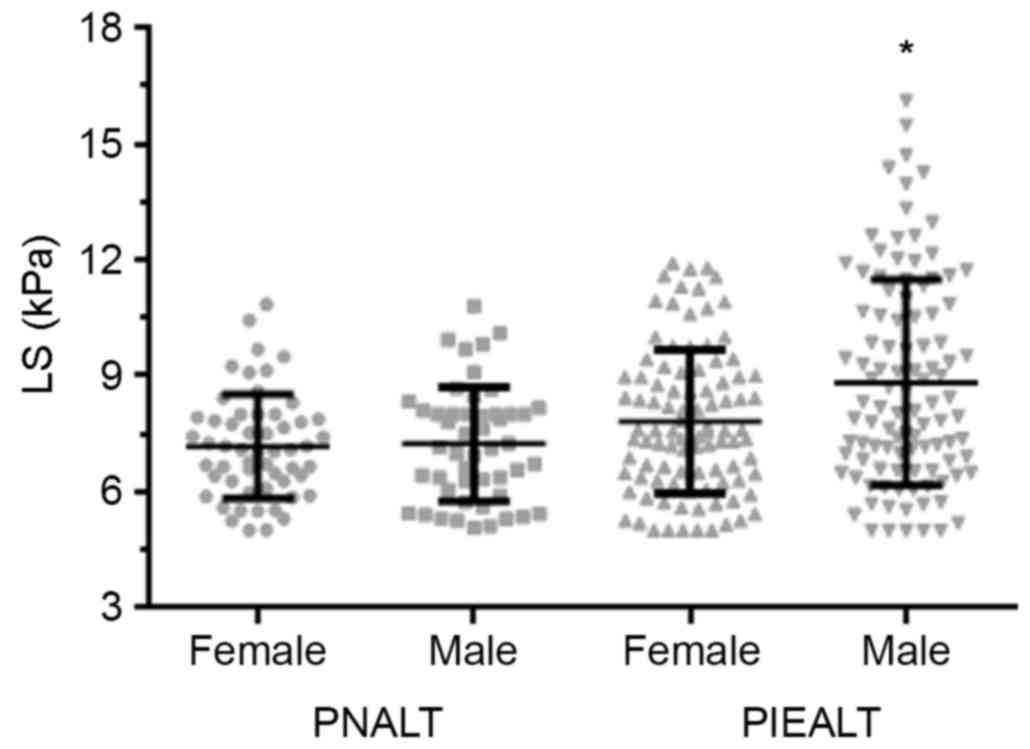
correlated with the LS value (r=0.34, P<0.001; Fig. 1). The association between sex and LS
was evaluated (Fig. 2). No
significant differences in LS values were observed between male and
females in the PNALT group (7.24±1.48 vs. 7.18±1.34 kPa). However,
in the PIEALT group, males exhibited a significantly higher LS
value compared with females (8.83±2.66 vs. 7.82±1.87 kPa;
P<0.01).
Analysis of predictors for liver
fibrosis among patients with PNALT and PIEALT
A total of 74 and 159 patients with LS >6.35 kPa
were identified in the PNALT and PIEALT groups, respectively. Liver
biopsy was performed in these patients. Among the 74 patients in
the PNALT group, 34 patients had a METAVIR fibrosis score of F0, 38
patients had a METAVIR score of F1 and 2 patients had a METAVIR
score of F2. Among the 159 patients with LS >6.35 kPa in the
PIEALT group, 39 patients had a METAVIR fibrosis score of ≥F2. A
total of 54.1% (40/74) and 72.3% (115/159) of patients with PNALT
or PIEALT had liver fibrosis (METAVIR score ≥F1), respectively. The
proportion of patients with liver fibrosis was significantly higher
in the PIEALT group compared with the PNALT group (P<0.001;
Table II).
| Table II.Proportion of patients with liver
fibrosis based on the METAVIR scoring system. |
Table II.
Proportion of patients with liver
fibrosis based on the METAVIR scoring system.
| Variable | PNALT group | PIEALT group | P-value |
|---|
| Liver biopsy,
n | 74 | 159 |
|
| Liver biopsy
result, n (%) |
|
| 0.001 |
| F0 | 34
(45.9) | 44 (27.7) |
|
| F1 | 38
(51.4) | 76 (47.8) |
|
| F2 | 2
(2.7) | 35 (22.0) |
|
| F3 | 0 (0) | 3 (1.9) |
|
| F4 | 0 (0) | 1 (0.6) |
|
| Liver stiffness,
(kPa) | 7.86±1.12 | 9.07±2.12 | <0.001 |
A multivariate logistic regression analysis was
performed for predictors of liver fibrosis (Table III) and advanced liver fibrosis
(Table IV). Among patients with
PNALT and PIEALT, high ALT levels was the only strong predictor for
liver fibrosis with an odds ratio (OR) of 2.69 (P=0.002) (Table III). However, male sex (P=0.007),
high ALT levels (P=0.029) and high HBV DNA load (P=0.005) were all
independent predictors for advanced liver fibrosis (Table IV).
| Table III.Univariate and multivariate logistic
regression analysis of predictors for liver fibrosis. |
Table III.
Univariate and multivariate logistic
regression analysis of predictors for liver fibrosis.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variable | OR | 95% CI | P-value | OR | 95% CI | P-value |
|---|
| Sex | 0.57 | 0.33–0.99 | 0.043 | 0.57 | 0.32–1.01 | 0.052 |
| Age (years) | 0.74 | 0.97–1.03 | 0.739 |
|
|
|
| ALT levels | 2.41 | 1.33–4.38 | 0.004 | 2.69 | 1.39–5.18 | 0.002 |
| HBV DNA | 1.12 | 0.97–1.31 | 0.134 |
|
|
|
| BMI | 1.04 | 0.95–1.13 | 0.392 |
|
|
|
| AST levels | 1.17 | 0.49–2.75 | 0.724 |
|
|
|
| HBeAg status | 0.63 | 0.36–1.10 | 0.105 |
|
|
|
| Table IV.Univariate and multivariate logistic
regression analysis of predictors for advanced liver fibrosis. |
Table IV.
Univariate and multivariate logistic
regression analysis of predictors for advanced liver fibrosis.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variable | OR | 95% CI | P-value | OR | 95% CI | P-value |
|---|
| Sex | 0.37 | 0.18–0.77 | 0.008 | 0.34 | 0.15–0.75 | 0.007 |
| Age (years) | 1.01 | 0.98–1.05 | 0.532 |
|
|
|
| ALT levels | 2.89 | 1.42–5.88 | 0.003 | 2.37 | 1.09–5.15 | 0.029 |
| HBV DNA | 1.35 | 1.09–1.66 | 0.004 | 1.39 | 1.11–1.75 | 0.005 |
| BMI | 1.06 | 0.96–1.18 | 0.237 |
|
|
|
| AST levels | 3.41 | 1.28–9.09 | 0.014 | 2.07 | 0.68–6.28 | 0.200 |
| HBeAg status | 0.86 | 0.44–1.69 | 0.670 |
|
|
|
Patients were further stratified according to HBeAg
status for regression analysis (Table
V). Among patients that were HBeAg positive, AST levels
(P=0.049), sex (P=0.009) and HBV DNA viral load (P=0.041) were
independent predictors for advanced liver fibrosis. Among patients
that were HBeAg negative, ALT levels (P=0.004) and HBV DNA
(P=0.050) were independent predictors for advanced liver
fibrosis.
| Table V.Univariate and multivariate logistic
regression analysis of predictors for advanced liver fibrosis in
patients with positive or negative HBeAg status. |
Table V.
Univariate and multivariate logistic
regression analysis of predictors for advanced liver fibrosis in
patients with positive or negative HBeAg status.
| A, HBeAg positive
patients (n=138) |
|---|
|
|---|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variables | OR | 95% CI | P-value | OR | 95% CI | P-value |
|---|
| Sex | 0.22 | 0.07–0.72 | 0.012 | 0.18 | 0.05–0.66 | 0.009 |
| Age (years) | 1.02 | 0.97–1.08 | 0.477 |
|
|
|
| ALT level | 1.11 | 0.41–2.99 | 0.846 |
|
|
|
| HBV DNA | 1.29 | 0.97–1.72 | 0.083 | 1.44 | 1.02–2.03 | 0.041 |
| BMI | 1.06 | 0.92–1.23 | 0.417 |
|
|
|
| AST levels | 6.55 | 1.44–29.84 | 0.015 | 5.31 | 1.01–27.97 | 0.049 |
|
| B, HBeAg
negative patients (n=167) |
|
|
| Univariate
analysis | Multivariate
analysis |
|
|
|
|
|
|
Variables | OR | 95% CI | P-value | OR | 95% CI | P-value |
|
| Sex | 0.55 | 0.21–1.42 | 0.217 |
|
|
|
| Age (years) | 1.01 | 0.95–1.06 | 0.893 |
|
|
|
| ALT levels | 7.91 | 2.61–24.05 | <0.001 | 5.42 | 1.74–16.910 | 0.004 |
| HBV DNA | 1.41 | 1.05–1.89 | 0.021 | 1.42 | 1.00–2.01 | 0.05 |
| BMI | 1.07 | 0.92–1.23 | 0.378 |
|
|
|
| AST levels | 2.06 | 0.55–7.71 | 0.284 |
|
|
|
Evaluation of suitable cut-off value
of ALT levels and HBV DNA load as predictors
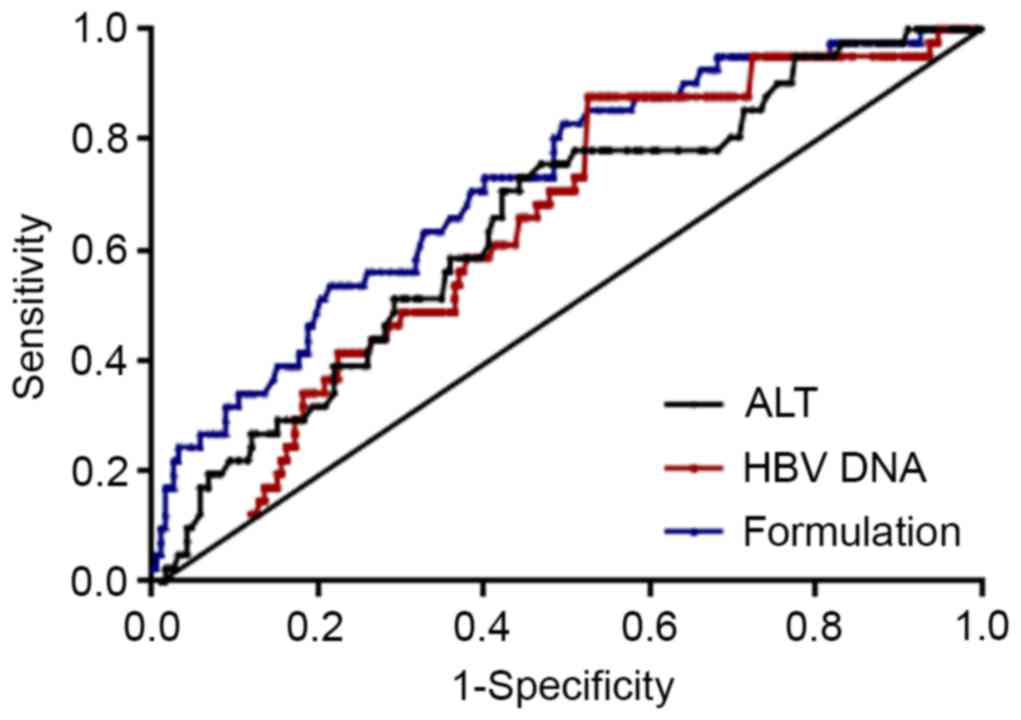
AUROC was used to examine the use of ALT levels and
HBV DNA load as indicators for advanced liver fibrosis (METAVIR
score F2-F4; Fig. 3). The AUROC was
0.65 (P=0.003) when using ALT levels to predict advanced liver
fibrosis. When an ALT level ≥0.88 ULN was set as a positive
indicator for advanced liver fibrosis, sensitivity and specificity
were 87.8 and 47.4%, respectively. The AUROC was 0.64 when HBV DNA
load was set as an indicator for advanced liver fibrosis (P=0.004).
If an HBV DNA value ≥4.99 log10 IU/ml was set as
positive for advanced liver fibrosis, the sensitivity and
specificity were 78.0 and 49.5%, respectively.
When ALT, HBV DNA load and sex were combined, a
formulation was obtained as follows: −2.632 + (0.93 × ALT) + (0.258
× DNA)-(0.995 × sex) (male=1, female=2). The formulation score was
well correlated with LS (r=0.33, P<0.001, data not shown). The
AUROC was 0.72 (P<0.001) when using the formulation score to
predict advanced liver fibrosis. When the formulation score was set
at >-2.22, the sensitivity and specificity to predict advanced
hepatic fibrosis were 61.5 and 70.7%, respectively (Fig. 3).
Discussion
The results of the present study demonstrate that
normal ALT levels do not always indicate the absence of advanced
liver fibrosis, although ALT and HBV DNA levels are independent
predictors of hepatic fibrosis in patients with CHB (16). The present data indicated that 54.1%
(40/74) and 72.3% (115/159) of patients with chronic HBV infection
with PNALT or PIEALT have liver fibrosis, respectively. These
results are notable as clinical guidelines recommend that patients
with liver fibrosis should not undergo treatment; consequently,
these patients are often ignored. ALT levels are commonly used to
assess liver inflammation and elevation of ALT is regarded as an
indicator for anti-HBV treatment (5). However serum ALT levels may vary due to
BMI, sex and metabolism disorder (8,17,18).
Therefore, ALT levels are an imperfect marker of the severity of
liver diseases. According to the results of the present study,
normal ALT levels do not indicate the absence of liver fibrosis in
patients with HBV infection. A combined analysis of ALT levels, sex
and serum HBV DNA load may more effectively identify high-risk
patients with HBV infection. To the best of our knowledge, the
study is the first to construct a formulation to identify advanced
hepatic fibrosis among this population. However, the use of this
formulation alone is not sufficient for clinical use. It would be
more practical to combine Fibroscan with the formulation score to
screen for liver fibrosis in patients with CHB.
Chronic HBV infection exacerbates liver fibrosis in
patients. Wang et al (19)
reported that interleukin (IL)-17 expression increased in
HBV-associated diseases, including CHB and post-hepatitis B liver
cirrhosis. Furthermore, there was a positive correlation between
IL-17 expression and the grade of liver fibrosis. Bai et al
(20) reported that HBV Dane
particles, × protein and c protein may induce hepatic stellate cell
proliferation via the platelet-derived growth factor (PDGF)-B/PDGF
receptor-β signaling pathway, which serves a key function in liver
fibrosis caused by HBV infection.
In order to determine the antiviral treatment
trigger point and improve survival rates, it is important to be
able to rapidly identify patients with CHB at risk of developing
fibrosis. Fagone et al (21)
performed a meta-analysis of two datasets from two different rodent
species and identified 254 and 132 genes that were significantly
upregulated and downregulated, respectively. These biomarkers may
provide novel pharmacological targets and be useful in assessing
the progression of CHB. Combined antiviral treatment and novel
therapeutic approaches may be effective at preventing end-stage
liver diseases, such as liver cirrhosis (22).
Another potential diagnostic method of assessing
liver fibrosis may be the analysis of circulating microRNAs
(miRNAs). miRNAs are short RNA sequences ~22 nucleotides long that
post-transcriptionally regulate gene expression. Zhang et al
(23) reported that a number of
miRNAs were differentially expressed in patients with CHB and liver
fibrosis. The miRNAs identified were involved in 100 signal
transduction pathways, the majority of which affected liver
fibrosis via the transforming growth factor-β/Smad, Wnt,
mitogen-activated protein kinase, Janus kinase/signal transducers
and activators of transcription and vascular endothelial growth
factor pathways. A study conducted by Lambrecht et al
(24) reported that miRNA-200b and
miRNA-122 were significantly upregulated during early liver
fibrosis and that miRNA-192, −92a and −150 were significantly
downregulated in patients with HBV. Zheng et al (25) identified that levels of serum
miR-125a-5p correlated with liver fibrosis and suggested that serum
miR-125a-5p may be used as a non-invasive biomarker to monitor the
progression of liver disease.
Previous studies have demonstrated that advanced
liver fibrosis is a precursor to end-stage liver diseases,
including HCC (26). Chronic HBV
infection with serum HBeAg-negative and serum HBV DNA-positive is
commonly encountered in clinical practice. A proportion of patients
with PNALT or PIEALT will develop advanced liver fibrosis (27) and it has been suggested that such
patients should be closely monitored with TE or liver biopsy
(28). Although liver biopsy is
still regarded as the gold standard for assessing liver fibrosis,
the invasive nature of the procedure results in complications
arising in 0.5% of cases and the mortality rate of liver biopsy is
~0.05%. Sampling error and inter-observer variability may also lead
to the understaging of cirrhosis (5). Therefore, it is important to develop
novel non-invasive methods for fibrosis detection. Fibroscan is a
non-invasive and reliable method of examining the degree of hepatic
fibrosis. Since its detection range is 100 times greater than that
of a liver biopsy, Fibroscan may more accurately reflect the degree
of liver fibrosis (29). However,
the diagnostic accuracy of Fibroscan may be affected by a number of
factors, including elevated ALT levels and high BMI values
(29). In addition, due to the
difficulty of operation, cost and lack of skilled operators,
Fibroscan is not yet widely used to determine LS. In the present
study, the progression of liver fibrosis in patients with PNALT or
PIEALT was evaluated according to sex, HBV DNA viral load and ALT
levels. It was indicated that male patients with ALT in normal high
levels (0.5 ULN≤ALT level<ULN) and high HBV DNA viral load are
at a higher risk of developing advanced liver fibrosis, suggesting
that liver biopsy should be considered for such patients.
In the present study, the proportion of patients
with liver fibrosis in the PIEALT group was significantly higher
compared with the PNALT group. ALT may be released into the
circulation when hepatocytes are damaged. ALT fluctuations in the
PIEALT group indicate that inflammation of the liver in these
patients is more severe compared with the PNALT group. Repeated
inflammatory activity in the liver will result in a more severe
degree of liver fibrosis (28). A
previous study with long-term follow-up indicated that patients
with elevated ALT have a higher mortality rate (30). According to the present study, liver
disease may progress in patients with PNALT, particularly those
with normal-high ALT levels. A new ALT ULN value (male, 30 U/l,
female, 19 U/l) has been proposed (31). Lin et al (32) reported that HBeAg-negative patients
with high-normal ALT and elevated HBV DNA levels were more likely
to experience adverse long-term outcomes. High-normal ALT was
considered to be associated with liver injury and the revised ULN
of ALT may be more suitable than the previous ULN (40 U/l) for
screening patients with CHB to determine disease progression. The
use of antiviral treatment and liver biopsy remains controversial
for patients with CHB that have ALT levels below the current
definition of ALT as <2× ULN but higher than the new ULN
definition.
In the present study, being male was identified as
one of the independent indicators of advanced liver fibrosis.
Similar results have been observed in the healthy population
(33). One hypothesis is that
ovarian hormones may reduce expression of types I and III
procollagen and inhibit deposition of hepatic collagen proteins,
thereby inhibiting development of fibrosis (34). According to the results of the
current study, sex should be taken into account when diagnosing
advanced hepatic fibrosis. The current results also highlight
concerns about the current guidelines that recommend using only
ALT, HBsAg and HBV DNA levels to define different phases of HBV
infection without performing liver biopsy (5). The current study suggests that patients
with chronic HBV infection, PNALT and high HBV DNA viral load may
progress to advanced liver disease. Further investigations are
required to design a novel method of defining the progression of
HBV infection.
Recently, Lemoine et al (35) reported that the
γ-glutamyl-transpeptidase to platelet ratio (GPR) was a novel serum
model able to accurately estimate advanced fibrosis and cirrhosis
among patients with CHB in West Africa. GPR has several beneficial
features, such as relatively high sensitivity and specificity,
compared with other noninvasive methods. However, as the authors
conclude, GPR requires further evaluation in other patient
populations. AST to platelet ratio index (APRI) and GPR have
previously been used to diagnose cirrhosis in patients with CHB
(8,36). However, the two parameters have
limitations, including a low level of sensitivity and positive
predictive value, and a lack of evidence in patients with CHB and
PNALT or PIEALT. In the present study, it was demonstrated that a
combination of ALT levels, sex and serum HBV DNA load may more
effectively identify patients with hepatitis at high risk of
developing fibrosis, compared with ALT levels or HBV DNA load
alone. The formulation has the advantage of only requiring
inexpensive laboratory tests that are available in primary care
centers; therefore it may be used to screen for liver fibrosis in
resource-limited areas.
One limitation of the current study is that the
results may be biased by the fact that all clinical data was
collected from one research center. However, the sample size of the
present study was sufficient to identify the predictors of liver
fibrosis among patients with CHB and PNALT or PIEALT. To further
validate the results, a prospective and multicenter study on a
larger scale is warranted.
In conclusion, normal ALT levels do not always
indicate the absence of hepatic fibrosis. A combination of ALT
levels, sex and serum HBV DNA load may more effectively identify
patients with CHB at high risk of developing fibrosis.
Glossary
Abbreviations
Abbreviations:
|
ALT
|
alanine aminotransferase
|
|
CHB
|
chronic hepatitis B
|
|
HCC
|
hepatocellular carcinoma
|
|
HBV
|
hepatitis B virus
|
|
LS
|
liver stiffness
|
|
TE
|
transient elastography
|
|
ULN
|
upper limit of normal
|
References
|
1
|
Clements CJ, Baoping Y, Crouch A, Hipgrave
D, Mansoor O, Nelson CB, Treleaven S, van Konkelenberg R and
Wiersma S: Progress in the control of hepatitis B infection in the
Western Pacific Region. Vaccine. 24:1975–1982. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Liaw YF: Antiviral therapy of chronic
hepatitis B: Opportunities and challenges in Asia. J Hepatol.
51:403–410. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ott JJ, Stevens GA, Groeger J and Wiersma
ST: Global epidemiology of hepatitis B virus infection: New
estimates of age-specific HBsAg seroprevalence and endemicity.
Vaccine. 30:2212–2219. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Liaw YF, Kao JH, Piratvisuth T, Chan HL,
Chien RN, Liu CJ, Gane E, Locarnini S, Lim SG, Han KH, et al:
Asian-Pacific consensus statement on the management of chronic
hepatitis B: A 2012 update. Hepatol Int. 6:531–561. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sarin SK, Kumar M, Lau GK, Abbas Z, Chan
HL, Chen CJ, Chen DS, Chen HL, Chen PJ, Chien RN, et al:
Asian-Pacific clinical practice guidelines on the management of
hepatitis B: A 2015 update. Hepatol Int. 10:1–98. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rukunuzzaman M and Karim MB: Chronic
hepatitis B in children - a review. Mymensingh Med J. 24:649–656.
2015.PubMed/NCBI
|
|
7
|
Bravo AA, Sheth SG and Chopra S: Liver
biopsy. N Engl J Med. 344:495–500. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Peng J, Cai S, Yu T, Chen Y, Zhu Y and Sun
J: Aspartate aminotransferase to platelet ratio index-a reliable
predictor of therapeutic efficacy and improvement of Ishak score in
chronic hepatitis B patients treated with nucleoside analogues.
Scand J Clin Lab Invest. 76:133–142. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Zeng J, Cai S, Liu J, Xue X, Wu X and
Zheng C: Dynamic changes in liver stiffness measured by transient
elastography predict clinical outcomes among patients with chronic
hepatitis B. J Ultrasound Med. 36:261–268. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cai S, Cao J, Yu T, Xia M and Peng J:
Effectiveness of entecavir or telbivudine therapy in patients with
chronic hepatitis B virus infection pre-treated with interferon
compared with de novo therapy with entecavir and telbivudine.
Medicine (Baltimore). 96:e70212017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
European Association for the Study of
Liver: EASL clinical practical guidelines: Management of alcoholic
liver disease. J Hepatol. 57:399–420. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Cai SH, Lv FF, Zhang YH, Jiang YG and Peng
J: Dynamic comparison between Daan real-time PCR and Cobas TaqMan
for quantification of HBV DNA levels in patients with CHB. BMC
Infect Dis. 14:852014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Castera L: Transient elastography and
other noninvasive tests to assess hepatic fibrosis in patients with
viral hepatitis. J Viral Hepat. 16:300–314. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Poynard T and Bedossa P: Age and platelet
count: A simple index for predicting the presence of histological
lesions in patients with antibodies to hepatitis C virus. METAVIR
and CLINIVIR Cooperative Study Groups. J Viral Hepat. 4:199–208.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sandrin L, Fourquet B, Hasquenoph JM, Yon
S, Fournier C, Mal F, Christidis C, Ziol M, Poulet B, Kazemi F, et
al: Transient elastography: A new noninvasive method for assessment
of hepatic fibrosis. Ultrasound Med Biol. 29:1705–1713. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cai S, Yu T, Jiang Y, Zhang Y, Lv F and
Peng J: Comparison of entecavir monotherapy and de novo lamivudine
and adefovir combination therapy in HBeAg-positive chronic
hepatitis B with high viral load: 48-week result. Clin Exp Med.
16:429–436. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sharaiha RZ, Kumta NA, Saumoy M, Desai AP,
Sarkisian AM, Benevenuto A, Tyberg A, Kumar R, Igel L, Verna EC, et
al: Endoscopic sleeve gastroplasty significantly reduces body mass
index and metabolic complications in obese patients. Clin
Gastroenterol Hepatol. 15:504–510. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ou H, Cai S, Liu Y, Xia M and Peng J: A
noninvasive diagnostic model to assess nonalcoholic hepatic
steatosis in patients with chronic hepatitis B. Therap Adv
Gastroenterol. 10:207–217. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wang L, Chen S and Xu K: IL-17 expression
is correlated with hepatitis B-related liver diseases and fibrosis.
Int J Mol Med. 27:385–392. 2011.PubMed/NCBI
|
|
20
|
Bai Q, An J, Wu X, You H, Ma H, Liu T, Gao
N and Jia J: HBV promotes the proliferation of hepatic stellate
cells via the PDGF-B/PDGFR-β signaling pathway in vitro. Int
J Mol Med. 30:1443–1450. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Fagone P, Mangano K, Mammana S, Pesce A,
Pesce A, Caltabiano R, Giorlandino A, Portale TR, Cavalli E, et al:
Identification of novel targets for the diagnosis and treatment of
liver fibrosis. Int J Mol Med. 36:747–752. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Fagone P, Mangano K, Pesce A, Portale TR,
Puleo S and Nicoletti F: Emerging therapeutic targets for the
treatment of hepatic fibrosis. Drug Discov Today. 21:369–375. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zhang Q, Xu M, Qu Y, Li Z, Zhang Q, Cai X
and Lu L: Analysis of the differential expression of circulating
microRNAs during the progression of hepatic fibrosis in patients
with chronic hepatitis B virus infection. Mol Med Rep.
12:5647–5654. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lambrecht J, Jan Poortmans P, Verhulst S,
Reynaert H, Mannaerts I and van Grunsven LA: Circulating
ECV-associated miRNAs as potential clinical biomarkers in early
stage HBV and HCV induced liver fibrosis. Front Pharmacol.
8:562017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zheng J, Zhou Z, Xu Z, Li G, Dong P, Chen
Z, Lin D, Chen B and Yu F: Serum microRNA-125a-5p, a useful
biomarker in liver diseases, correlates with disease progression.
Mol Med Rep. 12:1584–1590. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Yuen MF, Yuan HJ, Wong DK, Yuen JC, Wong
WM, Chan AO, Wong BC, Lai KC and Lai CL: Prognostic determinants
for chronic hepatitis B in Asians: Therapeutic implications. Gut.
54:1610–1615. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kumar M, Sarin SK, Hissar S, Pande C,
Sakhuja P, Sharma BC, Chauhan R and Bose S: Virologic and
histologic features of chronic hepatitis B virus-infected
asymptomatic patients with persistently normal ALT.
Gastroenterology. 134:1376–1384. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Terrault NA, Bzowej NH, Chang KM, Hwang
JP, Jonas MM and Murad MH: American Association for the Study of
Liver Diseases: AASLD guidelines for treatment of chronic hepatitis
B. Hepatology. 63:261–283. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Xue X and Cai S: Comment on ‘assessment of
liver stiffness in pediatric fontan patients using transient
elastography’. Can J Gastroenterol Hepatol. 2016:93439602016.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Tai DI, Lin SM, Sheen IS, Chu CM, Lin DY
and Liaw YF: Long-term outcome of hepatitis B e antigen-negative
hepatitis B surface antigen carriers in relation to changes of
alanine aminotransferase levels over time. Hepatology.
49:1859–1867. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Prati D, Taioli E, Zanella A, Della Torre
E, Butelli S, Del Vecchio E, Vianello L, Zanuso F, Mozzi F, Milani
S, et al: Updated definitions of healthy ranges for serum alanine
aminotransferase levels. Ann Intern Med. 137:1–10. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Lin CL, Liao LY, Liu CJ, Yu MW, Chen PJ,
Lai MY, Chen DS and Kao JH: Hepatitis B viral factors in
HBeAg-negative carriers with persistently normal serum alanine
aminotransferase levels. Hepatology. 45:1193–1198. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kumar M, Sharma P, Garg H, Kumar R, Bhatia
V and Sarin SK: Transient elastographic evaluation in adult
subjects without overt liver disease: Influence of alanine
aminotransferase levels. J Gastroenterol Hepatol. 26:1318–1325.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Yasuda M, Shimizu I, Shiba M and Ito S:
Suppressive effects of estradiol on dimethylnitrosamine-induced
fibrosis of the liver in rats. Hepatology. 29:719–727. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Lemoine M, Thursz M, Mallet V and
Shimakawa Y: Diagnostic accuracy of the gamma-glutamyl
transpeptidase to platelet ratio (GPR) using transient elastography
as a reference. Gut. 66:195–196. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Li Q, Lu C, Li W, Huang Y and Chen L: The
independent predictors of significant liver histological changes in
chronic hepatitis B virus infection patients with persistently
high-normal or low-normal alanine transaminase levels. Discov Med.
23:19–25. 2017.PubMed/NCBI
|