Introduction
Refractory wounds because of trauma, burn/scald,
vascular ulcer on the hand or foot, and the diabetic foot pose a
challenge in clinical hand and foot surgery (1). Clinical manifestations of refractory
wounds include local pain and discomfort, and secondary infection
of surrounding skin resulting in skin irritation, congestion,
exudation, erosion, and ulcers. The condition poses a substantial
challenge for clinical intervention, which causes great
psychological stress to patients and medical personnel. Patients
can lose confidence in both their ability to be cured and their
future quality of life (2). Vacuum
sealing drainage (VSD) is a therapeutic technique which involves a
vacuum dressing to promote healing of acute or chronic wounds. It
involves application of wound dressing made of polyethylene alcohol
hydrated alginate foam with drainage tubes to fill or cover the
wound surface of patients with skin or soft tissue defects. Next, a
biological semipermeable membrane film is applied to seal the wound
surface with the dressing on to form a closed microenvironment.
When the drainage tubes are connected with a vacuum source, a
controlled negative pressure is established, which draws out fluid
from the wound and increases blood flow to the affected area
(3). The established negative
pressure can also promote protein synthesis on the wound surface to
accelerate granulation tissue growth, and eventually promotes
healing of the wound. In addition, the closed microenvironment
formed through sealing with the biological semipermeable membrane
prevents the wound surface from infection from contact with the
outside environment. Drainage tubes with multiple side-openings
inserted in the wound dressing aspirate the necrotic tissue and
exudate in a timely manner, thus reducing the need for antibiotic
use (4). Epidermal growth factor
(EGF) is a multifunctional cellular growth factor that acts by
binding to the epidermal growth factor receptor (EGFR) on the cell
surface (5). EGFR is expressed on
the cell membrane of epidermal cells, fibroblasts, endothelial
cells, and smooth muscle cells. Furthermore, the highest levels of
EGFR expression are found in epidermal cells (6). Binding of EGF to EGFR with high
affinity stimulates the receptor's intrinsic protein tyrosine
kinase activity, which subsequently stimulates a signal
transduction cascade leading to multiple biochemical changes in the
cell. This includes elevation of calcium level, increase of
glycolysis and protein synthesis, and upregulation of EGFR
expression. Binding of EGF to EGFR eventually promotes DNA
synthesis and cell proliferation, resulting in accelerated cell
metabolism (7,8). A solution containing recombinant human
epidermal growth factor (rhEGF) for external use can be applied to
burn wounds (including shallow and deep second degree burn wounds),
residual wounds, various types of chronic ulcer wounds (including
vascular, radiation, and diabetic ulcer), and fresh wounds on skin
donor sites. In the present study, we evaluated the efficacy of VSD
combined with rhEGF treatment for refractory traumatic wounds of
the extremities, and its effect on the serum levels of
interleukin-6 (IL-6), TNF-α, and IL-2.
Patients and methods
Patients
Ninety-eight patients with refractory traumatic
wounds in the extremities who were admitted to Shengli Hospital
from January 2015 to December 2016 were recruited.
Inclusion criteria
i) Patients with chronic refractory wounds for over
1 month caused by all forms of trauma, continuous deteriorating
wounds, or wounds with a diameter >3 cm; ii) patients not
previously treated with VSD; iii) patients with no improvement
after 7 days of drug treatment for a normal wound; and iv) patients
with contaminated wounds.
Exclusion criteria
i) Patients with combined severe heart, brain,
liver, kidney, or hematopoietic diseases; ii) patients with
malignant tumors derived from skin or soft tissue; iii) patients
with immune diseases who were exposed to high doses of
immunosuppressive agents, steroid hormones, or chemotherapy drugs
for extended periods of time; iv) patients with severe malnutrition
or moderate to severe anemia; and v) patients with active bleeding
on the wound.
Causes for complete loss to follow-up
and remedial measure
There were two causes for complete loss to
follow-up. Either patients chose to withdraw from the trial or they
were transferred to other hospitals for further treatment. In case
of patient withdrawal, new patients were recruited according to the
inclusion and exclusion criteria.
Medical ethics
Patients or family members signed a consent form to
participate in the study. Safety and welfare of the patients were
protected according to relevant clinical guidelines. Privacy of the
patients was protected by keeping their medical records
confidential.
Clinical trial design:
Double-blind
Researchers were divided into four groups. The first
group was responsible for screening and grouping of the patients,
the second group for patient treatment, the third group for
collecting clinical data, and the fourth group for statistical
analysis and manuscript writing. Assignment of patients was
strictly confidential to them. Moreover, the detailed procedures
performed by the four groups of researchers were kept confidential
from each other.
Grouping of patients
In this study, a total of 70 males and 28 females,
aged 36–78 years, with mean age of 58.5±9.4 years were enrolled.
Regarding cause of wounds, there were 39 cases of injury from car
accident, 25 cases of injury from falling object, nine cases of
injury from electric shock, 10 cases of varicose ulcer, and 15
cases of diabetic foot. Regarding wound location, there were 32
cases with wounds on the heel, eight cases on the top of the foot,
18 cases on the ankle, 17 cases on the back of the hand, eight
cases on the palm, and 15 cases on the calf. Regarding wound
condition, there were 59 cases with slight wound contamination or
minimal purulent exudation, and 39 cases with severe infection or
obvious pus with foul odor. The 98 patients were randomly divided
into the combined treatment group (underwent combined treatment
with VSD and rhEGF) and control group (underwent VSD only), with 49
cases each. There were 36 males and 13 females with mean age of
59.21±10.23 years in the combined treatment group, and 34 males and
15 females with mean age of 57.80±9.24 years in the control group.
The medical Ethics Committee of Shengli Hospital reviewed and
approved this study. Patients or their families signed the informed
consent.
Methods
VSD was performed on all patients in both groups.
After successful local anesthesia with 1% lidocaine, wounds were
routinely rinsed three times with benzalkonium bromide, povidone
iodine, H2O2, and 0.5% iodophor solution,
followed by rinsing with saline to clean the wounds and surrounding
areas to remove the necrotic stratum corneum. For patients in the
combined treatment group, a solution of rhEGF was uniformly sprayed
on the surface of wounds after the surrounding skin was dry,
followed by incubation for at least 90 sec. For patients in the
control group, no rhEGF spray was applied after saline rinse and
air-dry. Specific application of the VSD dressing (Shandong
Chuangkang Biotechnology Co., Ltd.) depended on the shape and size
of the wound. If the wound area was large, it was covered by the
dressing in an imbricate mode, and the VSD dressing was made to
completely cover the wound and 2–3 cm of surrounding skin. If the
wound was deep, the dressing was filled completely to the bottom of
the cavity, leaving no dead space. The biologically permeable film
was applied above the dressing to cover an area of 4–5 cm wider
than the wound surface. After a double check of tight sealing, the
drainage tube was connected to a negative pressure drainage device
(Shandong Weigao New Life Medical Devices Co., Ltd., Weihai,
China), and a negative pressure of 80–125 mmHg was set and
maintained. The wound dressing was replaced every 5 days. During
the drainage period, wounds in the two groups were rinsed daily
with large amounts of saline. Additionally, a solution of rhEGF was
uniformly sprayed on the wound surface in patients in the combined
treatment group. During the application of VSD, an airproof seal
was observed and maintained, and the liquid level inside the
drainage bottle was observed regularly. If the drainage tube was
blocked, heparin water was injected into the drainage tube to flush
it through. The VSD process was carried out for 14 days in both
groups, following which the status of healing was evaluated.
Observed indicators
Formation of granulation tissue on the wound surface
was observed and scored within 1 month after treatment started. The
formation was rated good and assigned a score of 3 points if the
granulation tissue covered 95% of the wound area, was bright red
and appeared fine-grained, and bled easily when touched. The
formation was rated fairly good and assigned a score of 2 points if
the granulation tissue covered 50–95% of the wound area, was bright
red, and appeared to bleed when touched. The formation was assigned
a score of 1 point if the granulation tissue covered less than 50%
of the wound area, and did not appear to bleed when touched. The
wound healing rate was calculated after 1 week of treatment. Wound
healing rate (%) = (original wound area – non-healing wound area) ÷
original wound area × 100%. The time of complete healing and
epithelialization time were also recorded. The former was the time
period from beginning of treatment to the time when the wound
healed completely. The latter was the time period from beginning of
treatment to the time when epithelialization began to appear on the
wound surface. Changes in the levels of inflammatory factor were
monitored. Upper limb venous blood (5 ml) was drawn while fasting
in the morning on the day before treatment began and on the
following day after two weeks of continuous treatment. The serum
levels of IL-6, IL-2, and TNF-α were measured using a
double-antibody sandwich enzyme-linked immunosorbent assay. The kit
was from Shanghai Beyotime Biotechnology Inc. (Shanghai,
China).
Statistical analysis
Data were processed and analyzed using SPSS 20.0
statistical software (IBM SPSS, Armonk, NY, USA). Numerical data
are expressed as mean ± standard deviation. Intergroup comparisons
were by t-test, and paired t-test was used for intragroup
comparisons before and after treatment. Categorical data are
expressed as percentage (%). A Chi-square test (χ2 test)
was used for comparisons between groups. Wound healing was analyzed
using a log-rank test. Differences were considered statistically
significant when p<0.05.
Results
General data of patients
Patient age, sex ratio, and wound area were
comparable between the two groups, and the differences were not
statistically significant (p>0.05) (Table I). No patients withdrew from the
study in either group during the entire treatment process, and
there were no patients lost to follow-up because of adverse events.
The follow-up rate while in hospital and 12 weeks after treatment
reached 100%.
 | Table I.General data of patients in the two
groups. |
Table I.
General data of patients in the two
groups.
| Parameters | Combined treatment
group (n=49) | Control group
(n=49) |
χ2/t-value | P-value |
|---|
| Male/female | 36/13 | 34/15 | 0.051 | 0.821 |
| Age (years) | 59.2±10.2 | 57.8±9.2 | 0.957 | 0.352 |
| Wound cause |
|
|
|
|
| Car
accident | 21 | 18 | 0.194 | 0.65 |
| Struck by
falling object | 12 | 13 |
|
|
| Electric
shock | 4 | 5 |
|
|
| Diabetic
foot | 7 | 8 |
|
|
| Varicose
ulcer | 5 | 5 |
|
|
| Wound location |
|
|
|
|
| Heel | 15 | 17 | 0.044 | 0.807 |
| Top of
foot | 4 | 4 |
|
|
|
Ankle | 10 | 8 |
|
|
| Back of
hand | 9 | 8 |
|
|
| Palm | 4 | 4 |
|
|
| Calf | 7 | 8 |
|
|
| Wound
area (cm2) | 35.6±14.3 | 34.8±13.2 | 0.796 | 0.426 |
Formation of granulation tissue
The formation of granulation tissue in the two
groups was mostly similar before treatment, and there was no
significant difference between the two groups (p>0.05).
Formation of granulation tissue on the wound surface was
significantly improved 1 week after the start of treatment in the
combined treatment group (p<0.05). In the control group,
formation of granulation tissue was moderately improved 1 week
after treatment started, and the difference was statistically
significant (p<0.05). Comparing the two groups 1 week after
treatment started, formation of granulation tissue was superior in
the combined treatment group compared with the control group, and
the difference was statistically significant (p<0.05) (Table II). These results indicated that
combined treatment with VSD and rhEGF was significantly effective
after the first day of treatment, and wound symptoms subsided
quickly.
| Table II.Formation of granulation tissue 1 week
after the start of treatment in both groups. |
Table II.
Formation of granulation tissue 1 week
after the start of treatment in both groups.
|
|
|
| Granulation tissue
formation score |
|---|
|
|
|
|
|
|---|
| Group | n | Observation time | 1 point | 2 points | 3 points |
|---|
| Combined
treatment | 49 | Before treatment | 26 | 21 | 2 |
|
|
| After treatment | 1 | 26 | 22 |
| Control | 49 | Before treatment | 24 | 23 | 2 |
|
|
| After treatment | 6 | 31 | 12 |
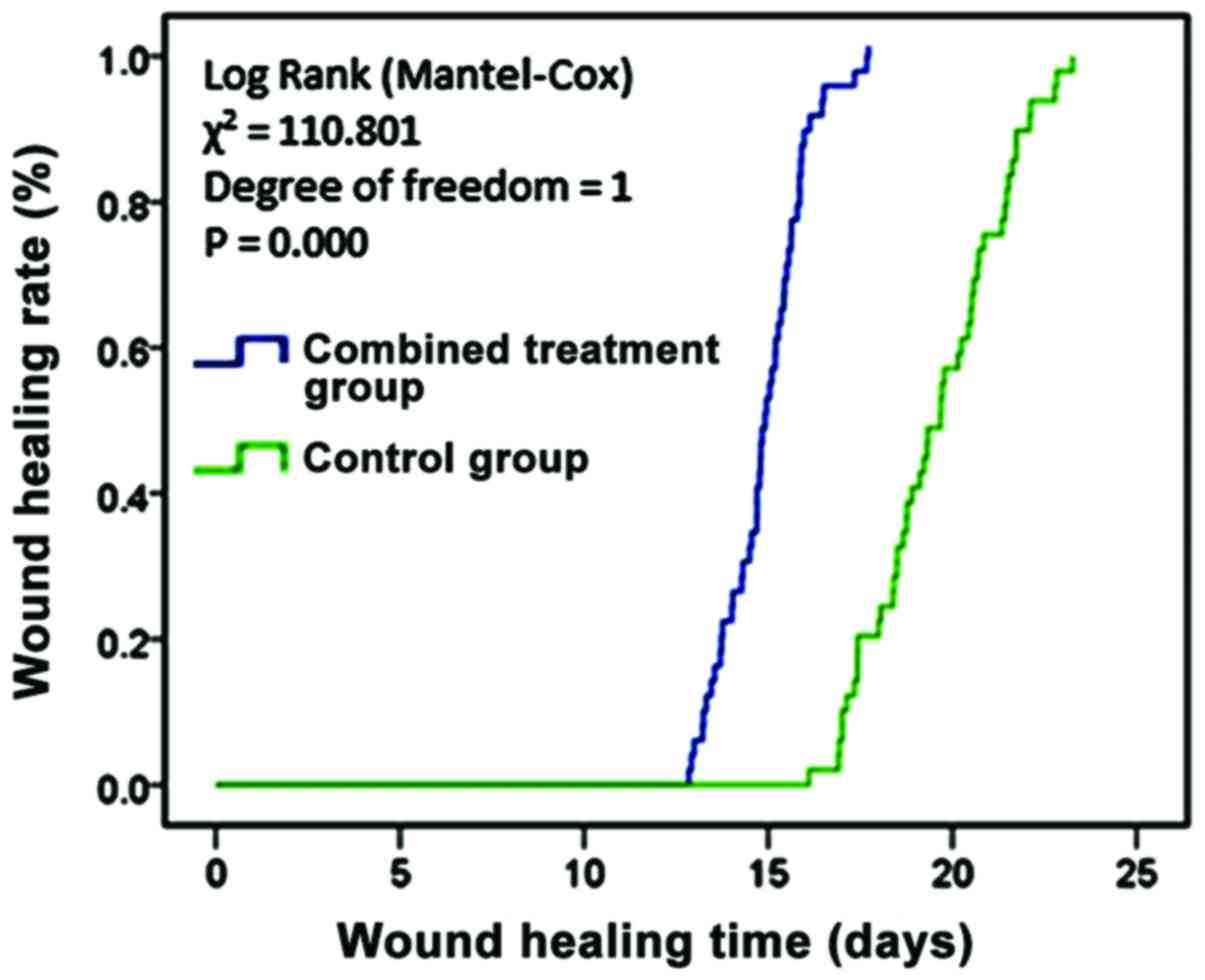
Wound healing in the two groups
One week after treatment started, the residual wound
area, wound healing rate, and time of complete healing were
compared between patients in the two groups. In the combined
treatment group, the parameters were 15.32±1.46 cm2,
63.50±4.75%, and 15.11±2.24 days, respectively. In the control
group, they were 23.1±2.2 cm2, 31.79±3.52%, and
19.36±2.76 days, respectively. The differences in the parameters
between the two groups were all statistically significant
(p<0.05) (Table III). Fig. 1 shows the comparison of wound healing
in the two groups, which indicated that combined treatment with VSD
and rhEGF improved the wound healing rate, and shortened the times
of epithelialization and wound healing.
| Table III.Wound healing in the two groups
(n=49). |
Table III.
Wound healing in the two groups
(n=49).
| Group | Residual wound area
(cm2) | Wound healing rate
(%) | Epithelialization
time (days) | Wound healing time
(days) |
|---|
| Combined
treatment | 15.32±1.46 | 63.50±4.75 | 3.72±1.51 | 15.11±1.24 |
| Control | 23.10±2.24 | 31.79±3.52 | 5.58±1.88 | 19.63±1.76 |
| t-test | 8.654 | 12.310 | 6.894 | 6.537 |
| P-value | 0.001 | <0.01 | 0.023 | 0.031 |
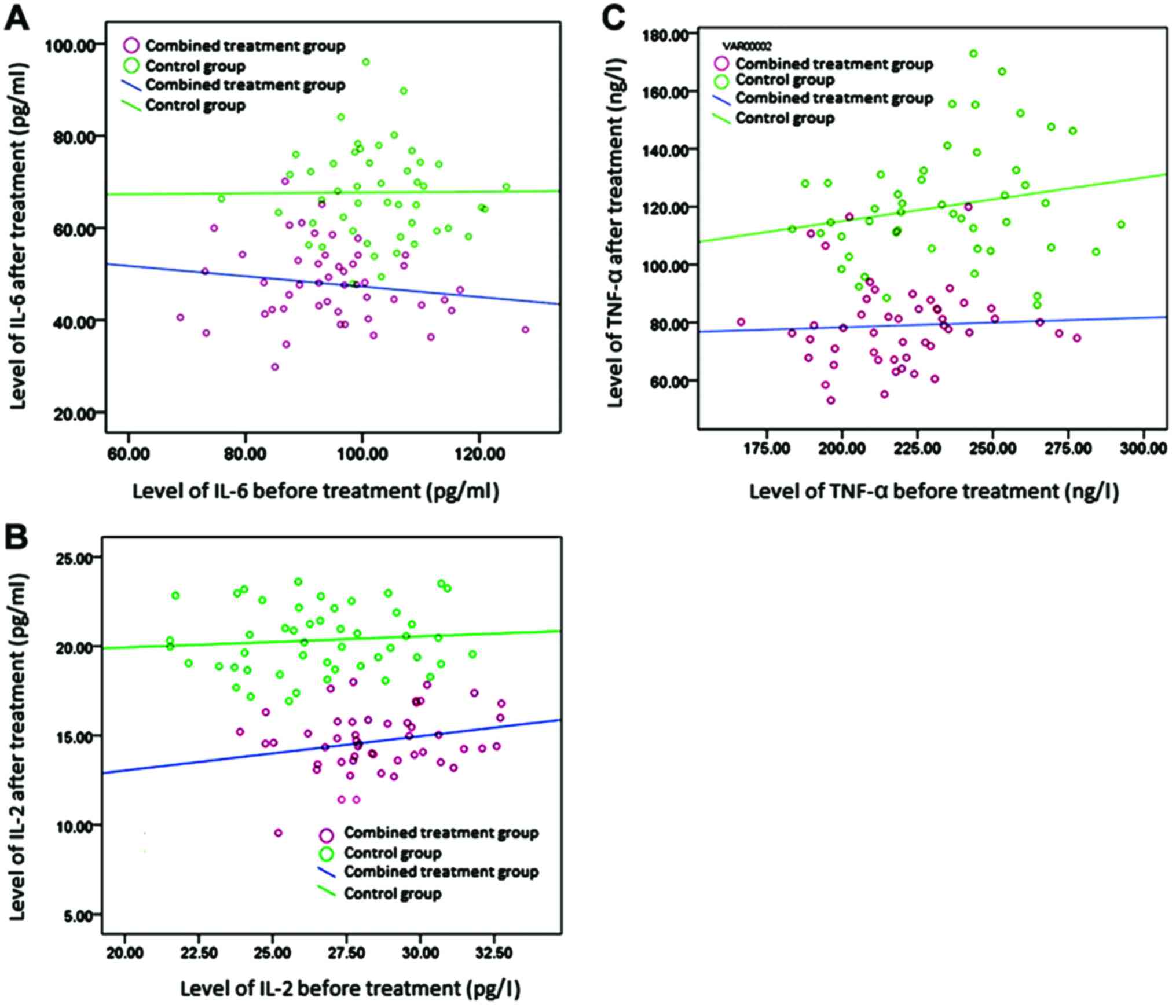
Changes in the levels of inflammatory
factors
The serum levels of inflammatory mediators, IL-6,
IL-2, and TNF-α, were comparable before treatment in the two
groups, and the differences were not statistically significant
(p>0.05). After treatment, the levels were significantly lower
in the combined treatment group than in the control group
(p<0.05). In another comparison, the levels of these three
inflammatory mediators were lower after treatment than before
treatment in both groups, and the differences were statistically
significant (p<0.05) (Tables
IV–VI and Fig. 2).
| Table IV.Serum levels of IL-6 before and after
treatment in the two groups (pg/ml, n=49). |
Table IV.
Serum levels of IL-6 before and after
treatment in the two groups (pg/ml, n=49).
| Group | Before treatment | After treatment | t-test | P-value |
|---|
| Combined
treatment | 94.37±12.56 | 48.64±8.91 | 11.007 | 0.001 |
| Control | 99.62±11.36 | 69.43±10.23 | 8.926 | 0.009 |
| t-test | 2.031 | 12.237 | – | – |
| P-value | 0.452 | 0.001 | – | – |
| Table VI.Serum levels of TNF-α before and
after treatment in the two groups (ng/l, n=49). |
Table VI.
Serum levels of TNF-α before and
after treatment in the two groups (ng/l, n=49).
| Group | Before
treatment | After
treatment | t-test | P-value |
|---|
| Combined
treatment | 224.43±24.58 | 80.53±14.62 | 14.522 | 0 |
| Control | 231.42±25.36 | 121.32±22.86 | 12.056 | 0.001 |
| t-test | 1.694 | 11.695 | – | – |
| P-value | 0.337 | <0.01 | – | – |
Discussion
Chronic refractory wounds in the extremities are
quite common in clinic. These wounds do not heal for a long period
of time, and their conventional treatment is mainly dressing
change. Wound healing takes a long time, and if the wound does not
heal, surgical skin-grafting is eventually performed to repair it
(9,10). Chronic ulcer wounds are often
associated with chronic infection, and are resistant to multiple
antibiotics, thus resulting in low survival rate of skin grafts and
posing a challenge in clinical treatment.
A number of studies have shown that (11–13) VSD
treatment can effectively shorten wound healing time, reduce the
pain associated with wound dressing changes, and effectively avoid
cross infection. VSD is performed in a closed system, and the
negative pressure drainage system promptly removes any exudates and
necrotic tissue to achieve zero necrotic tissue accumulation. In
addition, VSD can protect the wound from contamination, stimulate
the wound surface and granulation tissue for rapid and healthy
growth, promote wound healing, reduce application of antibiotics,
and increase blood flow in the wound surface. The continuous
negative pressure can be adjusted to match physiological conditions
so that it does not adversely affect blood circulation. Moreover,
it can effectively prevent the formation of residual abscesses and
dead space (14). More importantly,
the continuous negative pressure promotes the flow of body fluid
from the wound to the drainage tube, which provides an effective
and sustained auxiliary power to blood circulation (15). rhEGF is the active ingredient in the
rhEGF external solution which also contains 10% glycerol and 1.0%
mannitol as protective agents. It can promote the synthesis of DNA,
RNA, and hydroxyproline during the repair of skin and mucosal wound
tissues. In addition, it can accelerate granulation tissue
formation and epithelial cell proliferation, thus shortening the
wound-healing time. In this study, we found that patients in the
control group (treated with VSD only) had lower levels of
inflammatory factors and improved granulation tissue formation
score compared with before treatment (p<0.05).
EGF is an important growth factor synthesized in the
body. It has a potent stimulatory effects on division and growth of
epidermal cells. It can promote rapid proliferation of various
epithelial cells to accelerate healing of surface ulcer wounds
(16). Xing et al (17) reported that combined treatment with
VSD and EGF for surface refractory wounds is effective, and can
promote repair of damaged tissue and accelerate wound healing.
Dumantepe et al (18)
reported the efficacy of recombinant human EGF in the treatment of
chronic diabetic foot ulcer. Its debridement efficiency for
patients in the treatment group was significantly better than in
the control group. In addition, it reduced the wound infection
rate. Gainza et al (19)
prepared rhEGF-loaded Poly-Lactic-co-Glycolic-Acid-Alginate
microspheres for treatment in a Wistar rat model of diabetic skin
wound. The in vivo experiments showed a significant decrease
of the wound area by days 7 and 11, complete re-epithelialization
by day 11, and earlier resolution of the inflammatory process.
These findings demonstrated that application of rhEGF-loaded
microspheres promoted more effective wound healing. In this study,
we found that combined treatment with rhEGF and VSD was effective
in patients after the first day of treatment, and wound symptoms
subsided quickly. In addition, combined treatment with rhEGF and
VSD improved the wound-healing rate, and shortened the
epithelialization and wound-healing times. These findings indicated
that the effect of rhEGF on promoting epidermal cell growth was
enhanced under the continuous negative pressure of VSD treatment
because of improved blood circulation and decreased
inflammation.
Patients with refractory wounds experience strong
local inflammatory responses, demonstrated by elevated levels of
inflammatory mediators such as IL-6, IL-2, and TNF-α (20). Nasole et al (20) reported that IL-6 and TNF-α are key
mediators of general inflammation, which directly and indirectly
induce the production of other cytokines and growth factors that
affect endothelial and fibroblast function. IL-6 was confirmed to
be necessary for epithelial formation because of its role in
granulation tissue formation, as demonstrated by delayed wound
healing process in IL-6 knockout mice (21). With the healing of local wounds,
local inflammation was rapidly reduced, and the levels of
inflammatory factors returned to normal, resulting in decreased
decomposition of wound tissue protein and promotion of wound
healing (22). In this study, the
combined treatment was demonstrated to be more effective than the
control treatment in reducing the levels of inflammatory
factors.
In conclusion, combined treatment with VSD and rhEGF
contributed to shortened healing time of refractory wounds in the
extremities, and decreased inflammatory response on the wound
surface. Measurement of related inflammatory factors provided a
reference for prognostic assessment of refractory wounds, which
merits clinical promotion.
References
|
1
|
Game FL, Attinger C, Hartemann A,
Hinchliffe RJ, Löndahl M, Price PE and Jeffcoate WJ: International
Working Group on the Diabetic Foot: IWGDF guidance on use of
interventions to enhance the healing of chronic ulcers of the foot
in diabetes. Diabetes Metab Res Rev. 32 Suppl 1:75–83. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kim H, Kong WH, Seong KY, Sung DK, Jeong
H, Kim JK, Yang SY and Hahn SK: Hyaluronate-epidermal growth factor
conjugate for skin wound healing and regeneration.
Biomacromolecules. 17:3694–3705. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Suh H, Lee AY, Park EJ and Hong JP:
Negative pressure wound therapy on closed surgical wounds with dead
space: Animal study using a swine model. Ann Plast Surg.
76:717–722. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Poon H, Le Cocq H, Mountain AJ and
Sargeant ID: Dermal fenestration with negative pressure wound
therapy: A technique for managing soft tissue injuries associated
with high-energy complex foot fractures. J Foot Ankle Surg.
55:161–165. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Memon AA, Sundquist K, Ahmad A, Wang X,
Hedelius A and Sundquist J: Role of IL-8, CRP and epidermal growth
factor in depression and anxiety patients treated with
mindfulness-based therapy or cognitive behavioral therapy in
primary health care. Psychiatry Res. 254:311–316. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Guo XF, Zhu XF, Cao HY, Zhong GS, Li L,
Deng BG, Chen P, Wang PZ, Miao QF and Zhen YS: A bispecific
enediyne-energized fusion protein targeting both epidermal growth
factor receptor and insulin-like growth factor 1 receptor showing
enhanced antitumor efficacy against non-small cell lung cancer.
Oncotarget. 8:27286–27299. 2017.PubMed/NCBI
|
|
7
|
Gomez-Villa R, Aguilar-Rebolledo F,
Lozano-Platonoff A, Teran-Soto JM, Fabian-Victoriano MR,
Kresch-Tronik NS, Garrido-Espíndola X, Garcia-Solis A,
Bondani-Guasti A, Bierzwinsky-Sneider G, et al: Efficacy of
intralesional recombinant human epidermal growth factor in diabetic
foot ulcers in Mexican patients: A randomized double-blinded
controlled trial. Wound Repair Regen. 22:497–503. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Singla S, Garg R, Kumar A and Gill C:
Efficacy of topical application of beta urogastrone (recombinant
human epidermal growth factor) in Wagner's Grade 1 and 2 diabetic
foot ulcers: Comparative analysis of 50 patients. J Nat Sci Biol
Med. 5:273–277. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wu W, Zeng LN, Peng YY, Lu XH, Li CY and
Wang ZC: The effects of recombinant human epithelialgrowth factor
and protein-free calf blood extract for recovery of corneal
mechanical epithelial defects healing and neovascularization. Eur
Rev Med Pharmacol Sci. 18:3406–3411. 2014.PubMed/NCBI
|
|
10
|
Shin JU, Kang SW, Jeong JJ, Nam KH, Chung
WY and Lee JH: Effect of recombinant human epidermal growth factor
on cutaneous scar quality in thyroidectomy patients. J Dermatolog
Treat. 26:159–164. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ojalvo AG, Acosta JB, Marí YM, Mayola MF,
Pérez CV, Gutiérrez WS, Marichal II, Seijas EÁ, Kautzman AM,
Pacheco AE, et al: Healing enhancement of diabetic wounds by
locally infiltrated epidermal growth factor is associated with
systemic oxidative stress reduction. Int Wound J. 14:214–225. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yang F, Shi B and Cao L: Effect of vacuum
sealing drainage on the expression of VEGF and miRNA-17-5p in
seawater-immersed blast-injury wounds. Exp Ther Med. 13:1081–1086.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Braun LR, Fisk WA, Lev-Tov H, Kirsner RS
and Isseroff RR: Diabetic foot ulcer: An evidence-based treatment
update. Am J Clin Dermatol. 15:267–281. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ertugrul BM, Lipsky BA and Guvenc U;
Turkish Intralesional Epidermal Growth Factor Study Group for
Diabetic Foot Wounds, : An assessment of intralesional epidermal
growth factor for treating diabetic foot wounds the first
experiences in Turkey. J Am Podiatr Med Assoc. 107:17–29. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Cheng HT, Hsu YC and Wu CI: Efficacy and
safety of negative pressure wound therapy for Szilagyi grade III
peripheral vascular graft infection. Interact Cardiovasc Thorac
Surg. 19:1048–1052. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Novak A, Khan WS and Palmer J: The
evidence-based principles of negative pressure wound therapy in
trauma and orthopedics. Open Orthop J. 8:168–177. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Xing B, Wu F, Li T, Qi S, Xie J and Ye Z:
Experimental study of comparing rhEGF with rhβFGF on improving the
quality of wound healing. Int J Clin Exp Med. 6:655–661.
2013.PubMed/NCBI
|
|
18
|
Dumantepe M, Fazliogullari O, Seren M,
Uyar I and Basar F: Efficacy of intralesional recombinant human
epidermal growth factor in chronic diabetic foot ulcers. Growth
Factors. 33:128–132. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Gainza G, Aguirre JJ, Pedraz JL, Hernández
RM and Igartua M: rhEGF-loaded PLGA-Alginate microspheres enhance
the healing of full-thickness excisional wounds in diabetised
Wistar rats. Eur J Pharm Sci. 50:243–252. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Nasole E, Nicoletti C, Yang ZJ, Girelli A,
Rubini A, Giuffreda F, Di Tano A, Camporesi E and Bosco G: Effects
of alpha lipoic acid and its R+ enantiomer supplemented to
hyperbaric oxygen therapy on interleukin-6, TNF-α and EGF
production in chronic leg wound healing. J Enzyme Inhib Med Chem.
29:297–302. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Rozenblum N, Zeira E, Bulvik B, Gourevitch
S, Yotvat H, Galun E and Goldberg SN: Radiofrequency ablation:
inflammatory changes in the periablative zone can induce global
organ effects, including liver regeneration. Radiology.
276:416–425. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Okada Y, Shirai K, Reinach PS,
Kitano-Izutani A, Miyajima M, Flanders KC, Jester JV, Tominaga M
and Saika S: TRPA1 is required for TGF-β signaling and its loss
blocks inflammatory fibrosis in mouse corneal stroma. Lab Invest.
94:1030–1041. 2014. View Article : Google Scholar : PubMed/NCBI
|